Application of Botulinum Toxin in Temporomandibular Disorders: A Systematic Review of Randomized Controlled Trials (RCTs)

 , , , ,
, , , ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol
2.2. Eligibility Criteria
2.2.1. Literature Search
2.2.2. Data Selection and Extraction
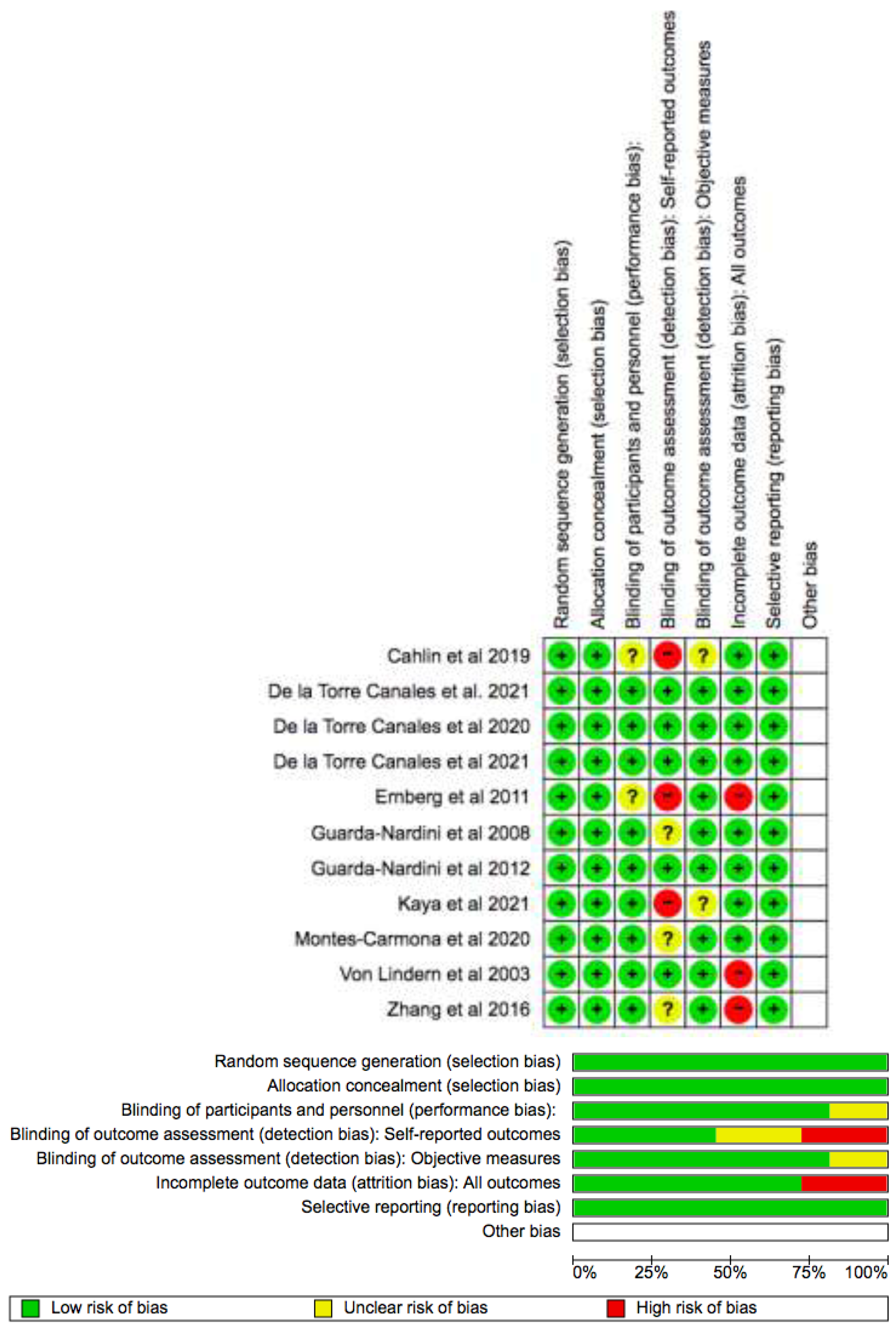
2.2.3. Risk of Bias and Quality of the Studies Assessment
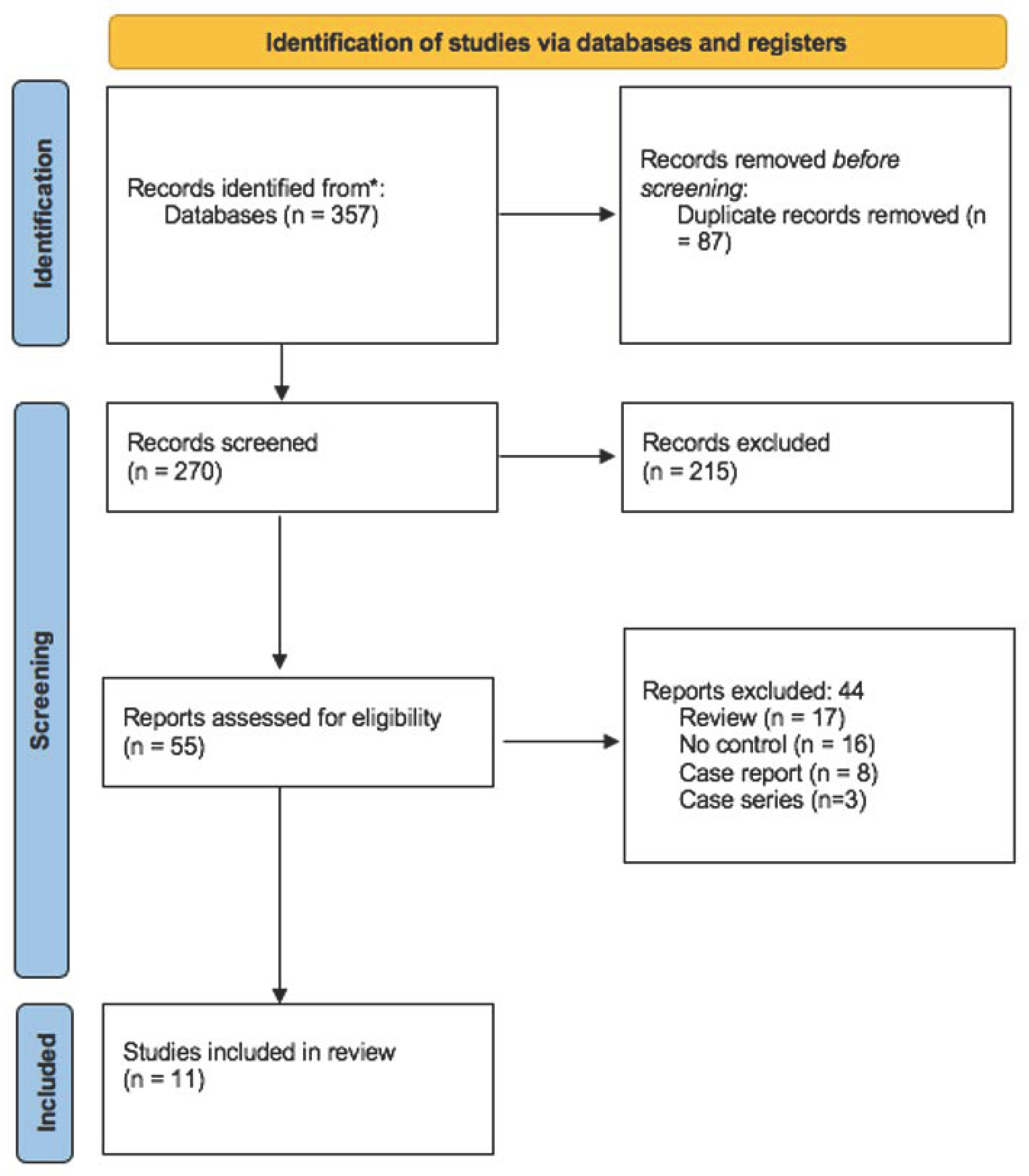
3. Results
Quality Assessment and Risk of Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| TMD | Temporomandibular disorder |
| TMJ | Temporomandibular joint |
| AADR | American Association for Dental Research |
| BoNT-A | Botulinum neurotoxin type A |
| SS | Saline solution |
| FID | Flat intraoral device |
References
- Van Bellinghen, X.; Idoux-Gillet, Y.; Pugliano, M.; Strub, M.; Bornert, F.; Clauss, F.; Schwinté, P.; Keller, L.; Benkirane-Jessel, N.; Kuchler-Bopp, S.; et al. Temporomandibular joint regenerative medicine. Int. J. Mol. Sci. 2018, 19, 446. [Google Scholar] [CrossRef] [Green Version]
- Jerele, C.; Avsenik, J.; Šurlan Popović, K. MRI characteristics of the asymptomatic temporomandibular joint in patients with unilateral temporomandibular joint disorder. Oral Radiol. 2021, 37, 469–475. [Google Scholar] [CrossRef] [PubMed]
- Gauer, R.L.; Semidey, M.J. Diagnosis and treatment of temporomandibular disorders. Am. Fam. Physician. 2015, 91, 378–386. [Google Scholar] [PubMed]
- Ferrillo, M.; Nucci, L.; Giudice, A.; Calafiore, D.; Marotta, N.; Minervini, G.; d’Apuzzo, F.; Ammendolia, A.; Perillo, L.; de Sire, A. Efficacy of conservative approaches on pain relief in patients with temporomandibular joint disorders: A systematic review with network meta-analysis. Cranio–J. Craniomandib. Pract. 2022, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Castroflorio, T.; Bracco, P.; Farina, D. Surface electromyography in the assessment of jaw elevator muscles. J. Oral Rehabil. 2008, 35, 638–645. [Google Scholar] [CrossRef]
- Newton, J.P.; McManus, F.C.; Menhenick, S. Jaw muscles in older overdenture patients. Gerodontology 2004, 21, 37–42. [Google Scholar] [CrossRef]
- Minervini, G.; Mariani, P.; Fiorillo, L.; Cervino, G.; Cicciù, M.; Laino, L. Prevalence of temporomandibular disorders in people with multiple sclerosis: A systematic review and meta-analysis. Cranio–J. Craniomandib. Pract. 2022, 31, 1–9. [Google Scholar] [CrossRef]
- Patel, J.; Cardoso, J.A.; Mehta, S. A systematic review of botulinum toxin in the management of patients with temporomandibular disorders and bruxism. Br. Dent. J. 2019, 226, 667–672. [Google Scholar] [CrossRef]
- Manfredini, D.; Favero, L.; Cocilovo, F.; Monici, M.; Guarda-Nardini, L. A comparison trial between three treatment modalities for the management of myofascial pain of jaw muscles: A preliminary study. Cranio–J. Craniomandib. Pract. 2018, 36, 327–331. [Google Scholar] [CrossRef]
- Canales, G.D.; Manfredini, D.; Grillo, C.M.; Guarda-Nardini, L.; Goncalves, L.M.; Barbosa, C.M.R. Therapeutic effectiveness of a combined counseling plus stabilization appliance treatment for myofascial pain of the jaw muscles: A pilot study. Cranio–J. Craniomandib. Pract. 2017, 35, 180–186. [Google Scholar]
- Mor, N.; Tang, C.; Blitzer, A. Temporomandibular Myofacial Pain Treated with Botulinum Toxin Injection. Toxins 2015, 7, 2791–2800. [Google Scholar] [CrossRef] [PubMed]
- Ferrario, V.F.; Tartaglia, G.M.; Maglione, M.; Simion, M.; Sforza, C. Neuromuscular coordination of masticatory muscles in subjects with two types of implant-supported prostheses. Clin. Oral Implants Res. 2004, 15, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, D.; Siriani, A.O.; Bérzin, F. Effect of conventional TENS on pain and electromyographic activity of masticatory muscles in TMD patients. Pesqui. Odontol. Bras. 2004, 18, 290–295. [Google Scholar] [CrossRef] [PubMed]
- Miranda, L.S.; Graciosa, M.D.; Puel, A.N.; Raulino de Oliveira, L.; Sonza, A. Masticatory muscles electrical activity, stress and posture in preadolescents and adolescents with and without temporomandibular dysfunction. Int. J. Pediatr. Otorhinolaryngol. 2021, 141, 110562. [Google Scholar] [CrossRef] [PubMed]
- Reddy, L.K.V.; Madithati, P.; Narapureddy, B.R.; Ravula, S.R.; Vaddamanu, S.K.; Alhamoudi, F.H.; Minervini, G.; Chaturvedi, S. Personalized Medicine Perception about Health Applications (Apps) in Smartphones towards Telemedicine during COVID-19: A Cross-Sectional Study. J. Pers. Med. 2022, 12, 1920. [Google Scholar] [CrossRef]
- Minervini, G.; D’amico, C.; Cicciù, M.; Fiorillo, L. Temporomandibular Joint Disk Displacement: Etiology, Diagnosis, Imaging, and Therapeutic Approaches. J. Craniofacial Surg. 2022, 14, 7–12. [Google Scholar]
- Serrera-Figallo, M.A.; Ruiz-de-León-Hernández, G.; Torres-Lagares, D.; Castro-Araya, A.; Torres-Ferrerosa, O.; Hernández-Pacheco, E.; Gutierrez-Perez, J.L. Use of Botulinum Toxin in Orofacial Clinical Practice. Toxins 2020, 12, 112. [Google Scholar] [CrossRef] [Green Version]
- Fernandes, G.; de Godoi Gonçalves, D.A.; de Siqueira, J.T.T.; Camparis, C.M. Painful temporomandibular disorders, self reported tinnitus, and depression are highly associated. Arq. Neuropsiquiatr. 2013, 71, 943–947. [Google Scholar] [CrossRef] [Green Version]
- Machado, D.; Martimbianco, A.L.C.; Bussadori, S.K.; Pacheco, R.L.; Riera, R.; Santos, E.M. Botulinum Toxin Type A for Painful Temporomandibular Disorders: Systematic Review and Meta-Analysis. J. Pain. 2020, 21, 281–293. [Google Scholar] [CrossRef]
- Yoshida, K. Effects of Botulinum Toxin Type A on Pain among Trigeminal Neuralgia, Myofascial Temporomandibular Disorders, and Oromandibular Dystonia. Toxins 2021, 13, 605. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Savović, J.; Page, M.J.; Elbers, R.G.; Sterne, J.A.C. Assessing risk of bias in a randomized trial. In Cochrane Handbook for Systematic Reviews of Interventions; Cohrane: London, UK, 2022; Available online: www.training.cochrane.org/handbook (accessed on 23 August 2022).
- Kaya, D.I.; Ataoglu, H. Botulinum toxin treatment of temporomandibular joint pain in patients with bruxism: A prospective and randomized clinical study. Niger. J. Clin. Pract. 2021, 24, 412–417. [Google Scholar] [CrossRef]
- De la Torre Canales, G.; Lorenzi Poluha, R.; Alvarez Pinzon, Y.N.; Rodrigues Conti, P.C.; Manfredini, D.; Sánchez-Ayala, A.; Rizzatti-Barbosa, C.M. Effects of Botulinum Toxin Type A on the Psychosocial Features of Myofascial Pain TMD Subjects: A Randomized Controlled Trial. J. Oral Facial Pain Headache. 2021, 35, 288–296. [Google Scholar] [CrossRef]
- De La Torre Canales, G.; Câmara-Souza, M.B.; Poluha, R.L.; Grillo, C.M.; Conti, P.C.R.; Sousa, M.D.L.R.D.; Rodrigues Garcia, R.C.M.; Rizzatti-Barbosa, C.M. Botulinum toxin type a and acupuncture for masticatory myofascial pain: A randomized clinical trial. J. Appl. Oral Sci. 2021, 29, e20201035. [Google Scholar] [CrossRef] [PubMed]
- Fiorillo, L.; de Stefano, R.; Cervino, G.; Crimi, S.; Bianchi, A.; Campagna, P.; Herford, A.S.; Laino, L.; Cicciù, M. Oral and psychological alterations in haemophiliac patients. Biomedicines 2019, 7, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, L.D.; Liu, Q.; Zou, D.R.; Yu, L.F. Occlusal force characteristics of masseteric muscles after intramuscular injection of botulinum toxin A(BTX–A) for treatment of temporomandibular disorder. Br. J. Oral Maxillofac. Surg. 2016, 54, 736–740. [Google Scholar] [CrossRef] [PubMed]
- Guarda-Nardini, L.; Stecco, A.; Stecco, C.; Masiero, S.; Manfredini, D. Myofascial pain of the jaw muscles: Comparison of short-term effectiveness of botulinum toxin injections and Fascial Manipulation technique. Cranio–J. Craniomandib. Pract. 2012, 30, 95–102. [Google Scholar] [CrossRef]
- Von Lindern, J.J.; Niederhagen, B.; Bergé, S.; Appel, T. Type A Botulinum Toxin in the Treatment of Chronic Facial Pain Associated with Masticatory Hyperactivity. J. Oral Maxillofac. Surg. 2003, 61, 774–778. [Google Scholar] [CrossRef]
- Ernberg, M.; Hedenberg-Magnusson, B.; List, T.; Svensson, P. Efficacy of botulinum toxin type A for treatment of persistent myofascial TMD pain: A randomized, controlled, double-blind multicenter study. Pain 2011, 152, 1988–1996. [Google Scholar] [CrossRef] [PubMed]
- Sitnikova, V.; Kämppi, A.; Teronen, O.; Kemppainen, P. Effect of Botulinum Toxin Injection on EMG Activity and Bite Force in Masticatory Muscle Disorder: A Randomized Clinical Trial. Toxins 2022, 14, 545. [Google Scholar] [CrossRef] [PubMed]
- De la Torre Canales, G.; Alvarez-Pinzon, N.; Muñoz-Lora, V.R.M.; Vieira Peroni, L.; Farias Gomes, A.; Sánchez-Ayala, A.; Haiter-Neto, F.; Manfredini, D.; Rizzatti-Barbosa, C.M. Efficacy and safety of botulinum toxin type a on persistentmyofascial pain: A randomized clinical trial. Toxins 2020, 12, 395. [Google Scholar] [CrossRef]
- Cahlin, B.J.; Lindberg, C.; Dahlström, L. Cerebral palsy and bruxism: Effects of botulinum toxin injections—A randomized controlled trial. Clin. Exp. Dent. Res. 2019, 5, 460–468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guarda-Nardini, L.; Manfredini, D.; Salamone, M.; Salmaso, L.; Tonello, S.; Ferronato, G. Efficacy of botulinum toxin in treating myofascial pain in bruxers: A controlled placebo pilot study. Cranio–J. Craniomandib. Pract. 2008, 26, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Long, H.; Liao, Z.; Wang, Y.; Liao, L.; Lai, W. Efficacy of botulinum toxins on bruxism: An evidence-based review. Int. Dent. J. 2012, 62, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Ågren, M.; Sahin, C.; Pettersson, M. The effect of botulinum toxin injections on bruxism: A systematic review. J. Oral Rehabil. 2020, 47, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Núñez, T.; Amghar-Maach, S.; Gay-Escoda, C. Efficacy of botulinum toxin in the treatment of bruxism: Systematic review. Med. Oral Patol. Oral Cir. Bucal 2019, 24, e416–e424. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Authors | Publication Year | Study Design | No. Patients | Comparison of Interventions | Follow-Up |
|---|---|---|---|---|---|
| De la Torre Canales et al. [23] | 2021 | RCT | 100 | FID vs. SS vs. BoNT-A | 6 months |
| Kaya et al. [22] | 2021 | RCT | 40 | Occlusal splint vs. BoNT-A | 6 months |
| De la Torre Canales et al. [24] | 2021 | RCT | 54 | Acupuncture vs. SS vs. BoNT-A | 1 month |
| De la Torre Canales et al. [31] | 2020 | RCT | 100 | FlD vs. SS vs. BoNT-A | 6 months |
| Montes-Carmona et al. [25] | 2020 | RCT | 60 | Lidocaine vs. SS vs. BoNT-A | 6 months |
| Cahlin et al. [32] | 2019 | RCT | 12 | SS vs. BoNT-A | 4 months |
| Zhang et al. [26] | 2016 | RCT | 30 | SS vs. no injection vs. BoNT-A | 6 months |
| Guarda-Nardini et al. [27] | 2012 | RCT | 30 | Fascial manipulationvs BoNT-A | 3 months |
| Ernberg et al. [29] | 2011 | RCT | 21 | SS vs. BoNT-A | 3 months |
| Guarda-Nardini et al. [33] | 2008 | RCT | 20 | SS vs. BoNT-A | 6 months |
| Von Lindern et al. [28] | 2003 | RCT | 90 | SS vs. BoNT-A | 3 months |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Francesco, F.; Lanza, A.; Di Blasio, M.; Vaienti, B.; Cafferata, E.A.; Cervino, G.; Cicciù, M.; Minervini, G. Application of Botulinum Toxin in Temporomandibular Disorders: A Systematic Review of Randomized Controlled Trials (RCTs). Appl. Sci. 2022, 12, 12409. https://doi.org/10.3390/app122312409
Di Francesco F, Lanza A, Di Blasio M, Vaienti B, Cafferata EA, Cervino G, Cicciù M, Minervini G. Application of Botulinum Toxin in Temporomandibular Disorders: A Systematic Review of Randomized Controlled Trials (RCTs). Applied Sciences. 2022; 12(23):12409. https://doi.org/10.3390/app122312409
Chicago/Turabian StyleDi Francesco, Fabrizio, Alessandro Lanza, Marco Di Blasio, Benedetta Vaienti, Emilio A. Cafferata, Gabriele Cervino, Marco Cicciù, and Giuseppe Minervini. 2022. "Application of Botulinum Toxin in Temporomandibular Disorders: A Systematic Review of Randomized Controlled Trials (RCTs)" Applied Sciences 12, no. 23: 12409. https://doi.org/10.3390/app122312409