
Thallium Use, Toxicity, and Detoxification Therapy: An Overview
by
 , , and
, , and
Giuseppe Genchi
1 ,
,
Alessia Carocci
2,*,
Graziantonio Lauria
1, 
Maria Stefania Sinicropi
1,† and
and
Alessia Catalano
2,† 1
Department of Pharmacy, Health and Nutritional Sciences, University of Calabria, Via Pietro Bucci, Arcavacata di Rende, 87036 Cosenza, Italy
2
Department of Pharmacy-Drug Sciences, University of Bari “Aldo Moro”, 70126 Bari, Italy
*
Author to whom correspondence should be addressed.
†
These authors equally contributed to this work.
Appl. Sci. 2021, 11(18), 8322; https://doi.org/10.3390/app11188322
Submission received: 11 August 2021
/
Revised: 4 September 2021
/
Accepted: 6 September 2021
/
Published: 8 September 2021
(This article belongs to the Special Issue Heavy Metal Toxicity: Environmental and Human Health Risk Assessment)
Abstract
:Thallium (Tl) is released into the environment, where is present at very low levels, from both natural and anthropogenic sources. Tl is considered as one of the most toxic heavy metals; it is a non-essential metal, present in low concentrations in humans. Tl toxicity causes dermatological and gastrointestinal diseases and disorders of the nervous system, and may even result in death. Many isotopes of Tl exist, with different uses. One of the isotopes of this metal (201Tl) is used in cardiovascular scintigraphy and for the diagnosis of malignant tumors such as breast or lung cancer and osteosarcoma bone cancer. Many Tl compounds are tasteless, colorless, and odorless. Due to these characteristics and their high toxicity, they have been used as poisons in suicides and murders for criminal purposes, as well as instances of accidental poisoning. Impaired glutathione metabolism, oxidative stress, and disruption of potassium-regulated homeostasis may play a role in the mechanism of Tl toxicity. Solanum nigrum L. and Callitriche cophocarpa have been suggested as promising agents for the phytoremediation of Tl. In addition, macrocyclic compounds such as crown ethers (18-crown-6) are good candidates to absorb Tl from wastewater. Through this review, we present an update to general information about the uses and toxicity of Tl. Furthermore, the attention is focused on detoxification therapies.
1. Introduction
Thallium (Tl) is a rare earth bluish-white heavy metal (81 atomic number, 204.38 atomic mass, 11.85 g/cm3), and is soft, malleable, and exists in two oxidation states (I and III). The name thallium derives from Greek thallos, a young olive-green shoot. Although thallium is present in the natural environment in low concentration, it is widely distributed in water environments [1]. The European COST Action TD1407 included Tl in the list of technology-critical elements, with associated environmental impacts and potential human health threats [2]. This element is a non-essential metal present in low concentration in human tissues but is endowed with high potential toxicity. Indeed, it has been considered one of the most toxic among the heavy metals, more toxic to humans than mercury, cadmium, lead, copper, or zinc [3,4]. Acute Tl poisoning in humans induces pathological changes in organs such as the stomach, liver, kidneys, brain, intestine, cardiovascular and nervous systems, along with chronic effects such as mental disorders or polyneuritis, and may even result in death [5]. The lethal dose of Tl for an adult human is only 8–10 mg/kg. Monovalent thallium is similar to potassium in ionic radius and electrical charge, and these factors contribute to its toxic nature. Thallium acts on several organs, interfering with cellular metabolism, affecting vital potassium-dependent processes and mitochondrial metabolism, affecting uncoupling mitochondrial oxidative phosphorylation. In addition, thallium increases reactive oxygen species (ROS) formation and phospholipid peroxidation, alters the mitochondrial membrane potential (MMP), causing mitochondrial depolarization and swelling with a release of cytochrome C from the inner mitochondrial membrane. These processes are likely to account for the neurotoxic effects of the metal [6]. Long-term, low-dose prenatal Tl exposure may cause dysfunction in the mother [7], whereas absorbed Tl can affect the developing fetus because it can cross the placental barrier [8]. Several treatment modalities have been used for thallium toxicity, but no single antidote has been shown to be effective in severe toxicity. However, combinations of different treatments have been proven to be beneficial in several cases. Prussian blue (PB) has been the most prescribed antidote to treat thallium poisoning. This chelator agent is administered by the oral route, decreasing the absorption of Tl to the enterohepatic circulation, and therefore increasing the elimination of Tl into feces [9]. Despite its effectiveness as an antidote, in severe cases of human thallotoxicosis, its administration is still ineffective. Other chelating agents have been administered alone or in combination with PB, such as sodium diethyldithiocarbamate and D-penicillamine [10,11]. The combined treatment of PB and metallothionein has proven to be a good antidotal option against thallotoxicosis [12]. Blood purification treatments are also a beneficial treatment option, especially for patients with severe thallium poisoning [13]. Despite its toxicity, known since the 1970s [14,15], this metal is applied in cardiovascular scintigraphy and as a tool for imaging malignant tumors such as lung cancer, breast cancer and osteosarcoma bone cancer [16]. Thallium-201 chloride (201Tl-thallous chloride) was the first radiopharmaceutical clinically used for cardiac imaging technique in the evaluation of ischemic heath disease. Short-lived radioactive thallium (emitting X-rays and gamma-rays) is administered by the intravenous route in the human body. It is obtained from metal mining, ore processing or smelting operations and is discarded as a by-product in the environment [17]. In recent years, Tl contamination incidences have been reported in many countries, mostly due to industrial activities such as the mining and smelting of Tl-rich sulfide ores, metallurgical production, coal combustion, and cement production [18]. Recent studies have shown that elevated Tl levels often occur in soils, waters, sediments, and agricultural products in the vicinity of industrial sites using Tl-bearing mineral resources [19]. Thallium can be released into the environment as waste from the production of cadmium, lead and zinc, and cement factories, and by the combustion of coal in coal-fired power plants. There is an increasing contemporary demand for this metal in the advanced technology field, in infrared spectrometers and other optical systems, electronic devices, alloys, semiconductors, and the laser industry [20,21]. High levels of thallium have been found in drinking water, vegetables, fruits and food due to anthropogenic activities [19,22]. Human beings are subjected to thallium exposure through the intake of contaminated fruits, vegetables, and other food, water, through the inhalation of polluted air, and living near industrial facilities such as cement and coal-fired power plants, mines and ore smelting. Aprea et al. reported a study which represents the most extensive human biomonitoring campaign for the evaluation of thallium exposure available at international level [22]. Staff et al. showed that urinary thallium concentrations were higher in thallium workers than in non-occupationally exposed people and general workers [23]. Therefore, the removal of this element from soil and water is vital to eradicate its health impacts. Phytoremediation is a green technology that uses plants to remove toxic and radioactive metals, and organic compounds such as pesticides and detergents from soil and water, and it is used for its cost-effectiveness and environmental friendliness [24]. Some plants are ideal for the phytoremediation process, especially when they grow fast and have a high biomass [25]. Solanum nigrum L., Brassica oleracea acephala L., Brassica napus, Brassica juncea, Iberis intermedia and Callitriche cophocarpa have been identified as good species for the phytoremediation of soil and waters contaminated by thallium [26,27,28]. This review intends to summarize the most interesting aspects of thallium, such as its properties, uses, toxicity and some of the methods used for the detoxification therapy.
2. Thallium Chemistry and Properties
Thallium (Tl; atomic number 81) is located between mercury and lead in the periodic table of elements and belongs to the metals of main Group 13 (IIIA, or boron group). Tl is a bluish-white heavy metal, and is ductile, malleable, shiny, with a density of 11.85 g/cm3 (Table 1). Thallium was discovered in 1861 by the English chemist William Crookes who observed a bright-green line never seen before in the spectrum of a sample of selenium, used in the production of sulfuric acid. The next year (1862), independently of each other, the English W. Crookes and the French C.A. Lamy isolated thallium. Its atomic weight (204.38) derives from a mixture of the two more stable isotopes: 203Tl (29.5%) and 205Tl (70.5%). Thallium has 41 isotopes with atomic masses ranging from 176 to 216. 204Tl is the most stable radioisotope with a half-life of 3.78 years; it emits beta particles, forming 204Pb. 201Tl has a half-life of 72.9 h and decays by electron capture (EC) in 201Hg. Thallium concentrations in the Earth’s crust range between 0.1 mg/kg and 1.7 mg/kg [29], and it is found in crookesite selenium-containing mineral [(Cu-Tl-Ag)2Se], in lorandite sulfur-containing mineral (TlAsS2) and in hutchinsonite sulfur-containing mineral [(TlPb)2As5S9]. It may also be found in iron, lead, cadmium, and zinc ores, from which it is obtained during refining and smelting processes [1]. Areas with high thallium concentrations are Rotokawa (New Zealand), Lengenbach (Switzerland), Guizhou Province (China) and Kavadarci (Macedonia). Thallium naturally accumulates in the environment where human activity is present, such as in the copper mines of El Loa (Chile). In this region, the concentration of thallium in potatoes and beans is very high (about 6800 µg/kg) [30]. In oxidation state I (Tl+, thallous cation), thallium is more stable with respect to Tl3+ (thallic cation, oxidation state III). All thallium compounds are highly toxic. Thallium forms univalent thallous (Tl+; chlorine, bromine, fluorine, and iodine) salts and trivalent thallic (Tl3+) salts, which are water-soluble and highly toxic. When exposed to air, this metal oxidizes, forming a thin Tl(I) oxide (Tl2O) coating at its surface, whereas at higher temperature it forms Tl(III) oxide (Tl2O3).
3. Thallium Toxicity
Although being a highly toxic element, thallium has been studied to a much lesser degree than other toxic elements such as lead, cadmium, or mercury [31,32]. This happens mainly because Tl is often undetected by classical analytical methods which tend to have poorer sensitivity for Tl than for other elements. All forms of thallium are soluble enough to be toxic to living organisms [1]. Tl is a colorless, water-soluble, tasteless, and affordable element; therefore, it may cause isolated and massive human poisoning. The first symptoms (Table 2) of poisoning can be different and non-specific, making differential diagnosis difficult. The effects of Tl toxicity in human beings arise after a couple of weeks from its administration, with alopecia being the main symptom, firstly with hair loss, then complete baldness, followed by axillary and pubic hair loss. Thallium poisoning becomes troubling when other symptoms occur such as gastrointestinal problems (nausea, vomiting and diarrhea), peripheral and central nervous system disorders (dysesthesia, ataxia, tremors, convulsions, paralysis, sleeplessness, hallucinations, and delirium), and cardiac problems, such as tachycardia and hypotension, lethargy, and coma) [33,34].
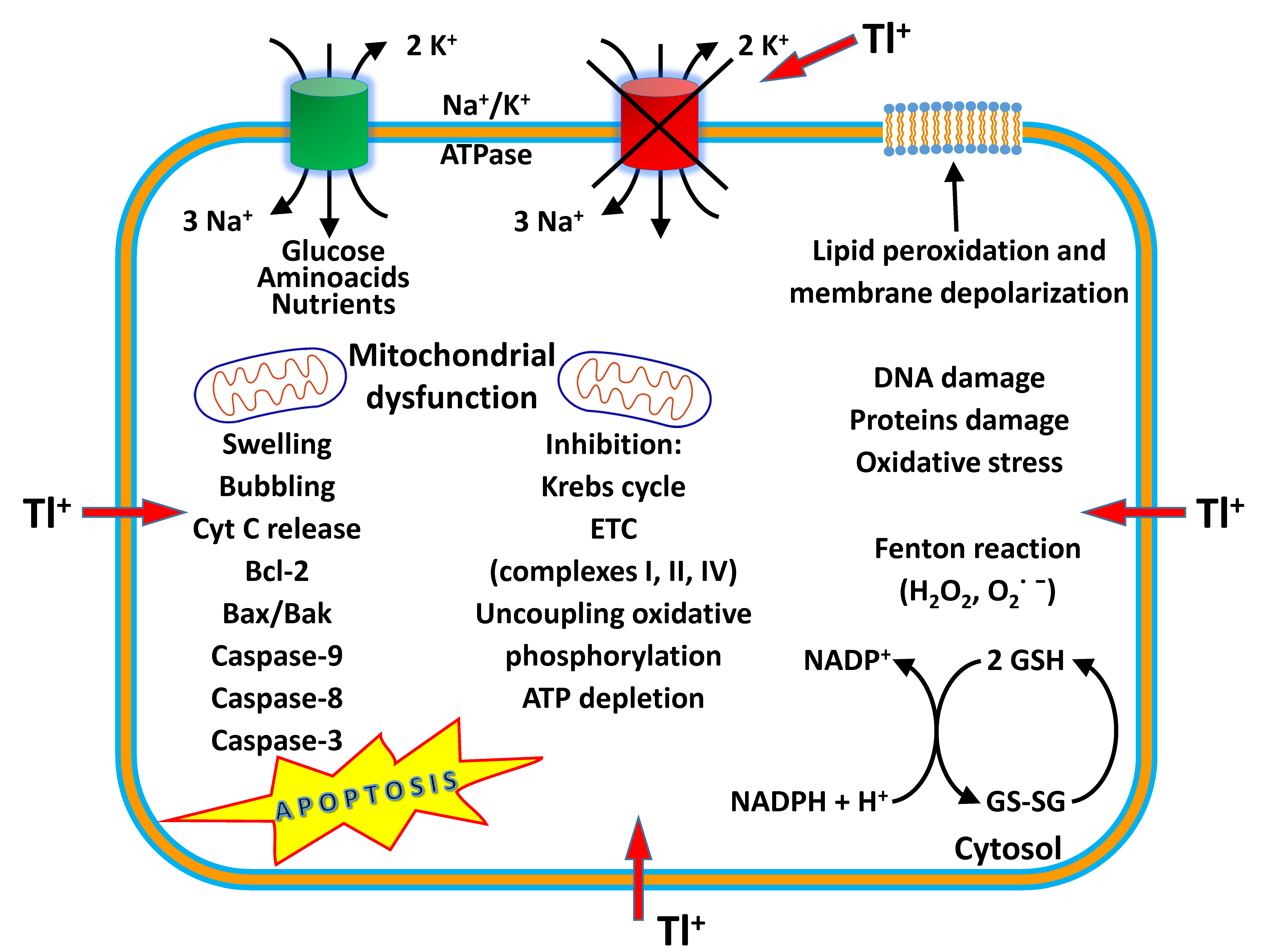
Thallium poisoning can even lead to death. Thallous sulfate is odorless and tasteless and was once successfully used as a household rodenticide and insecticide, but many countries in the Western word have banned such use due to numerous cases of unintentional or criminal poisonings of humans. After numerous cases of unintentional poisonings, the commercial use of thallium salts as household poison for rats, squirrels and ants was banned in the West [35]. Tl has been described as an infamous adulterant added to opioids, heroin, and cocaine [36,37]. In mammals, Tl is more toxic than mercury, lead, zinc, cadmium, and copper. Thallium is absorbed by the ingestion of polluted food of animal and vegetable origin, and the inhalation of contaminated air, through skin contact and mucous membranes; it is distributed throughout the body by the blood and can cross the encephalic and placental barriers. Thallium is accumulated in the liver, bones, brain, kidney, testes, stomach, lungs, spleen, and skin of the scalp; it has also been detected in hair, nails, tears, and breast milk. Concentrations of Tl in human organs follow this order: brain (0.42–1.5 ng/g), liver (1.5 ng/g), kidney (6.1 ng/g), hair (150–650 ng/g), bone (600 ng/g), and nail (1200 ng/g) [38]. The major route of elimination of this metal is mainly in urine and feces. The urine test is the most reliable and accurate way to determine Tl concentrations in the human body. Under normal conditions, thallium in urine does not have to exceed 1 mg/g creatinine and can be detected after 1 h for up to 2 months after exposure [1]. The measurement is usually carried out for spectrophotometric determination. The method is focused on the oxidation of 3-methyl-2-benzothiazolinone hydrazone hydrochloride by Tl3+ to diazonium cation, in the presence of imipramine hydrochloride in phosphoric acid medium to obtain a blue-colored solution with a maximum absorption length of 635 nm [39]. A possible mechanism of Tl toxicity is its ability to affect glutathione (GSH) activity. Indeed, glutathione binds heavy metals, including thallium, through its –SH group, inhibiting their toxicity. In addition, glutathione blocks the formation of ROS while maintaining the oxidant homeostasis of the plasma. Eskandari and collaborators studied the effects of Tl on rat liver mitochondria [40]. Tl+ in different concentrations induced a significant increase in mitochondrial ROS formation, ATP depletion, glutathione oxidation, mitochondrial membrane potential (MMP) collapse and mitochondrial outer membrane rupture with cytochrome C release, and peroxidation of membrane phospholipids, especially binding to anionic head groups (Figure 1). This suggests that Tl+ may alter the fluidity of the mitochondrial membranes, acting on phospholipid packing and affecting the activities of membrane-associated transport systems and enzymes, and disrupting receptor functions. Tl does not have biological functions; however, Tl+ can enter cells through potassium uptake channels due to its similarity in charge and ionic radius to potassium (K+). The estimated absorption of this metal through the respiratory apparatus in unpolluted environments is below 0.005 μg/day [41]. Tl follows potassium distribution pathways and, in this way, alters many of potassium-dependent processes. For example, Tl may inhibit the enzymatic activity of Na+/K+-ATPase [42]. Thallium can substitute K+ in Na+/K+-ATPase and shows a tenfold greater affinity for Na+/K+-ATPase by inhibiting the activity of this enzyme. This enzyme with an antiport mechanism across the cellular and mitochondrial membranes makes three sodium ions move against two potassium ions. This difference in charge provides the driving force to import with symport mechanism glucose, amino acids, and nutrients (Figure 1). In addition, in mitochondria Tl alters the balance of Bax/Bad/Bcl-2 proteins, activating caspase-9, caspase-8 and caspase-3, thus leading to apoptotic death [5]. Tl compromises mitochondrial energy production by inhibiting pyruvate dehydrogenase, succinate dehydrogenase, complexes I, II and IV of the electron transport chain (ETC), and uncoupling oxidative phosphorylation with decreasing ATP synthesis (Figure 1). In addition, thallium takes the place of potassium in the stabilization of ribosomes, as well as in physiological muscle contraction. Other possible mechanisms of Tl poisoning include cell mitosis, cell metabolic disorders, interference with DNA synthesis and the induction of chromosomal abnormalities. This metal interferes with the mechanisms of energy production especially in glycolysis, the Krebs cycle and oxidative phosphorylation [43]. Other mechanisms of Tl toxicity include the interference of Tl with the active sites of several enzymes as it interacts with amino-sulfhydryl groups. Thallium may inhibit the function of enzymes, such as pyruvate kinase, ATPase, and aldehyde dehydrogenase, by binding to the sulfhydryl groups (–SH) of cysteines [44]. In addition, thallium takes the place of potassium in the stabilization of ribosomes, as well as in physiological muscle contraction [45].
Thallium acts on cells and mitochondria by inducing oxidative stress and generating ROS, activating apoptosis, inhibiting the electron transport chain, reducing ATP synthesis, altering membrane permeability, and damaging DNA and proteins.
4. Detoxification Therapy
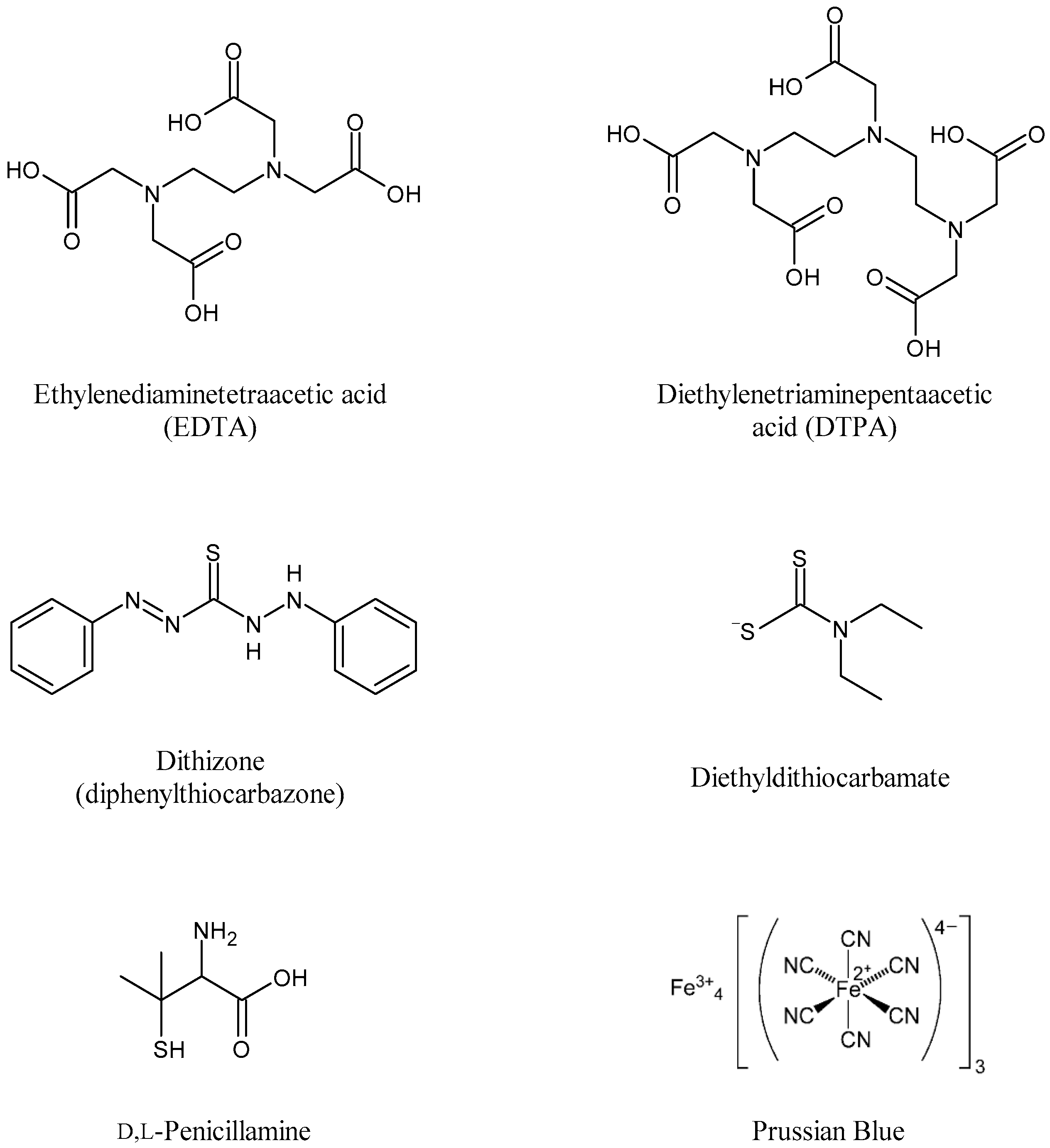
Several cases of thallium poisoning have been reported in the United States and other countries as result of the use of thallium for criminal purposes [46]. Thallium is a well-known poison described in numerous works of fictional literature and in many films. Many antidotes intended to neutralize the toxicity effects of this metal have proven to be ineffective [47]. Traditional chelation therapy (Figure 2) using ethylenediaminetetraacetic acid (EDTA) and diethylenetriaminepentaacetic acid (DTPA) is without benefit. The use of DL-penicillamine allows the withdrawal of thallium, but this procedure causes Tl redistribution into other vital organs. Dithizone (diphenylthiocarbazone) increases the fecal elimination of Tl in rats by 33%, but with adverse effects [48]. Another chelating agent, diethyldithiocarbamate (DDC), increases the urinary excretion of Tl; however, this compound forms a lipophilic complex with thallium, resulting in the redistribution of this xenobiotic into the central nervous system, increasing thallium levels in the brain [10]. In 2011, Montes et al. [11] observed that the treatment with a combination of DL-penicillamine and Prussian blue [potassium ferric hexacyanoferrate(II)] (approved by the United States Food and Drug Administration) in rats enabled the elimination of thallium without redistribution to the brain. Hemodialysis and hemoperfusion are also used to remove thallium from the blood stream [49]. Zhang et al. (2014) [50] treated nine patients with acute thallium poisoning with Prussian blue in combination with sequential hemodialysis, hemoperfusion and/or continuous veno-venous hemofiltration, obtaining satisfactory curative effects. In cases of severe poisoning and gastrointestinal ingestion, the efficacy of hemodialysis either alone or in combination with multi-dose activated charcoal and Prussian blue to remove thallium may be considered. Additionally, renal excretion of thallium can be obtained with potassium chloride treatment. In a case report of suicide, where the patient was poisoned with thallium sulfate, even when treated with combined therapy, namely, multi-dose activated charcoal with airway protection, Prussian blue, continuous renal replacement therapy, and an intravenous lorazepam infusion for sedation, did not overcome the crisis and died [47]. Yumoto and coauthors [35] at Kayama University Hospital in Japan (2017) reported a case of 23-year-old woman who was poisoned after drinking tea containing toxic substances. On the 10th day after intoxication, a colleague of the patient confessed his crime by reporting the use of thallium sulfate in tea. The physicians immediately began the detoxification therapy by administering multi-dose activated charcoal with airway protection, vit B12, Prussian blue and lorazepam. After six months of treatment, the patient was declared out of danger. In the first of the two cases of poisoning, treated clinically with the same procedure, the amounts of thallium determined in the blood and urine of the suicide subject were 5369 µg/L and >2000 µg/L, respectively, much higher than in the second case (223 µg/L and 351 µg/L, respectively); therefore, results of the detoxification procedure were not as successful as in the second case.
5. Thallium in the Environment
Thallium is naturally present in the environment. Emissions, which lead to increased concentrations of thallium in the environment, may be natural or associated with anthropogenic activities. The rapid technological and industrial expansion have resulted in increased risks of environmental contamination with thallium. It is estimated that approximately 5000 tons of thallium is released into the environment every year due to industrial activity, with approximately 1000 tons originating from the combustion of coal [1]. On average, the concentration of thallium in the Earth’s crust is around 0.1–1.7 mg/kg, generally present in the sulfide ores of zinc, copper, lead, and coal [17]. Higher thallium contents (1.7–55 mg/kg) are common in soil formed from limestone, marble, and granite. Wheat and maize grain can accumulate this heavy metal up to 55 mg/kg. Much higher values, up to 1000 mg/kg, have been found in coal mines from the Jurassic period [51,52]. Thallium is commonly found in granite, shale, volcanic rock, and pyrites used to make sulfuric acid, and is also recovered as flue dust from iron, lead, cadmium, and copper smelters. The most anthropogenic sources of thallium are emissions from coal combustion to generate electric power, petroleum-refining processes and oil drilling, processes for cement production, and the smelting of ores (copper, zinc, pyrite, and lead). Power-generating plants, such as those which use brown coal and coal from the Jurassic period as fuel, produce the highest emissions of thallium into the atmosphere. During the combustion of coal, this metal volatilizes and then condenses on ash particles. Once deposited, thallium tends to persist in the soil, particularly in the soil containing clay, organic matter, iron, and manganese oxides; in acidic soil, in contrast, thallium retention is less effective. In addition, thallium is emitted to the atmosphere as dust, vapors, or liquid during industrial processing, and deposited in the soil matrix, where soluble monovalent salts are transported thanks to aqueous routes into the environment, where it is taken up by the roots of plants and accumulates in plant biomass [1]. As a result, Tl enters the food chain and accumulates in living organisms. It can be consumed by human beings in water and foods of animal and vegetal origin (Table 3).
6. Uses of Thallium
The US Geological Survey estimates that the annual worldwide production of this metal is about 10 metric tons as a by-product from the smelting of copper, zinc and lead ores. About 17 million kilograms of global thallium resources are contained in zinc ores in Canada, the United States and Europe, whereas 630 million kilograms are in the world’s coal mines [17]. In the 1930s, thallium was used to treat venereal diseases (e.g., syphilis and gonorrhea), malaria, and ringworm as a depilatory agent. Thallium salts were first used as pesticides in Germany in the 1920s, and because of their severe toxicity eventually became used as rodenticides. However, after several poisonings, thallium use as rodenticide was banned in the United States in 1965 [47]. The odorless thallium sulfate and acetate have been used to kill rats, squirrels, and ants; however, after many cases of unintentional poisoning, it was banned in Western countries. Unfortunately, cases of thallium poisoning are still reported in countries where it is still illegally used as a rodenticide and ant killer. There is an increasing contemporary demand for thallium in advanced industrial technology. It is used in the manufacture of electronic equipment, camera lenses, semiconductor materials (Tl selenite), scintillator counters, laser equipment, low-temperature thermometers in alloys with mercury, and photoelectric cells. Special glass with a high index of refraction is prepared from thallium oxide. It is also used in imitation jewels and artificial diamonds, green fireworks, yellow-greenish glass (Tl sesquioxide), in the production of pesticides, phosphate fertilizers and in the impregnation of woods and leather against fungi and bacteria [17,31,41]. In medicine, the most important use of 201Tl (TlCl) is as radiological contrast agent in scintigraphy imaging of the heart, liver and testes, and in tumor visualization. Thallium, as a pharmaceutical cosmetic product, is applied for facial hair removal and fungal infections of the scalp [57]. Thallium acetate is currently used as a catalyst in organic synthesis in the oxidation of olefins and hydrocarbons, and in epoxidation and polymerization reactions [58]. Detection of Tl is a challenging task because its concentration in environmental samples may be at a nanogram per gram level or lower. Most studies for the determination of Tl are conducted in water matrices. Mass spectrometry, atomic absorption spectrometry and voltammetry are key analytical techniques used for the determination and monitoring of Tl in environmental samples [59,60,61].
7. 201Thallium Scintigraphy
Myocardial perfusion scintigraphy (MPS) is one of the most used techniques to perform noninvasive cardiac imaging tests in the diagnosis of acute onset chest pain as well as in the evaluation of subjects with coronary artery disease in conditions of exercise stress or pharmacological stress to increase coronary blood flow. An increase in coronary flow can be obtained increasing oxygen demand in healthy coronary dynamics under stress exercise (bicycle or treadmill), with dobutamide (a β1-adrenergic agonist), or by pharmacological vasodilatation with adenosine [62] or pyridamole for patients unable to perform exercise under effort. The clinic protocol involves intravenous injections of small quantities of radioactive compounds at peak stress followed by imaging of its distribution in the heart with a rotating gamma camera. There are three radioactive tracers available: 201thallium and two 99mtechnetium (sestamibi and tetrofosmin). Thallous (201) chloride has been used routinely as a tracer since the 1970s [14,15]. Single-photon emission computed tomography (SPECT) thallium is used as a screening test for coronary artery disease (CAD) [63] and coronary-to-pulmonary artery fistula (CPAF) [64]. 201Tl has a half-life of 73.1 h and decomposes by electron capture, emitting X-rays (68–80 KeV) and gamma-rays (137–167 KeV). 201Tl is incorporated into the myocytes via the Na+/K+-ATPase transport system and facilitates diffusion. Imaging of the process starts within 5–10 min after peak stress and injection when the heart is rested. After about 4 h from intravenous injection, there is a redistribution of thallium between the intra- and the extra-cellular spaces in all the myocytes, without considering perfusion [65]. The image soon after the injection is a combination of viability and perfusion, whereas the redistribution image only presents viability. The radiation exposure [100–150 mega Becquerel (MBq)] of 201Tl is high due to its relatively long half-life, and only 4% of the injected solution is absorbed by the myocytes. In addition, its low-energy emission leads to low-resolution images. The half-life of 99mTc is 6.00 h; thus, the radiation exposure is much lower than that thallium. In addition, the positive effects of technetium use include better images in obese subjects and women with large breasts. MPS is a good method for imaging the effects of coronary artery disease on the heart during exercise stress and pharmacological stress after an injection of 201Tl and 99mTc [66]. Several studies have highlighted the excellent accuracy in the detection of coronary artery disease in subjects with undiagnosed chest pain using the MPS technique [67]. 201Tl scintigraphy, unlike 99mTc, is commonly used in clinical oncology as a tool for imaging malignant neoplasms such as sarcoma, lung, and breast cancer [68]. Murata et al. (2008) [69] were able to distinguish a chondromyxoid fibroma (benign bone tumor) from a chondrosarcoma (primary bone sarcoma) in the left knee of an 18-year-old man by using 201Tl scintigraphy and magnetic resonance imaging. In a successive paper, the pigmented villonodular synovitis (tecnosynovial giant cell non-malignant tumor) in the right elbow of an 18-year-old woman was studied [70]. Magnetic resonance imaging revealed an isointense signal of the tumor; the use of 201Tl scintigraphy enabled the highlighting and location of an abnormal accumulation of a cancerous mass in the elbow, which was surgically removed. Inai and coauthors (2015) [71] used 201Tl scintigraphy to differentiate malignant bone tumors from benign bone tumors. The study involved 279 patients with bone lesions (228 benign and 51 malignant). The authors evaluated 201Tl intake by studying tumor-to-background contrast (TBC). Differences in TBC on early imaging (15 min after the injection of radioactive thallium) and delayed imaging (2 h after the injection of radioactive thallium) were measured by the Mann–Whitney U test. The authors found significant differences in median TBC between malignant tumors and benign tumors: 1.57 versus 0.09 (p < 0.001) for early imaging, as well as 0.83 versus 0.07 (p < 0.001) for delayed imaging. The authors chose a cut-off of 0.68 for early imaging and 0.38 for delayed imaging; thus, the prediction of malignancy had 77% sensitivity, 74% specificity and 75% accuracy for early imaging, and 80% sensitivity, 76% specificity and 77% accuracy for delayed imaging. Therefore, TBC values of 0.68 on early imaging and 0.38 on delayed imaging were meaningful indicators to differentiate malignant bone tumors from benign bone tumors. In addition to 201Tl scintigraphy, 99mTc and 2-[18F]-fluoro-2-deoxy-D-glucose (FDG) are also clinically used to detect coronary artery diseases, cartilaginous tumors of bone, and benign and malignant musculoskeletal tumors [68,72]
8. Thallium Phytoremediation from Soil and Water
Volcanoes and human activities, such as industrialization, pyrite mining and cement plants, the smelting of thallium-containing ores, and burning coal to produce energy are the major causes for the presence of toxic metal compounds in the ecosystem. Toxic metal pollution of soil, water and plants is a major environmental problem; heavy metals are not degradable and their accumulation in the soil and water can contaminate drinking water and the food chain (vegetables and fruits), with serious health effects for humans. Most conventional physical, chemical, and biochemical approaches do not provide solutions to these problems, and are often expensive and invasive, causing the alteration of soil properties and disturbing the soil microflora. Phytoremediation is a technology that uses plants to remove toxic and radioactive metals and organic compounds (pesticides, crude oils, and detergents) from the environment [73,74,75]. In the New Zealand laboratory of LaCoste (2001) [76], vegetables such as green bean, green cabbage, beetroot, lettuce, onion, pea, radish, spinach, tomato, turnip, water cress and Iberis intermedia were grown in pot trials in the presence of Tl (0.7 mg/kg to 3.7 mg/kg) to study the capability of these plants to remove this metal from polluted soils. The results showed that the uptake of thallium ranged from about 1 mg/kg in green bean to 400 mg/kg in Iberis intermedia. The Tl concentrations were analyzed by flame atomic absorption spectrometry (FAAS) for samples with higher thallium levels, or by graphite furnace atomic absorption spectrometry for samples with lower thallium concentrations. Wu, in their laboratory in Guangzhou (China) (2015) [28], evaluated the ability of black nightshade Solanum nigrum L. for Tl phytoremediation in pot culture. The accumulation of thallium into roots, stems, leaves and fruits were determined under field conditions. The results of Wu and collaborators were examined using different thallium concentrations (from 1 mg/kg to 20 mg/kg) after a 4-month pot culture, and suggested Solanum nigrum as a good candidate for the phytoremediation of thallium. Although it reduced growth, and chlorosis and leaf senescence were observed at a thallium concentration of ≥15 mg/kg, the authors recommended the choice of Solanum nigrum for the phytoremediation of moderately thallium-contaminated soil. Callitriche cophocarpa has been used for the phytoremediation of water polluted by thallium, cadmium, zinc, and lead [77]. The authors pointed out that the accumulation of the elements by Callitriche cophocarpa shoots (mg/kg dry weight) followed this order: Zn (1120), Tl (251), Cd (71) and Pb (35), whereas the bioconcentration factors were the highest for Cd (1177) and Tl (1043). The authors found that Callitriche cophocarpa was able to remove Tl from polluted water as well as Cd, Zn and Pb. Due its high toxicity, the removal of thallium from wastewater is very important, even though its concentration is very low. Adsorption is a method used for thallium removal and infinite types of absorbent have been used, including Prussian blue analogues and metal oxide hydrates such as iron oxide, super-magnetic Fe3O4, nano-Al2O3 [78], titanate nano tubes [79], etc. However, the use of these absorbents did not give excellent results. Zhao et al. (2020) [80] provided new macrocyclic compounds such as crown ethers as absorbents for thallium removal from wastewater. Notably, the cavity of crown ethers must be able to efficiently contain Tl+ ions to form a stable complex with negatively charged oxygen atoms. Considering the cavity of several crown ethers, thallium (Tl+) settles better in the cavity of 18-crown-6. Moreover, the oxygen atoms inside circle ether can be partially replaced with sulfur atoms to increase the affinity of the crown ether towards Tl+. Furthermore, another class of macrocyclic compounds, calixarenes, can be considered as promising absorbents for removing thallium from wastewater.
9. Summary
Thallium is a toxic heavy metal which was unintentionally discovered by Sir William Crookes in 1861, who burned dust from a sulfuric acid industrial plant. It is present in the natural environment in low concentrations, occurring most frequently in the sulfide ores of several heavy metals. It is more toxic to humans than other heavy metals, such as mercury, cadmium, lead, copper, or zinc, and has been responsible for many accidental, occupational, deliberate, and therapeutic intoxications. It was once used as a rodenticide and insecticide, but it was then banned because of numerous cases of unintentional or criminal poisonings of humans. Thallium scintigraphy is used as a potential test in detecting malignancy in solid and hematological tumors, such as breast cancers and lymphomas. SPECT thallium is used for CAD and CPAF. Appropriate protective measures should be considered to reduce occupational exposure to this metal and ensure workers’ health. However, the identification and control of Tl sources, and the monitoring environmental exposures and hazards, should be performed to counteract thallium toxicity, which represents a serious health problem all over the world and requires attention at both clinical and preclinical levels. In this review, we analyzed and summarized the properties, uses and toxicity of thallium, focusing on the most interesting papers reported in the literature for this metal.
Author Contributions
Writing-original draft preparation, G.G.; funding acquisition and supervision, M.S.S.; literature review, G.L.; conceptualization, A.C. (Alessia Catalano); writing-review and editing, A.C. (Alessia Carocci). All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
The authors gratefully acknowledge the financial support provided by Ministero dell’Università e della Ricerca (MIUR, Italia).
Conflicts of Interest
The authors declare that they have no conflict of interest.
Abbreviations
| ETC | electron transport chain |
| CAD | coronary artery disease |
| CPAF | coronary-to-pulmonary artery fistula |
| Cyt C | cytochrome C |
| DDC | diethyldithiocarbamate |
| DTPA | diethylenetriaminepentaacetic acid |
| EDTA | ethylenediaminetetraacetic acid |
| FAAS | flame atomic absorption spectrometry |
| FDG | 2-[18F]-fluoro-2-deoxy-D-glucose |
| GSH | glutathione |
| GSSG | reduced glutathione |
| MBq | mega Becquerel |
| MMP | mitochondrial membrane potential |
| MPS | myocardial perfusion scintigraphy |
| ROS | reactive oxygen species |
| SPECT | single-photon emission computed tomography |
| TBC | tumor-to-background contrast |
References
- Karbowska, B. Presence of thallium in the environment: Sources of contaminations, distribution and monitoring methods. Environ. Monit. Assess. 2016, 188, 640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cobelo-García, A.; Filella, M.; Croot, P.; Frazzoli, C.; Du Laing, G.; Ospina-Alvarez, N.; Rauch, S.; Salaun, P.; Schäfer, J.; Zimmermann, S. COST action TD1407: Network on technology-critical elements (NOTICE)—from environmental processes to human health threats. Environ. Sci. Pollut. Res. 2015, 22, 15188–15194. [Google Scholar] [CrossRef] [Green Version]
- Sinicropi, M.S.; Caruso, A.; Capasso, A.; Palladino, C.; Panno, A.; Saturnino, C. Heavy metals: Toxicity and carcinogenicity. Pharmacologyonline 2010, 2, 329–333. [Google Scholar]
- Carocci, A.; Rovito, N.; Sinicropi, M.S.; Genchi, G. Mercury toxicity and neurodegenerative effects. Rev. Environ. Contam. Toxicol. 2014, 229, 1–18. [Google Scholar]
- Osorio-Rico, L.; Santamaria, A.; Galván-Arzate, S. Thallium Toxicity: General Issues, Neurological Symptoms, and Neurotoxic Mechanisms. Adv. Neurobiol. 2017, 18, 345–353. [Google Scholar] [PubMed]
- Osorio-Rico, L.; Villeda-Hernández, J.; Santamaría, A.; Königsberg, M.; Galván-Arzate, S. The N-methyl-d-aspartate receptor antagonist MK-801 prevents thallium-induced behavioral and biochemical alterations in the rat brain. Int. J. Toxicol. 2015, 34, 505–513. [Google Scholar] [CrossRef]
- Zhu, B.; Liang, C.; Yan, S.; Li, Z.; Huang, K.; Xia, X.; Hao, J.; Zhu, P.; Tao, F. Association between serum thallium in early pregnancy and risk of gestational diabetes mellitus: The Ma’anshan birth cohort study. J. Trace Elem. Med. Biol. 2019, 52, 151–156. [Google Scholar] [CrossRef]
- Wu, M.; Shu, Y.; Song, L.; Liu, B.; Zhang, L.; Wang, L.; Liu, Y.; Bi, J.; Xiong, C.; Cao, Z.; et al. Prenatal exposure to thallium is associated with decreased mitochondrial DNA copy number in newborns: Evidence from a birth cohort study. Environ. Int. 2019, 129, 470–477. [Google Scholar] [CrossRef]
- Altagracia-Martínez, M.; Kravzov-Jinich, J.; Martínez-Núñez, J.M.; Ríos-Castañeda, C.; López-Naranjo, F. Prussian blue as an antidote for radioactive thallium and cesium poisoning. Orphan Drugs Res. Rev. 2012, 2, 13–21. [Google Scholar] [CrossRef]
- Kamerbeek, H.H.; Rauws, A.G.; Ten Ham, M.; Van Heijst, A.N.P. Dangerous redistribution of thallium by treatment with sodium diethyldithiocarbamate. Acta Med. Scandinav. 1971, 189, 149–154. [Google Scholar] [CrossRef]
- Montes, S.; Pérez-Barrón, G.; Rubio-Osornio, M.; Ríos, C.; Diaz-Ruíz, A.; Altagracia-Martínez, M.; Monroy-Noyola, A. Additive effect of DL-penicillamine plus Prussian blue for the antidotal treatment of thallotoxicosis in rats. Environ. Toxicol. Pharmacol. 2011, 32, 349–355. [Google Scholar] [CrossRef]
- Anaya-Ramos, L.; Díaz-Ruíz, A.; Ríos, C.; Montes, S.; Aguirre-Vidal, Y.; García-Jiménez, S.; Baron-Flores, V.; Monroy-Noyola, A. Metallothionein alone or in combination with Prussian blue attenuates acute thallium systemic toxicity in rats. Res. Sq. 2020. [Google Scholar] [CrossRef]
- Ghannoum, M.; Nolin, T.D.; Goldfarb, D.S.; Darren, M.R.; Mactier, R.; Mowry, J.B.; Dargan, P.I.; MacLaren, R.; Hoegberg, L.C.; Laliberté, M.; et al. Extracorporeal treatment for thallium poisoning: Recommendations from the EXTRIP Workgroup. Clin. J. Am. Soc. Nephrol. 2012, 7, 1682–1690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lebowitz, E.; Greene, M.V.; Fairchild, R.; Bradley-Moore, P.R.; Atkins, H.L.; Ansari, A.N.; Richards, P.; Belgrave, E. Thallium-201 for medical use. I. J. Nucl. Med. 1975, 16, 151–155. [Google Scholar]
- Ritchie, J.L.; Trobaugh, G.B.; Hamilton, G.W.; Gould, K.L.; Naraharn, K.A.; Williams, D.L. Myocardial imaging with thallium-201 at rest and during exercise: Comparison with coronary arteriography and resting and stress electrocardiography. Circulation 1977, 56, 66–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poudyal, B.; Shrestha, P.; Chowdhury, Y.S. Thallium-201. StatPearls [Internet]. 21 July 2020. Available online: https://www.ncbi.nlm.nih.gov/books/NBK560586/ (accessed on 11 August 2021).
- U.S. Geological Survey (U.S. GS). Thallium Statistics and Information. Available online: http://minerals.usgs.gov/minerals/pubs/commodity/thallium/ (accessed on 29 June 2021).
- Wang, J.; Zhou, Y.; Dong, X.; Yin, M.; Tsang, D.C.; Sun, J.; Liu, J.; Song, G.; Liu, Y. Temporal sedimentary record of thallium pollution in an urban lake: An emerging thallium pollution source from copper metallurgy. Chemosphere 2020, 242, 125172. [Google Scholar] [CrossRef]
- Liu, J.; Wei, X.; Zhou, Y.; Tsang, D.C.W.; Bao, Z.; Yin, M.; Lippold, H.; Yuan, W.; Wang, J.; Feng, Y.; et al. Thallium contamination, health risk assessment and source apportionment in common vegetables. Sci. Total Environ. 2020, 703, 135547. [Google Scholar] [CrossRef] [PubMed]
- Sander, S.; Kappenstein, O.; Ebner, I.; Fritsch, K.A.; Schmidt, R.; Ptaff, K.; Luch, A. Release of aluminium and thallium ions from uncoated food contact materials made of aluminium alloys into food and food simulant. PLoS ONE 2018, 13, e0200778. [Google Scholar] [CrossRef] [PubMed]
- Datta, A.; Fiala, J.; Becla, P.; Motakef, S. Stable room-temperature thallium bromide semiconductor radiation detectors. APL Mater. 2017, 5, 106109. [Google Scholar] [CrossRef] [Green Version]
- Aprea, M.C.; Nuvolone, D.; Petri, D.; Voller, F.; Bertelloni, S.; Aragona, I. Human biomonitoring to assess exposure to thallium following the contamination of drinking water. PLoS ONE 2020, 15, e0241223. [Google Scholar] [CrossRef]
- Staff, J.F.; Cotton, R.J.; Warren, N.D.; Morton, J. Comparison of urinary thallium levels in non-occupationally ex-posed people and workers. Int. Arch. Occup. Environ. Health 2014, 87, 275–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farooqi, Z.U.R. Phytoremediation of inorganic pollutants: An eco-friendly approach, its types and mechanisms. Plant Environ. 2012, 1, 110–129. [Google Scholar]
- Rai, G.K.; Bhat, B.A.; Mushtaq, M.; Tariq, L.; Rai, P.K.; Basu, U.; Dar, A.A.; Islam, S.T.; Dar, T.U.H.; Bhat, J.A. Insights into decontamination of soils by phytoremediation: A detailed account on heavy metal toxicity and mitigation strategies. Physiol. Plant. 2021, 173, 287–304. [Google Scholar] [PubMed]
- Al-Najar, H.; Schulz, R.; Römheld, V. Phytoremediation of thallium contaminated soils by brassicaceae. In Environmental Chemistry; Springer: Berlin/Heidelberg, Germany, 2005; pp. 187–196. [Google Scholar]
- Rader, S.T.; Maier, R.M.; Barton, M.D.; Mazdab, F.K. Uptake and fractionation of thallium by Brassica juncea in a geogenic thallium-amended substrate. Environ. Sci. Technol. 2019, 53, 2441–2449. [Google Scholar] [CrossRef] [PubMed]
- Wu, Q.; Leung, J.Y.S.; Huang, X.; Yao, B.; Yuan, X.; Ma, J.; Guo, S. Evaluation of the ability of black nightshade Solanum nigrum L. for phytoremediation of thallium-contaminated soil. Environ. Sci. Pollut. Res. 2015, 22, 11478–11487. [Google Scholar] [CrossRef]
- Kazantzis, G. Thallium in the environment and health effects. Environ. Geochem. Health 2000, 22, 275–280. [Google Scholar] [CrossRef]
- Queirolo, F.; Stegen, S.; Contreras-Ortega, C.; Ostapczuk, P.; Queirolo, A.; Paredes, B. Thallium levels and bioaccumulation in environmental samples of northern Chile: Human health risks. J. Chil. Chem. Soc. 2009, 54, 464–469. [Google Scholar] [CrossRef] [Green Version]
- Carocci, A.; Catalano, A.; Lauria, G.; Sinicropi, M.S.; Genchi, G. Lead toxicity, antioxidant defense andenvironment. Rev. Environ. Contam. Toxicol. 2016, 238, 45–67. [Google Scholar]
- Genchi, G.; Sinicropi, M.S.; Carocci, A.; Lauria, G.; Catalano, A. Mercury exposure and heart diseases. Int. J. Environ. Res. Public Health 2017, 14, 74. [Google Scholar] [CrossRef] [Green Version]
- Zavaliy, L.B.; Petrikov, S.S.; Simonova, A.Y.; Potskhveriya, M.M.; Zaker, F.; Ostapenko, Y.N.; Ilyashenko, K.K.; Dikaya, T.I.; Shakhova, O.B.; Evseev, A.K.; et al. Diagnosis and treatment of persons with acute thallium poisoning. Toxicol. Rep. 2021, 8, 277–281. [Google Scholar] [CrossRef]
- Kemnic, T.R.; Coleman, M. Thallium Toxicity; StatPearls Publishing: Treasure Island, NV, USA, 2021. [Google Scholar]
- Yumoto, T.; Tsukahara, K.; Naito, H.; Iida, A.; Nakao, A. A successfully treated case of criminal thallium poisoning. J. Clin. Diagn. Res. 2017, 11, OD01–OD02. [Google Scholar] [CrossRef] [PubMed]
- Ghaderi, A.; Vahdati-Mashhadian, N.; Oghabian, Z.; Moradi, V.; Afshari, R.; Mehrpour, O. Thallium exists in opioid poisoned patients. DARU J. Pharm. Sci. 2015, 23, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Molavi, N.; Ghaderi, A.; Banafshe, H.R. Determination of thallium in urine, blood, and hair in illicit opioid users in Iran. Hum. Exp. Toxicol. 2020, 39, 808–815. [Google Scholar] [CrossRef]
- Tyagi, R.; Rana, P.; Khan, A.R.; Bhatnagar, D.; Devi, M.M.; Chaturvedi, S.; Tripathi, R.P.; Khushu, S. Study of acute biochemical effects of thallium toxicity in mouse urine by NMR spectroscopy. J. Appl. Toxicol. 2011, 31, 663–670. [Google Scholar] [CrossRef] [PubMed]
- Nagaraja, P.; Ghllab Saeed Al-Tayar, N.; Shivakumar, A.; Shresta, A.K.; Gowda, A.K. Spectrophotometric determination of the trace amount of thallium in water and urine samples by novel oxidative coupling reaction. E-J. Chem. 2009, 6, 1153–1163. [Google Scholar] [CrossRef] [Green Version]
- Eskandari, M.R.; Mashayekhi, V.; Aslani, M.; Hosseini, M.J. Toxicity of thallium on isolated rat liver mitochondria: The role of oxidative stress and MPT pore opening. Environ. Toxicol. 2005, 30, 232–241. [Google Scholar] [CrossRef] [PubMed]
- International Programme on Chemical Safety (IPCS). Thallium. Environmental Health Criteria; World Health Organization: Geneva, Switzerland, 1996; Volume 182. [Google Scholar]
- Cvjetko, P.; Cvjetko, I.; Pavlica, M. Thallium Toxicity in Humans. Arh. Hig. Rada Toksikol. 2010, 61, 111–119. [Google Scholar] [CrossRef] [Green Version]
- Hoffman, R.S. Thallium toxicity and the role of Prussian blue in therapy. Toxicol. Rev. 2003, 22, 29–40. [Google Scholar] [CrossRef]
- Rodríguez-Mercado, J.J.; Altamirano-Lozano, M.A. Genetic toxicology of thallium: A review. Drug Chem. Toxicol. 2013, 36, 369–383. [Google Scholar] [CrossRef]
- Douglas, K.T.; Bunni, M.A.; Baindur, S.R. Thallium in biochemistry. Int. J. Biochem. 1990, 22, 429–438. [Google Scholar] [CrossRef]
- Al Hammouri, F.; Darwazeh, G.; Said, A.; Ghosh, R.A. Acute thallium poisoning: Series of ten cases. J. Med. Toxicol. 2011, 7, 306–311. [Google Scholar] [CrossRef]
- Riyaz, R.; Pandalai, S.L.; Schwartz, M.; Kazzi, Z.N. A fatal case of thallium toxicity: Challenges in management. J. Med. Toxicol. 2013, 9, 75–78. [Google Scholar] [CrossRef] [Green Version]
- Mercurio, M.; Hoffman, R.S. Thallium. In Goldfrank’s Toxicologic Emergencies, 8th ed.; Flomenbaum, N.E., Goldfrank, L.R., Hoffman, R.S., Howland, M.A., Lewin, N.A., Nelson, L.S., Eds.; McGraw-Hill: New York, NY, USA, 2006; pp. 1364–1372. [Google Scholar]
- Malbrain, M.L.; Lambrecht, G.L.; Zandijk, E.; Demedts, P.A.; Neels, H.M.; Lambert, W.; De Leenheer, A.P.; Lins, R.L.; Daelemans, R. Treatment of severe thallium intoxication. J. Toxicol. Clin. Toxicol. 1997, 35, 97–100. [Google Scholar] [CrossRef]
- Zhang, H.T.; Qiao, B.P.; Liu, B.P.; Zhao, X.G. Study on the treatment of acute thallium poisoning. Am. J. Med. Sci. 2014, 347, 377–381. [Google Scholar] [CrossRef]
- Peter, A.L.J.; Viraraghavan, T. Thallium: A review of public health and environmental concerns. Environ. Int. 2005, 31, 493–501. [Google Scholar] [CrossRef]
- Yang, C.; Chen, Y.; Peng, P.; Li, C.; Chang, X.; Xie, C. Distribution of natural and anthropogenic thallium in the soils in an industrial pyrite slag disposing area. Sci. Total Environ. 2005, 341, 159–172. [Google Scholar] [CrossRef] [PubMed]
- Sager, M. Thallium in agricultural practice. In Thallium in the Environment; Nriagu, J.O., Ed.; John Wiley & Sons: New York, NY, USA, 1998; pp. 59–87. [Google Scholar]
- Rose, M.; Baxter, M.; Brereton, N.; Baskaran, C. Dietary exposure to metals and other elements in the 2006 UK Total Diet Study and some trends over the last 30 years. Food Addit. Contam. Part A Chem. Anal. Control. Expo. Risk Assess. 2010, 27, 1380–1404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Das, A.K.; Chakraborty, R.; Cervera, M.L.; de la Guardia, M. Determination of thallium in biological samples. Anal. Bioanal. Chem. 2006, 385, 665–670. [Google Scholar] [CrossRef]
- Pappas, R.S.; Polzin, G.M.; Zhang, L.; Watson, C.H.; Paschal, D.C.; Ashley, D.L. Cadmium, lead, and thallium in mainstream tobacco smoke particulate. Food Chem. Toxicol. 2006, 44, 714–723. [Google Scholar] [CrossRef]
- Stockinger, H.E. Thallium. In Patty’s Industrial Hygiene and Toxicology: Vol. 2A: Toxicology, 3rd ed.; John Wiley and Sons Publishing: New York, NY, USA; Chichester: Brisbane, Australia; Toronto, ON, Canada, 1987; pp. 1914–1931. [Google Scholar]
- Blain, F.; Kazantzis, G. Thallium. In Handbook on the Toxicology of Metals, 4th ed.; Nordberg, G.F., Fowler, B.A., Nordberg, M., Eds.; Academic Press: Cambridge, MA, USA, 2015; pp. 1129–1240. ISBN 9780123973399. [Google Scholar]
- Lei, C.; Xu, X. Determination of Thallium in Drinking Water and Source Water by Using Inductively Coupled Plasma-mass Spectrometry. Fujian Anal. Test. 2012, 3, 27–29. [Google Scholar]
- Asadoulahi, T.; Dadfarnia, S.; Shabani, A.M.H. Determination of thallium traces by ETAAS after on-line matrix separation and preconcentration in a flow injection system. J. Braz. Chem. Soc. 2007, 18, 1353–1359. [Google Scholar] [CrossRef] [Green Version]
- Lukaszewski, Z.; Jakubowska, M.; Zembrzuski, W.; Karbowska, B.; Pasieczna, A. Flow-injection differential-pulse anodic stripping voltammetry as a tool for thallium monitoring in the environment. Electroanalysis 2010, 22, 1963–1966. [Google Scholar] [CrossRef]
- Bateman, T.M. Cardiac positron emission tomography and the role of adenosine pharmacologic stress. Am. J. Cardiol. 2004, 94, 19D–24D. [Google Scholar] [CrossRef] [PubMed]
- Fukami, M.; Tamura, K.; Nakamura, Y.; Nakatsukasa, S.; Sasaki, M. Evaluating the effectiveness of a single CT method for attenuation correction in stress-rest myocardial perfusion imaging with thallium-201 chloride SPECT. Radiol. Phys. Technol. 2020, 13, 20–26. [Google Scholar] [CrossRef]
- Lee, S.K.; Jung, J.I.; O, J.H.; Kim, H.W.; Youn, H.J. Coronary-to-pulmonary artery fistula in adults: Evaluation with thallium-201 myocardial perfusion SPECT. PLoS ONE 2017, 12, e0189269. [Google Scholar] [CrossRef] [Green Version]
- Grunwald, A.M.; Watson, D.D.; Holzgrefe, H.H.; Irving, J.F.; Beller, G.A. Myocardial thallium-201 kinetics in normal and ischemic myocardium. Circulation 1981, 64, 610–618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anagnostopoulos, C.; Davies, G.; Flint, J.; Harbinson, M.; Hilson, A.; Kelion, A.; Lahiri, A.; Lim, E.; Prvulovich, L.; Sabharwal, N.; et al. Setting up a myocardial perfusion scintigraphy service: Clinical and business aspects. Heart 2005, 91 (Suppl. S4), iv6–iv14. [Google Scholar] [PubMed] [Green Version]
- Fathala, A. Myocardial perfusion scintigraphy: Techniques, interpretation, indications and reporting. Ann. Saudi. Med. 2011, 31, 625–634. [Google Scholar] [CrossRef]
- Kubo, T.; Shimose, S.; Fujimori, J.; Furuta, T.; Ochi, M. Quantitative 201thallium scintigraphy for prediction of histological response to neoadjuvant chemotherapy in osteosarcoma; systematic review and meta-analysis. Surg. Oncol. 2015, 24, 194–199. [Google Scholar] [CrossRef]
- Murata, H.; Horie, N.; Matsui, T.; Akai, T.; Ueda, H.; Oshima, Y.; Konishi, E.; Kubo, T. Clinical usefulness of thallium-201 scintigraphy and magnetic resonance imaging in the diagnosis of chondromyxoid fibroma. Ann. Nucl. Med. 2008, 22, 221–224. [Google Scholar] [CrossRef]
- Koto, K.; Murata, H.; Sakabe, T.; Matsui, T.; Horie, N.; Sawai, Y.; Tsuji, Y.; Kubo, T. Magnetic resonance imaging and thallium-201 scintigraphy for the diagnosis of localizes pigmented villonodular synovitis arising from the elbow: A case report and review of the literature. Exp. Ther. Med. 2013, 5, 1277–1280. [Google Scholar] [CrossRef] [Green Version]
- Inai, R.; Shinya, T.; Tada, A.; Sato, S.; Fujiwara, T.; Takeda, K.; Kunisada, T.; Yanai, H.; Ozaki, T.; Kanazawa, S. Diagnostic value of Thallium-201 scintigraphy in differentiating malignant bone tumors from benign bone lesions. Ann. Nucl. Med. 2015, 29, 674–681. [Google Scholar] [CrossRef] [Green Version]
- Jo, I.; Gould, D.; Schlicht, S.; Taubman, K.; Choong, P. Diagnostic accuracy of functional imaging modalities for chondrosarcoma: A systematic review and meta-analysis. J. Bone Oncol. 2019, 19, 100262. [Google Scholar] [CrossRef]
- Genchi, G.; Sinicropi, M.S.; Lauria, G.; Carocci, A.; Catalano, A. The effects of cadmium toxicity. Int. J. Environ. Res. Public Health 2020, 17, 3782. [Google Scholar] [CrossRef]
- Genchi, G.; Lauria, G.; Catalano, A.; Carocci, A.; Sinicropi, M.S. The double face of metals: The intriguing case of chromium. Appl. Sci. 2021, 11, 638. [Google Scholar] [CrossRef]
- Genchi, G.; Carocci, A.; Lauria, G.; Sinicropi, M.S.; Catalano, A. Nickel: Human health and environmental toxicology. Int. Environ. Res. Public Health 2020, 17, 679. [Google Scholar] [CrossRef] [Green Version]
- LaCoste, C.; Robinson, B.; Brooks, R. Uptake of thallium by vegetables: Its significance for human health, phytoremediation, and phytomining. J. Plant. Nut. 2001, 24, 1205–1215. [Google Scholar] [CrossRef]
- Augustynowicz, J.; Tokarz, K.; Baran, A.; Płachno, B.J. Phytoremediation of water polluted by thallium, cadmium, zinc, and lead with the use of macrophyte Callitriche cophocarpa. Arch. Environ. Contam. Toxicol. 2014, 66, 572–581. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Huang, T.; Zhang, M.; Guo, X.; Yuan, Z. Studies on the capability and behavior of adsorption of thallium on nano-Al2O3. J. Hazard. Mater. 2008, 157, 352–357. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Zhang, P.; Borthwick, A.G.; Chen, H.; Ni, J. Adsorption mechanisms of thallium (I) and thallium (III) by titanate nanotubes: Ion-exchange and co-precipitation. J. Colloid Interf. Sci. 2014, 423, 67–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, Z.; Xiong, Y.; Cheng, X.; Hou, X.; Yang, Y.; Tian, Y.; You, J.; Xu, L. Adsorptive removal of trace thallium(I) from wastewater: A review and new perspectives. J. Hazard. Mater. 2020, 393, 122378. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Mechanism of thallium action.

Figure 2.
Structures of thallium chelating agents.


{kind=link}
{kind=link}
Table 1.
Physical and chemical properties of thallium (Tl).
| Atomic number | 81 |
| Atomic weight | 204.38 u |
| Thallium isotopes (41) | from 176 u to 216 u |
| Electronic configuration | [Xe] 4f145d106s26p1 |
| Melting point | 304 °C |
| Boiling point | 1473 °C |
| Density at 20 °C | 11.85 g/cm3 |
| Atomic radius | 170 pm |
| Van der Waals radius | 220 pm |
| Heat of fusion | 4.14 KJ/mol |
| Heat of vaporization | 165 KJ/mol |
| Pauling electronegativity number | 1.62 |
| First ionization energy | 589.4 KJ/mol |
| Second ionization energy | 1971.4 KJ/mol |
| Third ionization energy | 2878 KJ/mol |
| Electrical resistivity at 20 °C | 0.18 m |
Table 2.
Symptoms of thallium exposure.
| References | |
|---|---|
| Cardiac symptoms | [33,34] |
| Coma | |
| Hypotension | |
| Lethargy | |
| Tachycardia | |
| Dermatological symptoms | [34] |
| Alopecia (after about 3 weeks) | |
| Anhidrosis | |
| Hypohidrosis | |
| Mees lines on the nails (after about 1 month) | |
| Gastrointestinal symptoms | [34] |
| Diarrhea or constipation | |
| Nausea and vomiting | |
| Stool containing blood | |
| Hematologic symptoms | [34] |
| Anemia | |
| Eosinophilia | |
| Leukocytosis | |
| Neutrophilia | |
| Thrombocytopenia | |
| Neurologic symptoms (after 3–5 days) | [33,34] |
| Ataxia | |
| Convulsion | |
| Death | |
| Distal muscle weakness of the hands or feet | |
| Hallucination | |
| Headache | |
| Insomnia | |
| Paresthesia | |
| Tremor | |
| Ocular symptoms | [34] |
| Atrophy of the optic nerve | |
| Cranial nerve 7th palsy | |
| Nystagmus | |
| Lens opacity | |
| Optic neuropathy | |
| Ptosis |
Table 3.
Food sources of thallium.
| Food | Tl (µg/Kg) | References |
|---|---|---|
| Bream | 800–8600 | [41] |
| Brook trout | >3000 | [41] |
| Mollusks | 350–2930 | [41] |
| Shellfish | 350–2930 | [41] |
| Fish | 350–2930 | [41] |
| Red and white wines | 40–480 | [41] |
| Vegetables and cereals | 20–300 | [41] |
| Red meat | 50–70 | [41] |
| Potatoes (dry weight) | 20–30 | [41,53] |
| Milk | 10–30 | [53,54] |
| Poultry | 2.8 | [54] |
| Porcine (dry weight) | 1.7 | [55] |
| Tobacco per cigarette | 1.1–2.4 | [56] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Genchi, G.; Carocci, A.; Lauria, G.; Sinicropi, M.S.; Catalano, A. Thallium Use, Toxicity, and Detoxification Therapy: An Overview. Appl. Sci. 2021, 11, 8322. https://doi.org/10.3390/app11188322
AMA Style
Genchi G, Carocci A, Lauria G, Sinicropi MS, Catalano A. Thallium Use, Toxicity, and Detoxification Therapy: An Overview. Applied Sciences. 2021; 11(18):8322. https://doi.org/10.3390/app11188322
Chicago/Turabian StyleGenchi, Giuseppe, Alessia Carocci, Graziantonio Lauria, Maria Stefania Sinicropi, and Alessia Catalano. 2021. "Thallium Use, Toxicity, and Detoxification Therapy: An Overview" Applied Sciences 11, no. 18: 8322. https://doi.org/10.3390/app11188322
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.