
Complications Arising Due to Orthodontic Treatment—A Systematic Review and Meta-Analysis

 , ,
, ,  and
and 
Abstract
:1. Introduction
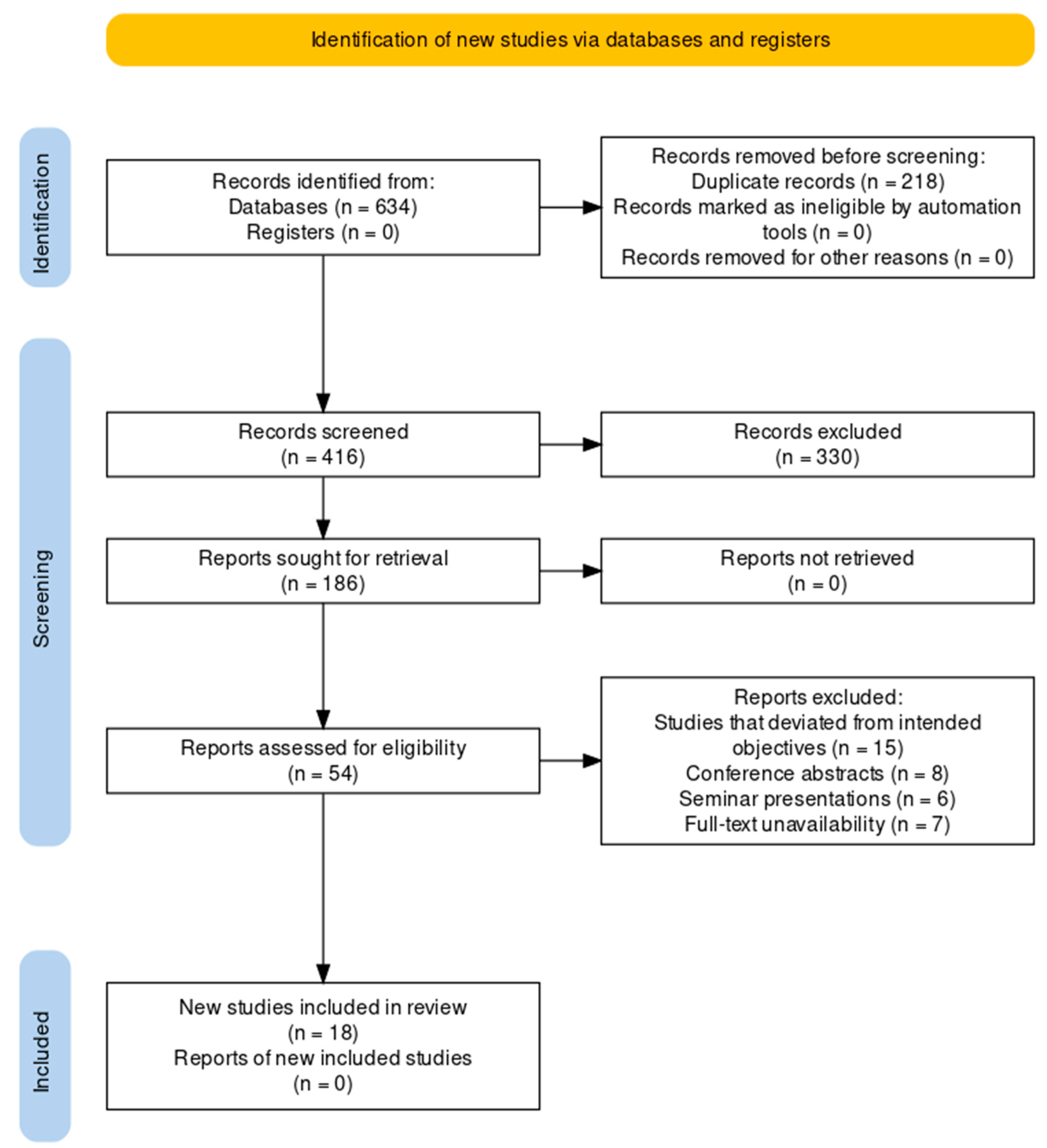
2. Materials and Methods
2.1. Study Design
2.2. Clinical Question Explored
2.3. Inclusion Criterion
- Studies that reported on complications arising due to orthodontic treatment in children and adults;
- Studies that reported on orthodontic treatments, including fixed appliances, removable appliances, clear aligners, or other types of orthodontic devices;
- Studies that reported on outcomes related to complications, including root resorption, periodontal disease, caries, pain, discomfort, or any other complications related to orthodontic treatment;
- Studies that reported comparisons between different types of orthodontic treatments, such as clear aligners vs. fixed appliances, or other comparisons;
- Studies that were conducted in humans.
2.4. Exclusion Criteria
- Studies that were not available as full texts or were not written in English;
- Studies that did not report on complications arising due to orthodontic treatment;
- Studies that reported on complications related to other dental treatments or surgeries, such as tooth extraction or implant placement;
- Studies that reported on orthodontic treatment in animals or in vitro studies;
- Studies that reported on orthodontic treatments that were not commonly used, such as self-ligating brackets or other unusual modalities;
- Case reports or case series;
- Studies that had atrociously low sample sizes (<10 participants);
- Studies that were duplicates or reported on the same population, intervention, or outcomes as other studies already included in the review.
2.5. Search Strategy
2.6. Data Gathering Protocol
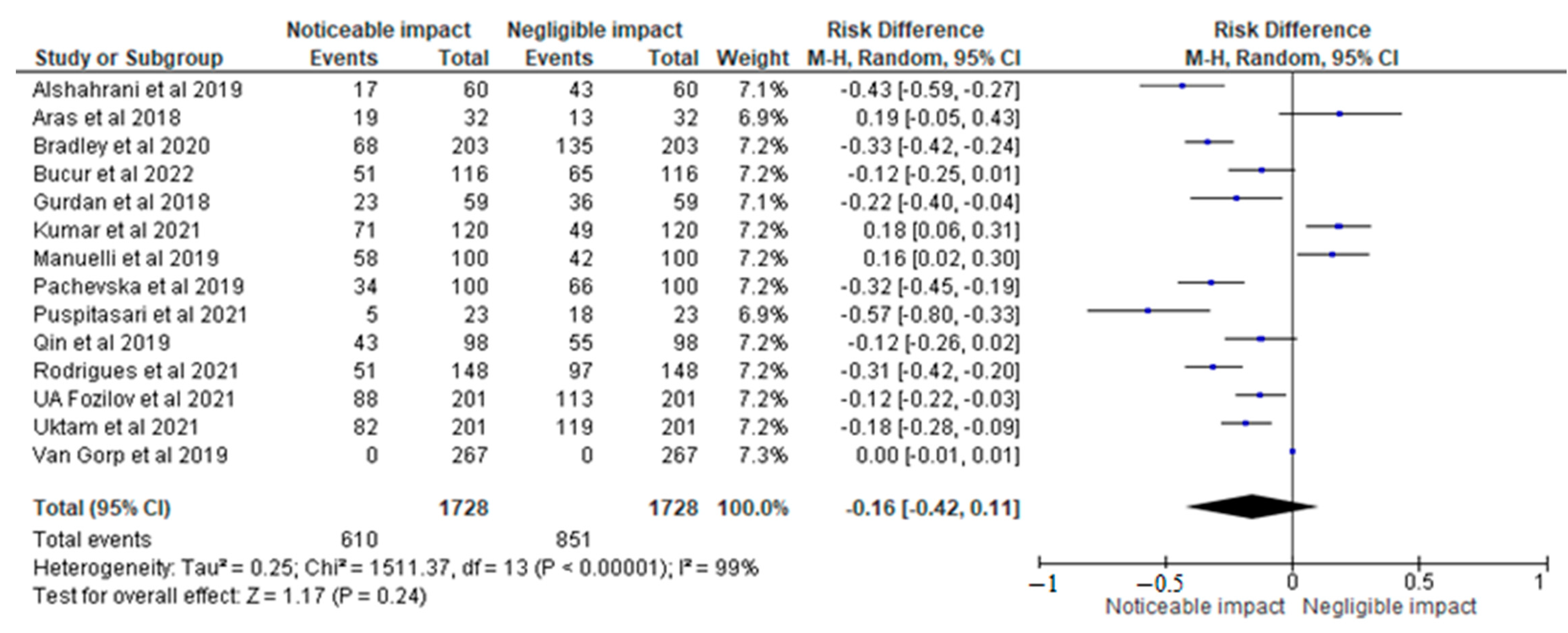
2.7. Statistical Analysis
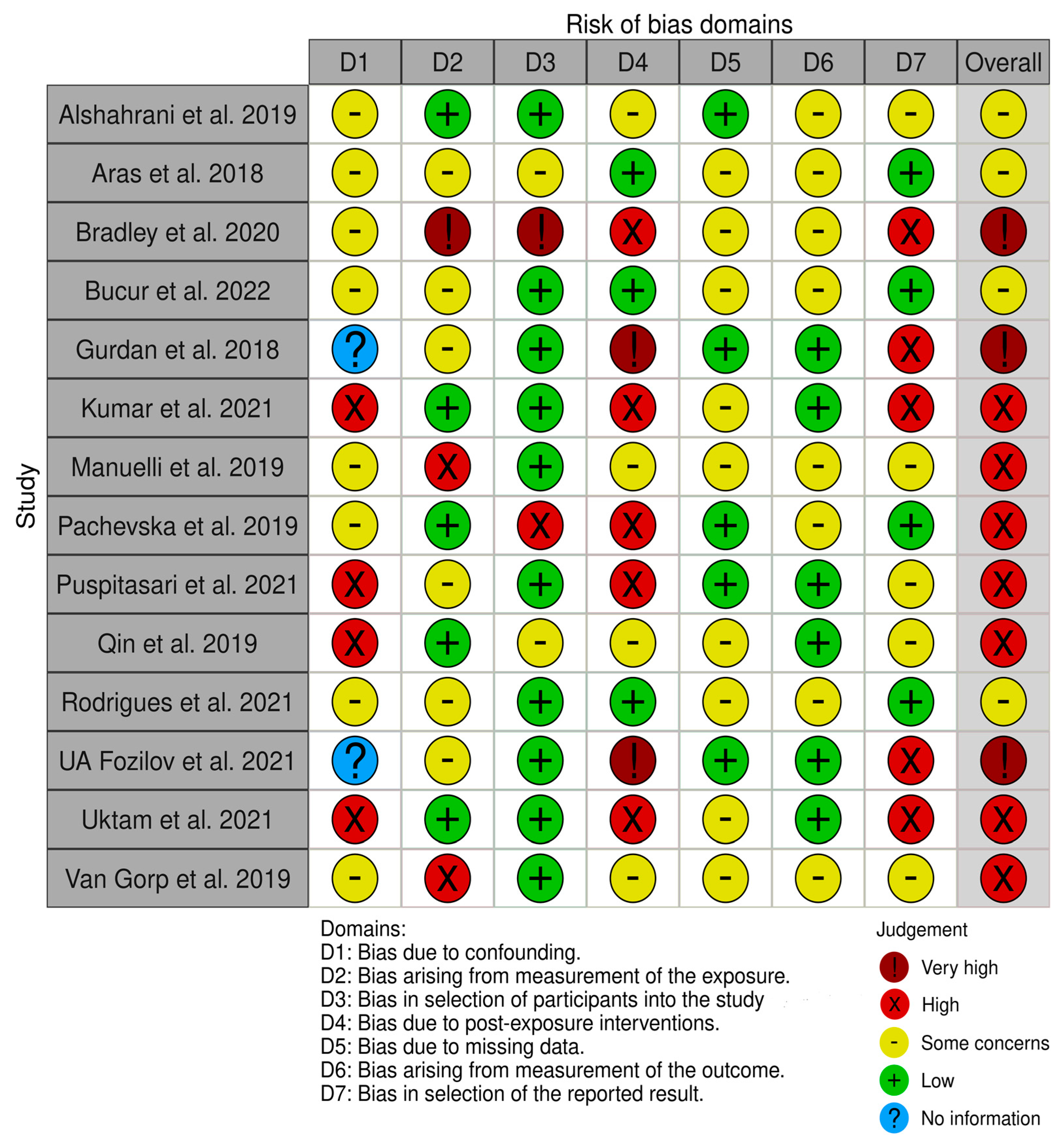
2.8. Risk of Bias Assessment



3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhang, M.; Mcgrath, C.; Hägg, U. The impact of malocclusion and its treatment on quality of life: A literature review. Int. J. Paediatr. Dent. 2006, 16, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Dab, S.; Chen, K.; Flores-Mir, C. Short- and long-term potential effects of accelerated osteogenic orthodontic treatment: A systematic review and meta-analysis. Orthod. Craniofacial Res. 2019, 22, 61–68. [Google Scholar] [CrossRef] [PubMed]
- NHS England. Guides for Commissioning Dental Specialties—Orthodontics. 2015. Available online: https://www.england.nhs.uk/commissioning/wp-content/uploads/sites/12/2015/09/guid-comms-orthodontics.pdf (accessed on 26 November 2022).
- Wang, X.; Bernabe, E.; Pitts, N.; Zheng, S.; Gallagher, J.E. Dental caries thresholds among adolescents in England, Wales, and Northern Ireland, 2013 at 12, and 15 years: Implications for epidemiology and clinical care. BMC Oral Health 2021, 21, 381–387. [Google Scholar] [CrossRef]
- Paes da Silva, S.; Pitchika, V.; Baumert, U.; Wehrbein, H.; Schwestka-Polly, R.; Drescher, D.; Kühnisch, J.; Wichelhaus, A. Oral health-related quality of life in orthodontics: A cross-sectional multicentre study on patients in orthodontic treatment. Eur. J. Orthod. 2019, 42, 270–280. [Google Scholar] [CrossRef] [PubMed]
- Kingsley, C.; Patel, S. Patient-reported outcome measures and patient-reported experience measures. BJA Educ. 2017, 17, 137–144. [Google Scholar] [CrossRef] [Green Version]
- Tsichlaki, A.; O’Brien, K. Do orthodontic research outcomes reflect patient values? A systematic review of randomized controlled trials involving children. Am. J. Orthod. Dentofac. Orthop. 2014, 146, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Lee, R.; Hwang, S.; Lim, H.; Cha, J.; Kim, K.; Chung, C.J. Treatment satisfaction and its influencing factors among adult orthodontic patients. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 808–817. [Google Scholar] [CrossRef]
- Pachêco-Pereira, C.; Pereira, J.R.; Dick, B.D.; Perez, A.; Flores-Mir, C. Factors associated with patient and parent satisfaction after orthodontic treatment: A systematic review. Am. J. Orthod. Dentofac. Orthop. 2015, 148, 652–659. [Google Scholar] [CrossRef]
- Wong, L.; Ryan, F.S.; Christensen, L.R.; Cunningham, S.J. Factors influencing satisfaction with the process of orthodontic treatment in adult patients. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 362–370. [Google Scholar] [CrossRef]
- Hodson, M.; Andrew, S.; Michael Roberts, C. Towards an understanding of PREMS and PROMS in COPD. Breathe 2013, 9, 358–364. [Google Scholar] [CrossRef] [Green Version]
- Bescos, R.; Casas-Agustench, P.; Belfield, L.; Brookes, Z.; Gabaldón, T. Coronavirus disease 2019 (COVID-19): Emerging and future challenges for dental and oral medicine. J. Dent. Res. 2020, 99, 1113. [Google Scholar] [CrossRef] [PubMed]
- Ather, A.; Patel, B.; Ruparel, N.B.; Diogenes, A.; Hargreaves, K.M. Coronavirus disease 19 (COVID-19): Implications for clinical dental care. J. Endod. 2020, 46, 584–595. [Google Scholar] [CrossRef]
- Suri, S.; Vandersluis, Y.R.; Kochhar, A.S.; Bhasin, R.; Abdallah, M. Clinical orthodontic management during the COVID-19 pandemic. Angle Orthod. 2020, 90, 473–484. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alshahrani, I.; Hameed, M.S.; Syed, S.; Amanullah, M.; Togoo, R.A.; Kaleem, S. Changes in Essential Salivary Parameters in Patients Undergoing Fixed Orthodontic Treatment: A Longitudinal Study. Niger. J. Clin. Pract. 2019, 22, 707–712. [Google Scholar] [CrossRef]
- Aras, I.; Unal, I.; Huniler, G.; Aras, A. Root resorption due to orthodontic treatment using self-ligating and conventional brackets: A cone-beam computed tomography study. J. Orofac. Orthop. 2018, 79, 181–190. [Google Scholar] [CrossRef]
- Bradley, E.; Shelton, A.; Hodge, T.; Morris, D.; Bekker, H.; Fletcher, S.; Barber, S. Patient-reported experience and outcomes from orthodontic treatment. J. Orthod. 2020, 47, 107–115. [Google Scholar] [CrossRef]
- Bucur, S.M.; Iantovics, L.B.; Bud, A.; Bud, E.S.; Cocoș, D.I.; Vlasa, A. Retrospective study regarding orthodontic retention complications in clinical practice. Appl. Sci. 2022, 12, 273. [Google Scholar] [CrossRef]
- Gurdan, Z.; Szalma, J. Evaluation of the success and complication rates of self-drilling orthodontic mini-implants. Niger. J. Clin. Pract. 2018, 21, 546–552. [Google Scholar] [CrossRef]
- Kumar, V.; Singh, P.; Arora, V.K.; Kaur, S.; Sarin, S.; Singh, H. Assessment of Effect of Fixed Orthodontic Treatment on Gingival Health: An Observational Study. J. Pharm. Bioallied Sci. 2021, 13 (Suppl. 1), S425–S428. [Google Scholar] [CrossRef] [PubMed]
- Manuelli, M.; Marcolina, M.; Nardi, N.; Bertossi, D.; De Santis, D.; Ricciardi, G.; Luciano, U.; Nocini, R.; Mainardi, A.; Lissoni, A.; et al. Oral mucosal complications in orthodontic treatment. Minerva Dent. Oral Sci. 2019, 68, 84–88. [Google Scholar] [CrossRef] [PubMed]
- Pachevska, A.V.; Filimonov, Y.V.; Filimonov, V.Y.; Dudik, O.P.; Popova, O.I.; Drachuk, N.V.; Kasianenko, D.M.; Biloshitska, A.V.; Istoshyn, V.M. Clinical and laboratory assessment the levelsof oral hygiene, total protein, hydrogen sulfide and nitrogen metabolites in oral fluid in the development of inflammatory complications during orthodontic treatment of children. Wiadomości Lek. 2019, 72, 744–747. [Google Scholar] [CrossRef]
- Puspitasari, Y.; Utama, M.D.; Bachtiar, R.; Achmad, H.; Ilmianti; Yusrini, S.; Novawati, E.; Rusdi, F.J. The Influence of Fixed Orthodontic Treatment on Tooth Discoloration among Dental Students in Makassar, Indonesia. Ann. Rom. Soc. Cell Biol. 2021, 1, 10720–10728. Available online: https://www.annalsofrscb.ro/index.php/journal/article/view/3844 (accessed on 26 November 2022).
- Qin, F.; Zhou, Y. The influence of bracket type on the external apical root resorption in class I extraction patients—A retrospective study. BMC Oral Health 2019, 19, 53. [Google Scholar] [CrossRef]
- Rodigues, L.; Shilpa, J.; Bhushan, J.; Sameer, P.; Vikram, G. A questionnaire study to assess and evaluate the common gingival problems faced by patients undergoing fixed orthodontic treatment. IP Int. J. Maxillofac. Imaging 2021, 6, 101–107. [Google Scholar] [CrossRef]
- Fozilov, U.A. Diagnostics and prevention of the development of caries and its complications in children at orthodontic treatment. J. A Multidiscip. Peer Rev. J. 2021, 6, 276–280. Available online: https://repo.journalnx.com/index.php/nx/article/view/1079 (accessed on 26 November 2022).
- Uktam, A.F. Prevention of Caries Development During Orthodontic Treatment. World Bull. Soc. Sci. 2021, 3, 61–66. Available online: https://scholarexpress.net/index.php/wbss/article/view/172 (accessed on 26 November 2022).
- Von Gorp, G.; Naomi, B.; Ingrid, V.; Guy, W.; Declerck, D. Orthodontic treatment recommendation and expected adverse reactions in patients with a history of dental trauma: A survey among general dentists, paediatric dentists, and orthodontic specialists. Int. J. Paediatr. Dent. 2019, 30, 360–369. [Google Scholar] [CrossRef]
- Currell, S.D.; Liaw, A.; Blackmore Grant, P.D.; Esterman, A.; Nimmo, A. Orthodontic mechanotherapies and their influence on external root resorption: A systematic review. Am. J. Orthod. Dentofac. Orthop. 2019, 155, 313–329. [Google Scholar] [CrossRef]
- Yi, J.; Li, M.; Li, Y.; Li, X.; Zhao, Z. Root resorption during orthodontic treatment with self-ligating or conventional brackets: A systematic review and meta-analysis. BMC Oral Health 2016, 16, 125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alzahawi, K.; Færøvig, E.; Brudvik, P.; Bøe, O.E.; Mavragani, M. Root resorption after leveling with super-elastic and conventional steel arch wires: A prospective study. Prog. Orthod. 2014, 15, 35. [Google Scholar] [CrossRef] [Green Version]
- Roscoe, M.G.; Meira, J.B.; Cattaneo, P.M. Association of orthodontic force system and root resorption: A systematic review. Am. J. Orthod. Dentofac. Orthop. 2015, 147, 610–626. [Google Scholar] [CrossRef] [PubMed]
- Aldeeri, A.; Alhammad, L.; Alduham, A.; Ghassan, W.; Shafshak, S.; Fatani, E. Association of orthodontic clear Aligners with root resorption using three-dimension measurements: A systematic review. J. Contemp. Dent. Pract. 2018, 19, 1559–1565. [Google Scholar] [CrossRef] [Green Version]
- Fang, X.; Qi, R.; Liu, C. Root resorption in orthodontic treatment with clear aligners: A systematic review and meta-analysis. Orthod. Craniofacial Res. 2019, 22, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, V.; Mehta, S.; Gauthier, M.; Mu, J.; Kuo, C.; Nanda, R.; Yadav, S. Comparison of external apical root resorption with clear aligners and pre-adjusted edgewise appliances in non-extraction cases: A systematic review and meta-analysis. Eur. J. Orthod. 2020, 43, 15–24. [Google Scholar] [CrossRef]
- Alam, M.K.; Abutayyem, H.; Kanwal, B.A.L.; Shayeb, M. Future of Orthodontics—A Systematic Review and Meta-Analysis on the Emerging Trends in This Field. J. Clinical Medicine 2023, 12, 532. [Google Scholar] [CrossRef]
- Geiger, A.M.; Gorelick, L.; Gwinnett, A.J.; Benson, B.J. Reducing white spot lesions in orthodontic populations with fluoride rinsing. Am. J. Orthod. Dentofac. Orthop. 1992, 101, 403–407. [Google Scholar] [CrossRef]
- Genco, R.J. Current view of risk factors for periodontal diseases. J. Periodontol. 1996, 67, 1041–1049. [Google Scholar] [CrossRef]
- Gorelick, L.; Geiger, A.M.; Gwinnett, A. Incidence of white spot formation after bonding and banding. Am. J. Orthod. 1982, 81, 93–98. [Google Scholar] [CrossRef]
- Harris, E.F. Root resorption during orthodontic therapy. Semin. Orthod. 2000, 6, 183–194. [Google Scholar] [CrossRef]
- Hwang, J.Y.; Tee, C.H.; Huang, A.T.; Taft, L. Effectiveness of thera-bite wafers in reducing pain. J. Clin. Orthod. 1994, 28, 291–292. [Google Scholar]
- Ketcham, A.H. A progress report of an investigation of apical root resorption of vital permanent teeth. Int. J. Orthod. Oral Surg. Radiogr. 1929, 15, 310–328. [Google Scholar] [CrossRef]
- Killiany, D.M. Root resorption caused by orthodontic treatment: Review of literature from 1998 to 2001 for evidence. Prog. Orthod. 2002, 3, 2–5. [Google Scholar] [CrossRef]
- Kremenak, C.R.; Kinser, D.D.; Harman, H.A.; Menard, C.C.; Jakobsen, J.R. Orthodontic risk factors for temporomandibular disorders (TMD). I: Premolar extractions. Am. J. Orthod. Dentofac. Orthop. 1992, 101, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Kremenak, C.R.; Kinser, D.D.; Meicher, T.J.; Wright, G.R.; Harrison, S.D.; Ziaja, R.R.; Harman, H.A.; Ordahl, J.N.; Demro, J.G.; Menard, C.C.; et al. Orthodontics as a risk factor for temporomandibular disorders (TMD). II. Am. J. Orthod. Dentofac. Orthop. 1992, 101, 21–27. [Google Scholar] [CrossRef]
- Krishnan, V. Critical issues concerning root resorption: A contemporary review. World J. Orthod. 2005, 6, 30–40. [Google Scholar]
- Krishnan, V.; Davidovitch, Z. Biological mechanisms of tooth movements, 2nd edition. J. Indian Orthod. Soc. 2015, 49, 126. [Google Scholar] [CrossRef]
- Kvinnsland, S.; Heyeraas, K.; Øfjord, E.S. Effect of experimental tooth movement on periodontal and pulpal blood flow. Eur. J. Orthod. 1989, 11, 200–205. [Google Scholar] [CrossRef]
- Steen Law, S.L.; Southard, K.A.; Law, A.S.; Logan, H.L.; Jakobsen, J.R. An evaluation of preoperative ibuprofen for treatment of pain associated with orthodontic separator placement. Am. J. Orthod. Dentofac. Orthop. 2000, 118, 629–635. [Google Scholar] [CrossRef]
- Levander, E.; Malmgren, O.; Eliasson, S. Evaluation of root resorption in relation to two orthodontic treatment regimes. A clinical experimental study. Eur. J. Orthod. 1994, 16, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Levander, E. Early radiographic diagnosis of apical root resorption during orthodontic treatment: A study of maxillary incisors. Eur. J. Orthod. 1998, 20, 57–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lew, K.K. Attitudes and perceptions of adults towards orthodontic treatment in an Asian community. Community Dent. Oral Epidemiol. 1993, 21, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Linge, L.; Linge, B.O. Patient characteristics and treatment variables associated with apical root resorption during orthodontic treatment. Am. J. Orthod. Dentofac. Orthop. 1991, 99, 35–43. [Google Scholar] [CrossRef]
- Malmgren, O.; Goldson, L.; Hill, C.; Orwin, A.; Petrini, L.; Lundberg, M. Root resorption after orthodontic treatment of traumatized teeth. Am. J. Orthod. 1982, 82, 487–491. [Google Scholar] [CrossRef] [PubMed]
- Mirabella, A.; Årtun, J. Risk factors for apical root resorption of maxillary anterior teeth in adult orthodontic patients. Am. J. Orthod. Dentofac. Orthop. 1995, 108, 48–55. [Google Scholar] [CrossRef]
- Mohlin, B.; Axelsson, S.; Paulin, G.; Pietilä, T.; Bondemark, L.; Brattström, V.; Hansen, K.; Holm, A. TMD in relation to Malocclusion and orthodontic treatment. Angle Orthod. 2007, 77, 542–548. [Google Scholar] [CrossRef]
- Ngan, P.; Kess, B.; Wilson, S. Perception of discomfort by patients undergoing orthodontic treatment. Am. J. Orthod. Dentofac. Orthop. 1989, 96, 47–53. [Google Scholar] [CrossRef]
- Ngan, P.; Wilson, S.; Shanfeld, J.; Amini, H. The effect of ibuprofen on the level of discomfort inpatients undergoing orthodontic treatment. Am. J. Orthod. Dentofac. Orthop. 1994, 106, 88–95. [Google Scholar] [CrossRef]
- Øgaard, B.; Rølla, G.; Arends, J. Orthodontic appliances and enamel demineralization. Am. J. Orthod. Dentofac. Orthop. 1988, 94, 68–73. [Google Scholar] [CrossRef]
- Øgaard, B.; Rølla, G.; Arends, J.; Ten Cate, J. Orthodontic appliances and enamel demineralization Part 2. Prevention and treatment of lesions. Am. J. Orthod. Dentofac. Orthop. 1988, 94, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Osterberg, T.; Carlsson, G.E. Symptoms and signs of mandibular dysfunction in 70-year-old men and women in Gothenburg, Sweden. Community Dent. Oral Epidemiol. 1979, 7, 315–321. [Google Scholar] [CrossRef]
- Parker, W.S. Root resorption—Long-term outcome. Am. J. Orthod. Dentofac. Orthop. 1997, 112, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Lucchese, A.; Bonini, C.; Noviello, M.; Lupo Stanghellini, M.T.; Greco, R.; Peccatori, J.; Biella, A.; Tassi, E.; Beretta, V.; Ciceri, F.; et al. The Effect of Removable Orthodontic Appliances on Oral Microbiota: A Systematic Review. Appl. Sci. 2021, 11, 2881. [Google Scholar] [CrossRef]
- Li, X.; Tang, Y.; Chen, Y. Interventions for pain during fixed orthodontic appliance therapy. Angle Orthod. 2010, 80, 925–932. [Google Scholar] [CrossRef]
- Polat, Ö. Pain and discomfort after orthodontic appointments. Semin. Orthod. 2007, 13, 292–300. [Google Scholar] [CrossRef]
- Pullinger, A.G.; Seligman, D.A.; Solberg, W.K. Temporomandibular disorders. Part I: Functional status, dentomorphologic features, and sex differences in a nonpatient population. J. Prosthet. Dent. 1988, 59, 228–235. [Google Scholar] [CrossRef]
- Pullinger, A.; Seligman, D.; Gornbein, J. A multiple logistic regression analysis of the risk and relative odds of Temporomandibular disorders as a function of common occlusal features. J. Dent. Res. 1993, 72, 968–979. [Google Scholar] [CrossRef]
- Rendell, J.K.; Norton, L.A.; Gay, T. Orthodontic treatment and temporomandibular joint disorders. Am. J. Orthod. Dentofac. Orthop. 1992, 101, 84–87. [Google Scholar] [CrossRef]
- Sadowsky, C.; BeGole, E.A. Long-term status of temporomandibular joint function and functional occlusion after orthodontic treatment. Am. J. Orthod. 1980, 78, 201–212. [Google Scholar] [CrossRef]
- Priti, M.; Adinegara, A.; Laxminarayan, K.; Raffaella, C.; Palna, K. Treatment of dental and orthodontic complications in thalassaemia. Cochrane Database Syst. Rev. 2023, 1, 1–10. [Google Scholar] [CrossRef]
- Ma, Z.; Zhu, Y.; Zhan, Y.; Zhang, Y.; Abdelrehem, A.; Wang, B.; Yang, C. Periosteum coverage versus collagen-membrane coverage in periodontally accelerated osteogenic orthodontics: A randomized controlled clinical trial in class II and class III malocclusions. BMC Oral Health 2022, 22. [Google Scholar] [CrossRef] [PubMed]
- Van, T.; Soyeon, K.; Jaeheon, K.; Joo, L.; Young-Seok, P. Revisiting the Complications of Orthodontic Miniscrew. BioMed Res. Int. 2022, 2022, 8720412. [Google Scholar] [CrossRef]
- Michele, I.A.; Giuseppina, M.; Stefania, C.; Maria, F.; Pasquale, A.; Merigrazia, C.; Fabio, P.; Assunta, P.; Irene, F.; Chiara, P.; et al. Tooth Complications after Orthodontic Miniscrews Insertion. Int. J. Environ. Res. Public Health 2023, 20, 1562. [Google Scholar] [CrossRef]
- Chaniotis, A.; Chanioti, A. Long-term complications of previously successful regenerative endodontic procedures after orthodontic movement: A report of 3 different complications after 4, 8, and 11 years. J. Endod. 2022, 48, 951–960. [Google Scholar] [CrossRef] [PubMed]
- Montasser, M.A.; Scribante, A. Root injury during Interradicular insertion is the most common complication associated with orthodontic Miniscrews. J. Evid. Based Dent. Pract. 2022, 22, 101688. [Google Scholar] [CrossRef] [PubMed]
- Rahimipour, K.; Mousavi, R.; Behnaz, M.; Dalaie, K.; Farahnaki, A.; Davoodi, N.S. Invisalign orthodontic system: Treatment efficacy, complications, patients’ attitude. Orthod. Forum 2020, 15, 108–123. [Google Scholar] [CrossRef]
- Habegger, M.; Renkema, A.; Bronkhorst, E.; Fudalej, P.S.; Katsaros, C. A survey of general dentists regarding orthodontic retention procedures. Eur. J. Orthod. 2016, 39, 69–75. [Google Scholar] [CrossRef] [Green Version]
- Chambers, D.W.; Zitterkopf, J.G. How people make decisions about whether or not to seek orthodontic care: Upstream in the treatment chain. Am. J. Orthod. Dentofac. Orthop. 2019, 155, 826–831. [Google Scholar] [CrossRef]
- Kučera, J.; Littlewood, S.J.; Marek, I. Fixed retention: Pitfalls and complications. Br. Dent. J. 2021, 230, 703–708. [Google Scholar] [CrossRef]
- Akbari, M.; Prabhu, R.; Khanna, S.; Turner, M.D. Resident commentary: Is there a significant difference in relapse and complication rate of surgically assisted rapid palatal expansion using tooth-borne, bone-borne, and orthodontic mini-implant-Borne appliances (Ploder et al, 2020)? J. Oral Maxillofac. Surg. 2021, 79, e1–e3. [Google Scholar] [CrossRef] [PubMed]
- Van Gorp, G.; Bormans, N.; Vanham, I.; Willems, G.; Declerck, D. Knowledge of orthodontic treatment approach of traumatized teeth by a group of Belgian general dentists, pediatric dentists, and orthodontists. Dent. Traumatol. 2019, 35, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Padmos, J.A.; Fudalej, P.S.; Renkema, A.M. Epidemiologic study of orthodontic retention procedures. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 496–504. [Google Scholar] [CrossRef]
- Mohaghegh, S.; Soleimani, M.; Kouhestani, F.; Motamedian, S.R. The effect of single/multiple micro-osteoperforation on the rate of orthodontic tooth movement and its possible complications: A systematic review and meta-analysis. Int. Orthod. 2021, 19, 183–196. [Google Scholar] [CrossRef] [PubMed]
- Alencar, L.B.; Sousa, S.C.; Silva, I.L.; Araújo, V.F.; Oliveira, E.B.; Fonseca-Filho, D.T.; Macena, M.C.; Fonseca, F.R. Allergic reactions in orthodontic patients: A review. Int. J. Odontostomatol. 2021, 15, 132–136. [Google Scholar] [CrossRef]
- Madurantakam, P.; Kumar, S. Are there more adverse effects with lingual orthodontics? Evid.-Based Dent. 2017, 18, 101–102. [Google Scholar] [CrossRef]
- Šimunović, L.; Blagec, T.; Vrankić, A.; Meštrović, S. Color Stability of Orthodontic Ceramic Brackets and Adhesives in Potentially Staining Beverages—In Vitro Study. Dent. J. 2022, 10, 115. [Google Scholar] [CrossRef]
- Yap, J. Measuring what really matters—Revisiting health system performance measurement. Int. J. Integr. Care 2022, 22, 108. [Google Scholar] [CrossRef]
- Yong, J.; Gröger, S.; Von Bremen, J.; Meyle, J.; Ruf, S. PD-L1, a potential Immunomodulator linking immunology and Orthodontically induced inflammatory root resorption (OIIRR): Friend or foe? Int. J. Mol. Sci. 2022, 23, 11405. [Google Scholar] [CrossRef]
- Msallam, F.A.; Grawish, M.E.; Hafez, A.M.; Abdelnaby, Y.L. Decalcification prevention around orthodontic brackets bonded to bleached enamel using different topical agents. Prog. Orthod. 2017, 18, 15. [Google Scholar] [CrossRef] [Green Version]
- Joss-Vassalli, I.; Grebenstein, C.; Topouzelis, N.; Sculean, A.; Katsaros, C. Orthodontic therapy and gingival recession: A systematic review. Orthod. Craniofacial Res. 2010, 13, 127–141. [Google Scholar] [CrossRef] [PubMed]
- Gokce, G. Complications and risks of orthodontic treatment. Dent. Med. J. Rev. 2021, 3, 38–51. Available online: https://dergipark.org.tr/tr/pub/dmj/issue/63407/910688 (accessed on 26 November 2022).
- Wishney, M. Potential risks of orthodontic therapy: A critical review and conceptual framework. Aust. Dent. J. 2017, 62, 86–96. [Google Scholar] [CrossRef] [Green Version]
- Kurniawan, F.K.; Roestamadji, R.I.; Takahashi, N.; Tedjosasongko, U.; Narmada, I.B.; Surboyo, M.D.; Diyatri, I. Oral microbiome profiles and inflammation in pregnant women who used orthodontic appliances. Dent. J. 2022, 10, 118. [Google Scholar] [CrossRef]
- Perkowski, K.; Baltaza, W.; Conn, D.B.; Marczyńska-Stolarek, M.; Chomicz, L. Examination of oral biofilm microbiota in patients using fixed orthodontic appliances in order to prevent risk factors for health complications. Ann. Agric. Environ. Med. 2019, 26, 231–235. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID | Target Group Size | Mean Age and Male: Female Ratio | Protocol of the Study | Objectives of the Paper | Inference from the Article |
|---|---|---|---|---|---|
| Alshahrani et al., 2019 [17] | 60 patients | 21.7 years | Retrospective study | This study sought to assess how the key salivary parameters of patients receiving fixed orthodontic treatment were affected; 60 patients had saliva samples taken both before and two months after starting fixed orthodontic treatment. | The introduction of orthodontic appliances changed the properties of saliva in the oral cavity, as shown in this study by significant changes in salivary flow rate, pH, buffering capacity, and total protein concentration, as well as amylase, calcium, and glucose levels, before and after treatment started. |
| Aras et al., 2018 [18] | 32 subjects | - | Comparative study | The goal of this study was to use cone beam computed tomography to volumetrically assess external root resorption (ERR) caused by orthodontic treatment in maxillary incisors, utilizing self-ligating brackets or conventional brackets. | Although there were significant differences in root volume between the two groups, there was no difference in ERR between the groups. Similar volume reduction was seen in the central and lateral incisors of the maxilla. |
| Bradley et al., 2020 [19] | 203 subjects | 12+ years; 68:130 | Cross-sectional survey | This study’s objective was to evaluate how orthodontic treatment affected patients’ perceptions of their pre-treatment anxieties, their treatment experiences, and their treatment results. | Alignment (89%) and being ashamed to grin (63) were the most often expressed pre-treatment worries. The most often expressed hopes for orthodontic treatment were increased self-assurance when eating (87%) and smiling (72%) in public, improved dental health (85%), and a decrease in bullying/teasing (63%). The three most often reported problems were gingivitis (39%), sore mouth (68%), and fixed appliance breakage (61%). |
| Bucur et al., 2022 [20] | 116 adult patients | 18.3–27.6 years; 38.79:61.21 | Retrospective study | A total of 116 adult patients wearing various kinds of orthodontic retainers were included in this retrospective analysis. The Quigley-Hein plaque index and the Navy plaque index, both modified by Turesky and Rustogi, were utilized by the authors to calculate the accumulation of dental plaque on a quantitative basis. | It was revealed that plaque accumulation was much lower in the case of mobile retainer wearers than fixed retainer users. When fixed retainers were used, periodontal recessions occurred more frequently. |
| Gurdan et al., 2018 [21] | 59 patients | Age not clearly defined; 25.4:74.6 | Retrospective study | This study aimed to calculate the success and complication rates of orthodontic mini-implants. | In this study, the success rate of the orthodontic mini-implants was 89.8%, and the typical loading time was 8.1 months. Infections of the soft tissues occurred in 6.3% to 33.3% of patients, whereas screw mobility occurred in 3.1% to 20.8% of cases, depending on the anatomic placement. |
| Kumar et al., 2021 [22] | 120 patients | 14.6 years; 47:73 | Observational study | The goal of this study was to evaluate the impact of fixed orthodontic therapy on gingival health. All patients’ full medical histories were documented. | Before and after treatment, the mean visible plaque values were found to be 3.11 and 5.81, respectively. Before and after therapy, the mean visible inflammation values were found to be 2.89 and 15.43, respectively. Before and after treatment, the mean gingival recession score values were reported to be 0.19 and 0.383, respectively. |
| Manuelli et al., 2019 [23] | 100 patients | - | Observational study | The goal of this research was to evaluate the effects of fixed orthodontic devices on soft tissue, bone, and tooth lesions. For this purpose, 100 participants with fixed orthodontic appliances were included in the research. | Regarding RPE, palatal lesions were reversible in 35% of patients, while tongue impressions were caused by the device in 45% of patients. Five percent of the individuals had tooth lesions and periodontal issues (i.e., dental caries). White spot lesions (WSL) and dental decay affected 15% of the participants; periodontal disease affected 10% of those using the Forsus appliance; and cheek mucosal lesions affected 20% of the patients. |
| Pachevska et al., 2019 [24] | 100 children | 9–15 years; NA | Randomized control trial | On the basis studying clinical and biochemical indicators, the purpose of this research was to improve the efficacy of prevention of inflammatory complications in the provision of orthodontic care to children with dentomaxillary abnormalities using non-removable orthodontic devices. | The usage of non-removable orthodontic appliances caused oral cavity irritation. The oral fluid’s levels of total protein, hydrogen sulfide, and nitrogen metabolites increased along with the decline in oral hygiene. |
| Puspitasari et al., 2021 [25] | 23 samples | - | Observational study | In Makassar, Indonesia, dental students participated in this study to learn more about how fixed orthodontic therapy affects tooth discoloration. | In this study, 2 samples (8.7%) and 12 samples (52.2%), respectively, showed discoloration degrees of 1 and 2; 10 samples (66.7%) of the 15 samples with treatment durations longer than 12 months had deterioration degrees of 1; and 2 samples (13.3%) had discoloration degrees 2. In contrast, 6 (75%) of the 8 samples with a treatment period of less than 12 months had discoloration of degree 0, while 2 (25%) had discoloration of degree 1. |
| Qin et al., 2019 [26] | 98 patients | 15.18 years; 51:47 | Retrospective study | This study sought to determine whether traditional and passive self-ligating braces had any impact on the quantity and intensity of external apical root resorption (EARR) in patients undergoing withdrawal. | Between the two groups, there was no discernible variation in the amount of EARR. Age and gender did not correslate with EARR; however, EARR did positively correlate with the length of the treatment. In the end, in class I extraction patients, the kind of bracket had no bearing on the occurrence or intensity of the external apical root resorption. |
| Rodrigues et al., 2021 [27] | 148 subjects | 14–35 years; 20.7:79.3 | Questionnaire-based study | This questionnaire study was conducted to evaluate the typical gingival issues experienced by patients receiving fixed orthodontic treatment. | According to this study, the vast majority of patients in both groups were cautious about keeping up proper oral hygiene. Occasionally itchy, painful, and swollen gums, or bleeding gums, were also reported by a small number of patients in both therapy groups. |
| UA Fozilov et al., 2021 [28] | 201 children | 7–18 years; 48.3:51.7 | Cross-sectional study | The major goal of this article was to make it easier to diagnose caries and associated problems during orthodontic treatment, and to prevent them from happening in the first place. | Children receiving orthodontic care exhibited elevated phosphorus levels, despite a tendency for calcium levels to drop, and normal pH levels. The evaluation of oral hygiene in the control groups based on the OHI-S and RNR indices was inadequate and went beyond the baseline indicators. |
| Uktam et al., 2021 [29] | 201 patients | 7–15 years; 48.3:51.7 | Cross-sectional study | This study’s objective was to enhance the detection and mitigation of caries and related consequences during orthodontic treatment. | Prior to receiving orthodontic treatments, all patients who had exams exhibited poor oral hygiene, as well as a lack of drive to practice good oral hygiene and prevent dental illnesses. Manual oral care skills were good in 12% of patients at greater risk of dental caries, but unsatisfactory in 67%. According to the OHI-S index, the sanitary conditions in the preventative subgroups were satisfactory at the end of the study. |
| Van Gorp et al., 2019 [30] | 267 dentists | NA; 30.23:69.24 | Questionnaire-based study | The goal of this study was to assess dental professionals’ understanding of this subject. In Flanders, general dentists, pediatric dentists, and orthodontists participated in a questionnaire survey (Belgium). | The most common adverse reaction in cases of ankylosis was noted to be difficulty in moving the tooth during orthodontic treatment. Tooth discoloration and apical root resorption were the two most commonly noted adverse reactions in cases with pulp and root canal obliteration. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alam, M.K.; Kanwal, B.; Abutayyem, H.; Alswairki, H.J.; Alfawzan, A.A.; Shqaidef, A.; Almakrami, L.H.; Alaqidi, S.F.S.; Alaskar, A.A.; Almutairi, I.A.; et al. Complications Arising Due to Orthodontic Treatment—A Systematic Review and Meta-Analysis. Appl. Sci. 2023, 13, 4035. https://doi.org/10.3390/app13064035
Alam MK, Kanwal B, Abutayyem H, Alswairki HJ, Alfawzan AA, Shqaidef A, Almakrami LH, Alaqidi SFS, Alaskar AA, Almutairi IA, et al. Complications Arising Due to Orthodontic Treatment—A Systematic Review and Meta-Analysis. Applied Sciences. 2023; 13(6):4035. https://doi.org/10.3390/app13064035
Chicago/Turabian StyleAlam, Mohammad Khursheed, Bushra Kanwal, Huda Abutayyem, Haytham Jamil Alswairki, Ahmed Ali Alfawzan, Abedalrahman Shqaidef, Laila Hamad Almakrami, Sultan Fadhel Shuaibi Alaqidi, Almothana Ali Alaskar, Ibrahim Ayiz Almutairi, and et al. 2023. "Complications Arising Due to Orthodontic Treatment—A Systematic Review and Meta-Analysis" Applied Sciences 13, no. 6: 4035. https://doi.org/10.3390/app13064035