
Augmented Reality, Virtual Reality and Artificial Intelligence in Orthopedic Surgery: A Systematic Review

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
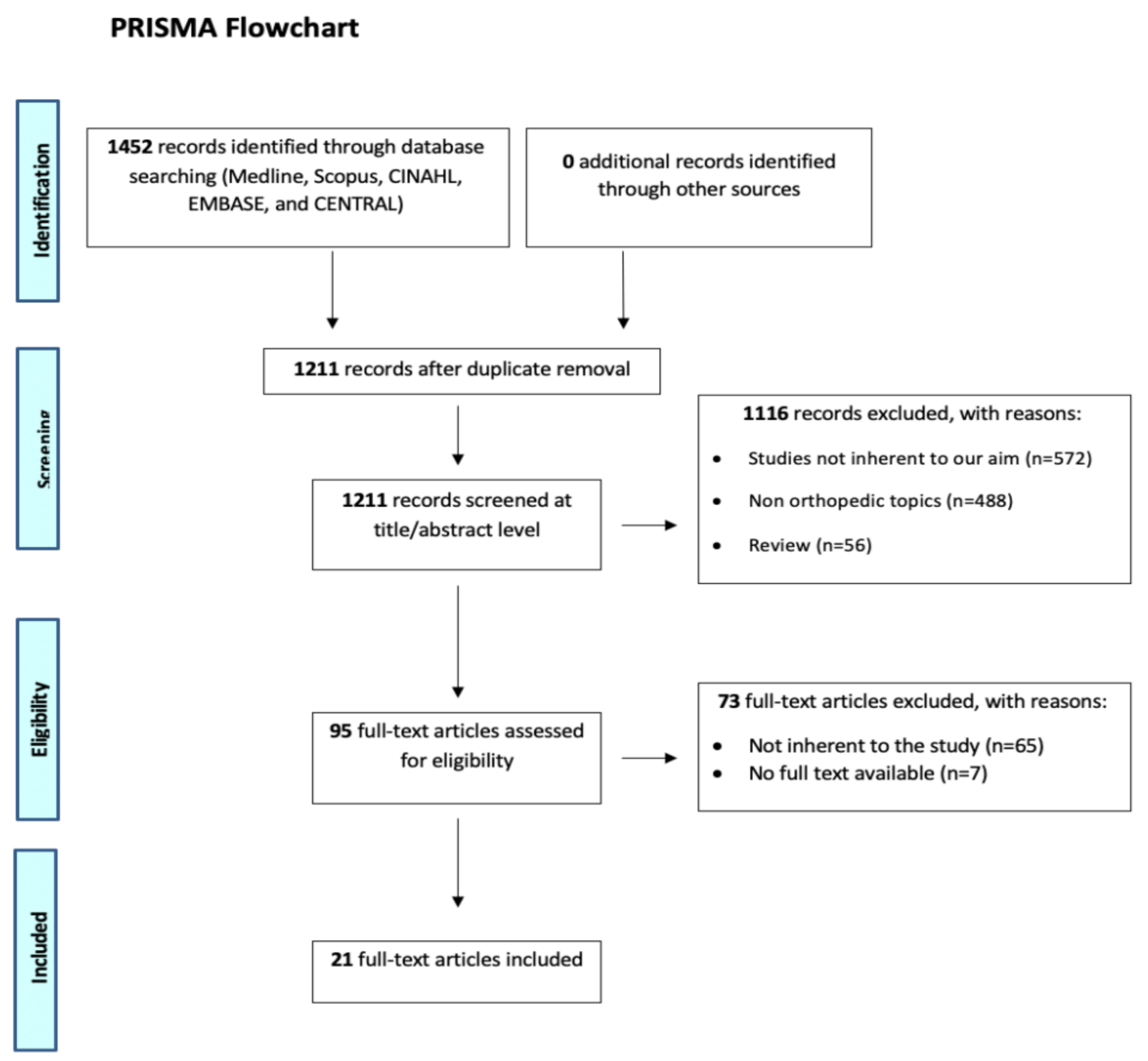
2.1. Eligibility Criteria and Search Strategy
2.2. Study Selection and Data Collection
2.3. Quality Assessment
- ⚬
- Overall score ≤1 High Quality;
- ⚬
- Overall score ≤3 Moderate Quality; and
- ⚬
- Overall score >3 Low Quality.
2.4. Data Synthesis and Analysis
3. Results
3.1. Study Selection and Patient Characteristics
3.2. Quality Assessment
3.3. Results of Individual Studies
3.3.1. Outcome: Preoperative Planning
3.3.2. Outcome: Intraoperative Use
3.3.3. Outcome: Surgical Training
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Verhey, J.T.; Haglin, J.M.; Verhey, E.M.; Hartigan, D.E. Virtual, augmented, and mixed reality applications in orthopedic surgery. Int. J. Med. Robot. 2020, 16, e2067. [Google Scholar] [CrossRef] [PubMed]
- Sakai, D.; Joyce, K.; Sugimoto, M.; Horikita, N.; Hiyama, A.; Sato, M.; Devitt, A.; Watanabe, M. Augmented, virtual and mixed reality in spinal surgery: A real-world experience. J. Orthop. Surg. 2020, 28. [Google Scholar] [CrossRef] [PubMed]
- Yuk, F.J.; Maragkos, G.A.; Sato, K.; Steinberger, J. Current innovation in virtual and augmented reality in spine surgery. Ann. Transl. Med. 2021, 9, 94. [Google Scholar] [CrossRef] [PubMed]
- Brigham, T.J. Reality Check: Basics of Augmented, Virtual, and Mixed Reality. Med. Ref. Serv. Q 2017, 36, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Logishetty, K.; Rudran, B.; Cobb, J.P. Virtual reality training improves trainee performance in total hip arthroplasty: A randomized controlled trial. Bone Joint J. 2019, 101-B, 1585–1592. [Google Scholar] [CrossRef] [PubMed]
- Madan, S.S.; Pai, D.R. Role of simulation in arthroscopy training. Simul. Healthc. 2014, 9, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Blyth, P.; Stott, N.S.; Anderson, I.A. A simulation-based training system for hip fracture fixation for use within the hospital environment. Injury 2007, 38, 1197–1203. [Google Scholar] [CrossRef]
- Berton, A.; Longo, U.G.; Candela, V.; Fioravanti, S.; Giannone, L.; Arcangeli, V.; Alciati, V.; Berton, C.; Facchinetti, G.; Marchetti, A.; et al. Virtual Reality, Augmented Reality, Gamification, and Telerehabilitation: Psychological Impact on Orthopedic Patients’ Rehabilitation. J. Clin. Med. 2020, 9, 2567. [Google Scholar] [CrossRef]
- Negrillo-Cárdenas, J.; Jiménez-Pérez, J.R.; Feito, F.R. The role of virtual and augmented reality in orthopedic trauma surgery: From diagnosis to rehabilitation. Comput. Methods Programs Biomed. 2020, 191, 105407. [Google Scholar] [CrossRef]
- Cannon, W.D.; Eckhoff, D.G.; Garrett, W.E.; Hunter, R.E.; Sweeney, H.J. Report of a group developing a virtual reality simulator for arthroscopic surgery of the knee joint. Clin. Orthop. Relat. Res. 2006, 442, 21–29. [Google Scholar] [CrossRef]
- Ogawa, H.; Hasegawa, S.; Tsukada, S.; Matsubara, M. A Pilot Study of Augmented Reality Technology Applied to the Acetabular Cup Placement During Total Hip Arthroplasty. J. Arthroplast. 2018, 33, 1833–1837. [Google Scholar] [CrossRef]
- Speicher, M.; Hall, B.D.; Nebeling, M. What is Mixed Reality? In Proceedings of the 2019 CHI Conference on Human Factors in Computing Systems, Glasgow, UK, 4–9 May 2019; pp. 1–15. [Google Scholar]
- Winkler-Schwartz, A.; Bissonnette, V.; Mirchi, N.; Ponnudurai, N.; Yilmaz, R.; Ledwos, N.; Siyar, S.; Azarnoush, H.; Karlik, B.; Del Maestro, R.F. Artificial Intelligence in Medical Education: Best Practices Using Machine Learning to Assess Surgical Expertise in Virtual Reality Simulation. J. Surg. Educ. 2019, 76, 1681–1690. [Google Scholar] [CrossRef]
- Mirchi, N.; Bissonnette, V.; Yilmaz, R.; Ledwos, N.; Winkler-Schwartz, A.; Del Maestro, R.F. The Virtual Operative Assistant: An explainable artificial intelligence tool for simulation-based training in surgery and medicine. PLoS ONE 2020, 15, e0229596. [Google Scholar] [CrossRef] [Green Version]
- Ramesh, A.N.; Kambhampati, C.; Monson, J.R.; Drew, P.J. Artificial intelligence in medicine. Ann. R Coll. Surg. Engl. 2004, 86, 334–338. [Google Scholar] [CrossRef] [Green Version]
- Panchmatia, J.R.; Visenio, M.R.; Panch, T. The role of artificial intelligence in orthopaedic surgery. Br. J. Hosp. Med. (Lond) 2018, 79, 676–681. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Van der Mierden, S.; Tsaioun, K.; Bleich, A.; Leenaars, C.H.C. Software tools for literature screening in systematic reviews in biomedical research. ALTEX 2019, 36, 508–517. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- LeBlanc, J.; Hutchison, C.; Hu, Y.; Donnon, T. A comparison of orthopaedic resident performance on surgical fixation of an ulnar fracture using virtual reality and synthetic models. J. Bone Joint Surg. Am. 2013, 95, e60. [Google Scholar] [CrossRef]
- Hooper, J.; Tsiridis, E.; Feng, J.E.; Schwarzkopf, R.; Waren, D.; Long, W.J.; Poultsides, L.; Macaulay, W.; Consortium, N.V.R. Virtual Reality Simulation Facilitates Resident Training in Total Hip Arthroplasty: A Randomized Controlled Trial. J. Arthroplast. 2019, 34, 2278–2283. [Google Scholar] [CrossRef]
- Ma, L.; Zhao, Z.; Chen, F.; Zhang, B.; Fu, L.; Liao, H. Augmented reality surgical navigation with ultrasound-assisted registration for pedicle screw placement: A pilot study. Int. J. Comput. Assist. Radiol. Surg. 2017, 12, 2205–2215. [Google Scholar] [CrossRef]
- Tsukada, S.; Ogawa, H.; Nishino, M.; Kurosaka, K.; Hirasawa, N. Augmented reality-based navigation system applied to tibial bone resection in total knee arthroplasty. J. Exp. Orthop. 2019, 6, 44. [Google Scholar] [CrossRef]
- Carl, B.; Bopp, M.; Saß, B.; Voellger, B.; Nimsky, C. Implementation of augmented reality support in spine surgery. Eur. Spine J. 2019, 28, 1697–1711. [Google Scholar] [CrossRef]
- Fotouhi, J.; Unberath, M.; Song, T.; Hajek, J.; Lee, S.C.; Bier, B.; Maier, A.; Osgood, G.; Armand, M.; Navab, N. Co-localized augmented human and X-ray observers in collaborative surgical ecosystem. Int. J. Comput. Assist. Radiol. Surg. 2019, 14, 1553–1563. [Google Scholar] [CrossRef]
- Hopkins, B.S.; Weber, K.A.; Kesavabhotla, K.; Paliwal, M.; Cantrell, D.R.; Smith, Z.A. Machine Learning for the Prediction of Cervical Spondylotic Myelopathy: A Post Hoc Pilot Study of 28 Participants. World Neurosurg. 2019, 127, e436–e442. [Google Scholar] [CrossRef]
- Teatini, A.; Kumar, R.P.; Elle, O.J.; Wiig, O. Mixed reality as a novel tool for diagnostic and surgical navigation in orthopaedics. Int. J. Comput. Assist. Radiol. Surg. 2021, 16, 407–414. [Google Scholar] [CrossRef]
- Gu, Y.; Yao, Q.; Xu, Y.; Zhang, H.; Wei, P.; Wang, L. A Clinical Application Study of Mixed Reality Technology Assisted Lumbar Pedicle Screws Implantation. Med. Sci. Monit. 2020, 26, e924982. [Google Scholar] [CrossRef]
- Fotouhi, J.; Alexander, C.P.; Unberath, M.; Taylor, G.; Lee, S.C.; Fuerst, B.; Johnson, A.; Osgood, G.; Taylor, R.H.; Khanuja, H.; et al. Plan in 2-D, execute in 3-D: An augmented reality solution for cup placement in total hip arthroplasty. J. Med. Imaging 2018, 5, 021205. [Google Scholar] [CrossRef] [Green Version]
- Hu, M.H.; Chiang, C.C.; Wang, M.L.; Wu, N.Y.; Lee, P.Y. Clinical feasibility of the augmented reality computer-assisted spine surgery system for percutaneous vertebroplasty. Eur. Spine J. 2020, 29, 1590–1596. [Google Scholar] [CrossRef]
- Chen, Y.; Jia, X.; Qiang, M.; Zhang, K.; Chen, S. Computer-Assisted Virtual Surgical Technology Versus Three-Dimensional Printing Technology in Preoperative Planning for Displaced Three and Four-Part Fractures of the Proximal End of the Humerus. J. Bone Joint Surg. Am. 2018, 100, 1960–1968. [Google Scholar] [CrossRef] [PubMed]
- Ishimoto, Y.; Jamaludin, A.; Cooper, C.; Walker-Bone, K.; Yamada, H.; Hashizume, H.; Oka, H.; Tanaka, S.; Yoshimura, N.; Yoshida, M.; et al. Could automated machine-learned MRI grading aid epidemiological studies of lumbar spinal stenosis? Validation within the Wakayama spine study. BMC Musculoskelet. Disord. 2020, 21, 158. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, H.; Kurosaka, K.; Sato, A.; Hirasawa, N.; Matsubara, M.; Tsukada, S. Does an Augmented Reality-based Portable Navigation System Improve the Accuracy of Acetabular Component Orientation During THA? A Randomized Controlled Trial. Clin. Orthop. Relat. Res. 2020, 478, 935–943. [Google Scholar] [CrossRef] [PubMed]
- Elmi-Terander, A.; Burström, G.; Nachabé, R.; Fagerlund, M.; Ståhl, F.; Charalampidis, A.; Edström, E.; Gerdhem, P. Augmented reality navigation with intraoperative 3D imaging vs fluoroscopy-assisted free-hand surgery for spine fixation surgery: A matched-control study comparing accuracy. Sci. Rep. 2020, 10, 707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yari, S.S.; Jandhyala, C.K.; Sharareh, B.; Athiviraham, A.; Shybut, T.B. Efficacy of a Virtual Arthroscopic Simulator for Orthopaedic Surgery Residents by Year in Training. Orthop. J. Sports Med. 2018, 6. [Google Scholar] [CrossRef] [Green Version]
- Edström, E.; Burström, G.; Persson, O.; Charalampidis, A.; Nachabe, R.; Gerdhem, P.; Elmi-Terander, A. Does Augmented Reality Navigation Increase Pedicle Screw Density Compared to Free-Hand Technique in Deformity Surgery? Single Surgeon Case Series of 44 Patients. Spine (Phila Pa 1976) 2020, 45, E1085–E1090. [Google Scholar] [CrossRef] [PubMed]
- Zheng, C.; Li, J.; Zeng, G.; Ye, W.; Sun, J.; Hong, J.; Li, C. Development of a Virtual Reality Preoperative Planning System for Postlateral Endoscopic Lumbar Discectomy Surgery and Its Clinical Application. World Neurosurg. 2019, 123, e1–e8. [Google Scholar] [CrossRef]
- Ponce, B.A.; Jennings, J.K.; Clay, T.B.; May, M.B.; Huisingh, C.; Sheppard, E.D. Telementoring: Use of augmented reality in orthopaedic education: AAOS exhibit selection. J. Bone Joint Surg. Am. 2014, 96, e84. [Google Scholar] [CrossRef]
- Vaughan, N.; Dubey, V.N.; Wainwright, T.W.; Middleton, R.G. A review of virtual reality based training simulators for orthopaedic surgery. Med. Eng. Phys. 2016, 38, 59–71. [Google Scholar] [CrossRef] [Green Version]
- Ponce, B.A.; Menendez, M.E.; Oladeji, L.O.; Fryberger, C.T.; Dantuluri, P.K. Emerging technology in surgical education: Combining real-time augmented reality and wearable computing devices. Orthopedics 2014, 37, 751–757. [Google Scholar] [CrossRef] [Green Version]
- Brouwers, L.; Pull Ter Gunne, A.F.; de Jongh, M.A.; Maal, T.J.J.; Vreeken, R.; van der Heijden, F.H.W.M.; Leenen, L.P.H.; Spanjersberg, W.R.; van Helden, S.H.; Verbeek, D.O.; et al. What is the value of 3D virtual reality in understanding acetabular fractures? Eur. J. Orthop. Surg. Traumatol. 2020, 30, 109–116. [Google Scholar] [CrossRef]
- Pauly, O.; Diotte, B.; Fallavollita, P.; Weidert, S.; Euler, E.; Navab, N. Machine learning-based augmented reality for improved surgical scene understanding. Comput. Med. Imaging Graph. 2015, 41, 55–60. [Google Scholar] [CrossRef]
- Guo, M.L.; Yue, S.T.; Wang, J.Y.; Cui, H.X. Comparative study on the clinical application of mixed reality technology leading micro-invasive intervertebral foramen puncture location and blind puncture location. Pak. J. Med. Sci 2020, 36, 559–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kriechling, P.; Roner, S.; Liebmann, F.; Casari, F.; Fürnstahl, P.; Wieser, K. Augmented reality for base plate component placement in reverse total shoulder arthroplasty: A feasibility study. Arch. Orthop. Trauma Surg. 2020. [Google Scholar] [CrossRef]
- Creighton, F.X.; Unberath, M.; Song, T.; Zhao, Z.; Armand, M.; Carey, J. Early Feasibility Studies of Augmented Reality Navigation for Lateral Skull Base Surgery. Otol. Neurotol. 2020, 41, 883–888. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Auvinet, E.; Giles, J.; Rodriguez, Y.; Baena, F. Augmented Reality Based Navigation for Computer Assisted Hip Resurfacing: A Proof of Concept Study. Ann. Biomed. Eng. 2018, 46, 1595–1605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elmi-Terander, A.; Burström, G.; Nachabe, R.; Skulason, H.; Pedersen, K.; Fagerlund, M.; Ståhl, F.; Charalampidis, A.; Söderman, M.; Holmin, S.; et al. Pedicle Screw Placement Using Augmented Reality Surgical Navigation with Intraoperative 3D Imaging: A First In-Human Prospective Cohort Study. Spine (Phila Pa 1976) 2019, 44, 517–525. [Google Scholar] [CrossRef]
- Ma, L.; Zhao, Z.; Zhang, B.; Jiang, W.; Fu, L.; Zhang, X.; Liao, H. Three-dimensional augmented reality surgical navigation with hybrid optical and electromagnetic tracking for distal intramedullary nail interlocking. Int. J. Med. Robot. 2018, 14, e1909. [Google Scholar] [CrossRef]
- Zhou, Z.; Hu, S.; Zhao, Y.Z.; Zhu, Y.J.; Wang, C.F.; Gu, X.; Fan, G.X.; He, S.S. Feasibility of Virtual Reality Combined with Isocentric Navigation in Transforaminal Percutaneous Endoscopic Discectomy: A Cadaver Study. Orthop. Surg. 2019, 11, 493–499. [Google Scholar] [CrossRef]
- Cho, H.S.; Park, Y.K.; Gupta, S.; Yoon, C.; Han, I.; Kim, H.S.; Choi, H.; Hong, J. Augmented reality in bone tumour resection: An experimental study. Bone Joint Res. 2017, 6, 137–143. [Google Scholar] [CrossRef] [Green Version]
- Andress, S.; Johnson, A.; Unberath, M.; Winkler, A.F.; Yu, K.; Fotouhi, J.; Weidert, S.; Osgood, G.; Navab, N. On-the-fly augmented reality for orthopedic surgery using a multimodal fiducial. J. Med. Imaging 2018, 5, 021209. [Google Scholar] [CrossRef]
- Lee, C.; Jang, J.; Lee, S.; Kim, Y.S.; Jo, H.J.; Kim, Y. Classification of femur fracture in pelvic X-ray images using meta-learned deep neural network. Sci. Rep. 2020, 10, 13694. [Google Scholar] [CrossRef]
- Langerhuizen, D.W.G.; Janssen, S.J.; Mallee, W.H.; van den Bekerom, M.P.J.; Ring, D.; Kerkhoffs, G.M.M.J.; Jaarsma, R.L.; Doornberg, J.N. What Are the Applications and Limitations of Artificial Intelligence for Fracture Detection and Classification in Orthopaedic Trauma Imaging? A Systematic Review. Clin. Orthop. Relat. Res. 2019, 477, 2482–2491. [Google Scholar] [CrossRef]
- Bi, Q.; Goodman, K.E.; Kaminsky, J.; Lessler, J. What is Machine Learning? A Primer for the Epidemiologist. Am. J. Epidemiol. 2019, 188, 2222–2239. [Google Scholar] [CrossRef]
- Soffer, S.; Ben-Cohen, A.; Shimon, O.; Amitai, M.M.; Greenspan, H.; Klang, E. Convolutional Neural Networks for Radiologic Images: A Radiologist’s Guide. Radiology 2019, 290, 590–606. [Google Scholar] [CrossRef]


{kind=link}
| Author | Sequence Generation | Allocation Concealment | Blinding of Participants and Personnel | Blinding of Outcome Assessment | Incomplete Outcome Data | Selective Outcome Reporting | Other Sources of Bias | Overall Score |
| Hooper, 2019 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| LeBlanc, 2013 | 0 | 0 | 0 | 2 | 0 | 0 | 0 | 2 |
| Logishetty, 2019 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 2 |
| Authors | Clearly Stated Aim | Inclusion of Consecutive Patients | Prospective Data Collection | Endpoints Appropriate to Study Aim | Unbiased Assessment of Study Endpoint | Follow-Up Period Appropriate to Study Aim | <5% Lost to Follow-Up | Prospective Calculation of Study Size | Adequate Control Group | Contemporary Groups | Baseline Equivalence of Groups | Adequate Statistical Analyses | Total Score (…/24) |
| Carl, 2018 | 2 | 2 | 0 | 2 | 0 | 0 | 0 | 2 | 0 | 0 | 0 | 0 | 8 |
| Chen, 2018 | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 2 | 0 | 2 | 2 | 2 | 20 |
| Edstrom, 2020 | 2 | 2 | 0 | 2 | 0 | 0 | 0 | 2 | 2 | 2 | 0 | 0 | 12 |
| Fotohui, 2018 | 2 | 0 | 0 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 6 |
| Fotouhi, 2019 | 2 | NA | 0 | 2 | 2 | 2 | 0 | NA | 2 | 2 | 0 | 0 | 12 |
| Gu, 2020 | 2 | 2 | 0 | 2 | 1 | 1 | 2 | 2 | 0 | 2 | 2 | 0 | 16 |
| Hopkins, 2019 | 2 | 2 | 0 | 2 | 0 | 2 | 2 | 2 | 0 | 0 | 0 | 0 | 10 |
| Hu, 2020 | 2 | 2 | 0 | 2 | 0 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 20 |
| Ishimoto, 2020 | 2 | 2 | 2 | 2 | 0 | 0 | 0 | 2 | 2 | 2 | 0 | 0 | 12 |
| Ma, 2017 | 2 | NA | 0 | 2 | 0 | 0 | 0 | NA | 0 | 0 | 0 | 2 | 6 |
| Ogawa, 2018 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 0 | 20 |
| Ogawa, 2019 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 22 |
| Ponce, 2014 | 2 | 0 | 2 | 2 | 2 | 2 | 2 | 2 | 0 | 2 | 0 | 2 | 18 |
| Shahram, 2018 | 2 | 2 | 2 | 2 | 2 | 0 | 0 | 2 | 2 | 2 | 2 | 2 | 20 |
| Teatini, 2021 | 2 | NA | 0 | 2 | 2 | 0 | 0 | NA | 0 | 0 | 0 | 0 | 6 |
| Terander, 2020 | 2 | 2 | 0 | 2 | 0 | 0 | 0 | 2 | 2 | 2 | 2 | 2 | 16 |
| Tsukada, 2019 | 2 | 2 | 0 | 2 | 0 | 0 | 0 | 2 | 2 | 2 | 2 | 2 | 16 |
| Zheng, 2018 | 2 | 2 | 0 | 2 | 0 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 18 |
| Author and Year | Country | Study Design, LOE | Sample | Purpose | Hardware | Procedure | Conclusion |
|---|---|---|---|---|---|---|---|
| Carl, 2019 [25] | Germany | PS, II | 10 | Intraoperative | AR | Spine surgery | AR greatly supports the surgeon in understanding the 3D anatomy, thereby facilitating surgery |
| Chen, 2018 [32] | China | PComS, II | 131 | Preoperative | VR | Fracture reduction | The clinical outcomes in both the virtual surgical and 3D printing groups were better than those in the conventional group. VR is more convenient and efficient |
| Edstrom, 2020 [37] | Sweden | RCohS, III | 44 | Intraoperative | AR | Pedicle screw placement | AR enables the surgeon to minimize the use of hooks in deformity surgery without prolonging the surgical time |
| Fotouhi, 2018 [30] | UK | RComS, III | 4 surgeons | Intraoperative | AR | Total hip arthroplasty | AR simplifies and allows accurate implantation of the acetabular cup |
| Fotouhi, 2019 [26] | USA | RComS, III | NA | Intraoperative | AR vs. X-Ray | Percutaneous fixation | AR solution provides a shared augmented experience between the human and X-ray viewer |
| Gu 2020 [29] | China | PComS, II | 50 | Intraoperative | AR (MR) | Lumbar pedicle screws placement | The safety of spinal surgery and implantation accuracy of pedicle screw fixation system could be increased by AR |
| Hooper, 2019 [22] | United States | RCT, I | 14 residents | Traning | VR | Total hip arthroplasty | VR-simulation improves resident surgical skills but has no significant effect on medical knowledge |
| Hopkins, 2019 [27] | USA | PCCS, II | 28 | Preoperative | AI | Prediction of CSM diagnosis and severity | AI provides a promising method for prediction, diagnosis, and even prognosis in patients affected by CSM. |
| Hu, 2020 [31] | Taiwan | PCCS, II | 18 | Intraoperative | AR | Percutaneous vertebroplasty | The guidance of the AR system provided a more accurate bony entry point with reduced operative time and unnecessary radiation exposure. |
| Ishimoto, 2020 [33] | UK | RCS, III | 971 | Preoperative | AI | Lumbar spinal stenosis | An automated system can learn with an excellent performance against the reference standard |
| LeBlanc, 2013 [21] | Canada | RCT, I | 22 residents | Training | VR | Ulnar fixation | The procedural measures used to assess resident performance demonstrated good reliability and validity, and both the Sawbones and the virtual simulator showed evidence of construct validity. |
| Logishetty, 2019 [5] | United Kingdom | RCT, I | 24 trainees | Training | VR | Total hip arthroplasty | VR training advanced trainees further up the learning curve, enabling exact component orientation and more efficient surgery. VR could augment traditional surgical training to improve how surgeons learn complex open procedures |
| Ma, 2017 [23] | China | PS, II | NA | Intraoperative | AR | Intramedullary nail fixation | The AR-guided distal interlocking method is feasible and has many potential applications in clinic after further evaluation. |
| Ogawa, 2018 [11] | Japan | PS, II | 54 | Intraoperative | AR | Total hip arthroplasty | AR system provided more accurate information than the conventional method |
| Ogawa, 2020 [34] | Japan | PComS, II | 46 | Intraoperative | AR | Total hip arthroplasty | AR system did not show better results compared to the traditional group |
| Ponce, 2014 [41] | USA | PS, II | 15 | Intraoperative | VR—Virtual interactive presence | Arthroscopic shoulder surgery | VIP technology was efficient, safe, and effective as a teaching tool |
| Yari, 2018 [36] | USA | POS, II | 18 residents | Training | VR—ArthroS simulator | Knee and shoulder arthroscopy | Residents training on a virtual arthroscopic simulator made significant improvements in both knee and shoulder arthroscopic surgery skills |
| Teatini, 2021 [28] | Sweden | PCohS, II | 8 surgeons | Intraoperative | AR (MR) | Visualization of joint and skeletal deformities | AR improve diagnostic accuracy and allow for safer and more precise surgeries, as well as provide for better learning conditions for orthopaedic surgeons in training |
| Terander, 2020 [35] | Sweden | POS, II | 20 | Intraoperative | AR | Spine surgery | Statistically higher screw placement accuracy compared to the free-hand technique in a cohort of spinal deformity cases |
| Tsukada, 2019 [24] | Japan | PS, II | 10 | Intraoperative | AR | Total knee arthroplasty | AR system provides reliable accuracy total knee arthroplasty. |
| Zheng, 2018 [38] | China | PCohS, II | 30 | Intraoperative | VR | Discectomy | Statistically higher accuracy was reported in the VR group |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Longo, U.G.; De Salvatore, S.; Candela, V.; Zollo, G.; Calabrese, G.; Fioravanti, S.; Giannone, L.; Marchetti, A.; De Marinis, M.G.; Denaro, V. Augmented Reality, Virtual Reality and Artificial Intelligence in Orthopedic Surgery: A Systematic Review. Appl. Sci. 2021, 11, 3253. https://doi.org/10.3390/app11073253
Longo UG, De Salvatore S, Candela V, Zollo G, Calabrese G, Fioravanti S, Giannone L, Marchetti A, De Marinis MG, Denaro V. Augmented Reality, Virtual Reality and Artificial Intelligence in Orthopedic Surgery: A Systematic Review. Applied Sciences. 2021; 11(7):3253. https://doi.org/10.3390/app11073253
Chicago/Turabian StyleLongo, Umile Giuseppe, Sergio De Salvatore, Vincenzo Candela, Giuliano Zollo, Giovanni Calabrese, Sara Fioravanti, Lucia Giannone, Anna Marchetti, Maria Grazia De Marinis, and Vincenzo Denaro. 2021. "Augmented Reality, Virtual Reality and Artificial Intelligence in Orthopedic Surgery: A Systematic Review" Applied Sciences 11, no. 7: 3253. https://doi.org/10.3390/app11073253