
Deep-Learning Algorithms for Prescribing Insoles to Patients with Foot Pain
 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Population
2.2. Input Variables
Resting Calcaneal Stance Position
2.3. Pelvic Elevation, Pelvic Tilt, and Pelvic Rotation
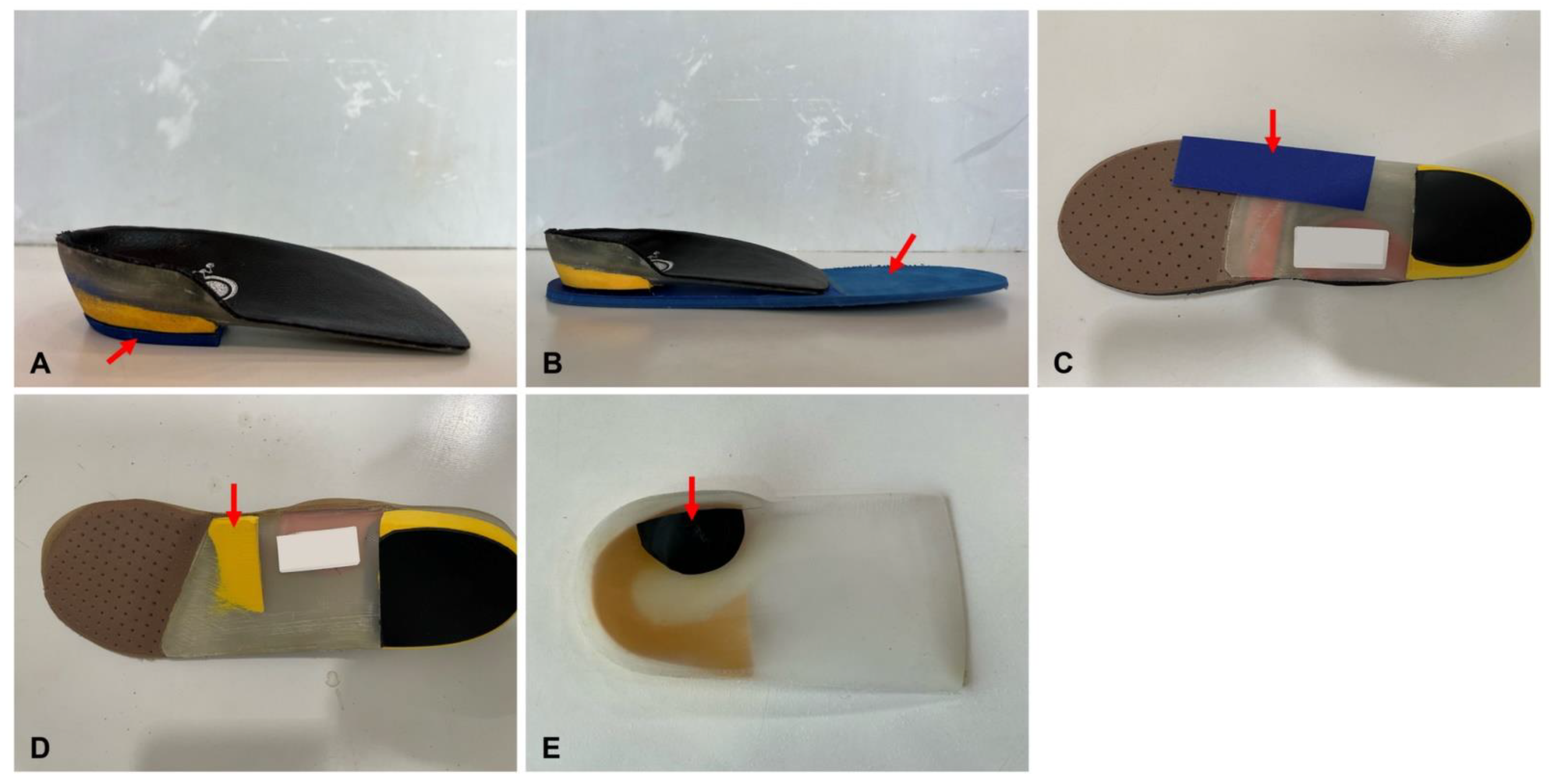
2.4. Target Variables
2.5. Deep-Learning Algorithms
3. Statistical Analysis
4. Results
5. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Choo, Y.J.; Park, C.H.; Chang, M.C. Rearfoot disorders and conservative treatment: A narrative review. Ann. Palliat. Med. 2020, 9, 3546–3552. [Google Scholar]
- Park, C.H.; Chang, M.C. Forefoot disorders and conservative treatment. Yeungnam Univ. J. Med. 2019, 36, 92–98. [Google Scholar] [CrossRef]
- Alqahtani, T.A. The prevalence of foot pain and its associated factors among Saudi school teachers in Abha sector, Saudi Arabia. Family Med Prim Care. 2020, 9, 4641–4647. [Google Scholar]
- Chang, M.C. The blind spot and challenges in pain management. J. Yeungnam Med. Sci. 2022, 39, 179–180. [Google Scholar]
- Park, C.H.; Boudier-Revéret, M.; Chang, M.C. Tarsal tunnel syndrome due to talocalcaneal coalition. Yeungnam Univ. J. Med. 2023, 40, 106–108. [Google Scholar] [CrossRef]
- Chow, T.H.; Chen, Y.S.; Hsu, C.C. Relationships between Plantar Pressure Distribution and Rearfoot Alignment in the Taiwanese College Athletes with Plantar Fasciopathy during Static Standing and Walking. Int. J. Environ. Res. Public Health 2021, 18, 12942. [Google Scholar]
- Menz, H.B.; Dufour, A.B.; Riskowski, J.L.; Hillstrom, H.J.; Hannan, M.T. Association of planus foot posture and pronated foot function are associated with foot pain: The Framingham foot study. Arthritis Care Res. 2013, 65, 1991–1999. [Google Scholar]
- Elattar, O.; Smith, T.; Ferguson, A.; Farber, D.; Wapner, K. Uses of Braces and Orthotics for Conservative Management of Foot and Ankle Disorders. Foot Ankle Orthop. 2018, 3, 2473011418780700. [Google Scholar] [CrossRef]
- Razeghi, M.; Batt, M.E. Biomechanical analysis of the effect of orthotic shoe inserts: A review of the literature. Sports Med. 2000, 29, 425–438. [Google Scholar] [CrossRef]
- Amer, A.O.; Jarl, G.M.; Hermansson, L.N. The effect of insoles on foot pain and daily activities. Prosthet. Orthot. Int. 2014, 38, 474–480. [Google Scholar]
- Gómez Carrión, Á.; Atín Arratibe, M.L.Á.; Morales Lozano, M.R.; Martínez Rincón, C.; Martínez Sebastián, C.; Saura Sempere, Á.; Nuñez-Fernandez, A.; Sánchez-Gómez, R. Changes in the Kinematics of Midfoot and Rearfoot Joints with the Use of Lateral Wedge Insoles. J. Clin. Med. 2022, 11, 4536. [Google Scholar]
- Paterson, K.L.; Hinman, R.S.; Metcalf, B.R.; McManus, F.; Jones, S.E.; Menz, H.B.; Munteanu, S.E.; Bennell, K.L. Effect of foot orthoses vs sham insoles on first metatarsophalangeal joint osteoarthritis symptoms: A randomized controlled trial. Osteoarthr. Cartil. 2022, 30, 956–964. [Google Scholar]
- Khamis, S.; Dar, G.; Peretz, C.; Yizhar, Z. The Relationship Between Foot and Pelvic Alignment While Standing. J. Hum. Kinet. 2015, 46, 85–97. [Google Scholar] [CrossRef]
- Fukuchi, C.A.; Lewinson, R.T.; Worobets, J.T.; Stefanyshyn, D.J. Effects of Lateral and Medial Wedged Insoles on Knee and Ankle Internal Joint Moments During Walking in Healthy Men. J. Am. Podiatr. Med. Assoc. 2016, 106, 411–418. [Google Scholar] [CrossRef]
- Kerrigan, D.C.; Lelas, J.L.; Goggins, J.; Merriman, G.J.; Kaplan, R.J.; Felson, D.T. Effectiveness of a lateral-wedge insole on knee varus torque in patients with knee osteoarthritis. Arch. Phys. Med. Rehabil. 2002, 83, 889–893. [Google Scholar]
- Mahmoud, A.; Abundo, P.; Basile, L.; Albensi, C.; Marasco, M.; Bellizzi, L.; Galasso, F.; Foti, C. Functional leg length discrepancy between theories and reliable instrumental assessment: A study about newly invented NPoS system. Muscles Ligaments Tendons J. 2017, 7, 293–305. [Google Scholar]
- Choo, Y.J.; Kim, J.K.; Kim, J.H.; Chang, M.C.; Park, D. Machine learning analysis to predict the need for ankle foot orthosis in patients with stroke. Sci. Rep. 2021, 11, 8499. [Google Scholar] [CrossRef]
- Kim, J.K.; Choo, Y.J.; Chang, M.C. Prediction of Motor Function in Stroke Patients Using Machine Learning Algorithm: Development of Practical Models. J. Stroke Cerebrovasc. Dis. 2021, 30, 105856. [Google Scholar]
- Kim, J.K.; Lv, Z.; Park, D.; Chang, M.C. Practical Machine Learning Model to Predict the Recovery of Motor Function in Patients with Stroke. Eur. Neurol. 2022, 85, 273–279. [Google Scholar]
- Kim, J.K.; Chang, M.C.; Park, D. Deep Learning Algorithm Trained on Brain Magnetic Resonance Images and Clinical Data to Predict Motor Outcomes of Patients With Corona Radiata Infarct. Front. Neurosci. 2022, 15, 795553. [Google Scholar]
- Shin, H.; Choi, G.S.; Shon, O.J.; Kim, G.B.; Chang, M.C. Development of convolutional neural network model for diagnosing meniscus tear using magnetic resonance image. BMC Musculoskelet. Disord. 2022, 23, 510. [Google Scholar] [CrossRef]
- Cho, Y.; Park, J.W.; Nam, K. The relationship between foot posture index and resting calcaneal stance position in elementary school students. Gait Posture 2019, 74, 142–147. [Google Scholar] [CrossRef]
- Keenan, A.M.; Bach, T.M. Clinicians’ assessment of the hindfoot: A study of reliability. Foot Ankle Int. 2006, 27, 451–460. [Google Scholar] [CrossRef]
- Kouhkan, S.; Rahimi, A.; Ghasemi, M.; Naimi, S.S.; Baghban, A.A. Postural Changes during First Pregnancy. Br. J. Med. Med. Res. 2015, 7, 744–753. [Google Scholar] [CrossRef]
- Wang, S.; Minku, L.L. AUC estimation and concept drift detection for imbalanced data streams with multiple classes. In Proceedings of the 2020 International Joint Conference on Neural Networks (IJCNN), Glasgow, UK, 19–24 July 2020; pp. 1–8. [Google Scholar]
- Mandrekar, J.N. Receiver operating characteristic curve in diagnostic test assessment. J. Thorac. Oncol. 2010, 5, 1315–1316. [Google Scholar] [CrossRef]
- Buchanan, K.R.; Davis, I. The relationship between forefoot, midfoot, and rearfoot static alignment in pain-free individuals. J. Orthop. Sports Phys. Ther. 2005, 35, 559–566. [Google Scholar]
- Kim, P.J.; Peace, R.; Mieras, J.; Thoms, T.; Freeman, D.; Page, J. Interrater and intrarater reliability in the measurement of ankle joint dorsiflexion is independent of examiner experience and technique used. J. Am. Podiatr. Med. Assoc. 2011, 101, 407–414. [Google Scholar]
- Menz, H.B. Foot orthoses: How much customisation is necessary? J Foot Ankle Res. 2009, 2, 23. [Google Scholar] [CrossRef]
- Severin, A.C.; Gean, R.P.; Barnes, S.G.; Queen, R.; Butler, R.J.; Martin, R.; Barnes, C.L.; Mannen, E.M. Effects of a corrective heel lift with an orthopaedic walking boot on joint mechanics and symmetry during gait. Gait Posture 2019, 73, 233–238. [Google Scholar]
- Yen, S.T.; Andrew, P.D.; Cummings, G.S. Short-term effect of correcting leg length discrepancy on performance of a forceful body extension task in young adults. Hiroshima J. Med. Sci. 1998, 47, 139–143. [Google Scholar]
- Kriegeskorte, N.; Golan, T. Neural network models and deep learning. Curr. Biol. 2019, 29, R231–R236. [Google Scholar]
- Sarker, I.H. Deep learning: A comprehensive overview on techniques, taxonomy, applications and research directions. SN Comput. Sci. 2021, 2, 420. [Google Scholar] [CrossRef]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar]
- Rajula, H.S.; Verlato, G.; Manchia, M.; Antonucci, N.; Fanos, V. Comparison of conventional statistical methods with machine learning in medicine: Diagnosis, drug development, and treatment. Medicina 2020, 56, 455. [Google Scholar] [CrossRef]
- Choo, Y.J.; Chang, M.C. Use of Machine Learning in Stroke Rehabilitation: A Narrative Review. Brain Neurorehabil. 2022, 15, e26. [Google Scholar]
- Lee, H.; Song, J. Introduction to convolutional neural network using Keras; an understanding from a statistician. Commun. Stat. Appl. Methods 2019, 26, 591–610. [Google Scholar] [CrossRef]
- Giulia, A.; Anna, S.; Antonia, B.; Dario, P.; Maurizio, C. Extending association rule mining to microbiome pattern analysis: Tools and guidelines to support real applications. Front. Bioinform. 2022, 1, 794547. [Google Scholar] [CrossRef]
- Mendez, K.M.; Pritchard, L.; Reinke, S.N.; Broadhurst, D.I. Toward collaborative open data science in metabolomics using Jupyter Notebooks and cloud computing. Metabolomics 2019, 15, 125. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Prescription Left DNN Regression Model | Prescription Right DNN Regression Model | |
|---|---|---|
| DNN model | - Four hidden layers with 256-128-128-64 neurons - RMSProp optimizer, ReLU activation - Learning rate 1 × 10−5, batch size 512 - Batch normalization for regularization | - Five hidden layers with 512-512-1024-1024-512 neurons - RMSProp optimizer, ReLU activation - Learning rate 2 × 10−3, batch size 512 - Batch normalization for regularization |
| Model performance | - MAE 1.460, RMSE 3.539 for training - MAE 1.408, RMSE 3.365 for validation | - MAE 1.560, RMSE 3.860 for training - MAE 1.601, RMSE 3.549 for validation |
| Sample size and ratio Sample class size and ratio | - 70% for training: 586; 30% for validation: 252; total: 838 - Class 0: 392 (66.9%), class 1: 64 (10.9%), class 2: 130 (22.2%) for training - Class 0: 169 (67.1%), class 1: 28 (11.1%), class 2: 55 (21.8%) for validation | |||||
| DNN model | - Five hidden layers with 512-512-1024-1024-512 neurons - Adam optimizer, ReLU activation - Learning rate 1 × 10−2 batch size 32 - Dropout layer for regularization - Training accuracy: 89.1%, validation accuracy: 89.7% | |||||
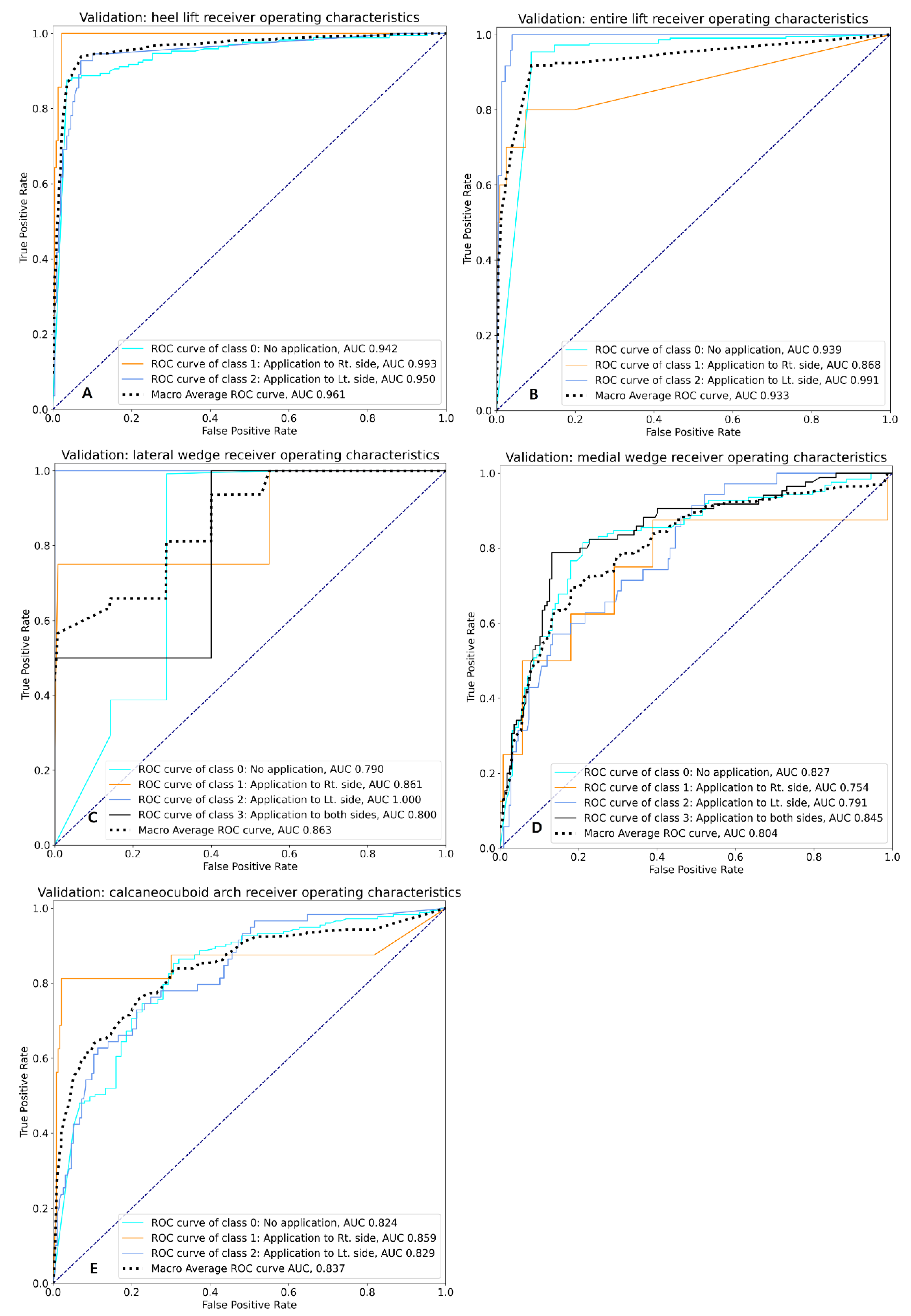
| Model performance (validation data) | Class | Precision | Recall | F1-score | Support | ROC AUC |
| 0 | 0.961 | 0.882 | 0.920 | 169 | 0.942 | |
| 1 | 0.839 | 0.939 | 0.881 | 28 | 0.993 | |
| 2 | 0.773 | 0.927 | 0.843 | 55 | 0.950 | |
| Macro average | 0.858 | 0.913 | 0.881 | 252 | 0.961 | |
| Micro average | 0.907 | 0.897 | 0.899 | 252 | 0.949 | |
| Sample size and ratio Sample class size and ratio | - 70% for training: 586; 30% for validation: 252; total: 838 - Class 0: 508 (86.7%), class 1: 23 (3.9%), class 2: 55 (9.4%) for training - Class 0: 218 (86.5%), class 1: 10 (4%), class 2: 24 (9.5%) for validation | |||||
| DNN model | - Three hidden layers with 256-256-512 neurons - RMSProp optimizer, ReLU activation - Learning rate 5 × 10−3, batch size 2 - Dropout layer for regularization - Training accuracy: 94.7%, validation accuracy: 94.8% | |||||
| Model performance (validation data) | Class | Precision | Recall | F1-score | Support | ROC AUC |
| 0 | 0.977 | 0.968 | 0.972 | 218 | 0.939 | |
| 1 | 0.750 | 0.600 | 0.667 | 10 | 0.868 | |
| 2 | 0.786 | 0.917 | 0.846 | 24 | 0.991 | |
| Macro average | 0.838 | 0.828 | 0.828 | 252 | 0.933 | |
| Micro average | 0.950 | 0.948 | 0.948 | 252 | 0.941 | |
| Sample size and ratio Sample class size and ratio | - 70% for training: 586; 30% for validation: 252; total: 838 - Class 0: 571 (97.4%), class 1: 9 (0.015%), class 2: 3 (0.005%), class 3: 3 (0.005%) for training - Class 0: 245 (97.2%), class 1: 4 (0.016%), class 2: 1 (0.004%), class 3: 2 (0.008%) for validation | |||||
| DNN model | - Two hidden layers with 256-1024 neurons - RMSProp optimizer, ReLU activation - Learning rate 5 × 10−4, batch size 128 - Dropout layer for regularization - Training accuracy: 98.8%, validation accuracy: 98.4% | |||||
| Model performance (validation data) | Class | Precision | Recall | F1-score | Support | ROC AUC |
| 0 | 0.988 | 0.996 | 0.992 | 245 | 0.790 | |
| 1 | 0.667 | 0.500 | 0.571 | 4 | 0.861 | |
| 2 | 1.000 | 1.000 | 1.000 | 1 | 1.000 | |
| 3 | 1.000 | 0.500 | 0.667 | 2 | 0.800 | |
| Macro average | 0.914 | 0.749 | 0.807 | 252 | 0.863 | |
| Micro average | 0.983 | 0.984 | 0.983 | 252 | 0.792 | |
| Sample size and ratio Sample class size and ratio | - 70% for training: 586; 30% for validation: 252; total: 838 - Class 0: 289 (49.3%), class 1: 19 (3.2%), class 2: 80 (13.7%), class 3: 198 (33.8%) for training - Class 0: 124 (49.2%), class 1: 8 (3.2%), class 2: 35 (13.9%), class 3: 85 (33.7%) for validation | |||||
| DNN model | - Two hidden layers with 256-1024 neurons - Nadam optimizer, ReLU activation - Learning rate 5 × 10−5, batch size 64 - Dropout layer for regularization - Training accuracy: 93.0%, validation accuracy: 72.2% | |||||
| Model performance (validation data) | Class | Precision | Recall | F1-score | Support | ROC AUC |
| 0 | 0.786 | 0.798 | 0.792 | 124 | 0.827 | |
| 1 | 0.333 | 0.250 | 0.285 | 8 | 0.754 | |
| 2 | 0.455 | 0.429 | 0.441 | 35 | 0.791 | |
| 3 | 0.759 | 0.776 | 0.767 | 85 | 0.845 | |
| Macro average | 0.583 | 0.583 | 0.572 | 252 | 0.804 | |
| Micro average | 0.716 | 0.722 | 0.719 | 252 | 0.826 | |
| Sample size and ratio Sample class size and ratio | - 70% for training: 586; 30% for validation: 252; total: 838 - Class 0: 412 (70.3%), class 1: 36 (6.1%), class 2: 138 (23.6%) for training - Class 0: 177 (70.2%), class 1: 16 (6.4%), class 2: 59 (23.4%) for validation | |||||
| DNN model | - Four hidden layers with 1024-512-256-128 neurons - RMSProp optimizer, ReLU activation - Learning rate 2 × 10−3, batch size 128 - Dropout layer for regularization - Training accuracy: 88.7%, validation accuracy: 79.8% | |||||
| Model performance (validation data) | Class | Precision | Recall | F1-score | Support | ROC AUC |
| 0 | 0.868 | 0.853 | 0.860 | 177 | 0.824 | |
| 1 | 0.684 | 0.812 | 0.743 | 16 | 0.859 | |
| 2 | 0.627 | 0.627 | 0.627 | 59 | 0.828 | |
| Macro average | 0.726 | 0.764 | 0.743 | 252 | 0.837 | |
| Micro average | 0.800 | 0.798 | 0.798 | 252 | 0.827 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.K.; Choo, Y.J.; Park, I.S.; Choi, J.-W.; Park, D.; Chang, M.C. Deep-Learning Algorithms for Prescribing Insoles to Patients with Foot Pain. Appl. Sci. 2023, 13, 2208. https://doi.org/10.3390/app13042208
Kim JK, Choo YJ, Park IS, Choi J-W, Park D, Chang MC. Deep-Learning Algorithms for Prescribing Insoles to Patients with Foot Pain. Applied Sciences. 2023; 13(4):2208. https://doi.org/10.3390/app13042208
Chicago/Turabian StyleKim, Jeoung Kun, Yoo Jin Choo, In Sik Park, Jin-Woo Choi, Donghwi Park, and Min Cheol Chang. 2023. "Deep-Learning Algorithms for Prescribing Insoles to Patients with Foot Pain" Applied Sciences 13, no. 4: 2208. https://doi.org/10.3390/app13042208