
The Application of a 3-Dimensional Printing Technique in Refining the Orthodontic Trans-Palatal Arch


1
College of Stomatology, Chongqing Medical University, Chongqing 400016, China
2
Chongqing Key Laboratory for Oral Diseases and Biomedical Sciences, Chongqing 401147, China
3
Chongqing Municipal Key Laboratory of Oral Biomedical Engineering of Higher Education, Chongqing 401147, China
*
Authors to whom correspondence should be addressed.
†
These authors contributed equally to this work.
Appl. Sci. 2022, 12(15), 7497; https://doi.org/10.3390/app12157497
Submission received: 26 April 2022
/
Revised: 15 July 2022
/
Accepted: 23 July 2022
/
Published: 26 July 2022
(This article belongs to the Topic State-of-the-Art Dentistry and Oral Health)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:The aim of this article was to describe the process of designing and manufacturing 3D TPAs and to discuss some clinical cases in which 3D TPAs were used. Digital models were acquired by scanning the casts, scanning the PVS impressions or scanning the dentitions directly. The scanning data in a common STL format was used for the computer design that follows. Then, the design instructions were sent to a 3D printer for fabrication. Finally, manual polishing should be performed. Seven clinical cases in which 3D TPAs were used to assist orthodontic treatment were presented and discussed. The presented clinical cases demonstrated that the 3D TPA was a simple, convenient appliance for the patient and the doctor, and thus, might be more cleansable. The 3D TPA could be designed in different types based on the clinical needs of each case. The application of 3D TPA could be expanded, but clinical trials are necessary to verify the advantages reported here.
1. Introduction
Advancements in digital technology have moved diagnosis and treatment planning from a two-dimensional (2D) age into a three-dimensional (3D) age. The innovative digital technique of 3D printing, also known as additive fabrication is more and more popular in medical fields. It has numerous advantages, including cost-effectiveness, improved quality control, speed and accuracy; and reduced labor [1,2]. In brief, 3D printing is a Computer-Aided Manufacturing (CAM) technique; it is a method that uses 3D Computer-Aided Design (CAD) datasets to produce 3D physical objects by the addition of material layers [3]. Its first medical application was the production of a model of cranial bony anatomy from CT image data in 1990; the constructed model provided full internal anatomical details [4]. Over the past few years, 3D techniques have become a preferred method for many dentists. Simultaneously, an ever-increasing variety of 3D products are becoming available in the fields of prosthodontics [5], oral and maxillofacial surgery [6], dental implantation [7], and, in particular, orthodontics [8,9,10,11,12,13,14] _ENREF_10_ENREF_8_ENREF_9. Orthodontics is keeping pace with the trend of 3D printing. Over the last decade, orthodontists have applied 3D printing to the fabrication of orthodontic appliances, such as customized lingual/labial brackets and arch wires [8,9], 3D-printed retainers [10,11], transparent aligners [12], digital titanium Herbst devices [13] and 3D-printed hyrax devices [14]. However, there are still some traditional orthodontic appliances that have yet to be digitalized, such as transpalatal arches (TPAs), Nance palatal arches, molar distalization appliances, maxillary protraction appliances and so on.
TPAs might be one of the most commonly used intraoral auxiliary fixed appliances in orthodontics [15]. The reason for this is that TPAs have a range of applications, and can be used in anchorage support, vertical control [15,16], transverse maintaining [15,17], the correction of buccally placed maxillary molars [18,19,20,21], molar intrusion [22,23], molar distalization [24,25] and even maxillary expansion [26,27]. However, traditional TPAs have some disadvantages that should not be overlooked, such as complicated workflow (which comprises teeth separation, band try-in, steel-wire bending, welding and so on), contraindications (a large cusp of Carabelli and a short crown), health problems (residual adhesives, gingival injury and gingivitis), patient discomfort (including long waiting times and uncomfortable fitting process). In order to overcome the shortcomings of traditional TPAs, efforts should be made to explore the possibility of manufacturing 3D-printed TPAs (3D TPAs) to refine the TPA techniques used both in clinics and laboratories.
Therefore, the aim of this article was to describe the process of designing and manufacturing 3D TPAs and to discuss some clinical cases in which 3D TPAs were used. It is hoped that the information provided in this study will fuel future research into 3D printing in orthodontics.
2. Materials and Methods
2.1. Acquisition of Digitized Dental Models
Digital models can be created using different methods, depending on the conditions of the clinic and the preferences of doctors or patients. The main methods are summarized as follows:
- (1)
- Impressions of the patient’s dentition are taken using routine impression materials; plaster casts are made and scanned with a SHINING 3D scanner (SHINING 3D, Hangzhou, China).
- (2)
- Impressions of the patient’s dentition are taken with polyvinyl siloxane (PVS) materials; the PVS impressions are scanned with a SHINING 3D scanner (SHINING 3D, China).
- (3)
- The dentitions are scanned directly using oral scanners.
The scanning data in a common STL format was used for the computer design process that follows.
2.2. Computer-Aided Design and 3D Printing
Dedicated high-performance workstations equipped with image processing software (3-matic STL software (version 10.2; Materialise, Leuven, Belgium)) and Concept Laser M lab (Concept Laser, Lichtenfels, Germany) were used to design and manufacture the appliance_ENREF_26_. The 3-matic software was used to design personalized 3D TPA. Specifically, with the assistance of the markup command, a preliminary 2D sketch of the TPA was constructed. The sketch was then expanded to a 3D orthodontic appliance by the WRAP operation. The 3D appliance was well matched with teeth through the Boolean operation. Some key principles of design are summarized as follows:
- (1)
- The undercut areas are analyzed to determine the appropriate path of insertion of the 3D TPAs.
- (2)
- To the greatest extent possible, the metal plate should be designed over the undercut line.
- (3)
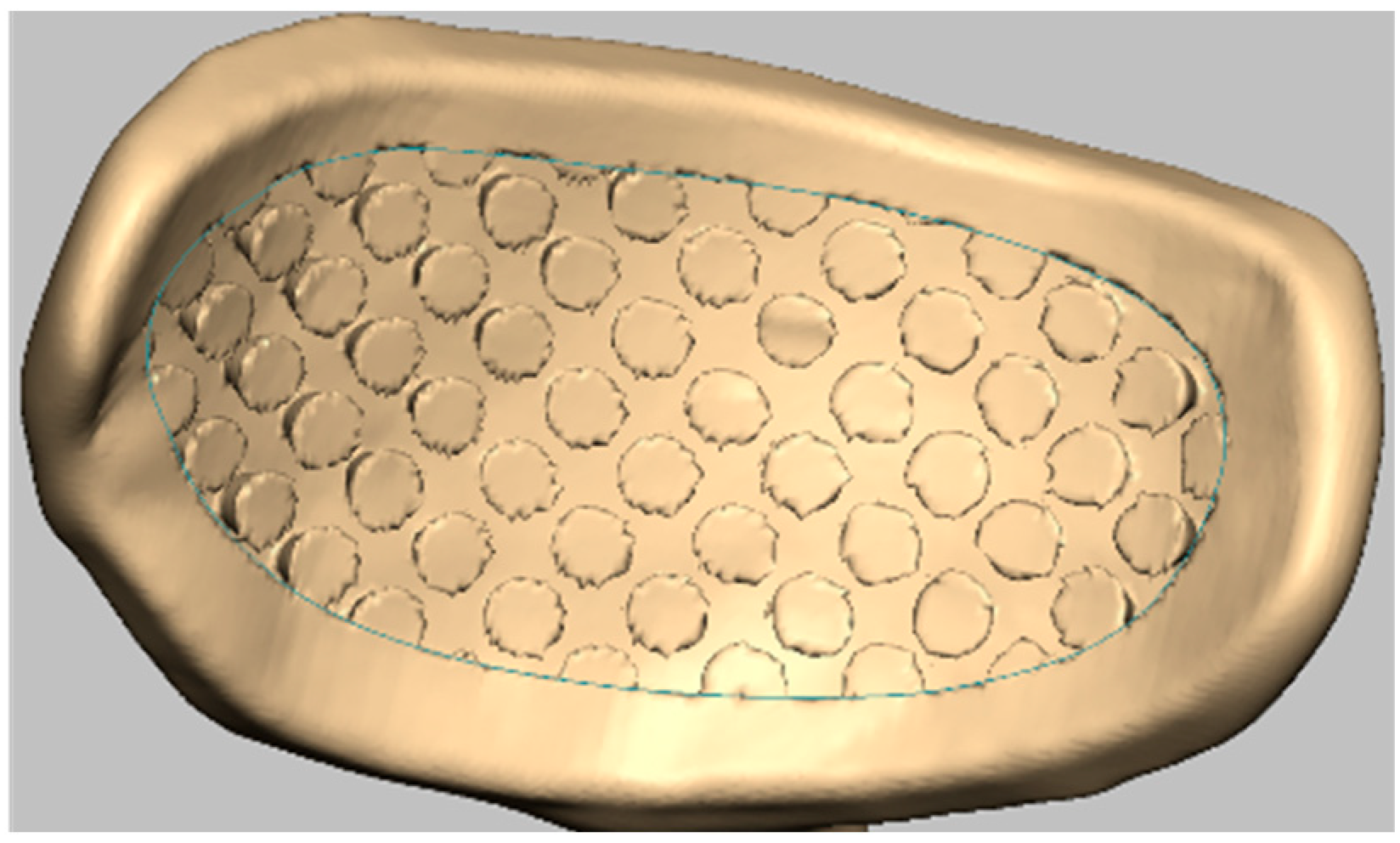
- The adhesive surface was modified with the undercut (Figure 1). The adhesive surface was an orthodontic bracket data provided by Jing Mei dental center (Chongqing, China).
- (4)
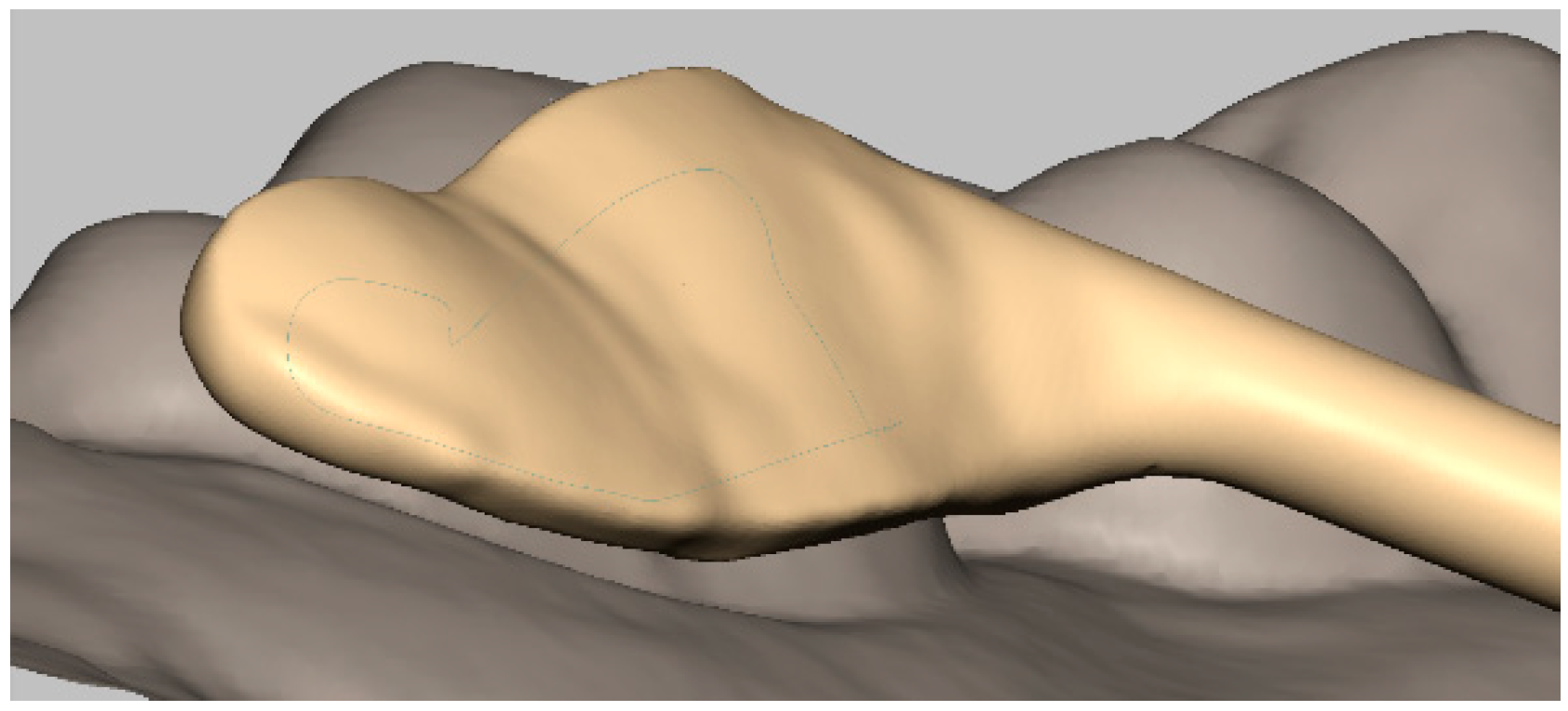
- The distance from the gingival margin to the plate margin should measure more than 1.5 mm to maintain a suitable and healthy gingival condition (Figure 2).
- (5)
- Care should be taken to avoid occlusal interferences.
- (6)
- The shape of the metal bar, the distance from the bar to the palatal mucosa and the affiliated apparatus are designed according to both the clinician’s preference and the nature of the malocclusion.
After completion of the CAD phase, design instructions are sent to a Concept Laser M lab (Concept Laser, Germany) for fabrication. The TPA is manufactured by selective laser melting (SLM) and the metal used for manufacturing is Titanium alloy powder (Dentaurum, Ispringen, Germany). During the process of 3D printing, the machine reads data from a CAD drawing and lays down successive layers of titanium alloy powder, and, in this way, builds up a model from a series of cross sections. These layers, which correspond to the virtual cross section from the CAD model, create the final shape when joined together.
The acrylic buttons are manually added according to the clinical needs.
Manual polishing should then be performed; during this final step, attention should be paid to avoid damaging the adhesive surface.
2.3. Bonding of 3D TPAs
Reinforced glass ionomer (GC Fuji Ortho LC, GC Corporation, Tokyo, Japan) is used to bond 3D TPA on the lingual surface of the teeth. Briefly, lingual surfaces of teeth are etched with 37% phosphoric acid for 30 s. The etching area should be similar to the area of bonding plates. Then, teeth are washed with clean water for 10 s and dried with clean air for 30 s. Finally, a moderate reinforced glass ionomer is spread on the bonding plates and the plates attached to the teeth. Excessive reinforced glass ionomer should be removed from the margin of the lingual plate.
3. Clinical Application
3.1. Case 1
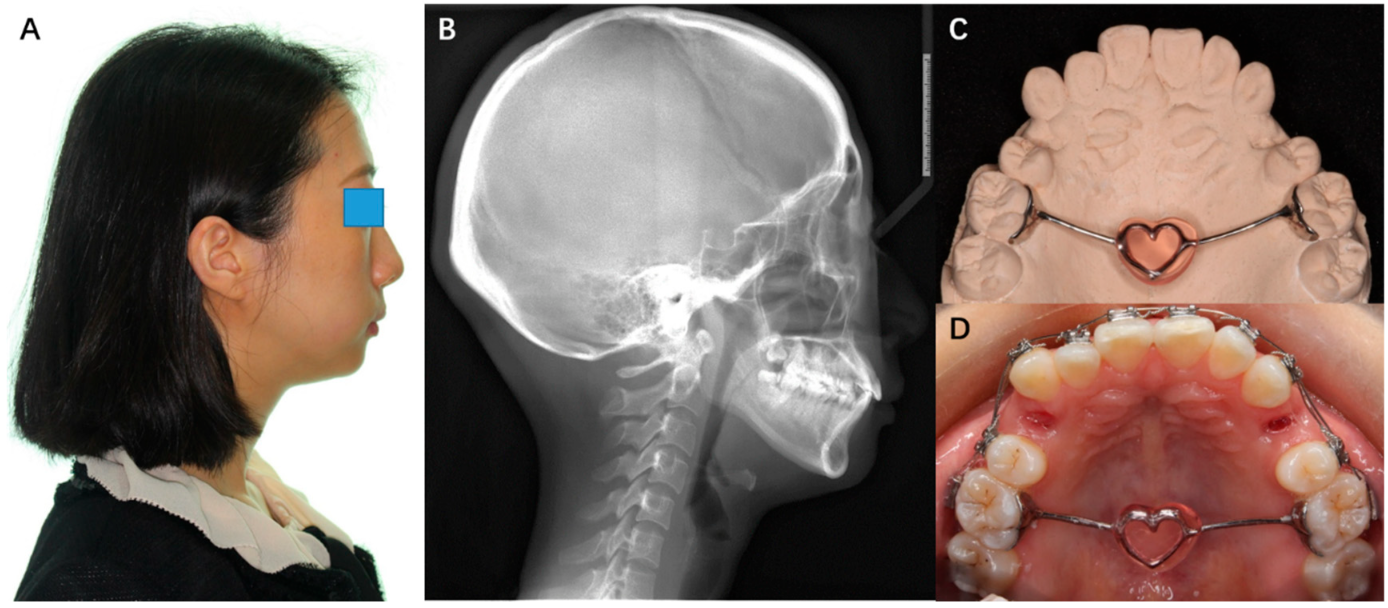
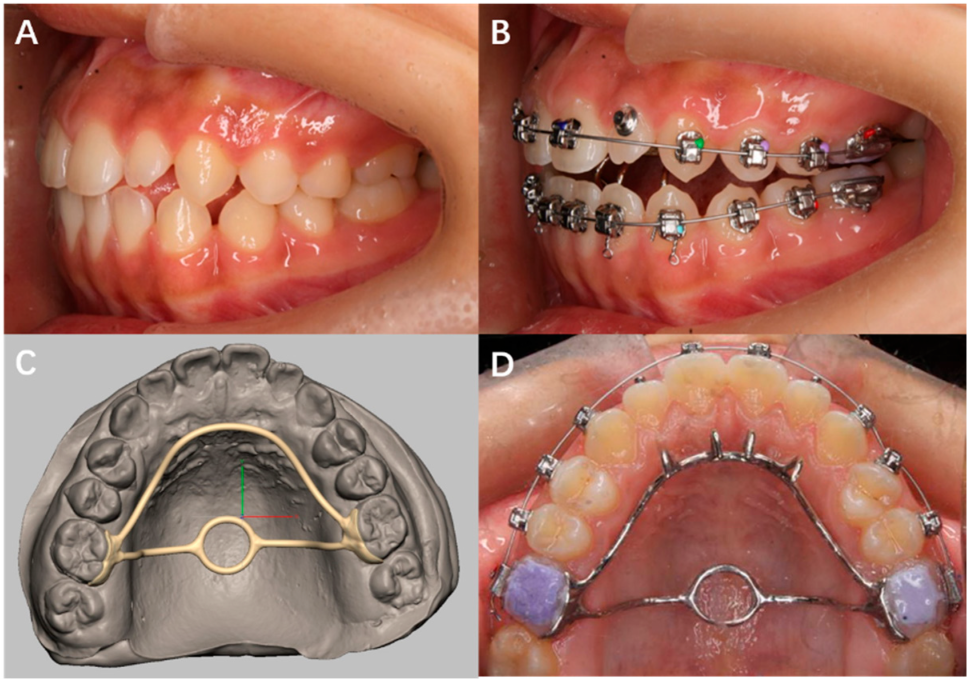
A patient was diagnosed with skeletal class II and high-angle malocclusion (Figure 3A,B). A TPA was needed to control the vertical height of the molars. The doctor chose a 3D TPA (China patent no. ZL 2017 2 0580517.1) for the patient. Digitized dental models were acquired by scanning the casts. The bar of the 3D TPA was designed to be heart-shaped according to the patient’s preference (Figure 3C,D).
3.2. Case 2
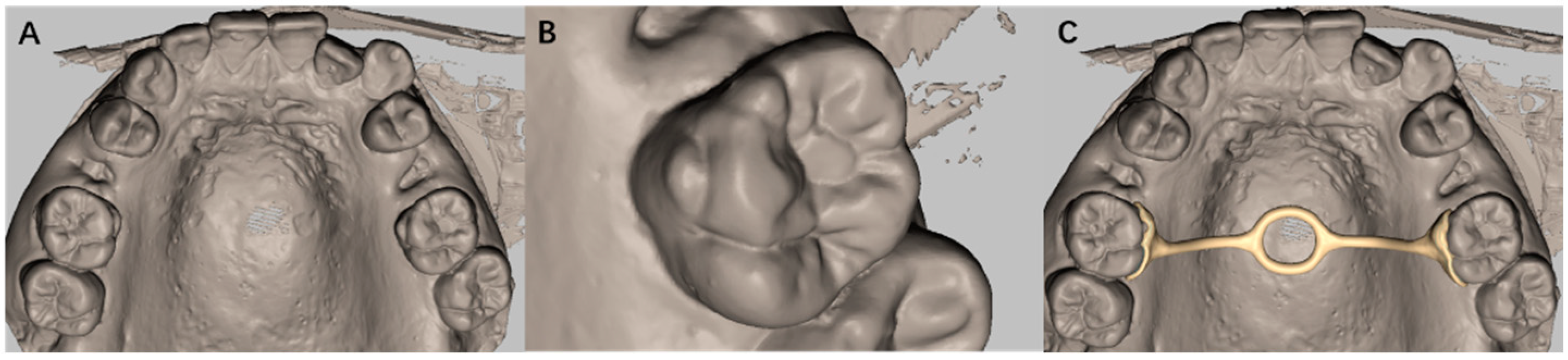
A patient presented with a large Carabelli cusp on the first upper molar (Figure 4A,B). A TPA was necessary for anchorage control and vertical control. However, a traditional TPA with a metal band was not suitable, because the prefabricated band was difficult to insert. Digitized dental models were acquired by scanning the casts. As such, the clinician recommended a 3D TPA (Figure 4C), which neatly fitted the surface of the Carabelli cusp.
3.3. Case 3
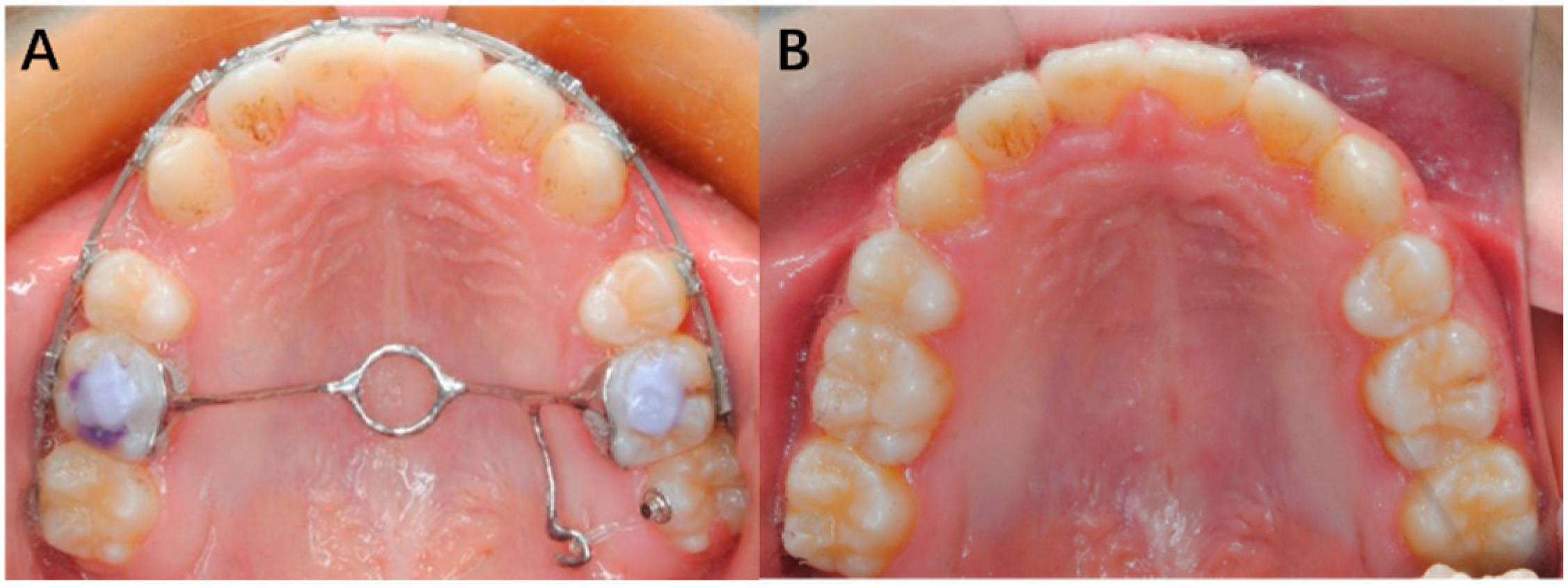
A patient was diagnosed with an open bite after all teeth were aligned (Figure 5A). To achieve vertical control, the doctor decided to use a TPA. To make a traditional TPA, the buccal tube should be debonded. It can be difficult to precisely position the metal band and in such a way as to ensure the correct positioning of the buccal tube. Therefore, digitized dental models were acquired by scanning the casts. The clinician chose a 3D TPA (Figure 5B), which would not affect the position of the already-aligned teeth. Finally, the open bite was successfully corrected (Figure 5C).
3.4. Case 4
A patient was diagnosed with a high MP-FH (Figure 6A), a protruded profile (Figure 6B) and a conspicuous open bite (Figure 6C). Both the first and second molars should be intruded to correct the malocclusion. Digitized dental models were acquired by scanning the casts. The doctor designed a 3D TPA (Figure 6D,E), connecting the first and second molars, to intrude both simultaneously and prevent the molars from inclining buccally; this was combined with mini implant anchorages.
3.5. Case 5
A patient was diagnosed with a habit of tongue thrusting, shallow overjet and an overbite (Figure 7A). A TPA was necessary to control the vertical height of the molars, and palatal bars were proposed as a method for correcting the posture of the tongue. Digitized dental models were acquired by scanning the casts. The doctor designed a 3D TPA that was modified with palatal thorns in order to achieve both vertical control and habit breaking (Figure 7C,D). The thorns were soldered for easy adjustment. After the 3D TPA modified with palatal thorns was affixed, the habit of tongue thrusting was immediately restricted (Figure 7B).
3.6. Case 6
A patient had a buccally flared maxillary second molar (Figure 8A). Digitized dental models were acquired by scanning the casts. The clinician designed a 3D TPA with a lateral arm to correct the flared teeth (Figure 8A). As shown in our previous Biomechanical study [28], in the buccolingual direction, the crown of the buccally flared maxillary second molar had an inclination of lingual displacement and the root had an inclination of buccal displacement. Moreover, in the vertical direction, the second molar showed a general inclination of intrusion movement. Finally, the second molar was aligned using the 3D TPA with a lateral arm (Figure 8B).
3.7. Case 7
A patient wanted to wear lingual brackets, but a palatally malposed canine restricted the use of lingual brackets and arch wires. Therefore, the malposed canine needed to be corrected before bonding the lingual brackets. To correct the malposed canine, digitized dental models were acquired by scanning the casts. Then the clinician designed a 3D TPA with a lateral hook to pull the canine (Figure 9A,B). Finally, the malposed canine was corrected, the lingual brackets were boned, and the lingual arch wires were successfully applied (Figure 9C).
4. Discussion
The primary advantage of 3D printing is its ability to create almost any complex shape or geometric feature, which has allowed for its widespread application in dentistry. In orthodontics, 3D printing has been used to fabricate customized brackets [8,9] and transparent aligners [12]; moreover, there has been a gradual increase in its use for fabricating orthodontic accessories, such as digital titanium, Herbst [13], and 3D-printed hyrax devices [14]. In this study, we further expanded the application of 3D printing in orthodontics and explored its benefits as a method that simplifies the treatment process, enhances the treatment outcomes, and reduces patient discomfort.
TPA is commonly used in orthodontics because it has many functions relevant to orthodontic treatments [16,17,18,19,20,21,22,23,24,25,26,27] _ENREF_19. Unfortunately, traditional TPA has some disadvantages and contraindications. Therefore, efforts have been made to use the advantages of 3D printing to refine TPA and overcome these shortcomings. It is well known that only reliable retention of appliances can ensure favorable expressions of orthodontic force. However, a traditional TPA may sometimes become detached from the teeth due to the limitations of its structure. Usually, traditional TPA is composed of metal bands and bars. The metal band is prefabricated rather than customized, which is not suitable for some situations, such as when the patient presents with a deep undercut, a large cusp of Carabelli as shown in the second case with a short crown. Sometimes, the band cannot fit the tooth surface very well, which may result in a big gap between the band and the tooth; in this instance, when bonding the TPA, the gap is filled with a large number of adhesives. In addition to this, the inner surface of the band is smooth. Altogether, these disadvantages can potentially compromise the final bonding effect. To solve these problems, a customized lingual plate with an undercut-modified adhesive surface (see Figure 2) was designed. Because the plate was personalized, it fitted the surface of the tooth very well regardless of the anomalous shape of the teeth, which ensured that only a thin layer of the adhesive was required between the teeth and plate. The undercut enhanced the connection between the adhesive and the plate. Therefore, the 3D-printed plate might result in a better bonding effect than a traditional metal band. It is worth noting that, the enhanced adhesive strength remains a subjective assumption; as such, extensive experiments on adhesive strength and clinical trials on appliance loosening are necessary to verify the bonding effect of 3D TPAs.
In addition to potentially improving the reliability of bonding and retention, 3D TPA might also be healthier and more comfortable. To ensure good retention, traditional TPAs are sometimes inserted close to the gingival margin or deep into the gingival sulcus, which might be harmful to gingival health. In contrast, 3D TPA can be inserted at least 1.5 mm away from the gingiva, which might make it easier for clinicians to thoroughly remove excess adhesive when bonding the 3D TPA; it, therefore, represents a more hygienic alternative to traditional TPAs. Additionally, traditional TPAs encompass four surfaces, including the buccal surface, the lingual surface, and two proximal surfaces, which can lead to gaps between teeth after debonding. As such, patients might sometimes complain of food impactions after removing their traditional TPAs. In contrast, 3D TPA only attaches to the lingual surface and not the proximal surface, which might reduce the possibility of proximal gaps and food impactions. Overall, in theory, 3D TPA has the potential to reduce periodontal complications and enhance patient comfort. However, further clinical trials should be conducted, focusing on periodontal indices such as the gingival index and sulcus bleeding index, and on patient feelings.
Moreover, the application of the 3D printing technique might reduce clinicians’ and technicians’ workloads because the workflow of 3D TPA is simpler than that of traditional TPA. In summary, to fabricate a traditional TPA, the teeth are routinely separated, and the bands are tied in, then an impression is made. Before pouring casts, it is necessary to check whether the bands were correctly localized in the impression. Sometimes, the bands are very tight on the teeth but not in the impression; in these cases, the band needs to be repositioned in the impression, which might compromise accuracy. In contrast, the process of acquiring digital models to design and fabricate 3D TPAs might be simpler than using plaster casts. During the design and manufacture process, traditional TPAs require a bar to be manually bent; then, the bars are positioned manually and soldered to the bands. It has been reported that there is a great likelihood of inaccurate placement and soldering defects when this technique is used [13]. In contrast, the plates and the bars of 3D TPAs are designed virtually by technicians using computers; then, the digital TPAs are sent to the printers for manufacture. The 3D TPAs might provide better stability than traditional TPAs because of their exact fit, discrepancies between the finished product and the virtual design are in the order of 10–30 microns, and no soldering defects would appear during the printing phase. In addition, 3D TPA has some advantages over traditional TPA during the bonding phase. When bonding traditional TPA, it might be difficult to precisely locate the band to ensure the correct positioning of the buccal tube. Sometimes, an auxiliary appliance is necessary to press the band in place; this pressure might distort the band, further compromising the accuracy of the buccal tube. In contrast, the process of bonding 3D TPAs is easier and more labor-saving and time-saving. In brief, the lingual surface is etched according to the designed bonding area, then, the TPA is bonded with light-cure adhesive. Moreover, the adhesive plates are attached to the lingual side of the teeth and do not implicate the buccal side. Therefore, it is easier to precisely locate the buccal tube or the brackets on the buccal side, and their positions are not affected by the 3D TPA, as shown in cases 3–6. Although the manufacturing and clinical application of 3D TPAs seem to require fewer steps than that of traditional TPAs, further investigations should be conducted to examine technicians’ and doctors’ responses to this technique.
The greatest advantage of 3D TPA might be that the design of appliances can be adapted according to the clinician’s preferences. The CAD technology allows the clinicians’ ideas to be precisely specified during the design phase, taking into account factors such as the number of teeth included, the distance from the bar to the palatal mucosa, the need for affiliated hooks, and so on. Moreover, the treatment order is very flexible. The matter of when 3D TPAs should be worn depends on the phase of treatment and the preferences of doctors. For example, if the target teeth were irregular and not suitable for TPA bonding, the buccal tube or bracket could first be bonded to align the teeth. After the target teeth were aligned, the digital model can be acquired to manufacture the 3D TPA. It is worth mentioning that, in order to expand the application of 3D TPAs, more highly standardized and efficient designing, manufacturing and application processes should be established.
Since 3D TPA has advantages over traditional TPA in terms of bonding strength, patient health and comforts, workflow and design flexibility, the use of 3D TPA represents a viable alternative technique. At the same time, however, 3D TPA has some limitations that should not be ignored. First, the price of the appliance was higher than that of traditional TPA because of the high costs associated with 3D printing such as the purchase of advanced equipment and software, the training of professional technicians and the demand for laboratory space. However, we expect the price to be reduced as demand increases. Second, the 3D TPAs cannot bear some adjustments. However, if the affiliated apparatus of 3D TPAs need to be adjusted, they could be welded to the 3D TPAs, like the thorns in Case 5. Third, the advantages of 3D TPA over traditional TPA are largely speculative, and, as of yet, have not been verified by well-designed experiments and clinical trials.
Considering the advantages and disadvantages of 3D TPA discussed above, clinicians should decide whether or not to use a 3D TPA by weighing up the costs that patients can afford with the benefits that patients and clinicians may derive from this method.
5. Conclusions
The use of 3D technology has the potential to make the design and manufacturing of TPAs simpler, faster and more accurate. The 3D TPA might have the benefits of enhanced adhesive strength, improved periodontal health and increased convenience for the patient. Therefore, the application of 3D TPA could be expanded, despite the increased associated costs, but clinical trials are necessary to verify the advantages reported here.
Author Contributions
Conceptualization, J.S. and L.H.; methodology, Y.K. and B.H.; writing—original draft preparation, Y.K.; writing—review and editing, B.H. and G.F.; supervision, J.S. and L.H.; case collection, L.H. and G.F.; funding acquisition, J.S. and L.H. All authors have read and agreed to the published version of the manuscript.
Funding
This study was funded by the Science and Technology Office of Chongqing Yubei District (2020-17), Chongqing medical scientific research project (Joint project of Chongqing Health Commission and Science and Technology Bureau) (2020MSXM129) and Project of Chongqing Graduate Tutor Team (dstd201903).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Stomatological hospital of Chongqing medical university ((2020)105 and 10 June 2020).
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Miyazaki, T.; Hotta, Y.; Kunii, J.; Kuriyama, S.; Tamaki, Y. A review of dental CAD/CAM: Current status and future perspectives from 20 years of experience. Dent. Mater. J. 2009, 28, 44–56. [Google Scholar] [CrossRef] [Green Version]
- Feuerstein, P. CAD/CAM: Enhancing productivity through automation. Compend. Contin. Educ. Dent. 2011, 32, 42–43. [Google Scholar]
- Peltola, S.M.; Melchels, F.P.W.; Grijpma, D.W.; Kellomäki, M. A review of rapid prototyping techniques for tissue engineering purposes. Ann. Med. 2008, 40, 268–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mankovich, N.J.; Cheeseman, A.M.; Stoker, N.G. The display of three-dimensional anatomy with stereolithographic models. J. Digit. Imaging 1990, 3, 200–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hems, E.; Knott, N.J. 3D printing in prosthodontics. Fac. Dent. J. 2014, 5, 152–157. [Google Scholar] [CrossRef]
- Seres, L.; Varga, J.E.; Kocsis, A.; Rasko, Z.; Bago, B.; Piffko, J. Correction of a severe facial asymmetry with computerized planning and with the use of a rapid prototyped surgical template: A case report/technique article. Head Face Med. 2014, 10, 27. [Google Scholar] [CrossRef] [Green Version]
- Tunchel, S.; Blay, A.; Kolerman, R.; Mijiritsky, E.; Shibli, J.A. 3D Printing/Additive Manufacturing Single Titanium Dental Implants: A Prospective Multicenter Study with 3 Years of Follow-Up. Int. J. Dent. 2016, 2016, 859097. [Google Scholar] [CrossRef] [Green Version]
- Wiechmann, D.; Rummel, V.; Thalheim, A.; Simon, J.S.; Wiechmann, L. Customized brackets and archwires for lingual orthodontic treatment. Am. J. Orthod. Dentofac. Orthop. 2003, 124, 593. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Sheng, Y.; Zhang, G. Design and Finite Element Analysis of the Personalized Labial Self-Ligating Bracket. Mach. Des. Manuf. 2018, 3, 71–74. [Google Scholar] [CrossRef]
- Retrouvey, J.M.; Kader, E.; Caron, E.; Tamimi, F.; Light, N. Printing Orthodontic Retainers Using CAD/CAM Technology. 2013. Available online: https://www.researchgate.net/profile/Jean-Marc-Retrouvey/publication/258699129_Printing_Orthodontic_Retainers_Using_CADCAM_Technology/links/0c960528d6a0be23fb000000/Printing-Orthodontic-Retainers-Using-CAD-CAM-Technology.pdf (accessed on 2 March 2022).
- Nasef, A.A.; El-Beialy, A.R.; Mostafa, Y.A. Virtual techniques for designing and fabricating a retainer. Am. J. Orthod. Dentofac. Orthop. 2014, 146, 394–398. [Google Scholar] [CrossRef] [PubMed]
- Hong, K.J. Transparent Aligner and Method for Manufacturing Same. U.S. Patent 10,258,431, 16 April 2019. [Google Scholar]
- Farronato, G.; Santamaria, G.; Cressoni, P.; Falzone, D.; Colombo, M. The digital-titanium Herbst. J. Clin. Orthod. 2011, 45, 263. [Google Scholar]
- Graf, S.; Cornelis, M.A.; Hauber, G.G.; Cattaneo, P.M. Computer-aided design and manufacture of hyrax devices: Can we really go digital? Am. J. Orthod. Dentofac. Orthop. 2017, 152, 870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yañez-Vico, R.M.; Perula, M.; Solano-Reina, E. Vertical and Transverse Management with Transpalatal Arches in an Adult with Class III Malocclusion. Case Rep. Dent. 2017, 2017, 4062105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wise, J.B.; Magness, W.B.; Powers, J.M. Maxillary molar vertical control with the use of transpalatal arches. Am. J. Orthod. Dentofac. Orthop. 1994, 106, 403. [Google Scholar] [CrossRef]
- Raucci, G.; Elyasi, M.; Pachêcopereira, C.; Grassia, V.; d’Apuzzo, F.; Flores-Mir, C.; Perillo, L. Predictors of long-term stability of maxillary dental arch dimensions in patients treated with a transpalatal arch followed by fixed appliances. Prog. Orthod. 2015, 16, 24. [Google Scholar] [CrossRef] [Green Version]
- Patel, D.R.; Mehta, D.F.; Mehta, D.S.; Khonde, D.S. Case report: Intra-arch non-compliant mechanics for maxillary 2nd molar buccal crossbite: A transpalatal arch with L-Loop. India J. Basic Appl. Med. Res. 2015, 4, 497–501. [Google Scholar]
- Ingervall, B.; Göllner, P.; Gebauer, U.; Fröhlich, K. A clinical investigation of the correction of unilateral first molar crossbite with a transpalatal arch. Am. J. Orthod. Dentofac. Orthop. 1995, 107, 418–425. [Google Scholar] [CrossRef]
- Sonawane, M.S.; Karandikar, G.R.; Pawar, P.A.; Shah, S.S. Reinstating Buccally Flared Molars using a Modified Transpalatal Arch. J. Contemp. Dent. 2013, 3, 98–101. [Google Scholar] [CrossRef]
- Mehta, D.F.; Patel, D.R.; Kharadi, D.L.; Mehta, S. A Modified Transpalatal Arch for Correction of Bucally Placed Maxillary 2nd Molars: Non-Compliant Mechanics. Iosr J. Dent. Med. Sci. 2014, 13, 24–26. [Google Scholar] [CrossRef]
- Durgekar, S.; Nagaraj, K. Modified transpalatal arch for molar intrusion. Int. J. Orthod. 2012, 23, 59. [Google Scholar]
- Gupta, G.; Rozario, J.E.; Patil, A.K.; Singh, R.K. Maxillary Molar Intrusion Evaluation using Mini-implants along with Transpalatal Arch Bar. J. Contemp. Dent. 2015, 5, 158–164. [Google Scholar] [CrossRef]
- Eyüboǧlu, S.; Bengi, A.O.; Gürton, A.U.; Akin, E. Asymmetric Maxillary First Molar Distalization with the Transpalatal Arch. Turk. J. Med. Sci. 2004, 34, 59–66. [Google Scholar]
- Miresmaeili, A.; Sajedi, A.; Moghimbeigi, A.; Farhadian, N. Three-dimensional analysis of the distal movement of maxillary 1st molars in patients fitted with mini-implant-aided trans-palatal arches. Korean J. Orthod. 2015, 45, 236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raucci, G.; Pachêcopereira, C.; Grassia, V.; d’Apuzzo, F.; Flores-Mir, C.; Perillo, L. Maxillary arch changes with transpalatal arch treatment followed by full fixed appliances. Angle Orthod. 2015, 85, 683–689. [Google Scholar] [CrossRef] [Green Version]
- Tsetsilas, M.; Konermann, A.C.; Keilig, L.; Reimann, S.; Jäger, A.; Bourauel, C. Symmetric and asymmetric expansion of molars using a Burstone-type transpalatal arch: Biomechanical and clinical analysis. J. Orofac. Orthop. 2015, 76, 377–390. [Google Scholar] [CrossRef]
- Kuang, Y.; Wang, C.; Hu, B.; Feng, G.; Wang, C.; Song, J. Biomechanical analysis of reinstating buccally flared maxillary 2nd molars using 3D printing anchorage supports: A 3D finite element study. Comput. Methods Biomech. Biomed. Eng. 2021, 24, 1085–1096. [Google Scholar] [CrossRef]
Figure 1.
Undercut-modified adhesive surface.

Figure 2.
An adhesive plate on the tooth.

Figure 3.
(A) The profile of patient before treatment; (B) the lateral cephalometric radiograph before treatment; (C) 3D TPA on model; (D) 3D TPA applied intraorally.
Figure 3.
(A) The profile of patient before treatment; (B) the lateral cephalometric radiograph before treatment; (C) 3D TPA on model; (D) 3D TPA applied intraorally.

Figure 4.
(A) Digital modal of dentition; (B) a big Carabelli cusp on the first upper molar; (C) a 3D TPA designed using the digital model.
Figure 4.
(A) Digital modal of dentition; (B) a big Carabelli cusp on the first upper molar; (C) a 3D TPA designed using the digital model.

Figure 5.
(A) Mild open bite in the anterior teeth; (B) a 3D TPA bonded on maxillary first molars; (C) corrected open bite.
Figure 5.
(A) Mild open bite in the anterior teeth; (B) a 3D TPA bonded on maxillary first molars; (C) corrected open bite.

Figure 6.
(A) The lateral cephalometric radiograph before treatment; (B) the profile before treatment; (C) conspicuous open bite in the anterior teeth; (D) a 3D TPA connecting maxillary first and second molars, see on a digital model; (E) the TPA applied intraorally.
Figure 6.
(A) The lateral cephalometric radiograph before treatment; (B) the profile before treatment; (C) conspicuous open bite in the anterior teeth; (D) a 3D TPA connecting maxillary first and second molars, see on a digital model; (E) the TPA applied intraorally.

Figure 7.
(A) A habit of tongue thrusting seen from an intraoral photograph; (B) the disappearance of tongue thrusting after wearing the 3D TPA; (C) digital design of a special 3D TPA (D) 3D TPA with palatal thorns bonded on teeth.
Figure 7.
(A) A habit of tongue thrusting seen from an intraoral photograph; (B) the disappearance of tongue thrusting after wearing the 3D TPA; (C) digital design of a special 3D TPA (D) 3D TPA with palatal thorns bonded on teeth.

Figure 8.
(A) A 3D TPA with a lateral arm, used to correct buccally flared second molar; (B) the buccally flared second molar corrected using the 3D TPA.
Figure 8.
(A) A 3D TPA with a lateral arm, used to correct buccally flared second molar; (B) the buccally flared second molar corrected using the 3D TPA.

Figure 9.
(A) Digital design of a 3D TPA with lateral arm to correct a palatally malposed canine; (B) the 3D TPA with a lateral arm applied intraorally; (C) the malposed canine was corrected with the 3D TPA.
Figure 9.
(A) Digital design of a 3D TPA with lateral arm to correct a palatally malposed canine; (B) the 3D TPA with a lateral arm applied intraorally; (C) the malposed canine was corrected with the 3D TPA.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Kuang, Y.; Hu, B.; Feng, G.; Huang, L.; Song, J. The Application of a 3-Dimensional Printing Technique in Refining the Orthodontic Trans-Palatal Arch. Appl. Sci. 2022, 12, 7497. https://doi.org/10.3390/app12157497
AMA Style
Kuang Y, Hu B, Feng G, Huang L, Song J. The Application of a 3-Dimensional Printing Technique in Refining the Orthodontic Trans-Palatal Arch. Applied Sciences. 2022; 12(15):7497. https://doi.org/10.3390/app12157497
Chicago/Turabian StyleKuang, Yunchun, Bo Hu, Ge Feng, Lan Huang, and Jinlin Song. 2022. "The Application of a 3-Dimensional Printing Technique in Refining the Orthodontic Trans-Palatal Arch" Applied Sciences 12, no. 15: 7497. https://doi.org/10.3390/app12157497
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.