
A Study Protocol to Evaluate the Effects of Vestibular Training on the Postural Control of Healthy Adults Using Virtual Reality

1
Department of Physical Therapy, Clarkson University, Potsdam, NY 13699, USA
2
Department of Mechanical & Aerospace Engineering, Clarkson University, Potsdam, NY 13699, USA
3
Department of Electrical and Computer Engineering, Clarkson University, Potsdam, NY 13699, USA
*
Author to whom correspondence should be addressed.
Appl. Sci. 2022, 12(23), 11937; https://doi.org/10.3390/app122311937
Submission received: 30 September 2022
/
Revised: 31 October 2022
/
Accepted: 3 November 2022
/
Published: 23 November 2022
(This article belongs to the Topic Virtual Reality, Digital Twins, the Metaverse)
Abstract
:Featured Application
This study protocol will promote efficient sensory reweighting and the integration of postural control, and will modify vestibular and motor responses. The training will be used as a rehabilitation protocol for neurological populations who have sensory integration issues, including those with mild traumatic brain injuries, strokes, and multiple sclerosis.
Abstract
Postural instability is a common symptom of vestibular dysfunction due to an insult to the vestibular system. Vestibular rehabilitation is effective in decreasing dizziness and visual symptoms, and improving postural control through several mechanisms, including sensory reweighting. As part of the sensory reweighting mechanisms, vestibular activation training with headshake activities influences vestibular reflexes. However, combining challenging vestibular and postural tasks to facilitate more effective rehabilitation outcomes is underutilized. Our research goal is to develop a virtual reality vestibular rehabilitation method for vestibular-postural control in neurological populations with vestibular and/or sensorimotor control impairment. The NeuroCom® SMART Balance Master (Natus Medical Inc., Pleasanton, CA, USA), which was used in a prior study, is expensive and bulky. Hence, a novel study protocol is established in this paper with the detailed objectives and pre-/post-intervention data analysis pipeline (ANOVA, t-test, post hoc analysis, etc.) involving modern off-the-shelf sensors and custom instrumentation (electromyography, electrooculography, video head impulse testing, force plates, and virtual reality headsets). It is expected that the training will significantly decrease vestibuloocular reflex gains and eye movement variability, as well as reweight the somatosensory ratio, finetune postural muscle activation, and consequently improve postural flexibility and produce a faster automatic postural response. The findings may have implications for the future development of vestibular rehabilitation protocols.
1. Introduction
Vestibular dysfunction with poor postural stability is most common among the elderly [1,2] and contributes to their increased risk of falls [3]. Healthy postural stability results from accurate somatosensory, visual, and vestibular inputs and the capacity of the central nervous system (CNS) to weigh these sensory inputs to produce optimal postural balance [3]. When visual and/or somatosensory inputs are inadequate or unreliable, the CNS relies more heavily on the vestibular system for balance [4]. Untreated, patients often exhibit signs and symptoms such as vertigo and poor balance which can be treated with vestibular rehabilitation [5,6,7]. The goal of vestibular rehabilitation is to reduce dizziness, improve gaze stabilization, correct the overdependence of the postural system on visual and somatosensory inputs, and improve balance, gait, and quality of life [6,8]. The underlying neural mechanisms to achieve these purposes in vestibular rehabilitation include adaptation, habituation, long-term potentiation (LTP), long-term depression (LTD), and sensory reweighting [6,9,10,11].
Several traditional vestibular rehabilitation methods focus mainly on head movements to activate the vestibular system. Adding balance training to vestibular activation activities has demonstrated significant improvement in subjective dizziness, oculomotor control, balance, and gait in neurologic patients [12,13,14]. Using the underlying mechanisms in vestibular rehabilitation, we demonstrated beneficial outcomes in vestibular and motor responses in healthy young adults following our concurrent headshake and weight shift training (Concurrent HS-WST) protocol. In this protocol, participants volitionally performed simultaneous weight shifts in standing and rhythmic head rotations in the horizontal direction while following targets on the computer screen of the NeuroCom® SMART Balance Master (Natus Medical Inc., Pleasanton, CA, USA). The simultaneous activity decreased the training duration in performing both activities and consequently encouraged real-time sensory reweighting and integration. The findings showed that there were significant positive changes in the vestibuloocular reflex (VOR) gain, eye movement variability, somatosensory reweighting, muscle activity in medial gastrocnemius, mediolateral sway, automatic postural control, and postural flexibility [15,16]. However, the NeuroCom® is a large, heavy, and expensive system; these qualities render it inaccessible to clinicians and other researchers aiming to obtain these promising benefits of the Concurrent HS-WST protocol.
To improve on the effectiveness and accessibility of the Concurrent HS-WST [15], the training will be adapted to a low cost, portable virtual reality (VR) tool. VR is one of the novel methods to engage individuals to participate in vestibular rehabilitation [17]. Using a VR environment to design a vestibular rehabilitation protocol may decrease the tediousness associated with the therapy and increase patients’ motivation and training adherence [18,19]. Performing the therapy in the immersive environment can better improve clinical outcomes compared to traditional vestibular rehabilitation methods [20,21,22]. In addition, the immersive VR environment compared to NeuroCom’s visual feedback screen will increase optic flow, thereby stimulating the visual-vestibular channels and modifying vestibular-postural responses [17]. The design of our protocol is, therefore, to encourage optokinetic (eye stabilization on the visual scene)–VOR calibration by incorporating immersive visual feedback during headshake movements and challenging the somatosensory system (through postural training). Combined, these would modify sensory reweighting and vestibular reflexes, as well as improve gaze stabilization and postural responses. The contributions of related vestibular rehabilitation studies have been summarized in Table 1. This current project is the essential first step toward our goal to rigorously evaluating the efficacy of the Concurrent VR HS-WST and rendering it accessible to the clinical and research communities. The purpose of this study is to determine whether concurrent vestibular activation with postural training using virtual reality can reweight the sensory system and change vestibular-ocular and -motor responses in healthy young adults.
Study Contribution: The contribution of this paper is a novel study protocol, alternative to the training modules of the NeuroCom® SMART Balance, to design a portable, accessible VR-based vestibular rehabilitation method. This paper also presents the pre-/post-intervention using off-the-shelf sensors and custom instrumentation outcome measures and a data analysis pipeline to evaluate the effectiveness of this study protocol.
2. Objectives and Hypotheses
The first aim of this study is to determine whether concurrent headshake and weight shift training using virtual reality (Concurrent VR HS-WST) can change vestibular-ocular and -motor responses in healthy young adults. It is hypothesized that VOR gain, eye movement variability, and the amplitude of the electromyography (EMG) signal will significantly decrease following the training intervention. Similarly, the center of pressure (COP) sway velocity during ramp perturbation will significantly increase (indicating improved postural flexibility), while COP sway area, anteroposterior standard deviation (AP Std), and mediolateral standard deviation (ML Std) sways will decrease following the training intervention. Moreover, the time between the COP maximum peak to the minimum peak of the trajectory during ramp perturbation will significantly decrease (indicating faster automatic postural response).
The second aim is to determine whether Concurrent VR HS-WST can reweight the sensory systems of postural control processing in healthy young adults. It is hypothesized that the Modified Clinical Test of Sensory Interaction on Balance (mCTSIB) equilibria and composite scores will significantly improve following the training intervention. Sensory weighting will change significantly, as indicated by changes in visual, somatosensory, and vestibular dependence. Postural stability will improve (i.e., COP sway area, velocity standard deviation [Vel Std], AP Std, and ML Std sways will decrease, while COP multiscale entropy velocity will increase).
3. The Details of the Proposed Human Study
3.1. Participants
To detect a significant difference between two groups in a 2 × 2 repeated-measures crossover design, at alpha 0.05, 0.30 effect size, and at beta = 0.80 [23], requires a minimum of sixteen (16) 18 to 35-year-old healthy participants. Assuming a 30% attrition (based on a pilot study), 24 participants will be recruited from students and staff in the Clarkson University community using fliers, campus-wide emails, and announcements. Participants who give written informed consent will be randomized into two groups. Group one will receive the training intervention for six days, while group two will not receive any training. Each group will be given a four-day washout period and the order of the interventions (sequence) will be reversed.
3.2. Inclusion and Exclusion Criteria
Healthy participants who can stand independently and can perform postural assessments, including reactive balance following mechanical perturbations, will be included in the study. Participants should be able to perform headshake activities and weight shift training while standing for 25 min with very minimal breaks. Participants will be excluded if they have had evidence of concussion, vestibular, balance, or oculomotor issues in the prior six months or have neuropathic conditions. In addition, participants with current musculoskeletal deficits including significant postural abnormalities or pain or limitations in neck range of motion will be excluded. Other exclusion criteria will include participants with recent (within six months) orthopedic surgery that can impact postural training and visual impairment below 20/50 (corrected) vision.
3.3. Study Methods
3.3.1. Outcome Measures and Assessment Procedure
Vestibuloocular Reflex
The video head impulse test (vHIT) device (GN Otometrics, Taastrup, Denmark) will be used to assess horizontal and vertical VOR gain. Participants will be seated 1.3 m away from a wall target, be fitted with vHIT device, and the device will be calibrated. The researcher will grip the participant’s head and quickly rotate it either to the left or right about 10–15 degrees for horizontal VOR assessment or up or down along the right anterior left posterior (RALP) or left anterior right posterior (LARP) orientations. During this, the participant will be instructed to keep their eyes fixated on the wall mounted target. Twenty unpredictable head impulses (ten in each direction) will be performed to assess the left/right horizontal and up/down vertical semicircular canals (SCCs) (Figure 1) [24].
Electromyography and Acceleration
The Delsys Trigno inertial measurement unit (IMU) wireless system (Delsys Inc., Boston, MA, USA) will be used to record EMG and acceleration data only during toes-up and toes-down rotations (i.e., perturbation trial assessments) on the force plate perturbation device. The 16-channel Delsys system will be used to assess muscle activity of eight postural muscles, namely: sternocleidomastoid, cervical erector spinae, rectus abdominis, lumbar erector spinae (L1/L2), rectus femoris, biceps femoris, medial gastrocnemius, and tibialis anterior (sampling rate = 1100 Hz). Electrode placement will follow the standard guidelines [25]. After skin preparations using razor blades and isopropyl alcohol wipes, participants will be instructed to lay down on a mat so the researcher can locate and mark the correct placements for the sensors, and then fix the IMU sensors to each participant’s forehead, neck, trunk, abdomen, and legs using Delsys adhesive patches. The forehead and first thoracic spinous process (T1) sensors will serve as the accelerometers.
Eye Movement Variables
The BlueGain electrooculography (EOG) device (Cambridge Research Systems) [26,27] will be used to assess horizontal and vertical eye movements (sampling rate = 1 kHz) only during perturbation trials. After skin preparation using isopropyl alcohol wipes, two sets of two “duck foot” surface gel electrodes (20 × 15 mm, Ag/AgCl sensor; Ambu Neuroline 700, Denmark) will be placed horizontally and vertically around the eye, with a reference electrode on the forehead. The wireless device will be connected to the EOG software on a desktop computer via Bluetooth connectivity, and the device will be affixed to the participant’s arm via its arm band case. The horizontal and vertical calibrations of the EOG device will be performed using two respective targets which are 42 cm apart, with the participant seated 1.3 m away from the wall targets.
Quiet Postural Balance
The mCTSIB is a clinical version of the Sensory Organization Test (SOT) and it is used to assess the sensory contributions necessary for balance during quiet standing. The mCTSIB has four different testing conditions, namely: Condition 1, eyes open (EO) on stable support (SS); Condition 2, eyes closed (EC) on SS; Condition 3, EO on a foam surface (FS); and Condition 4, EC on FS [28]. In this current study, the mCTSIB will be performed using the NeuroCom® extended force platform and an Airex foam pad (19.69 × 16.14 × 2.36 inches). Participants will be asked to stand upright, as stable as possible, for 10 s on the force platform with feet shoulder-width apart and hands by their sides for each of the four conditions. During the foam conditions, the participant will stand on the foam which will be placed on the force platform. Three trials will be performed for each condition. The trial will be terminated when the participant opens their eyes in an EC condition or loses balance and requires manual assistance to prevent a fall. The equilibrium scores and the COP data will be used to calculate the sensory ratios and sway measures, respectively.
Perturbed Postural Balance
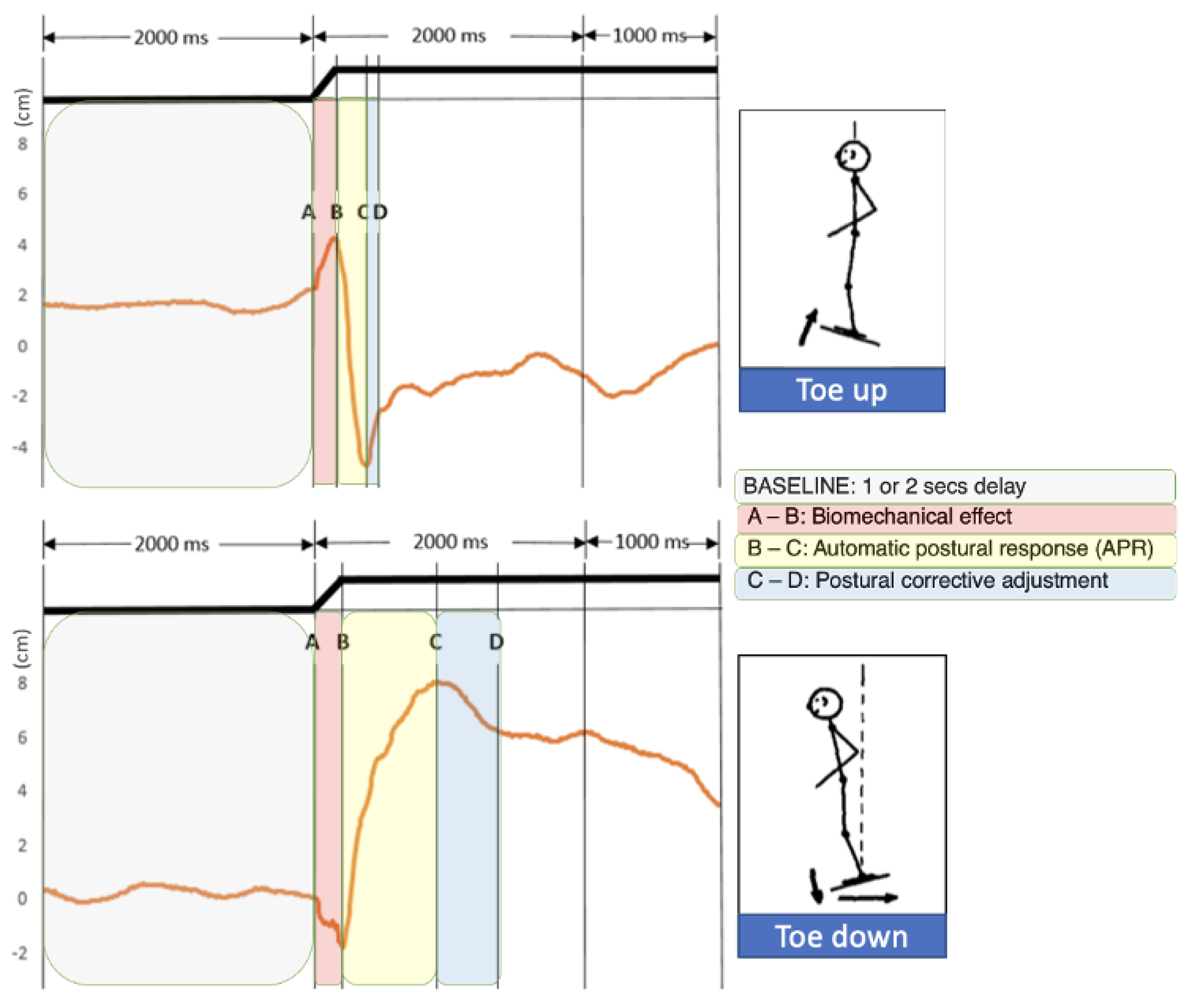
The force plate perturbation device will elicit toes-up and toes-down perturbations to assess how a participant would catch themselves from falling, simulating a forward or backward push. Participants will be put in a safety harness during the assessment and will also be spotted by the researcher. It will record the COP of the participant during the assessment (Figure 2). The angular velocity of the toes-up or toes-down rotations will be ±50°/s, with an amplitude of 10° and a 0.2 s duration [29,30,31]. Six 5 s trials (i.e., unpredictable three toes up, followed by three toes down) will be performed with random onset delays of 1, 2, or 3 s between each trial meant to elicit an automatic postural response. The Delsys trigger device will be used to synchronize the Delsys device to the BlueGain EOG and ramp perturbation devices.
3.3.2. Training Protocol
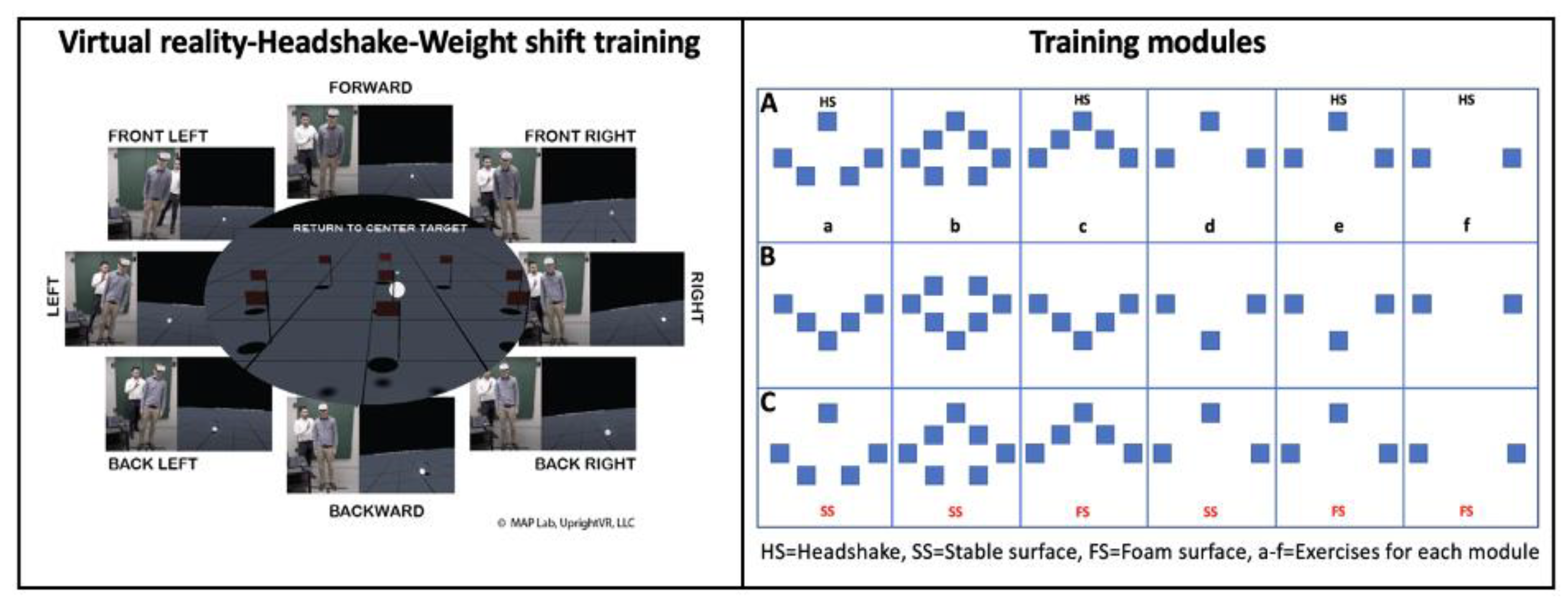
The Concurrent VR-HS-WST protocol (UpRight VR, LLC, Temple University) will be used for the training. The algorithms of the protocol have been derived from other related studies [32,33]. This protocol uses a VR Oculus Quest 2 headset which contains the programmed training modules, an Airex foam, weight shifting activities, and headshake activities to train participants in eight directions (Figure 3, left).
After baseline assessments, the participant will don the Oculus VR headset in a standing position on the floor (Figure 3, right a, b, d) or on the Airex foam (Figure 3, right c, e, f) and be instructed to shift their center of mass (COM) as quickly and accurately as they can to reach visual targets located in the eight possible directions (Figure 3, left). Note that each exercise has variable number of targets to avoid monotony, make the activity enjoyable, and minimize the amount of energy expended by the participant to complete the tasks. Each target will appear randomly every 4s as the participant shifts their COM into the new target and remain in that target for 4s until the next target shows up. While the participant performs the weight shifts, in some of the exercises (Figure 3, right a, c e, f), they will concurrently rotate the head in a horizontal rhythmic pattern (±30°) synchronously to a metronome (80–120 beats/min). Each training session will comprise 18 exercises (modules A–C, exercises a–f), each administered for 1 min. The level of the metronome beats/min and the limit of stability (LOS) between the exercise targets will be increased progressively. Training sessions will last for 25 min and will be performed for seven days with a weekend break. There will be a 15 s and 60 s break between each exercise and training module, respectively. The sequence of training will follow a training schedule (Table 2), where Group 1 will receive training intervention for seven days, with a four-day washout period, and a seven-day no-training period. Group two will follow the reverse sequence.
There will be immediate, 24-, and 48-h reassessments after training or no training periods. During the training, the participant will put on a safety harness and be spotted by a researcher. The total number of reported dizziness, headaches, and nausea will be obtained before and after each day’s training using a visual analog scale (VAS) symptom score. There will be no data collection during the training period except the number of targets reached per exercises as recorded by the training program in the Oculus headset.
4. Analysis of Outcome
The first objective of this project is to assess changes in vestibular-ocular and -motor responses following the Concurrent VR HS-WST. An average VOR gain will be calculated from the left and right horizontal SCCs gain and upward and downward vertical SCCs for each participant. The EOG horizontal and vertical signals during the perturbation trials will be calculated to quantify eye movement amplitude (degrees). Data will be filtered using a Butterworth lowpass filter of second order and at 30 Hz cutoff frequency. Filtered data will be detrended and the displacement (deg) will be calculated for the horizontal and vertical signals. The displacement will be differentiated to velocity (deg/s). Averages of the three trials will be found from the ramp onset to the end of the 5 s trials and from ramp onset to the next 200 ms. Eye movement area (using principal component analysis), velocity, horizontal eye movement, and vertical eye movement standard deviation will be calculated. EMG data will be normalized by using the ratio of the particular trial data to the mean and standard deviation of the resting EMG, expressed as a percentage. The normalized signals will be full wave-rectified, low pass-filtered, and smoothed at 10 Hz using a Butterworth filter of the fourth order (MATLAB 2022, Mathworks Inc., Natick, MA, USA). The means of the filtered signals will be calculated to obtain the muscle activations (amplitude) of each condition of the mCTSIB trials. Similarly, the ramp EMG data will be normalized and filtered as stated above. The means of ramp EMG signals will be calculated from ramp onset to the end of the 5 s trial to obtain the muscle activations. Means of toes-up and toes-down will be calculated separately. In addition, EMG amplitudes will be obtained from ramp onset to the next 200 ms. The time onset response with corresponding time onset amplitude, as well as peak amplitude with corresponding peak time, will be extracted using MATLAB’s “findpeaks” function. Where the locations are not correctly identified by MATLAB, visual inspection with the aid of MATLAB data tip tool will be used to identify them.
The COP of the ramp trials from onset to 200 ms and from onset to the end of the 5 s trial will be obtained and transformed into four COP sway variables: COP sway area (using principal component analysis), standard deviation of sway velocity (using path length divided by total time [velocity SD]), standard deviation of mediolateral (ML SD), and anteroposterior (AP SD) sways. Means of toes-up and toes-down will be calculated separately. In addition, the sway velocity of the peak-up and peak-down of the COP postural trajectory will be calculated to obtain the automatic postural response (APR). Repeated measures analysis of variance (RM ANOVA) will be used to analyze VOR gains, eye movement variables during toes-up and -down rotations, and muscle activation signals of the mCTSIB. RM ANOVA will be used to analyze the EMGs of individual trials and average trials for toes-up and -down rotations. RM ANOVA will be used to analyze COP sway measures and the ARP for toes-up and -down trials. Bonferroni post hoc adjustments will be used to adjust for multiple between-group comparisons. Simple frequency analysis will be used to compare the frequency of falls, number of targets reached per exercise, and self-reported VAS dizziness, headaches, and nausea.
The second objective is to assess changes in sensory reweighting of postural control processing following the Concurrent VR HS-WST. The total time in seconds of each mCTSIB condition will be calculated for each participant. To analyze the postural changes in different metric dimensions, the COP time series data of the mCTSIB will be transformed into COP sway area, velocity SD, ML SD, AP SD sways, and multiscale entropy (MSE) sway velocity (m = 2; r = 0.2, tau = 10) using custom MATLAB scripts performed offline. Data will be filtered at 30 Hz before the calculations. Sensory ratios, composite scores, and equilibrium scores will be calculated for each condition. RM ANOVA will be used to analyze the duration for each mCTSIB condition, COP sway measures, sensory ratios, composite scores and equilibrium scores. Bonferroni post hoc adjustments will be used to adjust for multiple between-group comparisons. All statistical analyses will be conducted using SPSS software (v28; IBM Corp., Armonk, NY, USA) and significance will be set at α ≤ 0.05.
5. Discussion
A summary of the proposed human study is that twenty-four young healthy individuals, aged 18–35 years, with no neurological, musculoskeletal, or balance issues, will be recruited and randomly placed into two groups for this crossover design study. Using the VR headset, group one will receive six days of training by performing rhythmic horizontal headshake activities via a visual feedback protocol while performing simultaneous weight shift training standing on a floor surface or on an Airex foam pad. Meanwhile, group two will perform no training for six days and the order will be reversed. Six pre- and post-assessments of VOR gain, eye movements, electromyography and balance will be collected at specific periods. A two-intervention (training vs. no-training) by six-time-points repeated measures ANOVA will be used to analyze data. Significance will be set at α ≤ 0.05. Post hoc tests will be conducted using a combination of paired t-tests with Bonferroni adjustments.
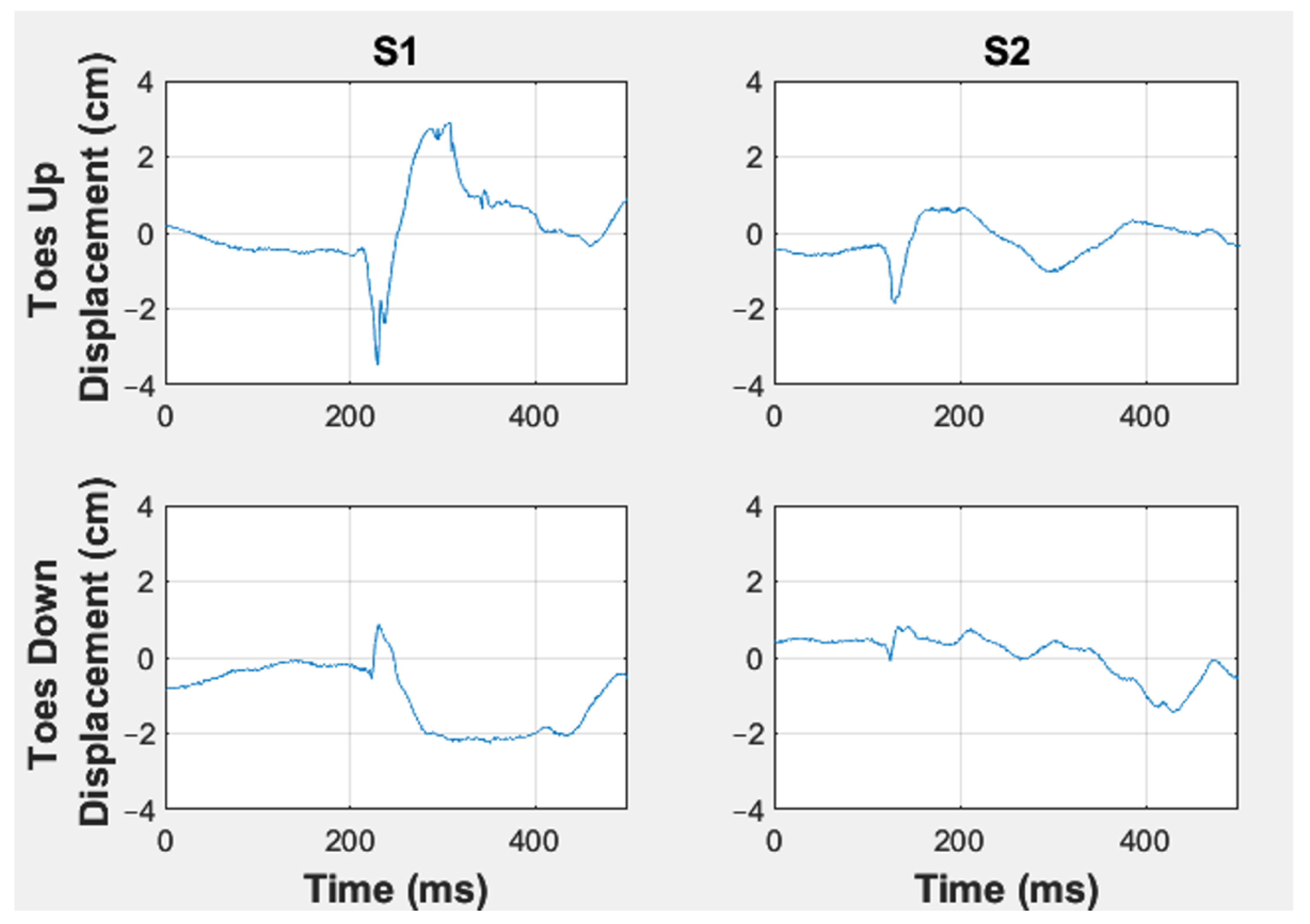
The overarching goal of this endeavor is that VR will be an effective means to deliver the Concurrent HS-WST comparable to the protocol of the NeuroCom® as indicated by enhancement in vestibuloocular and -motor responses. We expect that the effect of the novel training will significantly recalibrate VOR gains and decrease eye movement variability to maintain gaze stabilization (Figure 4).
The vestibuloocular recalibration and decreased eye movement variability will be due to the repeated, rhythmic headshake motions which will activate the SCCs and otolith organs to transit impulses through the vestibulocochlear nerve to the vestibular nerve at the lateral pontomedullary junction. Through mediating pathways including the abducens nucleus, medial longitudinal fasciculus, and oculomotor nuclei, specific extraocular muscles are driven to produce compensatory eye movements leading to gaze stabilization for postural stability [11,34]. Evidence of the gaze stabilization will be shown by the decreased eye movement variability. The recalibration of the VOR gain would likely be in the down-gain direction [16] following simultaneous enhancement and suppression of vestibular signals and eye movement signals via long-term potentiation (LTP) and depression (LTD), respectively, as the underlying mechanism [11].
We also anticipate that postural balance will be improved by reweighting the somatosensory ratio to compensate for the changes in the other sensory channels. The influence on the somatosensory system will mainly be due to the stimulation of proprioceptors in the soles of the feet and in the joints of the lower limbs during the WST. This will result in a bottom-up signal transmission, will modify spinal reflexes, and the somatosensory input which will be integrated in the CNS together with the vestibular and visual inputs to produce a more efficient postural response [34,35]. Our novel VR vestibular training is hypothesized to finetune postural muscle activation patterns by decreasing EMG amplitude signals, as less neural activity is required to produce the amount of force production for balance control (Figure 5) [16]. The modulation of the muscle activation would be suggestive of refined descending vestibular impulses following the activation of the semicircular canals [16].
Consequently, the training will lead to improved postural flexibility and shortened automatic postural response time through modulating of the descending vestibular responses as expected to be shown during the perturbation trial assessments (Figure 6) [16]. The improved postural flexibility is hypothesized to stem from an increased COP sway velocity variability which could indicate more flexibility as participants exhibit larger but optimal limits stability for balance control [36]. The automatic postural response will be indicated by an increased COP sway velocity following the training, which will suggest a faster response to the perturbation trials [15,30].
This study may have some limitations. Since we will employ healthy young adults without vestibular or postural deficits, the differences in the outcome measures may not be large as expected in a vestibular impaired population. In addition, the training is relatively short compared to a typical rehabilitation protocol, which may last for about six weeks. However, if statistically significant changes in the outcome measures are found (although they may not be large), it would suggest that our training protocol will have the potential of demonstrating effectiveness in the recalibration of the vestibular-postural system in a vestibular-impaired population.
6. Conclusions and Future Studies
Our proposed Concurrent VR HS-WST is expected to reweight the somatosensory system, recalibrate the VOR gain, and decrease eye movement variability to promote gaze stabilization. The amplitude of muscle activation is expected to decrease and be refined for better efficiency, with an improved postural stability and flexibility. The results of this pilot study will serve as the essential foundation for future work to develop targeted, effective vestibular rehabilitation interventions for patients with neurological impairments, such as those with vestibular disorders or sensory integration problems. Having established in future work the effectiveness of VR in delivering the Concurrent HS-WTS protocol with patients, it would further be adapted (i.e., apps developed) for use in home-exercise programs via smartphone solutions or tablets, which will further increase portability, accessibility, and affordability. Such solutions would also enable the monitoring of patients receiving interventions via “telemedicine” to accommodate public health requirements for social distancing. To ensure patients’ safety during the training, specific parameters of the training will be tailored to the patient’s postural control ability level following assessment by the clinician.
Author Contributions
K.O.A.-K.: Conception and design of the study, writing of protocol, design and collection of data and management system and drafting and revision of manuscript; E.L.: design and development of force plate perturbation device, providing results data, drafting and revision of manuscript; M.H.I.: conception of results, providing results data, drafting and revision of manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The prior study was conducted in accordance with the Declaration of Helsinki, and approved by the Research Administration Institutional Review Board of Temple University (protocol code, 23436 on 17 February 2017). The current proposed study has also been approved by the Institutional Review Board of Clarkson University (protocol code, 22–25 on 27 October 2021).
Informed Consent Statement
Written informed consent was obtained from the participant whose data has been included in the study.
Data Availability Statement
Not applicable.
Acknowledgments
We would like to acknowledge the use of the VR program (UpRight VR, LLC, Temple University) developed by W.G. Wright, in the Motion-Action-Perception lab.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Lee, J.D.; Kim, C.; Hong, S.M.; Kim, S.H.; Suh, M.; Kim, M.; Shim, D.B.; Chu, H.; Lee, N.H.; Kim, M.; et al. Prevalence of vestibular and balance disorders in children and adolescents according to age: A multi-center study. Int. J. Pediatr. Otorhinolaryngol. 2017, 94, 36–39. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, Y.; Carey, J.P.; Della Santina, C.C.; Schubert, M.C.; Minor, L.B. Disorders of Balance and Vestibular Function in US Adults: Data from the National Health and Nutrition Examination Survey, 2001–2004. Arch. Intern. Med. 2009, 169, 938. [Google Scholar] [CrossRef] [PubMed]
- Peterka, R.J. Sensorimotor integration in human postural control. J. Neurophysiol. 2002, 88, 1097–1118. [Google Scholar] [CrossRef] [Green Version]
- Nashner, L.M. Adaptation of human movement to altered environments. Trends Neurosci. 1982, 5, 358–361. [Google Scholar] [CrossRef]
- Shumway-Cook, A.; Woollacott, M.H. Motor Control: Translating Research into Clinical Practice; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2007. [Google Scholar]
- Hall, C.D.; Herdman, S.J.; Whitney, S.L.; Cass, S.P.; Clendaniel, R.A.; Fife, T.D.; Furman, J.M.; Getchius, T.S.; Goebel, J.A.; Shepard, N.T.; et al. Vestibular rehabilitation for peripheral vestibular hypofunction: An evidence-based clinical practice guideline: From the American Physical Therapy Association Neurology Section. J. Neurol. Phys. Ther. 2016, 40, 124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDonnell, M.N.; Hillier, S.L. Vestibular rehabilitation for unilateral peripheral vestibular dysfunction. Cochrane Database Syst. Rev. 2015, 1, 1–95. [Google Scholar] [CrossRef] [PubMed]
- Whitney, S.L.; Alghwiri, A.A.; Alghadir, A. An overview of vestibular rehabilitation. Handb. Clin. Neurol. 2016, 137, 187–205. [Google Scholar]
- Lee, Y.J.; Shin, J.E.; Park, M.S.; Kim, J.M.; Na, B.R.; Kim, C.-H.; Park, H.J. Comprehensive Analysis of Head-Shaking Nystagmus in Patients with Vestibular Neuritis. Audiol. Neurotol. 2012, 17, 228–234. [Google Scholar] [CrossRef] [PubMed]
- Telian, S.A.; Shepard, N.T.; Smith-Wheelock, M.; Kemink, J.L. Habituation Therapy for Chronic Vestibular Dysfunction: Preliminary Results. Otolaryngol. Head Neck Surg. 1990, 103, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Inagaki, K.; Hirata, Y. Computational theory underlying acute vestibulo-ocular reflex motor learning with cerebellar long-term depression and long-term potentiation. Cerebellum 2017, 16, 827–839. [Google Scholar] [CrossRef] [PubMed]
- Alsalaheen, B.A.; Mucha, A.; Morris, L.O.; Whitney, S.L.; Furman, J.M.; Camiolo-Reddy, C.E.; Collins, M.W.; Lovell, M.R.; Sparto, P.J. Vestibular Rehabilitation for Dizziness and Balance Disorders after Concussion. J. Neurol. Phys. Ther. 2010, 34, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Gottshall, K.R.; Hoffer, M.E. Tracking Recovery of Vestibular Function in Individuals with Blast-Induced Head Trauma Using Vestibular-Visual-Cognitive Interaction Tests. J. Neurol. Phys. Ther. 2010, 34, 94–97. [Google Scholar] [CrossRef] [PubMed]
- Nada, E.H.; Ibraheem, O.A.; Hassaan, M.R. Vestibular rehabilitation therapy outcomes in patients with persistent postural-perceptual dizziness. Ann. Otol. Rhinol. Laryngol. 2019, 128, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Appiah-Kubi, K.; Wright, W. Vestibular training promotes adaptation of multisensory integration in postural control. Gait Posture 2019, 73, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Appiah-Kubi, K.O.; Galgon, A.; Tierney, R.; Lauer, R.; Wright, W.G. Effects of Vestibular Training on Postural Control of Healthy Adults. Common Health 2020, 1, 31–36. [Google Scholar] [CrossRef] [Green Version]
- Viziano, A.; Micarelli, A.; Augimeri, I.; Micarelli, D.; Alessandrini, M. Long-term effects of vestibular rehabilitation and head-mounted gaming task procedure in unilateral vestibular hypofunction: A 12-month follow-up of a randomized controlled trial. Clin. Rehabil. 2019, 33, 24–33. [Google Scholar] [CrossRef]
- Song, J.J. Virtual reality for vestibular rehabilitation. Clin. Exp. Otorhinolaryngol. 2019, 12, 329–330. [Google Scholar] [CrossRef]
- Matsumura, M.; Murofushi, T. Vestibular Rehabilitation after Vestibulopathy Focusing on the Application of Virtual Reality. J. Otorhinolaryngol. Hear. Balance Med. 2021, 2, 5. [Google Scholar] [CrossRef]
- Kinne, B.L.; Owens, K.J.; Rajala, B.A.; Ticknor, S.K. Effectiveness of home-based virtual reality on vestibular rehabilitation outcomes: A systematic review. Phys. Ther. Rev. 2019, 24, 280–290. [Google Scholar] [CrossRef]
- Xie, M.; Zhou, K.; Patro, N.; Chan, T.; Levin, M.; Gupta, M.K.; Archibald, J. Virtual reality for vestibular rehabilitation: A systematic review. Otol. Neurotol. 2021, 42, 967–977. [Google Scholar] [CrossRef]
- Chu, H.Y.; Song, N.; Li, Z.F.; Zhou, Z.R.; Yang, X. Can virtual reality-assisted therapy offer additional benefits to patients with vestibular disorders compared with conventional vestibular physical therapy? A meta-analysis. Arch. Phys. Med. Rehabil. 2022, in press, pre-proof version. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- MacDougall, H.G.; Weber, K.P.; McGarvie, L.A.; Halmagyi, G.M.; Curthoys, I. The video head impulse test: Diagnostic accuracy in peripheral vestibulopathy. Neurology 2009, 73, 1134–1141. [Google Scholar] [CrossRef] [Green Version]
- Stegeman, D.F.; Hermens, H.J. Standards for surface electromyography: The European project “Surface EMG for non-invasive assessment of muscles (SENIAM)”. Enschede Roessingh Res. Dev. 2007, 10, 8–12. [Google Scholar]
- Robins, R.K.; Hollands, M.A. The effects of constraining vision and eye movements on whole-body coordination during standing turns. Exp. Brain Res. 2017, 235, 3593–3603. [Google Scholar] [CrossRef]
- Ross, A.I.; Schenk, T.; Hesse, C. The effect of gaze position on reaching movements in an obstacle avoidance task. PLoS ONE 2015, 10, e0144193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shumway-Cook, A.; Horak, F.B. Assessing the influence of sensory interaction on balance: Suggestion from the field. Phys. Ther. 1986, 66, 1548–1550. [Google Scholar] [CrossRef]
- Carpenter, M.G.; Allum, J.H.J.; Honegger, F. Directional sensitivity of stretch reflexes and balance corrections for normal subjects in the roll and pitch planes. Exp. Brain Res. 1999, 129, 93–113. [Google Scholar] [CrossRef]
- Chen, C.-L.; Lou, S.-Z.; Wu, H.-W.; Wu, S.-K.; Yeung, K.-T.; Su, F.-C. Effects of the type and direction of support surface perturbation on postural responses. J. Neuroeng. Rehabil. 2014, 11, 50. [Google Scholar] [CrossRef] [Green Version]
- Keshner, E.A.; Woollacott, M.H.; Debu, B. Neck, trunk and limb muscle responses during postural perturbations in humans. Exp. Brain Res. 1988, 71, 455–466. [Google Scholar] [CrossRef]
- Wright, W.G.; McDevitt, J.; Tierney, R.; Haran, F.J.; Appiah-Kubi, K.O.; Dumont, A. Assessing subacute mild traumatic brain injury with a portable virtual reality balance device. Disabil. Rehabil. 2017, 39, 1564–1572. [Google Scholar] [CrossRef] [PubMed]
- Marchetto, J.; Wright, W.G. The validity of an oculus rift to assess postural changes during balance tasks. Hum. Factors 2019, 61, 1340–1352. [Google Scholar] [CrossRef] [PubMed]
- McCall, A.A.; Yates, B.J. Compensation Following Bilateral Vestibular Damage. Front. Neurol. 2011, 2, 88. [Google Scholar] [CrossRef] [Green Version]
- Herdman, S.J. Vestibular rehabilitation. Curr. Opin. Neurol. 2013, 26, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Horak, F.B.; Nutt, J.G.; Nashner, L.M. Postural inflexibility in parkinsonian subjects. J. Neurol. Sci. 1992, 111, 46–58. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
VOR gain testing using the ICS impulse system.

Figure 2.
Toes-up and -down ramp perturbation trajectories of a participant. A–B: Time between the ramp onset to the max peak, reflecting the biomechanical effects of the platform perturbation (reversal for ramp down trials). B–C: Time between max peak and min peak, reflecting the reflexive response (reversal for ramp down trials). This is the automatic postural response (APR). C–D: Time between min peak and next max peak, reflecting postural corrective adjustment (reversal for ramp down trials).
Figure 2.
Toes-up and -down ramp perturbation trajectories of a participant. A–B: Time between the ramp onset to the max peak, reflecting the biomechanical effects of the platform perturbation (reversal for ramp down trials). B–C: Time between max peak and min peak, reflecting the reflexive response (reversal for ramp down trials). This is the automatic postural response (APR). C–D: Time between min peak and next max peak, reflecting postural corrective adjustment (reversal for ramp down trials).

Figure 3.
Training. (Left); VR HS-WST showing participant with VR headset and leaning in eight different directions. (Right); Training modules (A, B, C) showing each of the six exercises (a–f; 18 in total) with targets that would randomly change every 4 s, in which a participant would move his/her COM to reach. Targets in training modules (A, B, C) of similar exercises (a–f) differ by 70% limits of stability (LOS) and 90% LOS. Exercises will be performed on stable (SS) or foam (FS) surfaces and with or without headshake (HS). Each of the exercises (a–f) has two to seven targets that have been selected from the original eight directional targets. Each of the 18 exercises will last for 1 min.
Figure 3.
Training. (Left); VR HS-WST showing participant with VR headset and leaning in eight different directions. (Right); Training modules (A, B, C) showing each of the six exercises (a–f; 18 in total) with targets that would randomly change every 4 s, in which a participant would move his/her COM to reach. Targets in training modules (A, B, C) of similar exercises (a–f) differ by 70% limits of stability (LOS) and 90% LOS. Exercises will be performed on stable (SS) or foam (FS) surfaces and with or without headshake (HS). Each of the exercises (a–f) has two to seven targets that have been selected from the original eight directional targets. Each of the 18 exercises will last for 1 min.

Figure 4.
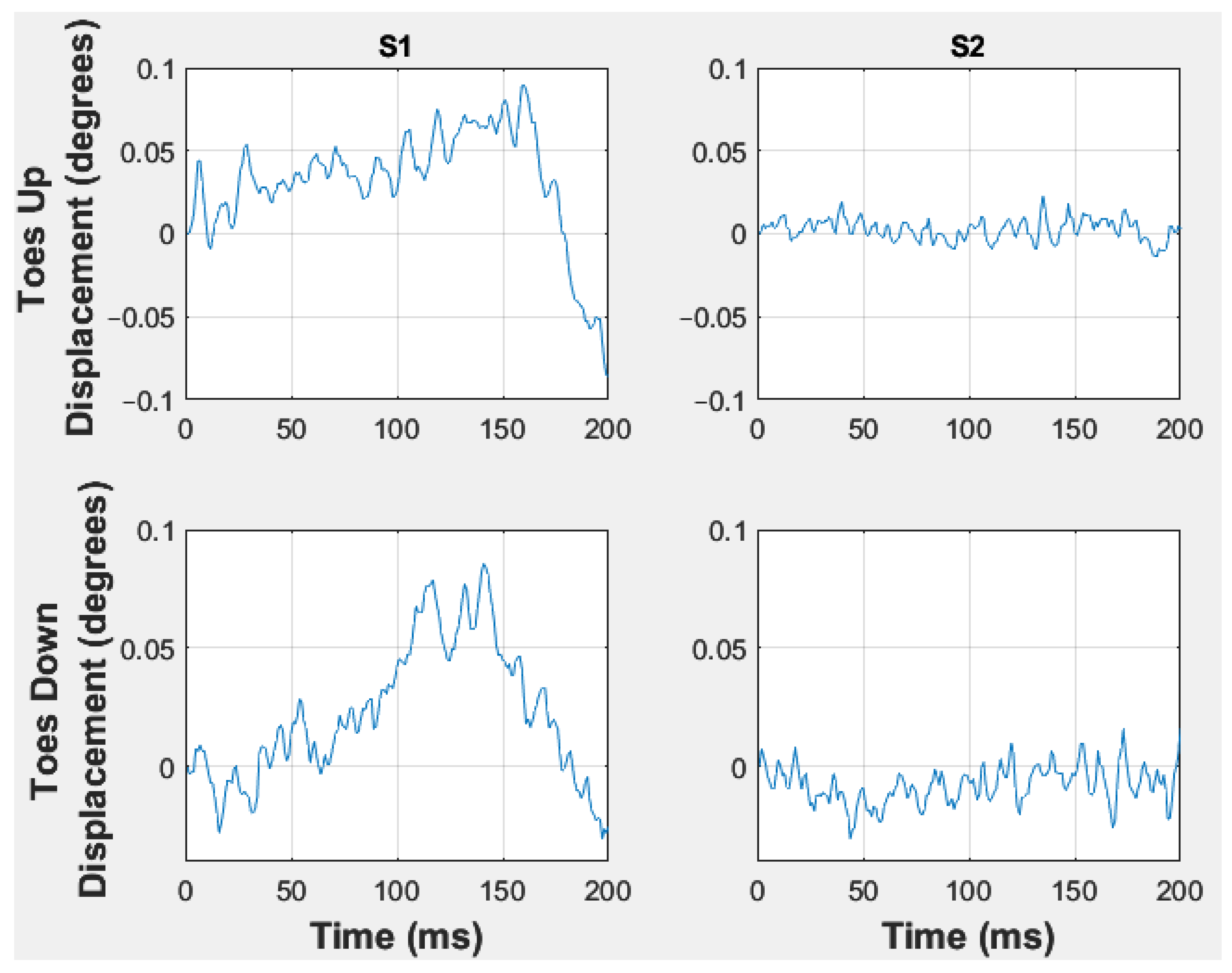
Horizontal eye movement. Representative data of the horizontal eye movements of a participant performing balance assessment on the force plate perturbation device. S1 = pre-assessment, S2 = post-assessment.
Figure 4.
Horizontal eye movement. Representative data of the horizontal eye movements of a participant performing balance assessment on the force plate perturbation device. S1 = pre-assessment, S2 = post-assessment.

Figure 5.
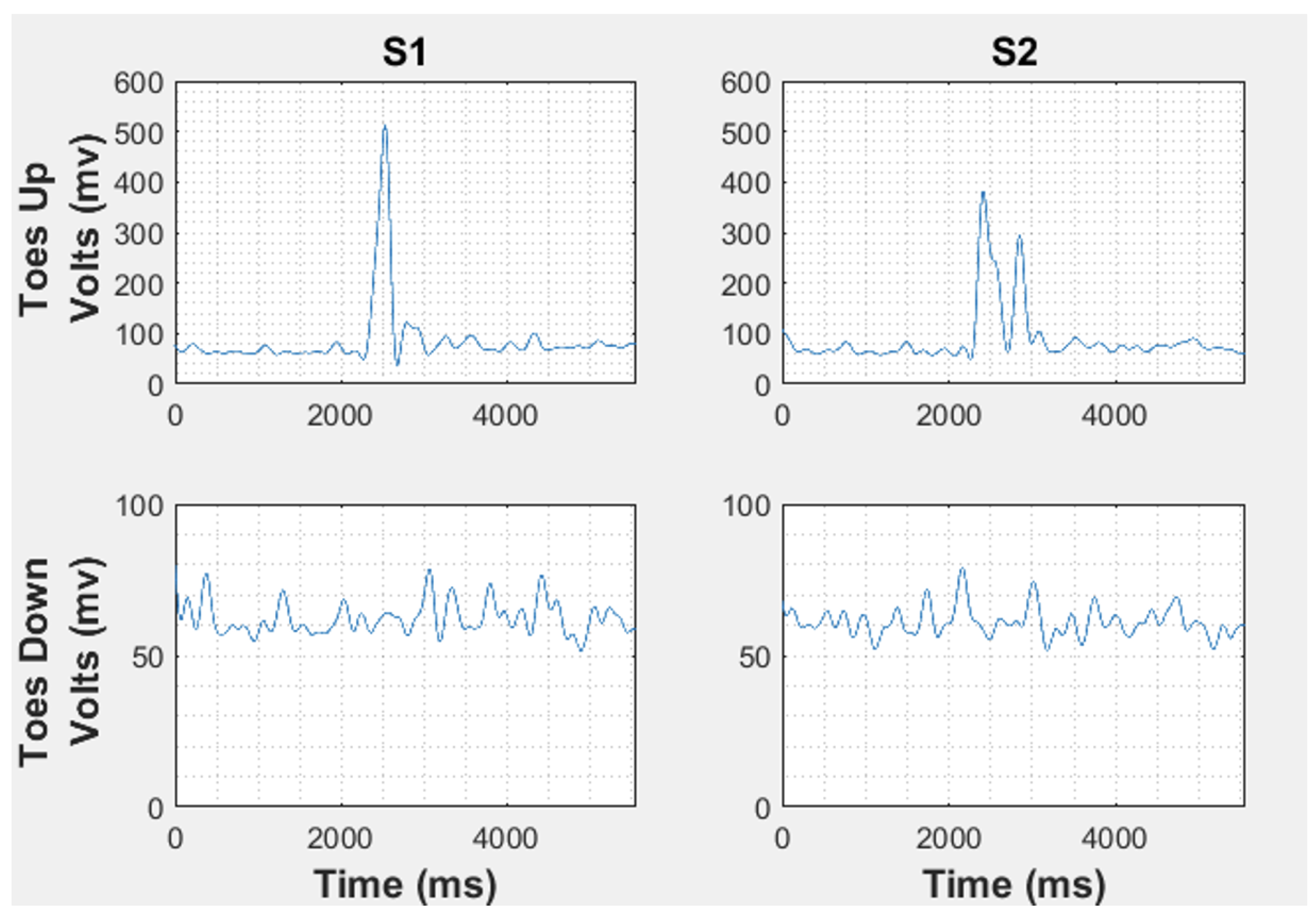
EMG amplitude. Representative data of the right gastrocnemius activation of a participant performing balance assessment on the force plate perturbation device. S1 = pre-assessment, S2 = post-assessment.
Figure 5.
EMG amplitude. Representative data of the right gastrocnemius activation of a participant performing balance assessment on the force plate perturbation device. S1 = pre-assessment, S2 = post-assessment.

Figure 6.
COP path length. Representative data of a participant performing balance assessment on the force plate perturbation device. S1 = pre-assessment, S2 = post-assessment.
Figure 6.
COP path length. Representative data of a participant performing balance assessment on the force plate perturbation device. S1 = pre-assessment, S2 = post-assessment.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Review of the related literature.
| Study | Purpose and Contribution of the Study |
|---|---|
| Appiah-Kubi & Wright [15] | Assessment of sensory reweighting of postural control processing after combined vestibular activation with voluntary weight shift training. Improvements in somatosensory reweighting, center of pressure (COP) multiscale entropy sway velocity, and COP mediolateral standard deviation sway. |
| Appiah-Kubi et al. [16] | Assessment of vestibular and motor responses following concurrent vestibular and balance training. Significant changes in VOR gain, eye fixation, refined muscle activation, and postural flexibility. |
| Viziano et al. [17] | Evaluation of virtual reality-based vestibular rehabilitation in unilateral vestibular dysfunction. Significantly higher VOR gain, improved posturography scores, and better reduction in dizziness scores in the virtual reality-based vestibular rehabilitation group compared to the traditional vestibular rehabilitation group. |
| Song [18] | A short review of the efficacy of VR to enhance vestibular rehabilitation. The use of VR devices in vestibular rehabilitation motivates participants to enjoy the training, increase their concentration, and decreases the dropout rate, as well as helps individuals with visual vertigo. |
| Matsumura & Murofushi [19] | A review of vestibular rehabilitation (VeR) for BVP (Bilateral vestibulopathy) and VeR using VR to increase vestibuloocular reflex gain and decrease dizziness. |
| Kinne et al. [20] | A systematic review to investigate the effectiveness of VR-based vestibular rehabilitation. The addition of VR to vestibular rehabilitation showed equal benefits in individuals with vestibular dysfunction and may be more beneficial than traditional rehabilitation alone. |
| Xie et al. [21] | A systematic review of the effectiveness of VR-based vestibular rehabilitation. Evidence suggests that there are clinical benefits in VR-based vestibular rehabilitation. |
| Chu et al. [22] | A meta-analysis to assess the advantages of VR-based vestibular rehabilitation over traditional vestibular rehabilitation. VR-based vestibular rehabilitation is suggested to demonstrate additional clinical benefits to vestibular dysfunction, especially to those with peripheral disorders. |
Table 2.
Training Schedule.
| GROUP | DAY | |||||||||||||||
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | |
| 1 | A T | T | T | T | T | T A | A WO | A WO | WO | WO | A NT | NT | NT | NT | NT | A NT |
| 2 | A NT | NT | NT | NT | NT | A NT | A WO | A WO | WO | WO | A T | T | T | T | T | T A |
| A = Assessment, NT = No training, T = Training, WO = Washout period | ||||||||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Appiah-Kubi, K.O.; Laing, E.; Imtiaz, M.H. A Study Protocol to Evaluate the Effects of Vestibular Training on the Postural Control of Healthy Adults Using Virtual Reality. Appl. Sci. 2022, 12, 11937. https://doi.org/10.3390/app122311937
AMA Style
Appiah-Kubi KO, Laing E, Imtiaz MH. A Study Protocol to Evaluate the Effects of Vestibular Training on the Postural Control of Healthy Adults Using Virtual Reality. Applied Sciences. 2022; 12(23):11937. https://doi.org/10.3390/app122311937
Chicago/Turabian StyleAppiah-Kubi, Kwadwo O., Evan Laing, and Masudul H. Imtiaz. 2022. "A Study Protocol to Evaluate the Effects of Vestibular Training on the Postural Control of Healthy Adults Using Virtual Reality" Applied Sciences 12, no. 23: 11937. https://doi.org/10.3390/app122311937
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.