
Linking Artificial Light at Night with Human Health via a Multi-Component Framework: A Systematic Evidence Map


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Objectives and Scope
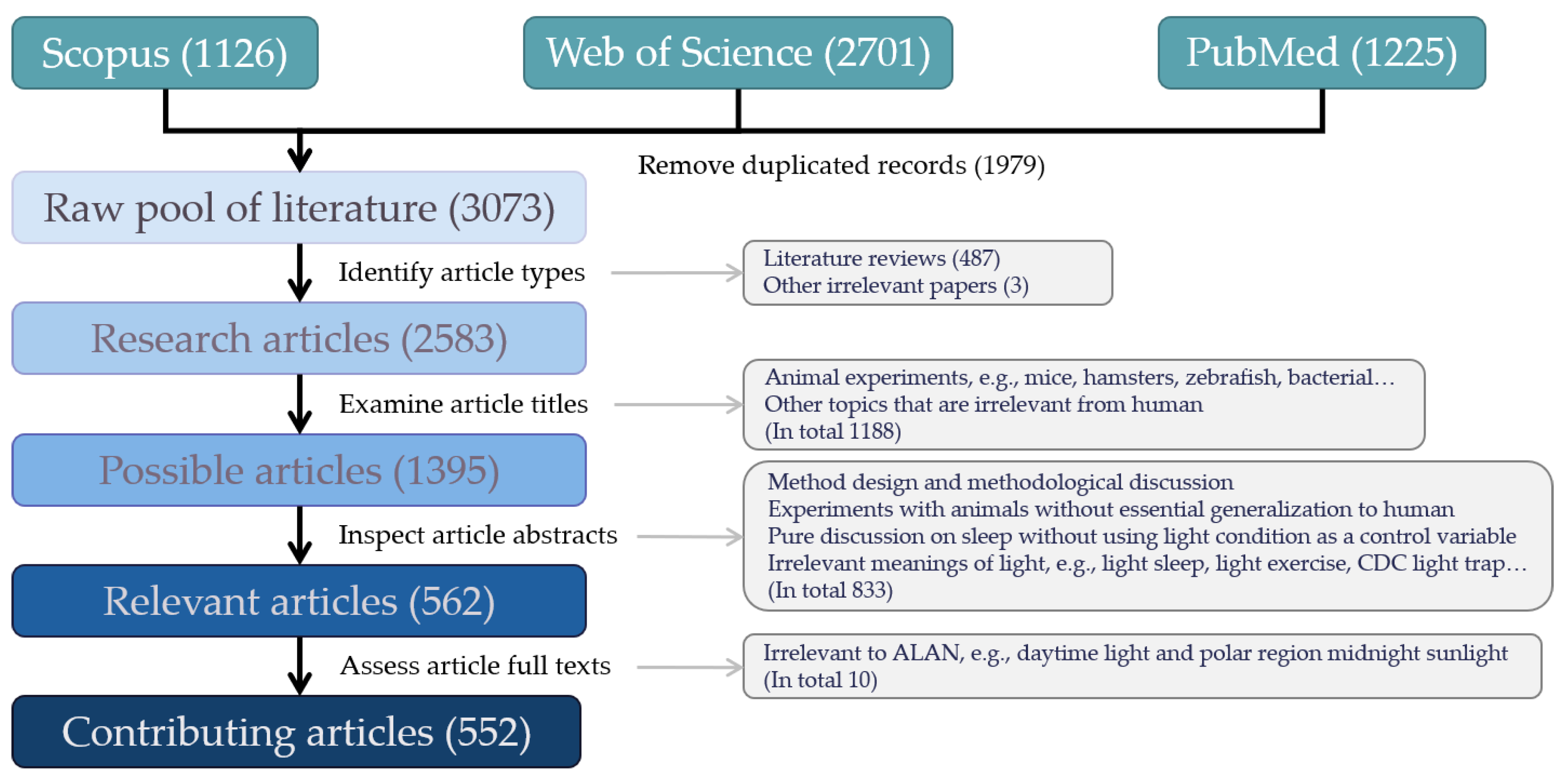
2.2. Initial Generalized Search and Literature Screening
2.3. Data Extraction and Study Quality Assessment
3. Results
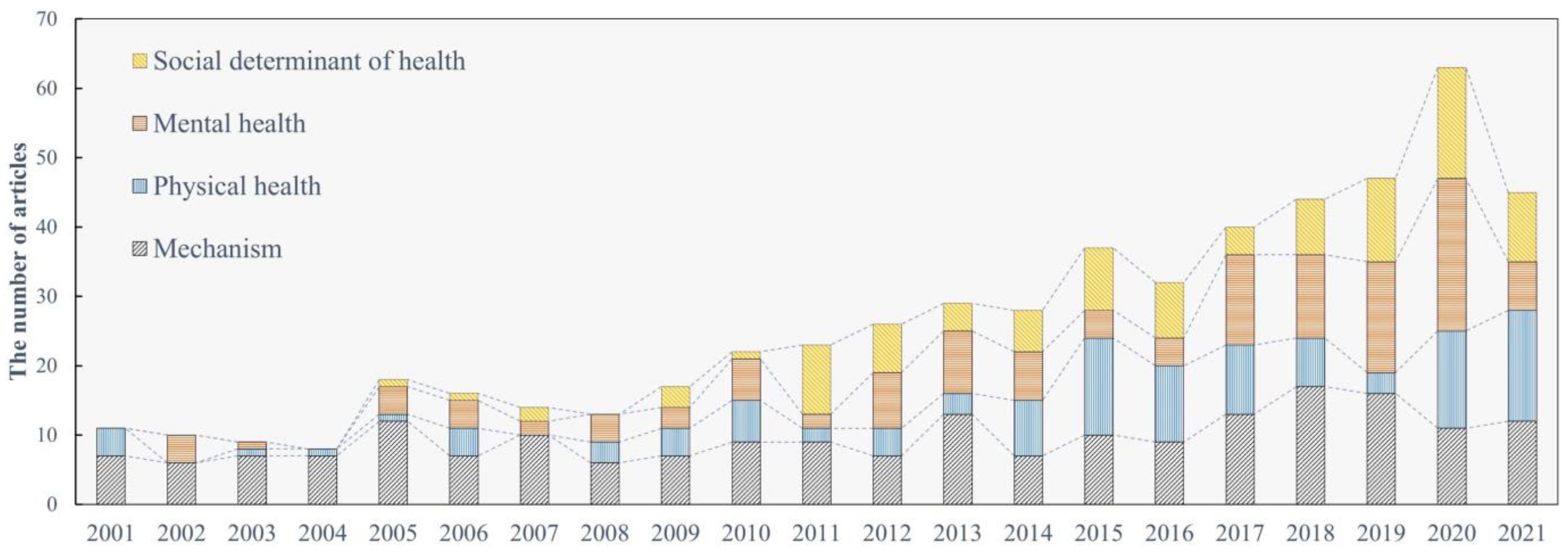
3.1. Research on ALAN’s Health Effects on Human Health in the Last Two Decades
3.2. How ALAN May Affect Human Health
3.3. Exposure to ALAN and Human Physical Health
3.4. Exposure to ALAN and Human Mental Health
3.5. ALAN as a Social Determinant of Human Health and Safety
3.6. Indirect Effects of ALAN on Human Health
3.7. A Framework for Linking ALAN with Human Health
4. Discussion
4.1. From Lab Experiments to Epidemiological Investigations
4.2. From Overemphasizing Negative Effects to a Multi-Component Framework
4.3. ALAN as a Social Determinant of Human Health and Social Justice
4.4. Limitations of This Systematic Evidence Map
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- James, S.R.; Dennell, R.; Gilbert, A.S.; Lewis, H.T.; Gowlett, J.; Lynch, T.F.; McGrew, W.; Peters, C.R.; Pope, G.G.; Stahl, A.B. Hominid use of fire in the Lower and Middle Pleistocene: A review of the evidence [and comments and replies]. Curr. Anthropol. 1989, 30, 1–26. [Google Scholar] [CrossRef]
- Sanderson, S.W.; Simons, K.L. Light emitting diodes and the lighting revolution: The emergence of a solid-state lighting industry. Res. Policy 2014, 43, 1730–1746. [Google Scholar] [CrossRef]
- DiLaura, D. A brief history of lighting. Opt. Photonics News 2008, 19, 22–28. [Google Scholar] [CrossRef]
- WHO. Constitution of the World Health Organization. 2020. Available online: https://apps.who.int/gb/bd/PDF/bd47/EN/constitution-en.pdf?fbclid=IwAR3bSPmEMO5GR9oP9tFp5lD0BZFJM-fAtc12ogjAp8kFTD2t_fahFbfFeNY (accessed on 14 January 2022).
- WHO. Mental health: Strengthening our Response. 30 March 2018. Available online: https://cdn.ymaws.com/www.safestates.org/resource/resmgr/connections_lab/glossary_citation/mental_health_strengthening_.pdf (accessed on 20 January 2022).
- WHO. Social Determinants of Health. Available online: https://www.who.int/health-topics/social-determinants-of-health#tab=tab_1 (accessed on 12 January 2022).
- Xiao, Q.; James, P.; Breheny, P.; Jia, P.; Park, Y.; Zhang, D.; Fisher, J.A.; Ward, M.H.; Jones, R.R. Outdoor light at night and postmenopausal breast cancer risk in the NIH-AARP diet and health study. Int. J. Cancer 2020, 147, 2363–2372. [Google Scholar] [CrossRef] [PubMed]
- Stevens, R.G. Light-at-night, circadian disruption and breast cancer: Assessment of existing evidence. Int. J. Epidemiol. 2009, 38, 963–970. [Google Scholar] [CrossRef]
- Rybnikova, N.; Portnov, B.A. Population-level study links short-wavelength nighttime illumination with breast cancer incidence in a major metropolitan area. Chronobiol. Int. 2018, 35, 1198–1208. [Google Scholar] [CrossRef] [PubMed]
- Watson, L.A.; Phillips, A.J.K.; Hosken, I.T.; McGlashan, E.M.; Anderson, C.; Lack, L.C.; Lockley, S.W.; Rajaratnam, S.M.W.; Cain, S.W. Increased sensitivity of the circadian system to light in delayed sleep-wake phase disorder. J. Physiol. 2018, 596, 6249–6261. [Google Scholar] [CrossRef] [PubMed]
- Joo, E.Y.; Abbott, S.M.; Reid, K.J.; Wu, D.; Kang, J.; Wilson, J.; Zee, P.C. Timing of light exposure and activity in adults with delayed sleep-wake phase disorder. Sleep Med. 2017, 32, 259–265. [Google Scholar] [CrossRef]
- Kloog, I.; Haim, A.; Stevens, R.G.; Portnov, B.A. Global co-distribution of light at night (LAN) and cancers of prostate, colon, and lung in men. Chronobiol. Int. 2009, 26, 108–125. [Google Scholar] [CrossRef]
- Srour, B.; Plancoulaine, S.; Andreeva, V.A.; Fassier, P.; Julia, C.; Galan, P.; Hercberg, S.; Deschasaux, M.; Latino-Martel, P.; Touvier, M. Circadian nutritional behaviours and cancer risk: New insights from the NutriNet-sante prospective cohort study. Int. J. Cancer 2018, 143, 2369–2379. [Google Scholar] [CrossRef] [Green Version]
- Obayashi, K.; Saeki, K.; Iwamoto, J.; Ikada, Y.; Kurumatani, N. Independent associations of exposure to evening light and nocturnal urinary melatonin excretion with diabetes in the elderly. Chronobiol. Int. 2014, 31, 394–400. [Google Scholar] [CrossRef] [PubMed]
- Obayashi, K.; Saeki, K.; Iwamoto, J.; Ikada, Y.; Kurumatani, N. Exposure to light at night and risk of depression in the elderly. J. Affect. Disord. 2013, 151, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Esaki, Y.; Obayashi, K.; Saeki, K.; Fujita, K.; Iwata, N.; Kitajima, T. Association between light exposure at night and manic symptoms in bipolar disorder: Cross-sectional analysis of the APPLE cohort. Chronobiol. Int. 2020, 37, 887–896. [Google Scholar] [CrossRef]
- Chinoy, E.D.; Harris, M.P.; Kim, M.J.; Wang, W.; Duffy, J.F. Scheduled evening sleep and enhanced lighting improve adaptation to night shift work in older adults. Occup. Environ. Med. 2016, 73, 869–876. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Figueiro, M.G.; Sahin, L.; Wood, B.; Plitnick, B. Light at night and measures of alertness and performance: Implications for shift workers. Biol. Res. Nurs. 2016, 18, 90–100. [Google Scholar] [CrossRef]
- Lim, Y.M.; Sung, M.H. Home environmental and health-related factors among home fallers and recurrent fallers in community dwelling older Korean women. Int. J. Nurs. Pract. 2012, 18, 481–488. [Google Scholar] [CrossRef]
- Stevens, R.G.; Davis, S. The melatonin hypothesis: Electric power and breast cancer. Environ. Health Perspect. 1996, 104, 135–140. [Google Scholar]
- Hastings, M.H.; Maywood, E.S.; Brancaccio, M. Generation of circadian rhythms in the suprachiasmatic nucleus. Nat. Rev. Neurosci. 2018, 19, 453–469. [Google Scholar] [CrossRef]
- Reszka, E.; Peplonska, B.; Wieczorek, E.; Sobala, W.; Bukowska, A.; Gromadzinska, J.; Lie, J.-A.; Kjuus, H.; Wasowicz, W. Circadian gene expression in peripheral blood leukocytes of rotating night shift nurses. Scand. J. Work Environ. Health 2013, 39, 187–194. [Google Scholar] [CrossRef] [Green Version]
- Cheng, P.; Tallent, G.; Burgess, H.J.; Tran, K.M.; Roth, T.; Drake, C.L. Daytime sleep disturbance in night shift work and the role of PERIOD3. J. Clin. Sleep Med. 2018, 14, 393–400. [Google Scholar] [CrossRef] [Green Version]
- Kervezee, L.; Cuesta, M.; Cermakian, N.; Boivin, D.B. The phase-shifting effect of bright light exposure on circadian rhythmicity in the human transcriptome. J. Biol. Rhythm. 2019, 34, 84–97. [Google Scholar] [CrossRef]
- Resuehr, D.; Wu, G.; Johnson, R.L., Jr.; Young, M.E.; Hogenesch, J.B.; Gamble, K.L. Shift work disrupts circadian regulation of the transcriptome in hospital nurses. J. Biol. Rhythm. 2019, 34, 167–177. [Google Scholar] [CrossRef]
- Aoki, K.; Yokoi, M.; Masago, R.; Iwanaga, K.; Kondo, N.; Katsuura, T. Modification of internal temperature regulation for cutaneous vasodilation and sweating by bright light exposure at night. Eur. J. Appl. Physiol. 2005, 95, 57–64. [Google Scholar] [CrossRef] [PubMed]
- de Blasiis, K.; Mauvieux, B.; Elsworth-Edelsten, C.; Peze, T.; Jouffroy, R.; Hurdiel, R. Photoperiod impact on a sailor’s sleep-wake rhythm and core body temperature in polar environment. Wilderness Environ. Med. 2019, 30, 343–350. [Google Scholar] [CrossRef]
- Cuesta, M.; Boudreau, P.; Cermakian, N.; Boivin, D.B. Skin temperature rhythms in humans respond to changes in the timing of sleep and light. J. Biol. Rhythm. 2017, 32, 257–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- James, F.O.; Cermakian, N.; Boivin, D.B. Circadian rhythms of melatonin, cortisol, and clock gene expression during simulated night shift work. Sleep 2007, 30, 1427–1436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galina, S.D.; Souza, J.C.; Valdez, P.; Azevedo, C.V.M. Daily light exposure, sleep-wake cycle and attention in adolescents from different urban contexts. Sleep Med. 2021, 81, 410–417. [Google Scholar] [CrossRef]
- Schernhammer, E.S.; Laden, F.; Speizer, F.E.; Willett, W.C.; Hunter, D.J.; Kawachi, I.; Colditz, G.A. Rotating night shifts and risk of breast cancer in women participating in the nurses’ health study. J. Natl. Cancer Inst. 2001, 93, 1563–1568. [Google Scholar] [CrossRef] [Green Version]
- Macchi, M.M.; Bruce, J.N. Human pineal physiology and functional significance of melatonin. Front. Neuroendocrinol. 2004, 25, 177–195. [Google Scholar] [CrossRef] [PubMed]
- Gooley, J.J.; Chamberlain, K.; Smith, K.A.; Khalsa, S.B.S.; Rajaratnam, S.M.W.; Van Reen, E.; Zeitzer, J.M.; Czeisler, C.A.; Lockley, S.W. Exposure to room light before bedtime suppresses melatonin onset and shortens melatonin duration in humans. J. Clin. Endocrinol. Metab. 2011, 96, E463–E472. [Google Scholar] [CrossRef] [Green Version]
- Kayumov, L.; Casper, R.F.; Hawa, R.J.; Perelman, B.; Chung, S.A.; Sokalsky, S.; Shapiro, C.M. Blocking low-wavelength light prevents nocturnal melatonin suppression with no adverse effect on performance during simulated shift work. J. Clin. Endocrinol. Metab. 2005, 90, 2755–2761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagare, R.; Plitnick, B.; Figueiro, M.G. Effect of exposure duration and light spectra on nighttime melatonin suppression in adolescents and adults. Light. Res. Technol. 2019, 51, 530–543. [Google Scholar] [CrossRef]
- Wen, P.; Tan, F.; Wu, M.; Cai, Q.; Xu, R.; Zhang, X.; Wang, Y.; Khan, M.S.A.; Chen, W.; Hu, X. The effects of different bedroom light environments in the evening on adolescents. Build. Environ. 2021, 206, 108321. [Google Scholar] [CrossRef]
- Nie, J.; Zhou, T.; Chen, Z.; Dang, W.; Jiao, F.; Zhan, J.; Chen, Y.; Chen, Y.; Pan, Z.; Kang, X.; et al. The effects of dynamic daylight-like light on the rhythm, cognition, and mood of irregular shift workers in closed environment. Sci. Rep. 2021, 11, 13059. [Google Scholar] [CrossRef] [PubMed]
- Kozaki, T.; Hidaka, Y.; Takakura, J.; Kusano, Y. Salivary melatonin suppression under 100-Hz flickering blue light and non-flickering blue light conditions. Neurosci. Lett. 2020, 722, 134857. [Google Scholar] [CrossRef] [PubMed]
- Razavi, P.; Devore, E.E.; Bajaj, A.; Lockley, S.W.; Figueiro, M.G.; Ricchiuti, V.; Gauderman, W.J.; Hankinson, S.E.; Willett, W.C.; Schernhammer, E.S. Shift work, chronotype, and melatonin rhythm in nurses. Cancer Epidemiol. Biomark. Prev. 2019, 28, 1177–1186. [Google Scholar] [CrossRef] [PubMed]
- Hébert, M.; Martin, S.K.; Lee, C.; Eastman, C.I. The effects of prior light history on the suppression of melatonin by light in humans. J. Pineal Res. 2002, 33, 198–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kozaki, T.; Taketomi, R.; Hidaka, Y.; Ide, N.; Yasuda, T. Preventive effect of morning bluish LED light on light-induced melatonin suppression at night. J. Sci. Technol. Light. 2018, 41, 206–210. [Google Scholar] [CrossRef]
- Jung, C.M.; Khalsa, S.B.S.; Scheer, F.; Cajochen, C.; Lockley, S.W.; Czeisler, C.A.; Wright, K.P. Acute effects of bright light exposure on cortisol levels. J. Biol. Rhythm. 2010, 25, 208–216. [Google Scholar] [CrossRef]
- Driller, M.W.; Jacobson, G.; Uiga, L. Hunger hormone and sleep responses to the built-in blue-light filter on an electronic device: A pilot study. Sleep Sci. 2019, 12, 171–177. [Google Scholar] [CrossRef]
- Nguyen, J.; Wright, K.P., Jr. Influence of weeks of circadian misalignment on leptin levels. Nat. Sci. Sleep 2010, 2, 9–18. [Google Scholar]
- Papantoniou, K.; Pozo, O.J.; Espinosa, A.; Marcos, J.; Castano-Vinyals, G.; Basagana, X.; Juanola Pages, E.; Mirabent, J.; Martin, J.; Such Faro, P.; et al. Increased and mistimed sex hormone production in night shift workers. Cancer Epidemiol. Biomark. Prev. 2015, 24, 854–863. [Google Scholar] [CrossRef] [Green Version]
- Gómez-Acebo, I.; Dierssen-Sotos, T.; Papantoniou, K.; García-Unzueta, M.T.; Santos-Benito, M.F.; Llorca, J. Association between exposure to rotating night shift versus day shift using levels of 6-sulfatoxymelatonin and cortisol and other sex hormones in women. Chronobiol. Int. 2015, 32, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Davis, S.; Mirick, D.K.; Stevens, R.G. Night shift work, light at night, and risk of breast cancer. J. Natl. Cancer Inst. 2001, 93, 1557–1562. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.; Smith, M.; Eastman, C. A compromise phase position for permanent night shift workers: Circadian phase after two night shifts with scheduled sleep and light/dark exposure. Chronobiol. Int. 2006, 23, 859–875. [Google Scholar] [CrossRef]
- Smith, M.R.; Revell, V.L.; Eastman, C.I. Phase advancing the human circadian clock with blue-enriched polychromatic light. Sleep Med. 2009, 10, 287–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khodasevich, D.; Tsui, S.; Keung, D.; Skene, D.J.; Revell, V.; Martinez, M.E. Characterizing the modern light environment and its influence on circadian rhythms. Proc. Biol. Sci. 2021, 288, 20210721. [Google Scholar] [CrossRef] [PubMed]
- Yelden, K.; Duport, S.; Kempny, A.; Playford, E.D. A rehabilitation unit at night: Environmental characteristics of patient rooms. Disabil. Rehabil. 2015, 37, 91–96. [Google Scholar] [CrossRef]
- Green, A.; Cohen-Zion, M.; Haim, A.; Dagan, Y. Evening light exposure to computer screens disrupts human sleep, biological rhythms, and attention abilities. Chronobiol. Int. 2017, 34, 855–865. [Google Scholar] [CrossRef]
- Mantua, J.; Ritland, B.M.; Naylor, J.A.; Simonelli, G.; Mickelson, C.A.; Choynowski, J.J.; Bessey, A.F.; Sowden, W.J.; Burke, T.M.; McKeon, A.B. Physical sleeping environment is related to insomnia risk and measures of readiness in US army special operations soldiers. BMJ Mil. Health 2021. [Google Scholar] [CrossRef]
- Fossum, I.N.; Nordnes, L.T.; Storemark, S.S.; Bjorvatn, B.; Pallesen, S. The association between use of electronic media in bed before going to sleep and insomnia symptoms, daytime sleepiness, morningness, and chronotype. Behav. Sleep Med. 2014, 12, 343–357. [Google Scholar] [CrossRef]
- Rahman, S.A.; Marcu, S.; Kayumov, L.; Shapiro, C.M. Altered sleep architecture and higher incidence of subsyndromal depression in low endogenous melatonin secretors. Eur. Arch. Psychiatry Clin. Neurosci. 2010, 260, 327–335. [Google Scholar] [CrossRef] [PubMed]
- Rivkees, S.A.; Mayes, L.; Jacobs, H.; Gross, I. Rest-activity patterns of premature infants are regulated by cycled lighting. Pediatrics 2004, 113, 833–839. [Google Scholar] [CrossRef] [PubMed]
- Gringras, P.; Gamble, C.; Jones, A.P.; Wiggs, L.; Williamson, P.R.; Sutcliffe, A.; Montgomery, P.; Whitehouse, W.P.; Choonara, I.; Allport, T.; et al. Melatonin for sleep problems in children with neurodevelopmental disorders: Randomised double masked placebo-controlled trial. BMJ 2012, 345, e6664. [Google Scholar] [CrossRef] [Green Version]
- Paksarian, D.; Rudolph, K.E.; Stapp, E.K.; Dunster, G.P.; He, J.; Mennitt, D.; Hattar, S.; Casey, J.A.; James, P.; Merikangas, K.R. Association of outdoor artificial light at night with mental disorders and sleep patterns among US adolescents. JAMA Psychiatry 2020, 77, 1266–1275. [Google Scholar] [CrossRef]
- Crowley, S.J.; Cain, S.W.; Burns, A.C.; Acebo, C.; Carskadon, M.A. Increased sensitivity of the circadian system to light in early/mid-puberty. J. Clin. Endocrinol. Metab. 2015, 100, 4067–4073. [Google Scholar] [CrossRef] [PubMed]
- Baker, F.C.; Driver, H.S. Circadian rhythms, sleep, and the menstrual cycle. Sleep Med. 2007, 8, 613–622. [Google Scholar] [CrossRef] [PubMed]
- Hurley, S.; Goldberg, D.; Nelson, D.; Hertz, A.; Horn-Ross, P.L.; Bernstein, L.; Reynolds, P. Light at night and breast cancer risk among California teachers. Epidemiology 2014, 25, 697–706. [Google Scholar] [CrossRef]
- Sun, S.; Cao, W.; Ge, Y.; Ran, J.; Sun, F.; Zeng, Q.; Guo, M.; Huang, J.; Lee, R.S.; Tian, L.; et al. Outdoor light at night and risk of coronary heart disease among older adults: A prospective cohort study. Eur. Heart J. 2021, 42, 822–830. [Google Scholar] [CrossRef]
- Green, A.; Cohen-Zion, M.; Haim, A.; Dagan, Y. Comparing the response to acute and chronic exposure to short wavelength lighting emitted from computer screens. Chronobiol. Int. 2018, 35, 90–100. [Google Scholar] [CrossRef] [PubMed]
- Bartel, K.; Scheeren, R.; Gradisar, M. Altering adolescents’ pre-bedtime phone use to achieve better sleep health. Health Commun. 2019, 34, 456–462. [Google Scholar] [CrossRef] [PubMed]
- Grønli, J.; Byrkjedal, I.K.; Bjorvatn, B.; Nødtvedt, Ø.; Hamre, B.; Pallesen, S. Reading from an iPad or from a book in bed: The impact on human sleep. A randomized controlled crossover trial. Sleep Med. 2016, 21, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Higuchi, S.; Lin, Y.; Qiu, J.; Zhang, Y.; Ohashi, M.; Lee, S.-i.; Kitamura, S.; Yasukouchi, A. Is the use of high correlated color temperature light at night related to delay of sleep timing in university students? A cross-country study in Japan and China. J. Physiol. Anthropol. 2021, 40, 7. [Google Scholar] [CrossRef] [PubMed]
- Zhong, C.; Franklin, M.; Wiemels, J.; Chung, N.; Benbow, J.; Wang, S.; Lacey, J.; Longcore, T. Outdoor artificial light at night, sleep duration, and sleep quality in the California teachers study cohort. Sleep 2020, 43, A147. [Google Scholar] [CrossRef]
- Monma, T.; Ando, A.; Asanuma, T.; Yoshitake, Y.; Yoshida, G.; Miyazawa, T.; Ebine, N.; Takeda, S.; Omi, N.; Satoh, M.; et al. Sleep disorder risk factors among student athletes. Sleep Med. 2018, 44, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Francis, G.; Bishop, L.; Luke, C.; Middleton, B.; Williams, P.; Arendt, J. Sleep during the Antarctic winter: Preliminary observations on changing the spectral composition of artificial light. J. Sleep Res. 2008, 17, 354–360. [Google Scholar] [CrossRef]
- Janz, N.K.; Musch, D.C.; Gillespie, B.W.; Wren, P.A.; Niziol, L.M. Evaluating clinical change and visual function concerns in drivers and nondrivers with glaucoma. Invest. Ophthalmol. Vis. Sci. 2009, 50, 1718–1725. [Google Scholar] [CrossRef] [PubMed]
- Miranda-Ackerman, R.C.; Lira-Trujillo, M.; Gollaz-Cervantez, A.C.; Cortés-Flores, A.O.; Zuloaga-Fernández Del Valle, C.J.; García-González, L.A.; Morgan-Villela, G.; Barbosa-Camacho, F.J.; Pintor-Belmontes, K.J.; Guzmán-Ramírez, B.G.; et al. Associations between stressors and difficulty sleeping in critically ill patients admitted to the intensive care unit: A cohort study. BMC Health Serv. Res. 2020, 20, 631. [Google Scholar] [CrossRef]
- Jiang, Y.; Xia, Q.; Zhou, P.; Jiang, S.; Diwan, V.K.; Xu, B. Environmental hazards increase the fall risk among residents of long-term care facilities: A prospective study in Shanghai, China. Age Ageing 2021, 50, 875–881. [Google Scholar] [CrossRef]
- Sunde, E.; Pedersen, T.; Mrdalj, J.; Thun, E.; Gronli, J.; Harris, A.; Bjorvatn, B.; Waage, S.; Skene, D.J.; Pallesen, S. Alerting and circadian effects of short-wavelength vs. long-wavelength narrow-bandwidth light during a simulated night shift. Clocks Sleep 2020, 2, 502–522. [Google Scholar] [CrossRef]
- Lee, H.-S.; Lee, E.; Moon, J.-H.; Kim, Y.; Lee, H.-J. Circadian disruption and increase of oxidative stress in male and female volunteers after bright light exposure before bed time. Mol. Cell. Toxicol. 2019, 15, 221–229. [Google Scholar] [CrossRef]
- Grubisic, M.; Haim, A.; Bhusal, P.; Dominoni, D.M.; Gabriel, K.M.; Jechow, A.; Kupprat, F.; Lerner, A.; Marchant, P.; Riley, W. Light pollution, circadian photoreception, and melatonin in vertebrates. Sustainability 2019, 11, 6400. [Google Scholar] [CrossRef] [Green Version]
- O’Leary, E.S.; Schoenfeld, E.R.; Stevens, R.G.; Kabat, G.C.; Henderson, K.; Grimson, R.; Gammon, M.D.; Leske, M.C. Shift work, light at night, and breast cancer on Long Island, New York. Am. J. Epidemiol. 2006, 164, 358–366. [Google Scholar] [CrossRef] [Green Version]
- Stevens, R.G. Artificial lighting in the industrialized world: Circadian disruption and breast cancer. Cancer Causes Control 2006, 17, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Zheng, T.; Holford, T.R.; Boyle, P.; Zhang, Y.; Dai, M. Light at night and breast cancer risk: Results from a population-based case-control study in Connecticut, USA. Cancer Causes Control 2010, 21, 2281–2285. [Google Scholar] [CrossRef] [Green Version]
- White, A.J.; Weinberg, C.R.; Park, Y.-M.; D’Aloisio, A.A.; Vogtmann, E.; Nichols, H.B.; Sandler, D.P. Sleep characteristics, light at night and breast cancer risk in a prospective cohort. Int. J. Cancer 2017, 141, 2204–2214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ritonja, J.; McIsaac, M.A.; Sanders, E.; Kyba, C.C.M.; Grundy, A.; Cordina-Duverger, E.; Spinelli, J.J.; Aronson, K.J. Outdoor light at night at residences and breast cancer risk in Canada. Eur. J. Epidemiol. 2020, 35, 579–589. [Google Scholar] [CrossRef]
- Clarke, R.B.; Amini, H.; James, P.; von Euler-Chelpin, M.; Jørgensen, J.T.; Mehta, A.; Cole-Hunter, T.; Westendorp, R.; Mortensen, L.H.; Loft, S.; et al. Outdoor light at night and breast cancer incidence in the Danish nurse cohort. Environ. Res. 2021, 194, 110631. [Google Scholar] [CrossRef]
- Johns, L.E.; Jones, M.E.; Schoemaker, M.J.; McFadden, E.; Ashworth, A.; Swerdlow, A.J. Domestic light at night and breast cancer risk: A prospective analysis of 105 000 UK women in the generations sudy. Br. J. Cancer 2018, 118, 600–606. [Google Scholar] [CrossRef] [Green Version]
- Li, W.; Ray, R.M.; Thomas, D.B.; Davis, S.; Yost, M.; Breslow, N.; Gao, D.L.; Fitzgibbons, E.D.; Camp, J.E.; Wong, E.; et al. Shift work and breast cancer among women textile workers in Shanghai, China. Cancer Causes Control 2015, 26, 143–150. [Google Scholar] [CrossRef] [Green Version]
- Papantoniou, K.; Castano-Vinyals, G.; Espinosa, A.; Aragones, N.; Perez-Gomez, B.; Burgos, J.; Gomez-Acebo, I.; Llorca, J.; Peiro, R.; Jimenez-Moleon, J.J.; et al. Night shift work, chronotype and prostate cancer risk in the MCC-Spain case-control study. Int. J. Cancer 2015, 137, 1147–1157. [Google Scholar] [CrossRef]
- Kim, K.Y.; Lee, E.; Kim, Y.J.; Kim, J. The association between artificial light at night and prostate cancer in Gwangju city and South Jeolla Province of South Korea. Chronobiol. Int. 2017, 34, 203–211. [Google Scholar] [CrossRef]
- Garcia-Saenz, A.; de Miguel, A.S.; Espinosa, A.; Valentin, A.; Aragones, N.; Llorca, J.; Amiano, P.; Sanchez, V.M.; Guevara, M.; Capelo, R.; et al. Evaluating the association between artificial light-at-night exposure and breast and prostate cancer risk in Spain (MCC-Spain study). Environ. Health Perspect. 2018, 126, 047011. [Google Scholar] [CrossRef]
- Schernhammer, E.S.; Razavi, P.; Li, T.Y.; Qureshi, A.A.; Han, J. Rotating night shifts and risk of skin cancer in the nurses’ health study. J. Natl. Cancer Inst. 2011, 103, 602–606. [Google Scholar] [CrossRef] [Green Version]
- Heckman, C.J.; Kloss, J.D.; Feskanich, D.; Culnan, E.; Schernhammer, E.S. Associations among rotating night shift work, sleep and skin cancer in Nurses’ Health Study II participants. Occup. Environ. Med. 2017, 74, 169–175. [Google Scholar] [CrossRef] [Green Version]
- Kloog, I.; Stevens, R.G.; Haim, A.; Portnov, B.A. Nighttime light level co-distributes with breast cancer incidence worldwide. Cancer Causes Control 2010, 21, 2059–2068. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J.; Lee, E.; Lee, H.S.; Kim, M.; Park, M.S. High prevalence of breast cancer in light polluted areas in urban and rural regions of South Korea: An ecologic study on the treatment prevalence of female cancers based on National Health Insurance data. Chronobiol. Int. 2015, 32, 657–667. [Google Scholar] [CrossRef] [PubMed]
- Koo, Y.S.; Song, J.-Y.; Joo, E.-Y.; Lee, H.-J.; Lee, E.; Lee, S.-k.; Jung, K.-Y. Outdoor artificial light at night, obesity, and sleep health: Cross-sectional analysis in the KoGES study. Chronobiol. Int. 2016, 33, 301–314. [Google Scholar] [CrossRef]
- Rybnikova, N.A.; Haim, A.; Portnov, B.A. Does artificial light-at-night exposure contribute to the worldwide obesity pandemic? Int. J. Obes. 2016, 40, 815–823. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.X.; Zhang, A.H.; Yu, Y.; Wan, Y.H.; Tao, F.B.; Sun, Y. Sex-specific association of exposure to bedroom light at night with general and abdominal adiposity in young adults. Ecotoxicol. Environ. Saf. 2021, 223, 112561. [Google Scholar] [CrossRef]
- Park, Y.-M.M.; White, A.J.; Jackson, C.L.; Weinberg, C.R.; Sandler, D.P. Association of exposure to artificial light at night while sleeping with risk of obesity in women. JAMA Intern. Med. 2019, 179, 1061–1071. [Google Scholar] [CrossRef]
- Zhang, D.; Jones, R.R.; Powell-Wiley, T.M.; Jia, P.; James, P.; Xiao, Q. A large prospective investigation of outdoor light at night and obesity in the NIH-AARP diet and health study. Environ. Health 2020, 19, 74. [Google Scholar] [CrossRef]
- McHill, A.W.; Melanson, E.L.; Higgins, J.; Connick, E.; Moehlman, T.M.; Stothard, E.R.; Wright, K.P., Jr. Impact of circadian misalignment on energy metabolism during simulated nightshift work. Proc. Natl. Acad. Sci. USA 2014, 111, 17302–17307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knutson, K.L.; Wu, D.; Patel, S.R.; Loredo, J.S.; Redline, S.; Cai, J.; Gallo, L.C.; Mossavar-Rahmani, Y.; Ramos, A.R.; Teng, Y.; et al. Association between sleep timing, obesity, diabetes: The hispanic community health study/study of Latinos (HCHS/SOL) cohort study. Sleep 2017, 40, zsx014. [Google Scholar] [CrossRef] [Green Version]
- Butler, M.P.; Smales, C.; Wu, H.; Hussain, M.V.; Mohamed, Y.A.; Morimoto, M.; Shea, S.A. The circadian system contributes to apnea lengthening across the night in obstructive sleep apnea. Sleep 2015, 38, 1793–1801. [Google Scholar] [CrossRef] [Green Version]
- Obayashi, K.; Saeki, K.; Iwamoto, J.; Ikada, Y.; Kurumatani, N. Association between light exposure at night and nighttime blood pressure in the elderly independent of nocturnal urinary melatonin excretion. Chronobiol. Int. 2014, 31, 779–786. [Google Scholar] [CrossRef]
- Obayashi, K.; Saeki, K.; Kurumatani, N. Light exposure at night is associated with subclinical carotid atherosclerosis in the general elderly population: The HEIJO-KYO cohort. Chronobiol. Int. 2015, 32, 310–317. [Google Scholar] [CrossRef]
- Lopez-Gil, N.; Peixoto-De-Matos, S.C.; Thibos, L.N.; Gonzalez-Meijome, J.M. Shedding light on night myopia. J. Vis. 2012, 12, 4. [Google Scholar] [CrossRef]
- Ahn, J.; Ahn, S.-E.; Yang, K.-S.; Kim, S.-W.; Oh, J. Effects of a high level of illumination before sleep at night on chorioretinal thickness and ocular biometry. Exp. Eye Res. 2017, 164, 157–167. [Google Scholar] [CrossRef]
- Li, X.; Xu, X.; Song, Y.; Cui, S.; Xue, C.; Wang, L.; Wu, J.; Yuan, J. An association between cumulative exposure to light at night and the prevalence of hyperuricemia in steel workers. Int. J. Occup. Med. Environ. Health 2021, 34, 385–401. [Google Scholar] [CrossRef]
- Zhang, S.K.; Wang, Y.B.; Zhu, Y.; Li, X.M.; Song, Y.; Yuan, J.X. Rotating night shift work, exposure to light at night, and glomerular filtration rate: Baseline results from a Chinese occupational cohort. Int. J. Environ. Res. Public Health 2020, 17, 9035. [Google Scholar] [CrossRef]
- Burgess, H.J.; Park, M.; Ong, J.C.; Shakoor, N.; Williams, D.A.; Burns, J. Morning versus evening bright light treatment at home to improve function and pain sensitivity for women with fibromyalgia: A pilot study. Pain Med. 2017, 18, 116–123. [Google Scholar] [CrossRef] [Green Version]
- Green, A.; Barak, S.; Shine, L.; Kahane, A.; Dagan, Y. Exposure by males to light emitted from media devices at night is linked with decline of sperm quality and correlated with sleep quality measures. Chronobiol. Int. 2020, 37, 414–424. [Google Scholar] [CrossRef] [Green Version]
- Feskanich, D.; Hankinson, S.E.; Schernhammer, E.S. Nightshift work and fracture risk: The nurses’ health study. Osteoporos. Int. 2009, 20, 537–542. [Google Scholar] [CrossRef] [Green Version]
- Meng, Y.; Zhu, V.; Zhu, Y. Co-distribution of light at night (LAN) and COVID-19 incidence in the United States. BMC Public Health 2021, 21, 1509. [Google Scholar] [CrossRef]
- Cheng, P.; Tallent, G.; Bender, T.J.; Tran, K.M.; Drake, C.L. Shift work and cognitive flexibility: Decomposing task performance. J. Biol. Rhythm. 2017, 32, 143–153. [Google Scholar] [CrossRef] [Green Version]
- Manousakis, J.E.; Scovelle, A.J.; Rajaratnam, S.M.W.; Naismith, S.L.; Anderson, C. Advanced circadian timing and sleep fragmentation differentially impact on memory complaint subtype in subjective cognitive decline. J. Alzheimers Dis. 2018, 66, 565–577. [Google Scholar] [CrossRef]
- Namita; Ranjan, D.P.; Shenvi, D.N. Effect of shift working on reaction time in hospital employees. Indian J. Physiol. Pharmacol 2010, 54, 289–293. [Google Scholar]
- Ganesan, S.; Magee, M.; Stone, J.E.; Mulhall, M.D.; Collins, A.; Howard, M.E.; Lockley, S.W.; Rajaratnam, S.M.W.; Sletten, T.L. The impact of shift work on sleep, alertness and performance in healthcare workers. Sci. Rep. 2019, 9, 4635. [Google Scholar] [CrossRef] [Green Version]
- McHill, A.W.; Wright, K.P., Jr. Cognitive impairments during the transition to working at night and on subsequent night shifts. J. Biol. Rhythm. 2019, 34, 432–446. [Google Scholar] [CrossRef]
- Chang, A.-M.; Aeschbach, D.; Duffy, J.F.; Czeisler, C.A. Evening use of light-emitting eReaders negatively affects sleep, circadian timing, and next-morning alertness. Proc. Natl. Acad. Sci. USA 2015, 112, 1232–1237. [Google Scholar] [CrossRef] [Green Version]
- Green, A.; Dagan, Y.; Haim, A. Exposure to screens of digital media devices, sleep, and concentration abilities in a sample of Israel adults. Sleep Biol. Rhythm. 2018, 16, 273–281. [Google Scholar] [CrossRef]
- Anderson, C.; Sullivan, J.P.; Flynn-Evans, E.E.; Cade, B.E.; Czeisler, C.A.; Lockley, S.W. Deterioration of neurobehavioral performance in resident physicians during repeated exposure to extended duration work shifts. Sleep 2012, 35, 1137–1146. [Google Scholar] [CrossRef] [Green Version]
- Scullin, M.K.; Hebl, M.R.; Corrington, A.; Nguyen, S. Experimental sleep loss, racial bias, and the decision criterion to shoot in the Police Officer’s Dilemma task. Sci. Rep. 2020, 10, 20581. [Google Scholar] [CrossRef]
- Gazenkampf, K.A.; Omelenchuk, R.K.; Emelyanova, V.N.; Shnayder, N.A.; Alekseeva, A.N.; Alekseeva, O.V.; Kazantsev, A.D.; Fadeeva, E.P.; Dmitrenko, D.V. Circadian sleep disorders in schoolchildren of countryside Siberia. Rus. Zhunal Det. Nevrol. 2017, 12, 40–42. [Google Scholar] [CrossRef] [Green Version]
- Obayashi, K.; Saeki, K.; Kurumatani, N. Association between light exposure at night and insomnia in the general elderly population: The HEIJO-KYO cohort. Chronobiol. Int. 2014, 31, 976–982. [Google Scholar] [CrossRef]
- Herrmann, W.J.; Flick, U. External barriers to good sleep from the nursing home residents’ perspective. Pflege Z. 2012, 65, 744–748. [Google Scholar]
- Min, J.-y.; Min, K.-b. Outdoor light at night and the prevalence of depressive symptoms and suicidal behaviors: A cross-sectional study in a nationally representative sample of Korean adults. J. Affect. Disord. 2018, 227, 199–205. [Google Scholar] [CrossRef]
- Obayashi, K.; Saeki, K.; Kurumatani, N. Bedroom light exposure at night and the incidence of depressive symptoms: A longitudinal study of the HEIJO-KYO cohort. Am. J. Epidemiol. 2018, 187, 427–434. [Google Scholar] [CrossRef]
- Esaki, Y.; Kitajima, T.; Obayashi, K.; Saeki, K.; Fujita, K.; Iwata, N. Light exposure at night and sleep quality in bipolar disorder: The APPLE cohort study. J. Affect. Disord. 2019, 257, 314–320. [Google Scholar] [CrossRef]
- Gumenyuk, V.; Howard, R.; Roth, T.; Korzyukov, O.; Drake, C.L. Sleep loss, circadian mismatch, and abnormalities in reorienting of attention in night workers with shift work disorder. Sleep 2014, 37, 545–556. [Google Scholar] [CrossRef] [Green Version]
- Olson, J.A.; Artenie, D.Z.; Cyr, M.; Raz, A.; Lee, V. Developing a light-based intervention to reduce fatigue and improve sleep in rapidly rotating shift workers. Chronobiol. Int. 2020, 37, 573–591. [Google Scholar] [CrossRef]
- Sunde, E.; Mrdalj, J.; Pedersen, T.; Thun, E.; Bjorvatn, B.; Grønli, J.; Harris, A.; Waage, S.; Pallesen, S. Role of nocturnal light intensity on adaptation to three consecutive night shifts: A counterbalanced crossover study. Occup. Environ. Med. 2020, 77, 249–255. [Google Scholar] [CrossRef]
- Bjorvatn, B.; Waage, S. Bright light improves sleep and psychological health in shift working nurses. J. Clin. Sleep Med. 2013, 9, 647–648. [Google Scholar] [CrossRef] [Green Version]
- Moscovici, L.; Kotler, M. A multistage chronobiologic intervention for the treatment of depression: A pilot study. J. Affect. Disord. 2009, 116, 201–207. [Google Scholar] [CrossRef]
- Kaplan, K.A.; Mashash, M.; Williams, R.; Batchelder, H.; Starr-Glass, L.; Zeitzer, J.M. Effect of light flashes vs sham therapy during sleep with adjunct cognitive behavioral therapy on sleep quality among adolescents: A randomized clinical trial. JAMA Netw. Open 2019, 2, e1911944. [Google Scholar] [CrossRef] [Green Version]
- Suhner, A.G.; Murphy, P.J.; Campbell, S.S. Failure of timed bright light exposure to alleviate age-related sleep maintenance insomnia. J. Am. Geriatr. Soc. 2002, 50, 617–623. [Google Scholar] [CrossRef]
- Figueiro, M.G.; Plitnick, B.A.; Lok, A.; Jones, G.E.; Higgins, P.; Hornick, T.R.; Rea, M.S. Tailored lighting intervention improves measures of sleep, depression, and agitation in persons with Alzheimer’s disease and related dementia living in long-term care facilities. Clin. Interv. Aging 2014, 9, 1527–1537. [Google Scholar] [CrossRef] [Green Version]
- Henriksen, T.E.; Skrede, S.; Fasmer, O.B.; Schoeyen, H.; Leskauskaite, I.; Bjørke-Bertheussen, J.; Assmus, J.; Hamre, B.; Grønli, J.; Lund, A. Blue-blocking glasses as additive treatment for mania: A randomized placebo-controlled trial. Bipolar Disord. 2016, 18, 221–232. [Google Scholar] [CrossRef] [Green Version]
- Tao, L.; Jiang, R.; Zhang, K.; Qian, Z.; Chen, P.; Lv, Y.; Yao, Y. Light therapy in non-seasonal depression: An update meta-analysis. Psychiatry Res. 2020, 291, 113247. [Google Scholar] [CrossRef]
- Brown, T.M.; Brainard, G.C.; Cajochen, C.; Czeisler, C.A.; Hanifin, J.P.; Lockley, S.W.; Lucas, R.J.; Münch, M.; O’Hagan, J.B.; Peirson, S.N. Recommendations for daytime, evening, and nighttime indoor light exposure to best support physiology, sleep, and wakefulness in healthy adults. PLoS Biol. 2022, 20, e3001571. [Google Scholar] [CrossRef]
- Moore-Ede, M.; Heitmann, A.; Guttkuhn, R. Circadian potency spectrum with extended exposure to polychromatic white LED light under workplace conditions. J. Biol. Rhythm. 2020, 35, 405–415. [Google Scholar] [CrossRef]
- Sadeghniiat-Haghighi, K.; Yazdi, Z.; Jahanihashemi, H.; Aminian, O. The effect of bright light on sleepiness among rapid-rotating 12-hour shift workers. Scand. J. Work Environ. Health 2011, 37, 77–79. [Google Scholar] [CrossRef] [Green Version]
- Karchani, M.; Kakooei, H.; Yazdi, Z.; Zare, M. Do bright-light shock exposures during breaks reduce subjective sleepiness in night workers? Sleep Biol. Rhythm. 2011, 9, 95–102. [Google Scholar] [CrossRef]
- Harrison, E.M.; Schmied, E.A.; Easterling, A.P.; Yablonsky, A.M.; Glickman, G.L. A hybrid effectiveness-implementation study of a multi-component lighting intervention for hospital shift workers. Int. J. Environ. Res. Public Health 2020, 17, 9141. [Google Scholar] [CrossRef]
- Postnova, S.; Robinson, P.A.; Postnov, D.D. Adaptation to shift work: Physiologically based modeling of the effects of lighting and shifts’ start time. PLoS ONE 2013, 8, e53379. [Google Scholar] [CrossRef] [Green Version]
- Figueiro, M.G.; Plitnick, B.; Rea, M.S.; Gras, L.Z.; Rea, M.S. Lighting and perceptual cues: Effects on gait measures of older adults at high and low risk for falls. BMC Geriatr. 2011, 11, 49. [Google Scholar] [CrossRef] [Green Version]
- Wood, J.M.; Isoardi, G.; Black, A.; Cowling, I. Night-time driving visibility associated with LED streetlight dimming. Accid. Anal. Prev. 2018, 121, 295–300. [Google Scholar] [CrossRef]
- Abegaz, T.; Berhane, Y.; Worku, A.; Assrat, A.; Assefa, A. Effects of excessive speeding and falling asleep while driving on crash injury severity in Ethiopia: A generalized ordered logit model analysis. Accid. Anal. Prev. 2014, 71, 15–21. [Google Scholar] [CrossRef]
- Chang, F.; Li, M.; Xu, P.; Zhou, H.; Haque, M.M.; Huang, H. Injury severity of motorcycle riders involved in traffic crashes in Hunan, China: A mixed ordered logit approach. Int. J. Environ. Res. Public Health 2016, 13, 714. [Google Scholar] [CrossRef]
- Plainis, S.; Murray, I.J.; Pallikaris, I.G. Road traffic casualties: Understanding the night-time death toll. Inj. Prev. 2006, 12, 125–128. [Google Scholar] [CrossRef] [Green Version]
- Marchant, P.; Hale, J.D.; Sadler, J.P. Does changing to brighter road lighting improve road safety? Multilevel longitudinal analysis of road traffic collision frequency during the relighting of a UK city. J. Epidemiol. Community Health 2020, 74, 467–472. [Google Scholar] [CrossRef] [Green Version]
- Claudio, L. Switch on the night: Policies for smarter lighting. Environ. Health Perspect. 2009, 117, A28–A31. [Google Scholar] [CrossRef] [Green Version]
- Kimlin, J.A.; Black, A.A.; Wood, J.M. Nighttime driving in older adults: Effects of glare and association with mesopic visual function. Invest. Ophthalmol. Vis. Sci. 2017, 58, 2796–2803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lorenc, T.; Petticrew, M.; Whitehead, M.; Neary, D.; Clayton, S.; Wright, K.; Thomson, H.; Cummins, S.; Sowden, A.; Renton, A. Fear of crime and the environment: Systematic review of UK qualitative evidence. BMC Public Health 2013, 13, 496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Innes, M.; Jones, V. Neighbourhood Security and Urban Change: Risk, Resilience and Recovery; Joseph Rowntree Foundation: York, UK, 2006. [Google Scholar]
- Lee, C.; Lee, C.; Stewart, O.T.; Carlos, H.A.; Adachi-Mejia, A.; Berke, E.M.; Doescher, M.P. Neighborhood environments and utilitarian walking among older vs. younger rural adults. Front. Public Health 2021, 9, 634751. [Google Scholar] [CrossRef] [PubMed]
- Evenson, K.R.; Scott, M.M.; Cohen, D.A.; Voorhees, C.C. Girls’ perception of neighborhood factors on. physical activity, sedentary behavior, and BMI. Obesity 2007, 15, 430–445. [Google Scholar] [CrossRef] [PubMed]
- Uddin, R.; Burton, N.W.; Khan, A. Perceived environmental barriers to physical activity in young adults in Dhaka City, Bangladesh-does gender matter? Int. Health 2018, 10, 40–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Welsh, B.C.; Farrington, D.P. Effects of improved street lighting on crime. Campbell Syst. Rev. 2008, 4, 1–51. [Google Scholar] [CrossRef]
- Green, J.; Perkins, C.; Steinbach, R.; Edwards, P. Reduced street lighting at night and health: A rapid appraisal of public views in England and Wales. Health Place 2015, 34, 171–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larkin, A.; van Donkelaar, A.; Geddes, J.A.; Martin, R.V.; Hystad, P. Relationships between changes in urban characteristics and air quality in East Asia from 2000 to 2010. Environ. Sci. Technol. 2016, 50, 9142–9149. [Google Scholar] [CrossRef] [Green Version]
- Huss, A.; van Wel, L.; Bogaards, L.; Vrijkotte, T.; Wolf, L.; Hoek, G.; Vermeulen, R. Shedding some light in the dark—A comparison of personal measurements with satellite-based estimates of exposure to light at night among children in the Netherlands. Env. Health Perspect. 2019, 127, 67001. [Google Scholar] [CrossRef] [Green Version]
- Wong, K.W.; Stutz, J. Influence of nocturnal vertical stability on daytime chemistry: A one-dimensional model study. Atmos. Environ. 2010, 44, 3753–3760. [Google Scholar] [CrossRef]
- Stark, H.; Brown, S.S.; Wong, K.W.; Stutz, J.; Elvidge, C.D.; Pollack, I.B.; Ryerson, T.B.; Dube, W.P.; Wagner, N.L.; Parrish, D.D. City lights and urban air. Nat. Geosci. 2011, 4, 730–731. [Google Scholar] [CrossRef]
- Brown, S.; Ryerson, T.; Wollny, A.; Brock, C.; Peltier, R.; Sullivan, A.; Weber, R.; Dube, W.; Trainer, M.; Meagher, J.F. Variability in nocturnal nitrogen oxide processing and its role in regional air quality. Science 2006, 311, 67–70. [Google Scholar] [CrossRef]
- Bedi, T.K.; Puntambekar, K.; Singh, S. Light pollution in India: Appraisal of artificial night sky brightness of cities. Environ. Dev. Sustain. 2021, 23, 18582–18597. [Google Scholar] [CrossRef]
- Sun, Y.; Wang, S.; Wang, Y. Estimating local-scale urban heat island intensity using nighttime light satellite imageries. Sustain. Cities Soc. 2020, 57, 102125. [Google Scholar] [CrossRef]
- Rund, S.S.C.; Labb, L.F.; Benefiel, O.M.; Duffield, G.E. Artificial light at night increases Aedes aegypti mosquito biting behavior with implications for arboviral disease transmission. Am. J. Trop. Med. Hyg. 2020, 103, 2450–2452. [Google Scholar] [CrossRef] [PubMed]
- Duffield, G.E.; Acri, D.J.; George, G.F.; Sheppard, A.D.; Beebe, N.W.; Ritchie, S.A.; Burkot, T.R. Diel flight activity of wild-caught Anopheles farauti (s.s.) and An. hinesorum malaria mosquitoes from northern Queensland, Australia. Parasites Vectors 2019, 12, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osório, H.C.; Zé-Zé, L.; Amaro, F.; Alves, M.J. Mosquito surveillance for prevention and control of emerging mosquito-borne diseases in Portugal—2008–2014. Int. J. Environ. Res. Public Health 2014, 11, 11583–11596. [Google Scholar] [CrossRef] [Green Version]
- Sheppard, A.D.; Rund, S.S.C.; George, G.F.; Clark, E.; Acri, D.J.; Duffield, G.E. Light manipulation of mosquito behaviour: Acute and sustained photic suppression of biting activity in the Anopheles gambiae malaria mosquito. Parasites Vectors 2017, 10, 255. [Google Scholar] [CrossRef] [PubMed]
- Fyie, L.R.; Gardiner, M.M.; Meuti, M.E. Artificial light at night alters the seasonal responses of biting mosquitoes. J. Insect Physiol. 2021, 129, 104194. [Google Scholar] [CrossRef]
- Aklilu, E.; Gebresilassie, A.; Yared, S.; Kindu, M.; Tekie, H.; Balkew, M.; Warburg, A.; Hailu, A.; Gebre-Michael, T. Comparative study on the nocturnal activity of phlebotomine sand flies in a highland and lowland foci of visceral leishmaniasis in north-western Ethiopia with special reference to Phlebotomus orientalis. Parasites Vectors 2017, 10, 393. [Google Scholar] [CrossRef]
- Escobar, L.E.; Peterson, A.T.; Papeş, M.; Favi, M.; Yung, V.; Restif, O.; Qiao, H.; Medina-Vogel, G. Ecological approaches in veterinary epidemiology: Mapping the risk of bat-borne rabies using vegetation indices and night-time light satellite imagery. Vet. Res. 2015, 46, 92. [Google Scholar] [CrossRef] [Green Version]
- Song, Y.; McCurry, S.M.; Lee, D.; Josephson, K.R.; McGowan, S.K.; Fung, C.H.; Irwin, M.R.; Teng, E.; Alessi, C.A.; Martin, J.L. Development of a dyadic sleep intervention for Alzheimer’s disease patients and their caregivers. Disabil. Rehabil. 2021, 43, 1861–1871. [Google Scholar] [CrossRef] [PubMed]
- Esaki, Y.; Obayashi, K.; Saeki, K.; Fujita, K.; Iwata, N.; Kitajima, T. Bedroom light exposure at night and obesity in individuals with bipolar disorder: A cross-sectional analysis of the APPLE cohort. Physiol. Behav. 2021, 230, 113281. [Google Scholar] [CrossRef] [PubMed]
- Harrison, E.M.; Yablonsky, A.M.; Powell, A.L.; Ancoli-Israel, S.; Glickman, G.L. Reported light in the sleep environment: Enhancement of the sleep diary. Nat. Sci. Sleep 2019, 11, 11. [Google Scholar] [CrossRef] [Green Version]
- Siraji, M.A.; Lazar, R.R.; van Duijnhoven, J.; Schlangen, L.J.; Haque, S.; Kalavally, V.; Vetter, C.; Glickman, G.; Smolders, K.C.; Spitschan, M. Light exposure behaviour assessment (LEBA): A novel self-reported instrument to capture light exposure-related behaviour. In Proceedings of the CIE Australia Lighting Research Conference, Online, 8 February 2022; p. 1. [Google Scholar]
- Katz, Y.; Levin, N. Quantifying urban light pollution—A comparison between field measurements and EROS-B imagery. Remote Sens. Environ. 2016, 177, 65–77. [Google Scholar] [CrossRef]
- Levin, N.; Kyba, C.C.; Zhang, Q.; de Miguel, A.S.; Román, M.O.; Li, X.; Portnov, B.A.; Molthan, A.L.; Jechow, A.; Miller, S.D. Remote sensing of night lights: A review and an outlook for the future. Remote Sens. Environ. 2020, 237, 111443. [Google Scholar] [CrossRef]
- Kyba, C.C. Defense meteorological satellite program data should no longer be used for epidemiological studies. Chronobiol. Int. 2016, 33, 943–945. [Google Scholar] [CrossRef] [Green Version]
- McIsaac, M.A.; Sanders, E.; Kuester, T.; Aronson, K.J.; Kyba, C.C. The impact of image resolution on power, bias, and confounding: A simulation study of ambient light at night exposure. Environ. Epidemiol. 2021, 5, e145. [Google Scholar] [CrossRef]
- Kwan, M.-P. The uncertain geographic context problem. Ann. Assoc. Am. Geogr. 2012, 102, 958–968. [Google Scholar] [CrossRef]
- Kwan, M.-P. The neighborhood effect averaging problem (NEAP): An elusive confounder of the neighborhood effect. Int. J. Environ. Res. Public Health 2018, 15, 1841. [Google Scholar] [CrossRef] [Green Version]
- Stone, J.E.; McGlashan, E.M.; Facer-Childs, E.R.; Cain, S.W.; Phillips, A.J. Accuracy of the GENEActiv device for measuring light exposure in sleep and circadian research. Clocks Sleep 2020, 2, 143–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.; Kou, L.; Kwan, M.-P.; Shakespeare, R.M.; Lee, K.; Park, Y.M. An integrated individual environmental exposure assessment system for real-time mobile sensing in environmental health studies. Sensors 2021, 21, 4039. [Google Scholar] [CrossRef] [PubMed]
- Buman, M.P.; Phillips, B.A.; Youngstedt, S.D.; Kline, C.E.; Hirshkowitz, M. Does nighttime exercise really disturb sleep? Results from the 2013 National Sleep Foundation Sleep in America Poll. Sleep Med. 2014, 15, 755–761. [Google Scholar] [CrossRef]
- Stanhope, J.; Liddicoat, C.; Weinstein, P. Outdoor artificial light at night: A forgotten factor in green space and health research. Environ. Res. 2021, 197, 111012. [Google Scholar] [CrossRef] [PubMed]
- Ta, N.; Kwan, M.-P.; Lin, S.; Zhu, Q. The activity space-based segregation of migrants in suburban Shanghai. Appl. Geogr. 2021, 133, 102499. [Google Scholar] [CrossRef]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, Y.; Yu, C.; Wang, K.; Kwan, M.-P.; Tse, L.A. Linking Artificial Light at Night with Human Health via a Multi-Component Framework: A Systematic Evidence Map. Environments 2023, 10, 39. https://doi.org/10.3390/environments10030039
Liu Y, Yu C, Wang K, Kwan M-P, Tse LA. Linking Artificial Light at Night with Human Health via a Multi-Component Framework: A Systematic Evidence Map. Environments. 2023; 10(3):39. https://doi.org/10.3390/environments10030039
Chicago/Turabian StyleLiu, Yang, Changda Yu, Keli Wang, Mei-Po Kwan, and Lap Ah Tse. 2023. "Linking Artificial Light at Night with Human Health via a Multi-Component Framework: A Systematic Evidence Map" Environments 10, no. 3: 39. https://doi.org/10.3390/environments10030039