
Endodontic Regenerative Procedures in Necrotic Adult Teeth

 , , , and
, , , and
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria: PICO Question
2.1.1. P-Population
2.1.2. O-Outcome
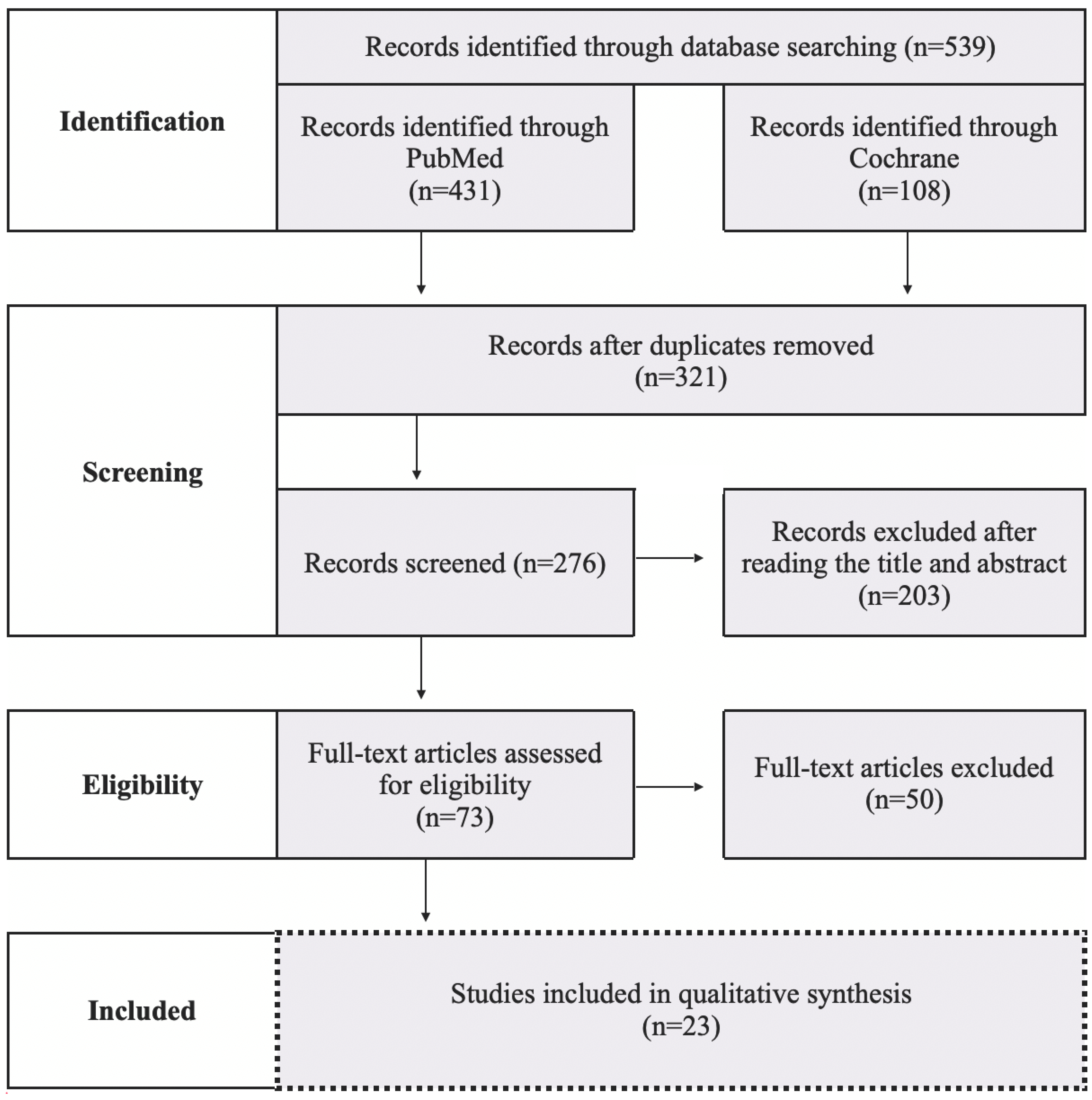
2.2. Search Strategy
2.3. Study Selection
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Association of Endodontists, Glossary of Endodontic Terms (Tenth Edition). Available online: https://www.aae.org/specialty/clinical-resources/glossary-endodontic-terms/ (accessed on 15 February 2021).
- Lopes, L.B.; Neves, J.A.; Botelho, J.; Machado, V.; Mendes, J.J. Regenerative Endodontic Procedures: An Umbrella Review. Int. J. Environ. Res. Public Health 2021, 18, 754. [Google Scholar] [CrossRef] [PubMed]
- American Association of Endodontics, Colleagues for Excellence Newsletter. Regenerative Endodontics. AAE. Available online: https://f3f142zs0k2w1kg84k5p9i1o-wpengine.netdna-ssl.com/specialty/wp-content/uploads/sites/2/2017/06/ecfespring2013.pdf (accessed on 13 April 2021).
- Galler, K.M.; Krastl, G.; Simon, S. European Society of Endodontology position statement: Revitalization procedures. Int. Endod. J. 2016, 49, 717–723. [Google Scholar] [CrossRef] [PubMed]
- Duggal, M.; Tong, H.J.; Al-Ansary, M. Interventions for the endodontic management of non-vital traumatised immature permanent anterior teeth in children and adolescents: A systematic review of the evidence and guidelines of the European Academy of Paediatric Dentistry. Eur. Arch. Paediatr. Dent. 2017, 18, 139–151. [Google Scholar] [CrossRef] [PubMed]
- Alghamdi, F.T.; Alqurashi, A.E. Regenerative Endodontic Therapy in the Management of Immature Necrotic Permanent Dentition: A Systematic Review. Sci. World J. 2020, 2020, 7954357. [Google Scholar] [CrossRef] [PubMed]
- Cabral, C.S.L.; Genizelli, L.O.; Cruz, R.G.Z. Tratamento de dentes com rizogênese incompleta após procedimentos regenerativos ou de apicificação: Uma revisão sistemática de literatura. Rev. Bras. Odontol. 2016, 73, 336–339. [Google Scholar] [CrossRef] [Green Version]
- Shamszadeh, S.; Asgary, S.; Nosrat, A. Regenerative Endodontics: A Scientometric and Bibliometric Analysis. J. Endod. 2019, 45, 272–280. [Google Scholar] [CrossRef]
- Tong, H.J.; Rajan, S.; Bhujel, N. Regenerative Endodontic Therapy in the Management of Nonvital Immature Permanent Teeth: A Systematic Review-Outcome Evaluation and Meta-analysis. J. Endod. 2017, 43, 1453–1464. [Google Scholar] [CrossRef]
- Torabinejad, M.; Nosrat, A.; Verma, P. Regenerative Endodontic Treatment or Mineral Trioxide Aggregate Apical Plug in Teeth with Necrotic Pulps and Open Apices: A Systematic Review and Meta-analysis. J. Endod. 2017, 43, 1806–1820. [Google Scholar] [CrossRef]
- Digka, A.; Sakka, D.; Lyroudia, K. Histological assessment of human regenerative endodontic procedures (REP) of immature permanent teeth with necrotic pulp/apical periodontitis: A systematic review. Aust. Endod. J. 2020, 46, 140–153. [Google Scholar] [CrossRef]
- Wilkström, A.; Brundin, M.; Lopes, M.F. What is the best long-term treatment modality for immature permanent teeth with pulp necrosis and apical periodontitis? Eur. Arch. Paediatr. Dent. 2021, 22, 311–340. [Google Scholar] [CrossRef]
- Ducret, M.; Costantini, A.; Gobert, S. Fibrin-based scaffolds for dental pulp regeneration: From biology to nanotherapeutics. Eur. Cell Mater. 2021, 41, 1–14. [Google Scholar] [CrossRef] [PubMed]
- He, L.; Zhong, J.; Gong, Q. Treatment of Necrotic Teeth by Apical Revascularization: Meta-analysis. Sci. Rep. 2017, 7, 13941. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tabassum, S.; Khan, F.R. Failure of endodontic treatment: The usual suspects. Eur. J. Dent. 2016, 10, 144–147. [Google Scholar] [CrossRef] [PubMed]
- Setzer, F.C.; Shah, S.B.; Kohli, M.R. Outcome of endodontic surgery: A meta-analysis of the literature--part 1: Comparison of traditional root-end surgery and endodontic microsurgery. J. Endod. 2010, 36, 1757–1765. [Google Scholar] [CrossRef] [PubMed]
- Imura, N.; Pinheiro, E.T.; Gomes, B.P. The outcome of endodontic treatment: A retrospective study of 2000 cases performed by a specialist. J. Endod. 2007, 33, 1278–1282. [Google Scholar] [CrossRef] [PubMed]
- Murray, P.E.; Garcia-Godoy, F.; Hargreaves, K.M. Regenerative endodontics: A review of current status and a call for action. J. Endod. 2007, 33, 377–390. [Google Scholar] [CrossRef]
- Hargreaves, K.M.; Giesler, T.; Henry, M. Regeneration potential of the young permanent tooth: What does the future hold? J. Endod. 2008, 34 (Suppl. S7), S51–S56. [Google Scholar] [CrossRef]
- Panda, S.; Mishra, L.; Arbildo-Vega, H.I. Effectiveness of Autologous Platelet Concentrates in Management of Young Immature Necrotic Permanent Teeth-A Systematic Review and Meta-Analysis. Cells 2020, 9, 2241. [Google Scholar] [CrossRef]
- Metlerska, J.; Fagogeni, I.; Nowicka, A. Efficacy of Autologous Platelet Concentrates in Regenerative Endodontic Treatment: A Systematic Review of Human Studies. J. Endod. 2019, 45, 20–30. [Google Scholar] [CrossRef]
- Meschi, N.; Castro, A.B.; Vandamme, K. The impact of autologous platelet concentrates on endodontic healing: A systematic review. Platelets 2016, 27, 613–633. [Google Scholar] [CrossRef]
- Lolato, A.; Bucchi, C.; Taschieri, S. Platelet concentrates for revitalization of immature necrotic teeth: A systematic review of the clinical studies. Platelets 2016, 27, 383–392. [Google Scholar] [CrossRef] [PubMed]
- Brau, C.; Aguadé, E. Tratamiento del diente con el ápice inmaduro. In Endodoncia: Técnicas Clinicas y Bases Cientificas, 3rd ed.; Elsevier: Barcelona, Spain, 2014; pp. 259–270. [Google Scholar]
- Lähteenvuo, J.; Rosenzweig, A. Effects of aging on angiogenesis. Circ. Res. 2012, 110, 1252–1264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morse, D.R. Age-related changes of the dental pulp complex and their relationship to systemic aging. Oral Surg. Oral Med. Oral Pathol. 1991, 72, 721–745. [Google Scholar] [CrossRef]
- Iezzi, I.; Pagella, P.; Mattioli-Belmonte, M. The effects of ageing on dental pulp stem cells, the tooth longevity elixir. Eur. Cell Mater. 2019, 37, 175–185. [Google Scholar] [CrossRef] [PubMed]
- Chrepa, V.; Henry, M.A.; Daniel, B.J. Delivery of Apical Mesenchymal Stem Cells into Root Canals of Mature Teeth. J. Dent. Res. 2015, 94, 1653–1659. [Google Scholar] [CrossRef]
- Estefan, B.S.; El Batouty, K.M.; Nagy, M.M. Influence of Age and Apical Diameter on the Success of Endodontic Regeneration Procedures. J. Endod. 2016, 42, 1620–1625. [Google Scholar] [CrossRef]
- Laureys, W.G.; Cuvelier, C.A.; Dermaut, L.R. The critical apical diameter to obtain regeneration of the pulp tissue after tooth transplantation, replantation, or regenerative endodontic treatment. J. Endod. 2013, 39, 759–763. [Google Scholar] [CrossRef]
- Chiego, D. Erupción y caída de los dientes. In Principios de Histología y Embriología Bucal, 4th ed.; Elsevier: Barcelona, Spain, 2014; pp. 77–91. [Google Scholar]
- Brizuela, C.; Meza, G.; Urrejola, D. Cell-Based Regenerative Endodontics for Treatment of Periapical Lesions: A Randomized, Controlled Phase I/II Clinical Trial. J. Dent. Res. 2020, 99, 523–529. [Google Scholar] [CrossRef]
- El-Kateb, N.M.; El-Backly, R.N.; Amin, W.M. Quantitative Assessment of Intracanal Regenerated Tissues after Regenerative Endodontic Procedures in Mature Teeth Using Magnetic Resonance Imaging: A Randomized Controlled Clinical Trial. J. Endod. 2020, 46, 563–574. [Google Scholar] [CrossRef]
- Arslan, H.; Ahmed, H.M.A.; Şahin, Y. Regenerative Endodontic Procedures in Necrotic Mature Teeth with Periapical Radiolucencies: A Preliminary Randomized Clinical Study. J. Endod. 2019, 45, 863–872. [Google Scholar] [CrossRef] [PubMed]
- Cordero, C.B.; Santander, G.M.; González, D.U. Allogeneic Cellular Therapy in a Mature Tooth with Apical Periodontitis and Accidental Root Perforation: A Case Report. J. Endod. 2020, 46, 1920–1927.e1. [Google Scholar] [CrossRef] [PubMed]
- Arslan, H.; Şahin, Y.; Topçuoğlu, H.S. Histologic Evaluation of Regenerated Tissues in the Pulp Spaces of Teeth with Mature Roots at the Time of the Regenerative Endodontic Procedures. J. Endod. 2019, 45, 1384–1389. [Google Scholar] [CrossRef] [PubMed]
- Nagas, E.; Uyanik, M.O.; Cehreli, Z.C. Revitalization of necrotic mature permanent incisors with apical periodontitis: A case report. Restor. Dent. Endod. 2018, 43, e31. [Google Scholar] [CrossRef] [PubMed]
- Saoud, T.M.; Mistry, S.; Kahler, B. Regenerative Endodontic Procedures for Traumatized Teeth after Horizontal Root Fracture, Avulsion, and Perforating Root Resorption. J. Endod. 2016, 42, 1476–1482. [Google Scholar] [CrossRef]
- Prasad, M.G.S.; Ramakrishna, J.; Babu, D.N. Allogeneic stem cells derived from human exfoliated deciduous teeth (SHED) for the management of periapical lesions in permanent teeth: Two case reports of a novel biologic alternative treatment. J. Dent. Res. Dent. Clin. Dent. Prospect. 2017, 11, 117–122. [Google Scholar] [CrossRef] [Green Version]
- Arora, A.; Bhesania, D.; Kapoor, S. A 5 years’ follow-up of root anatomy-based maturogenesis achieved in infected immature molars using regenerative techniques—A case series. J. Conserv. Dent. 2020, 23, 422–427. [Google Scholar] [CrossRef]
- Nivedhitha, M.S.; Jacob, B.; Ranganath, A. Concentrated Growth Factor: A Novel Platelet Concentrate for Revascularization of Immature Permanent Teeth-A Report of Two Cases. Case Rep. Dent. 2020, 2020, 1329145. [Google Scholar] [CrossRef]
- Kandemir, G.; Güneri, P.; Çalışkan, M.K. Regenerative Endodontic Therapy with Platelet Rich Fibrin: Case Series. J. Clin. Pediatr. Dent. 2020, 44, 15–19. [Google Scholar] [CrossRef]
- Nagaveni, N.B.; Poornima, P.; Mathew, M.G. A Comparative Evaluation of Revascularization Done in Traumatized Immature, Necrotic Anterior Teeth with and without Platelet-rich Fibrin: A Case Report. Int. J. Clin. Pediatr. Dent. 2020, 13, 98–102. [Google Scholar] [CrossRef]
- Brogni, J.K.; Vitali, F.C.; Cardoso, I.V. A second attempt at pulp revascularisation on an immature traumatised anterior tooth: A case report with two-year follow-up. Aust. Endod. J. 2021, 47, 90–96. [Google Scholar] [CrossRef]
- Antov, H.; Duggal, M.S.; Nazzal, H. Management of discolouration following revitalization endodontic procedures: A case series. Int. Endod. J. 2019, 52, 1660–1670. [Google Scholar] [CrossRef] [PubMed]
- Adhikari, H.D.; Gupta, A. Report of a case of platelet-rich fibrin-mediated revascularization of immature 12 with histopathological evaluation. J. Conserv. Dent. 2018, 21, 691–695. [Google Scholar] [CrossRef] [PubMed]
- Suresh, N.; Arul, B.; Kowsky, D. Successful Regenerative Endodontic Procedure of a Nonvital Immature Permanent Central Incisor Using Amniotic Membrane as a Novel Scaffold. Dent. J. 2018, 6, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aunmeungtong, W.; Krongbaramee, T.; Khongkhunthian, P. Endodontic Management of a Chronic Periapical Abscess in a Maxillary Central Incisor with an Immature Root Apex Using Platelet-Rich Fibrin: A Case Report. Eur. Endod. J. 2018, 3, 192–196. [Google Scholar] [CrossRef]
- Plascencia, H.; Díaz, M.; Moldauer, B.I. Non-Surgical Endodontic Management of Type II Dens Invaginatus with Closed and Open Apex. Iran. Endod. J. 2017, 12, 534–539. [Google Scholar] [CrossRef]
- Prasad, J.; de Ataide, I.N.; Chalakkal, P. Comparison between the Outcomes of Two Platelet-Rich Concentrates on Apexogenesis in Young Permanent Incisors Requiring Endodontic Retreatment. Contemp. Clin. Dent. 2018, 9 (Suppl. S1), S156–S159. [Google Scholar] [CrossRef]
- Pinto, N.; Harnish, A.; Cabrera, C. An Innovative Regenerative Endodontic Procedure Using Leukocyte and Platelet-rich Fibrin Associated with Apical Surgery: A Case Report. J. Endod. 2017, 43, 1828–1834. [Google Scholar] [CrossRef]
- Bakhtiar, H.; Esmaeili, S.; Fakhr Tabatabayi, S. Second-generation Platelet Concentrate (Platelet-rich Fibrin) as a Scaffold in Regenerative Endodontics: A Case Series. J. Endod. 2017, 43, 401–408. [Google Scholar] [CrossRef]
- Al-Tammami, M.F.; Al-Nazhan, S.A. Retreatment of failed regenerative endodontic of orthodontically treated immature permanent maxillary central incisor: A case report. Restor. Dent. Endod. 2017, 42, 65–71. [Google Scholar] [CrossRef] [Green Version]
- Gaviño Orduña, J.F.; Caviedes-Bucheli, J.; Manzanares Céspedes, M.C. Use of Platelet-rich Plasma in Endodontic Procedures in Adults: Regeneration or Repair? A Report of 3 Cases with 5 Years of Follow-up. J. Endod. 2017, 43, 1294–1301. [Google Scholar] [CrossRef]
- Scelza, P.; Gonçalves, F.; Caldas, I.; Nunes, F.; Lourenço, E.S.; Tavares, S.; Magno, M.; Pintor, A.; Montemezzi, P.; Edoardo, E.D.; et al. Prognosis of Regenerative Endodontic Procedures in Mature Teeth: A Systematic Review and Meta-Analysis of Clinical and Radiographic Parameters. Materials 2021, 14, 4418. [Google Scholar] [CrossRef] [PubMed]
- Glynis, A.; Foschi, F.; Kefalou, I.; Koletsi, D.; Tzanetakis, G.N. Regenerative Endodontic Procedures for the Treatment of Necrotic Mature Teeth with Apical Periodontitis: A Systematic Review and Meta-analysis of Randomized Controlled Trials. J. Endod. 2021, 47, 873–882. [Google Scholar] [CrossRef] [PubMed]
- American Association of Endodontics. AAE Clinical Considerations for a Regenerative Procedure. Available online: https://f3f142zs0k2w1kg84k5p9i1o-wpengine.netdna-ssl.com/specialty/wp-content/uploads/sites/2/2018/06/ConsiderationsForRegEndo_AsOfApril2018.pdf (accessed on 4 January 2018).
- Lin, J.; Zeng, Q.; Wei, X. Regenerative Endodontics Versus Apexification in Immature Permanent Teeth with Apical Periodontitis: A Prospective Randomized Controlled Study. J. Endod. 2017, 43, 1821–1827. [Google Scholar] [CrossRef] [PubMed]
- Diogenes, A.; Henry, M.A.; Teixeira, F.B. An update on clinical regenerative endodontics. Endod. Top. 2013, 28, 2–23. [Google Scholar] [CrossRef]
- Fang, Y.; Wang, X.; Zhu, J. Influence of Apical Diameter on the Outcome of Regenerative Endodontic Treatment in Teeth with Pulp Necrosis: A Review. J. Endod. 2017, 44, 414–431. [Google Scholar] [CrossRef]
- Oesterle, L.J.; Cronin, R.J., Jr.; Ranly, D.M. Maxillary implants and the growing patient. Int. J. Oral Maxillofac. Implant. 1993, 8, 377–387. [Google Scholar]
- Zitzmann, N.U.; Özcan, M.; Scherrer, S.S.; Bühler, J.M.; Weiger, R.; Krastl, G. Resin-bonded restorations: A strategy for managing anterior tooth loss in adolescence. J. Prosthet. Dent. 2015, 113, 270–276. [Google Scholar] [CrossRef] [Green Version]
- Iohara, K.; Utsunomiya, S.; Kohara, S.; Nakashima, M. Allogeneic transplantation of mobilized dental pulp stem cells with the mismatched dog leukocyte antigen type is safe and efficacious for total pulp regeneration. Stem Cell Res. Ther. 2018, 9, 116. [Google Scholar] [CrossRef] [Green Version]
- Nakashima, M.; Iohara, K.; Zayed, M. Pulp Regeneration: Current Approaches, Challenges, and Novel Rejuvenating Strategies for an Aging Population. J. Endod. 2020, 46, S135–S142. [Google Scholar] [CrossRef]
- Hancerliogullari, D.; Erdemir, A.; Kisa, U. The effect of different irrigation solutions and activation techniques on the expression of growth factors from dentine of extracted premolar teeth. Int. Endod. J. 2021, 54, 1915–1924. [Google Scholar] [CrossRef]
- Galler, K.M.; Buchalla, W.; Hiller, K.A.; Federlin, M.; Eidt, A.; Schiefersteiner, M.; Schmalz, G. Influence of root canal disinfectants on growth factor release from dentin. J. Endod. 2015, 41, 363–368. [Google Scholar] [CrossRef] [PubMed]
- Tavares, S.; Pintor, A.; Mourão, C.F.A.B.; Magno, M.; Montemezzi, P.; Sacco, R.; Alves, G.; Scelza, M.Z. Effect of Different Root Canal Irrigant Solutions on the Release of Dentin-Growth Factors: A Systematic Review and Meta-Analysis. Materials 2021, 14, 5829. [Google Scholar] [CrossRef] [PubMed]
- Jung, C.; Kim, S.; Sun, T.; Cho, Y.B.; Song, M. Pulp-dentin regeneration: Current approaches and challenges. J. Tissue Eng. 2019, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castelo-Baz, P.; Martín-Biedma, B.; Cantatore, G. In vitro comparison of passive and continuous ultrasonic irrigation in simulated lateral canals of extracted teeth. J. Endod. 2012, 38, 688–691. [Google Scholar] [CrossRef] [PubMed]
- Kahler, B.; Rossi-Fedele, G. A Review of Tooth Discoloration after Regenerative Endodontic Therapy. J. Endod. 2016, 42, 563–569. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| P-Population | I-Intervention | C-Comparison | O-Outcome |
|---|---|---|---|
| Necrotic mature and immature adult permanent teeth. The population was determined according to the tooth treated depending on the patient’s age, as is showed in Table 2. | REP (in teeth where all root canals were treated). | Without comparison. | Outcomes are specified in Table 3. Follow-up time: 1 year or more. |
| Patient Age (Years) | Tooth |
|---|---|
| ≥9 | Lower central incisor. |
| ≥10 | Upper central incisor. Lower lateral incisor. Lower and upper first molar. |
| ≥11 | Upper lateral incisor. |
| ≥13 | Lower canine. |
| ≥14 | Lower and upper first premolar. Upper second premolar. |
| ≥15 | Upper canine. Lower second premolar. Lower second molar. |
| ≥16 | Upper second molar. |
| ≥25 | Lower and upper third molar. |
| Primary Goal | Secondary Goal | Tertiary Goal | |
|---|---|---|---|
| Necrotic mature adult permanent teeth | Elimination of symptoms and evidence of bony healing. | Positive response to sensitivity testing. | |
| Necrotic mature adult permanent teeth | Increased root wall thickness, and increased root length. Apex closure (desirable, but perhaps not essential). | Elimination of symptoms and evidence of bony healing. | Positive response to sensitivity testing. |
| Randomized Clinical Trial | Age Group | Number of Teeth Treated |
|---|---|---|
| 1. Brizuela 2020 [32] | 16–58 | 18 |
| 2. El-Kateb 2020 [33] | 20–40 | 18 |
| 3. Arslan 2019 [34] | 20.58 ± 2.53 | 26 |
| Case Report | Age Group | Tooth Treated |
|---|---|---|
| 1. Cordero 2020 [35] | 19 | 1.2 |
| 2. Arslan 2019 [36] | 20 | 1.1 and 1.2 |
| 3. Nagas 2018 [37] | 21 | 2.1 and 2.2 |
| 4. Saoud 2016 [38] | 16 | 1.1 |
| 5. Prasad 2017 [39] | 12 | 3.1 and 4.1 |
| Case Report | Patient’s Age | Tooth Treated |
|---|---|---|
| 1. Arora 2020 [40] | 16 | 4.7 |
| 2. Nivedhitha 2020 [41] | 23 | 1.2 |
| 21 | 2.1 | |
| 3. Kandemir 2020 [42] | 14 | 1.2 |
| 14 | 1.1 | |
| 13 | 1.1 | |
| 4. Nagaveni 2020 [43] | 11 | 1.2 and 2.2 |
| 5. Brogni 2020 [44] | 21 | 1.1 |
| 6. Antov 2019 [45] | 15 | 1.1 |
| 14 | 2.1 | |
| 7. Adhikari 2018 [46] | 29 | 1.2 |
| 8. Suresh 2018 [47] | 18 | 1.1 |
| 9. Aunmentong 2018 [48] | 15 | 2.1 |
| 10. Plascencia 2017 [49] | 11 | 2.1 |
| 11. Prasad 2018 [50] | 13 | 1.1, 1.2, 2.1 and 2.2 |
| 12. Pinto 2017 [51] | 20 | 2.2 |
| 13. Prasad 2017 [39] | 12 | 1.1 |
| 14. Bakhtiar 2017 [52] | 18 | 1.2 |
| 15. Al-Tammami 2017 [53] | 12 | 1.1 |
| 16. Gaviño 2017 [54] | 35 | 1.1 |
| 21 | 1.1 | |
| 24 | 2.2 |
| Primary Outcome | Secondary Outcome: Positive Response to Sensitivity Testing | |
|---|---|---|
| Evidence of Bony Healing | Absence of Symptoms | |
| 97.35% (60 of 62 teeth) | 100% (62 of 62 teeth) | 58% (36 of 62 teeth) |
| Primary Outcome | Secondary Outcome: Positive Response to Sensitivity Testing | |
|---|---|---|
| Evidence of Bony Healing | Absence of Symptoms | |
| 100% (8 of 8 teeth) | 100% (8 of 8 teeth) | 62.5% (5 of 8 teeth) |
| Primary Outcome | Secondary Outcome | Tertiary Outcome: Positive Response to Sensitivity Testing | ||
|---|---|---|---|---|
| Increased Root Wall Thickness | Increased Root Length | Evidence of Bony Healing | Absence of Symptoms | |
| 69.23% (18 of 26 teeth) | 69.23% (18 of 26 teeth) Apex closure 34.61% (9 of 26 teeth) | 100% (26 of 26 teeth) | 96.15% (25 of 26 teeth) | 43.75% (7 of 16 teeth) |
| Root development (both increased root wall thickness and length): 61.5% (16 of 26 teeth) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garrido-Parada, S.; Castelo-Baz, P.; Feijoo-Pato, N.; Gaviño-Orduña, J.; Martín-Biedma, B. Endodontic Regenerative Procedures in Necrotic Adult Teeth. Appl. Sci. 2022, 12, 4212. https://doi.org/10.3390/app12094212
Garrido-Parada S, Castelo-Baz P, Feijoo-Pato N, Gaviño-Orduña J, Martín-Biedma B. Endodontic Regenerative Procedures in Necrotic Adult Teeth. Applied Sciences. 2022; 12(9):4212. https://doi.org/10.3390/app12094212
Chicago/Turabian StyleGarrido-Parada, Sara, Pablo Castelo-Baz, Nancy Feijoo-Pato, José Gaviño-Orduña, and Benjamín Martín-Biedma. 2022. "Endodontic Regenerative Procedures in Necrotic Adult Teeth" Applied Sciences 12, no. 9: 4212. https://doi.org/10.3390/app12094212