
Ozonized Water Administration in Peri-Implant Mucositis Sites: A Randomized Clinical Trial

 ,
,  , ,
, , 
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Materials
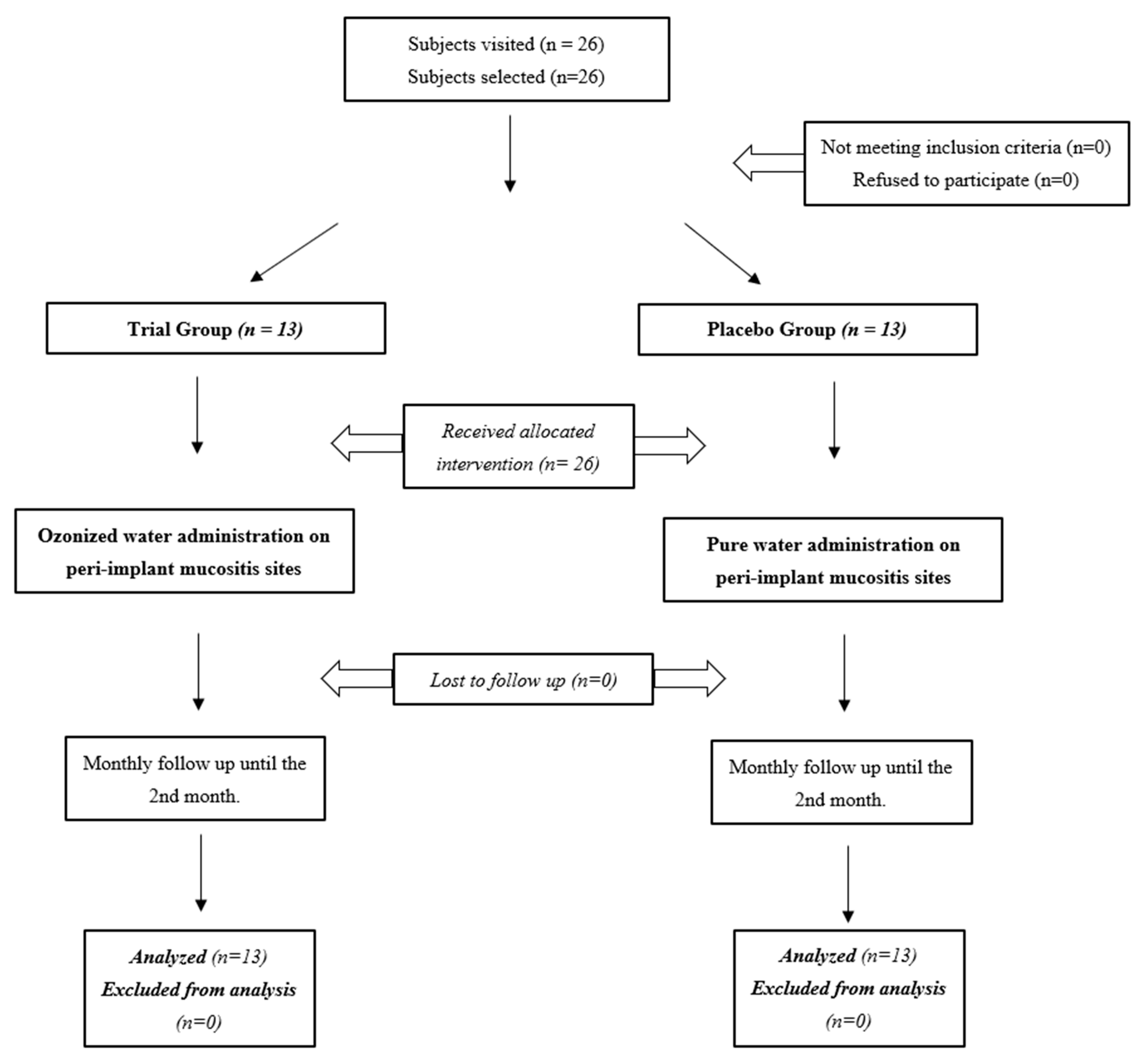
2.2. Randomized Clinical Trial
2.2.1. Trial Design
2.2.2. Participants
2.2.3. Interventions and Outcomes
2.2.4. Sample Size
2.2.5. Randomization and Blinding
2.2.6. Statistical Methods
3. Results
3.1. Baseline Characteristics
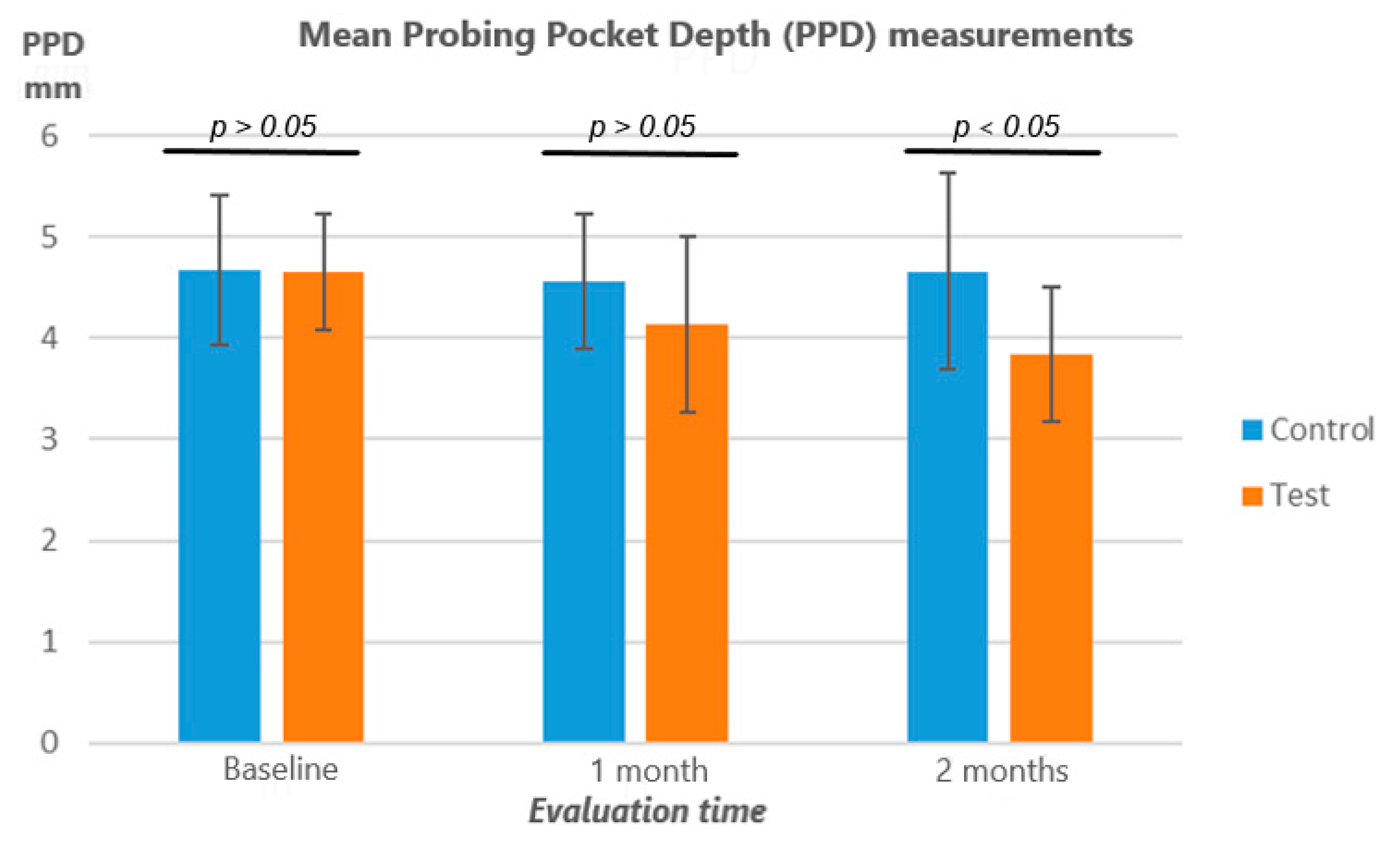
3.2. Probing Pocket Depth (PPD)
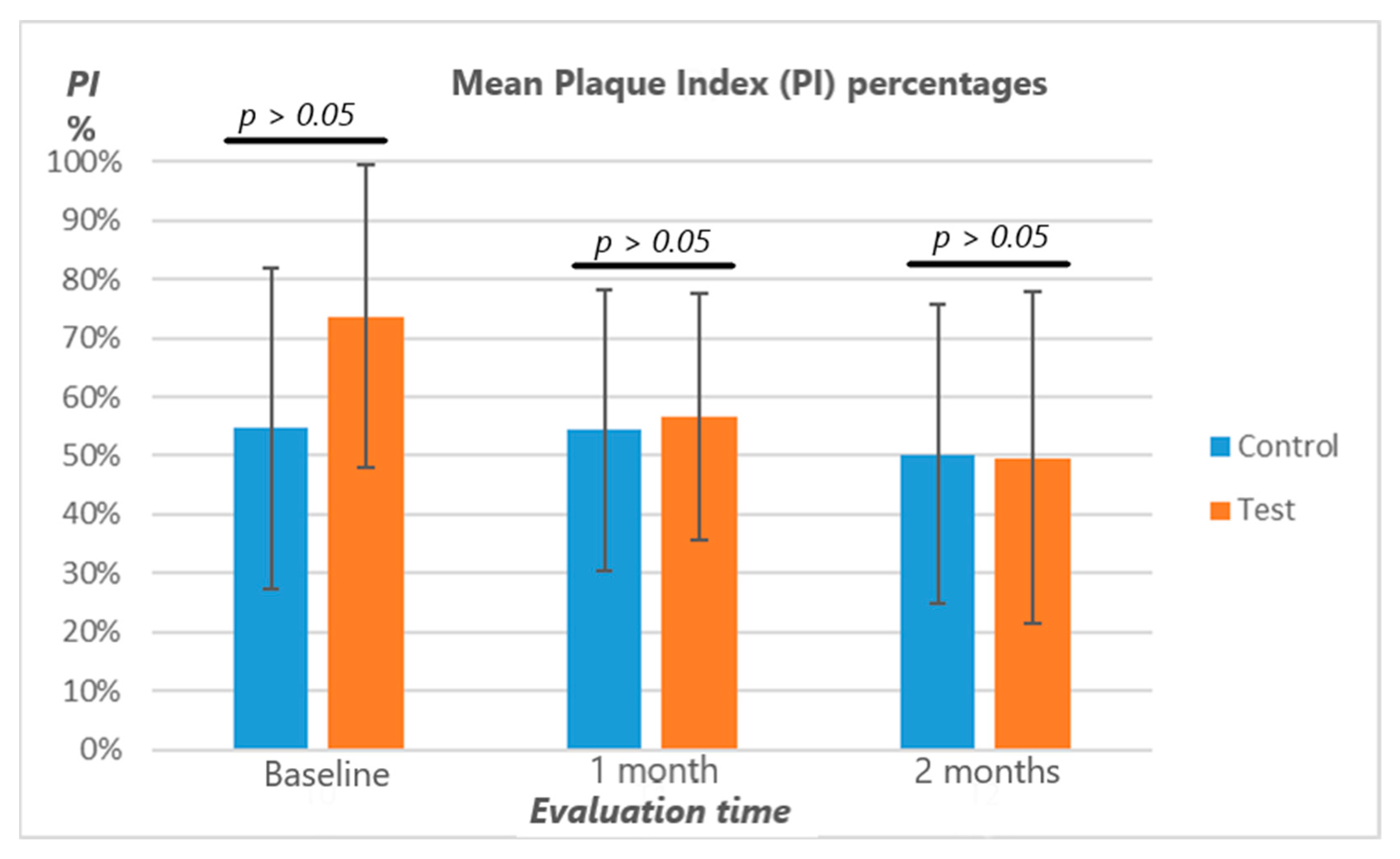
3.3. Plaque Index (PI%)
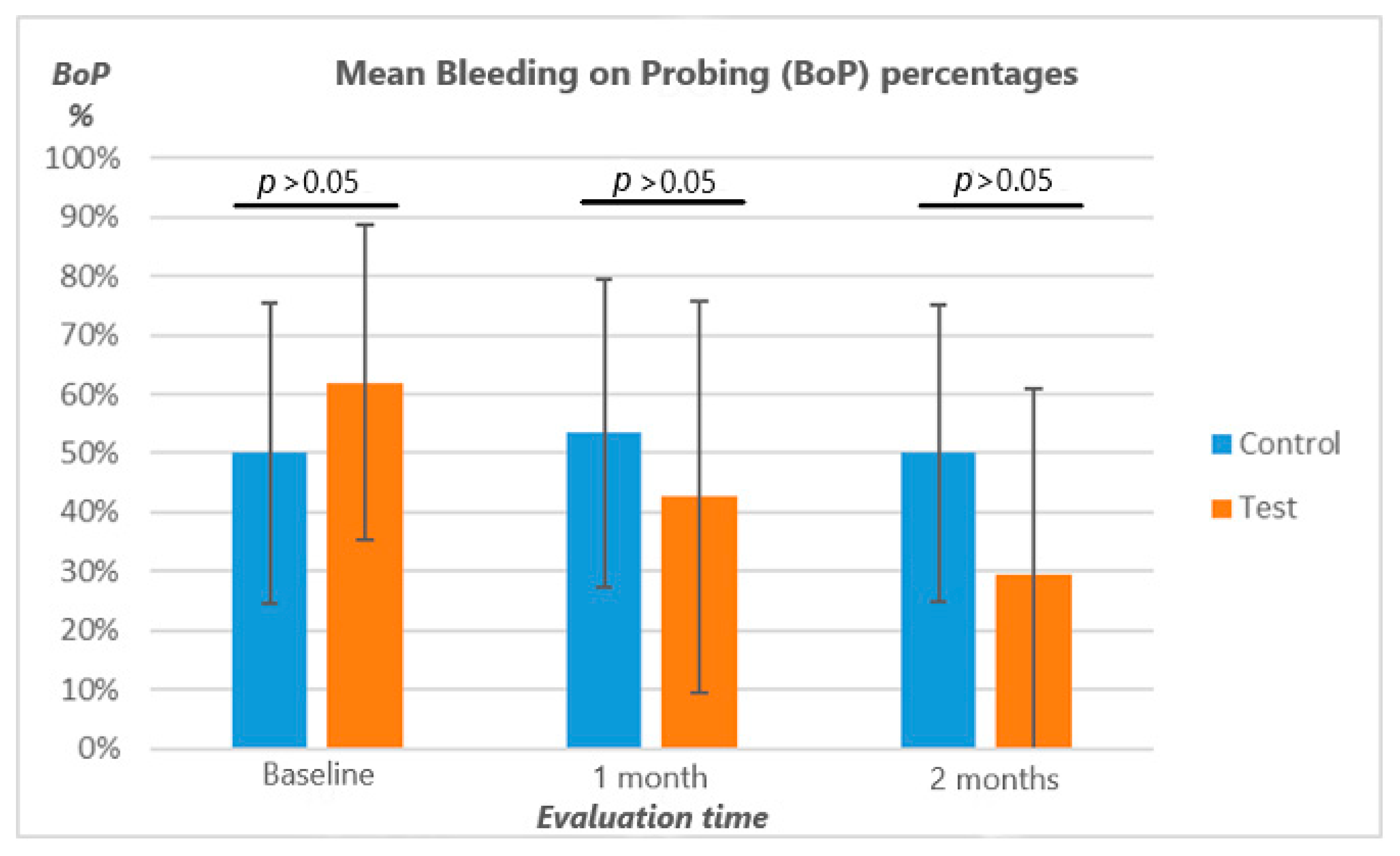
3.4. Bleeding on Probing (BOP)
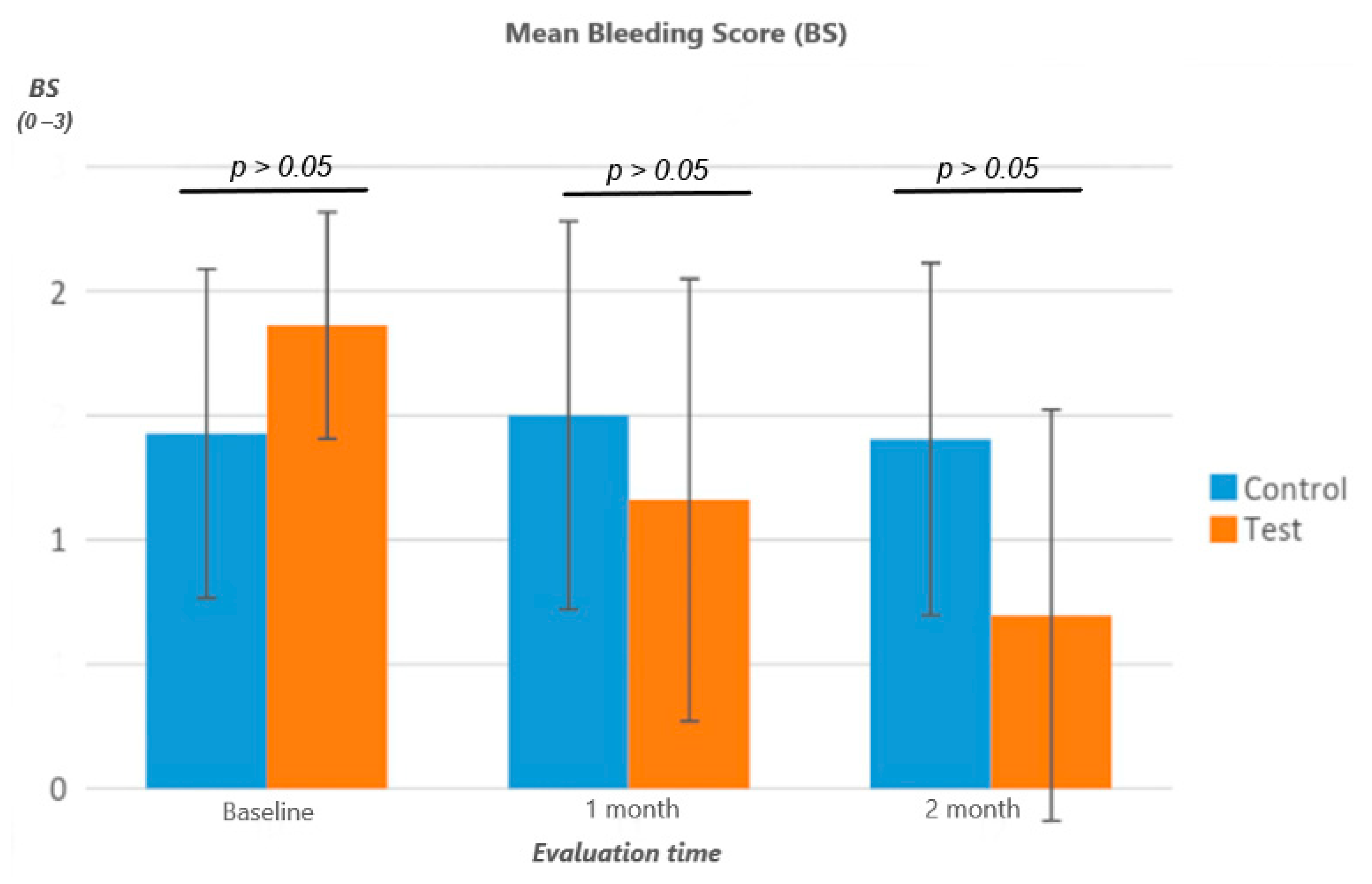
3.5. Bleeding Score
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sechi, L.A.; Lezcano, I.; Nunez, N.; Espim, M.; Duprè, I.; Pinna, A.; Molicotti, P.; Fadda, G.; Zanetti, S. Antibacterial activity of ozonized sunflower oil (Oleozon). J. Appl. Microbiol. 2001, 90, 279–284. [Google Scholar] [CrossRef] [Green Version]
- Lezcano, I.; Nuñez, N.; Espino, M.; Gómez, M. Antibacterial activity of ozonized sunflower oil, oleozon, against Staphylococcus aureus and Staphylococcus epidermidis. Ozone Sci. Eng. 2000, 22, 207–214. [Google Scholar] [CrossRef]
- Mascarenhas, L.A.B.; Oliveira, F.O.; da Silva, E.S.; dos Santos, L.M.C.; de Alencar Pereira Rodrigues, L.; Neves, P.R.F.; Santos, A.Á.B.; Moreira, G.A.F.; Lobato, G.M.; Nascimento, C.; et al. Technological Advances in Ozone and Ozonized Water Spray Disinfection Devices. Appl. Sci. 2021, 11, 3081. [Google Scholar] [CrossRef]
- Giuroiu, C.L.; Andrian, S.; Stoleriu, S.; Scurtu, M.; Țănculescu, O.; Poroch, V.; Sălceanu, M. The Combination of Diode Laser and Ozonated Water in the Treatment of Complicated Pulp Gangrene. Appl. Sci. 2020, 10, 4203. [Google Scholar] [CrossRef]
- Silva, V.; Peirone, C.; Capita, R.; Alonso-Calleja, C.; Marques-Magallanes, J.A.; Pires, I.; Maltez, L.; Pereira, J.E.; Igrejas, G.; Poeta, P. Topical Application of Ozonated Oils for the Treatment of MRSA Skin Infection in an Animal Model of Infected Ulcer. Biology 2021, 10, 372. [Google Scholar] [CrossRef] [PubMed]
- Di Mauro, R.; Cantarella, G.; Bernardini, R.; Di Rosa, M.; Barbagallo, I.; Distefano, A.; Longhitano, L.; Vicario, N.; Nicolosi, D.; Lazzarino, G.; et al. The Biochemical and Pharmacological Properties of Ozone: The Smell of Protection in Acute and Chronic Diseases. Int. J. Mol. Sci. 2019, 20, 634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monzillo, V.; Lallitto, F.; Russo, A.; Poggio, C.; Scribante, A.; Arciola, C.R.; Bertuccio, F.R.; Colombo, M. Ozonized Gel Against Four Candida Species: A Pilot Study and Clinical Perspectives. Materials 2020, 13, 1731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallo, S.; Scribante, A. Ozone therapy in dentistry: From traditional applications towards innovative ones. A review of the literature. IOP Conf. Ser. Earth Environ. Sci. 2021, 707, 012001. [Google Scholar] [CrossRef]
- Suh, Y.; Shrey, P.; Re, K.; Gandhi, J.; Joshi, G. Clinical utility of ozone therapy in dental and oral medicine. Med. Gas. Res. 2019, 9, 163–167. [Google Scholar] [PubMed]
- Colombo, M.; Gallo, S.; Garofoli, A.; Poggio, C.; Arciola, C.R.; Scribante, A. Ozone Gel in Chronic Periodontal Disease: A Randomized Clinical Trial on the Anti-Inflammatory Effects of Ozone Application. Biology 2021, 10, 625. [Google Scholar] [CrossRef]
- El Hadary, A.A.; Yassin, H.H.; Mekhemer, S.T.; Holmes, J.C.; Grootveld, M. Evaluation of the effect of ozonated plant oils on the quality of osseointegration of dental implants under the influence of Cyclosporin A an in vivo study. J. Oral Implantol. 2011, 37, 247–257. [Google Scholar] [CrossRef]
- Yücesoy, T.; Seker, E.D.; Cenkcı, E.; Yay, A.; Alkan, A. Histologic and Biomechanical Evaluation of Osseointegrated Miniscrew Implants Treated with Ozone Therapy and Photobiomodulation at Different Loading Times. Int. J. Oral. Maxillofac. Implants 2019, 34, 1337–1345. [Google Scholar] [CrossRef] [PubMed]
- Karaca, I.R.; Ergun, G.; Ozturk, D.N. Is Low-level laser therapy and gaseous ozone application effective on osseointegration of immediately loaded implants? Niger J. Clin. Pract. 2018, 21, 703–710. [Google Scholar] [CrossRef]
- Shekhar, A.; Srivastava, S.; Kumar Bhati, L.; Chaturvedi, A.; Singh, S.; Agarwal, B.; Arora, K. An evaluation of the effect of ozone therapy on tissues surrounding dental implants. Int. Immunopharmacol. 2021, 96, 107588. [Google Scholar] [CrossRef] [PubMed]
- Butera, A.; Gallo, S.; Maiorani, C.; Molino, D.; Chiesa, A.; Preda, C.; Esposito, F.; Scribante, A. Probiotic Alternative to Chlorhexidine in Periodontal Therapy: Evaluation of Clinical and Microbiological Parameters. Microorganisms 2020, 9, 69. [Google Scholar] [CrossRef]
- Könönen, E.; Gursoy, M.; Gursoy, U.K. Periodontitis: A Multifaceted Disease of Tooth-Supporting Tissues. J. Clin. Med. 2019, 8, 1135. [Google Scholar] [CrossRef] [Green Version]
- Roos-Jansaker, A.M.; Lindahl, C.; Renvert, H.; Renvert, S. Nine- to fourteen-year follow-up of implant treatment. Part I: Implant loss and associations to various factors. J. Clin. Periodontol. 2006, 33, 283–289. [Google Scholar] [CrossRef]
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-implant dis-eases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45, S286–S291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heitz-Mayfield, L.J.A.; Salvi, G.E. Peri-implant mucositis. J. Clin. Periodontol. 2018, 45, S237–S245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ericsson, I.; Berglundh, T.; Marinello, C.; Liljenberg, B.; Lindhe, J. Long-standing plaque and gingivitis at implants and teeth in thedog. Clin. Oral Implants Res. 1992, 3, 99–103. [Google Scholar] [CrossRef]
- Khammissa, R.A.; Feller, L.; Meyerov, R.; Lemmer, J. Peri-implant mucositis and peri-implantitis: Clinical and histopathological characteristics and treatment. S. Afr. Dent. J. 2012, 67, 122, 124–126. [Google Scholar]
- Aimetti, M.; Mariani, G.M.; Ferrarotti, F.; Ercoli, E.; Liu, C.C.; Romano, F. Adjunctive efficacy of diode laser in the treatment of peri-implant mucositis with mechanical therapy: A randomized clinical trial. Clin. Oral Implants Res. 2019, 30, 429–438. [Google Scholar] [CrossRef] [PubMed]
- Ji, Y.J.; Tang, Z.H.; Wang, R.; Cao, J.; Cao, C.F.; Jin, L.J. Effect of glycine powder air-polishing as an adjunct in the treatment of peri-implant mucositis: A pilot clinical trial. Clin. Oral Implants Res. 2014, 25, 683–689. [Google Scholar] [CrossRef] [PubMed]
- Schulz, K.F.; Chalmers, I.; Grimes, D.A.; Altman, D.G. Assessing the quality of randomization from reports of controlled trials published in obstetrics and gynecology journals. JAMA 1994, 272, 125–128. [Google Scholar] [CrossRef]
- Ermetici, M.; Segù, M.; Butera, A. Comparison to the scanning electron microscope of professional dental hygiene methods on metal-free layered structures and metal-free monolithic structures processed by different polymerization cycles. Minerva Stomatol. 2014, 63, 189–202. [Google Scholar] [PubMed]
- Sahm, N.; Becker, J.; Santel, T.; Schwarz, F. Non-surgical treatment of peri-implantitis using an air-abrasive device or mechanical debridement and local application of chlorhexidine: A prospective, randomized, controlled clinical study. J. Clin. Periodontol. 2011, 38, 872–878. [Google Scholar] [CrossRef]
- De Araujo, N.; Capelas, C.; Alves, A.; Almeida, T.; Carvalho, R.; Antunes, E.; Oliveira, D.; Cardador, A.; Maló, P. Non-surgical treatment of peri-implant pathology. Int. J. Dent. Hygiene 2006, 4, 84–90. [Google Scholar] [CrossRef]
- Louropoulou, A.; Slot, D.E.; van der Weijden, F.A. Titanium surface alterations following the use of different mechanical instruments: A systematic review. Clin. Oral Implants Res. 2012, 23, 643–658. [Google Scholar] [CrossRef] [PubMed]
- McKenna, D.F.; Borzabadi-Farahani, A.; Lynch, E. The effect of subgingival ozone and/or hydrogen peroxide on the development of peri-implant mucositis: A double-blind randomized controlled trial. Int. J. Oral Maxillofac. Implants 2013, 28, 1483–1489. [Google Scholar] [CrossRef] [Green Version]
- Isler, S.C.; Unsal, B.; Soysal, F.; Ozcan, G.; Peker, E.; Karaca, I.R. The effects of ozone therapy as an adjunct to the surgical treatment of peri-implantitis. J. Periodontal Implant Sci. 2018, 48, 136–151. [Google Scholar] [CrossRef]
- Preda, C.; Butera, A.; Pelle, S.; Pautasso, E.; Chiesa, A.; Esposito, F.; Oldoini, G.; Scribante, A.; Genovesi, A.M.; Cosola, S. The Efficacy of Powered Oscillating Heads vs. Powered Sonic Action Heads Toothbrushes to Maintain Periodontal and Peri-Implant Health: A Narrative Review. Int. J. Environ. Res. Public. Health 2021, 18, 1468. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Appointment | Procedures |
|---|---|
| ● Signature to the informed consent for the study. | |
| ● Assessment of periodontal clinical indexes. | |
| ● Professional supragingival and subgingival oral hygiene. | |
| Baseline (T0) | ● Supragingival and subgingival decontamination of glycine powders. |
| Trial Group: administration of ozonized water on peri-implant mucositis sites. | |
| Placebo Group: administration of pure water on peri-implant mucositis sites. | |
| ● Assessment of periodontal clinical indexes. | |
| ● Supragingival and subgingival decontamination of glycine powders. | |
| After 1 month (T1) After 2 months (T2) | Trial Group: administration of ozonized water on peri-implant mucositis sites. |
| Placebo Group: administration of water only on peri-implant mucositis sites. |
| Group | Time | Mean | St Dev | Min | Median | Max | Intragroup Differences * | Intergroup Differences † |
|---|---|---|---|---|---|---|---|---|
| Trial Group | T0 | 4.65 | 0.57 | 4.00 | 4.70 | 5.71 | A | T0: ns |
| T1 | 4.14 | 0.87 | 3.00 | 4.00 | 5.82 | B | T1: ns | |
| T2 | 3.84 | 0.67 | 3.00 | 3.63 | 5.24 | C | T2: p < 0.05 | |
| Placebo Group | T0 | 4.67 | 0.75 | 4.00 | 4.50 | 6.33 | A | |
| T1 | 4.55 | 0.66 | 3.33 | 4.75 | 5.54 | A | ||
| T2 | 4.66 | 0.96 | 3.25 | 4.34 | 6.91 | A |
| Group | Time | Mean | St Dev | Min | Median | Max | Intragroup Differences * | Intergroup Differences † |
|---|---|---|---|---|---|---|---|---|
| Trial Group | T0 | 73.65 | 25.67 | 25.00 | 75.00 | 100.00 | A | T0: ns |
| T1 | 56.71 | 21.02 | 25.00 | 50.00 | 100.00 | B | T1: ns | |
| T2 | 49.68 | 28.13 | 0.00 | 50.00 | 100.00 | B | T2: ns | |
| Placebo Group | T0 | 54.62 | 27.38 | 22.50 | 50.00 | 100.00 | B | |
| T1 | 54.31 | 23.86 | 25.00 | 50.00 | 87.50 | B | ||
| T2 | 50.29 | 25.54 | 0.00 | 50.00 | 100.00 | B |
| Group | Time | Mean | St Dev | Min | Median | Max | Intragroup Differences * | Intergroup Differences † |
|---|---|---|---|---|---|---|---|---|
| Trial Group | T0 | 61.96 | 26.69 | 16.67 | 63.33 | 100.00 | A | T0: ns |
| T1 | 42.60 | 33.15 | 0.00 | 33.33 | 100.00 | B | T1: ns | |
| T2 | 29.55 | 31.43 | 0.00 | 29.17 | 100.00 | C | T2: ns | |
| Placebo Group | T0 | 50.14 | 25.43 | 16.67 | 50.00 | 100.00 | D | |
| T1 | 53.46 | 26.10 | 16.67 | 50.00 | 100.00 | D | ||
| T2 | 50.00 | 25.21 | 15.33 | 50.00 | 100.00 | D |
| Group | Time | Mean | St Dev | Min | Median | Max | Intragroup Differences * | Intergroup Differences † |
|---|---|---|---|---|---|---|---|---|
| Trial Group | T0 | 1.86 | 0.46 | 1.00 | 2.00 | 3.00 | A | T0: ns |
| T1 | 1.16 | 0.89 | 0.00 | 1.00 | 3.00 | B | T1: ns | |
| T2 | 0.70 | 0.83 | 0.00 | 0.50 | 3.00 | C | T2: ns | |
| Placebo Group | T0 | 1.43 | 0.66 | 0.55 | 1.25 | 2.50 | D | |
| T1 | 1.50 | 0.78 | 0.60 | 1.25 | 3.00 | D | ||
| T2 | 1.40 | 0.71 | 0.50 | 1.21 | 3.00 | D |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Butera, A.; Gallo, S.; Pascadopoli, M.; Luraghi, G.; Scribante, A. Ozonized Water Administration in Peri-Implant Mucositis Sites: A Randomized Clinical Trial. Appl. Sci. 2021, 11, 7812. https://doi.org/10.3390/app11177812
Butera A, Gallo S, Pascadopoli M, Luraghi G, Scribante A. Ozonized Water Administration in Peri-Implant Mucositis Sites: A Randomized Clinical Trial. Applied Sciences. 2021; 11(17):7812. https://doi.org/10.3390/app11177812
Chicago/Turabian StyleButera, Andrea, Simone Gallo, Maurizio Pascadopoli, Gabriele Luraghi, and Andrea Scribante. 2021. "Ozonized Water Administration in Peri-Implant Mucositis Sites: A Randomized Clinical Trial" Applied Sciences 11, no. 17: 7812. https://doi.org/10.3390/app11177812