
Effectiveness of the 5A Counseling Model-Based Interventions on Physical Activity Indicators in Adults: A Systematic Review
 , , and
, , and
Abstract
:1. Introduction
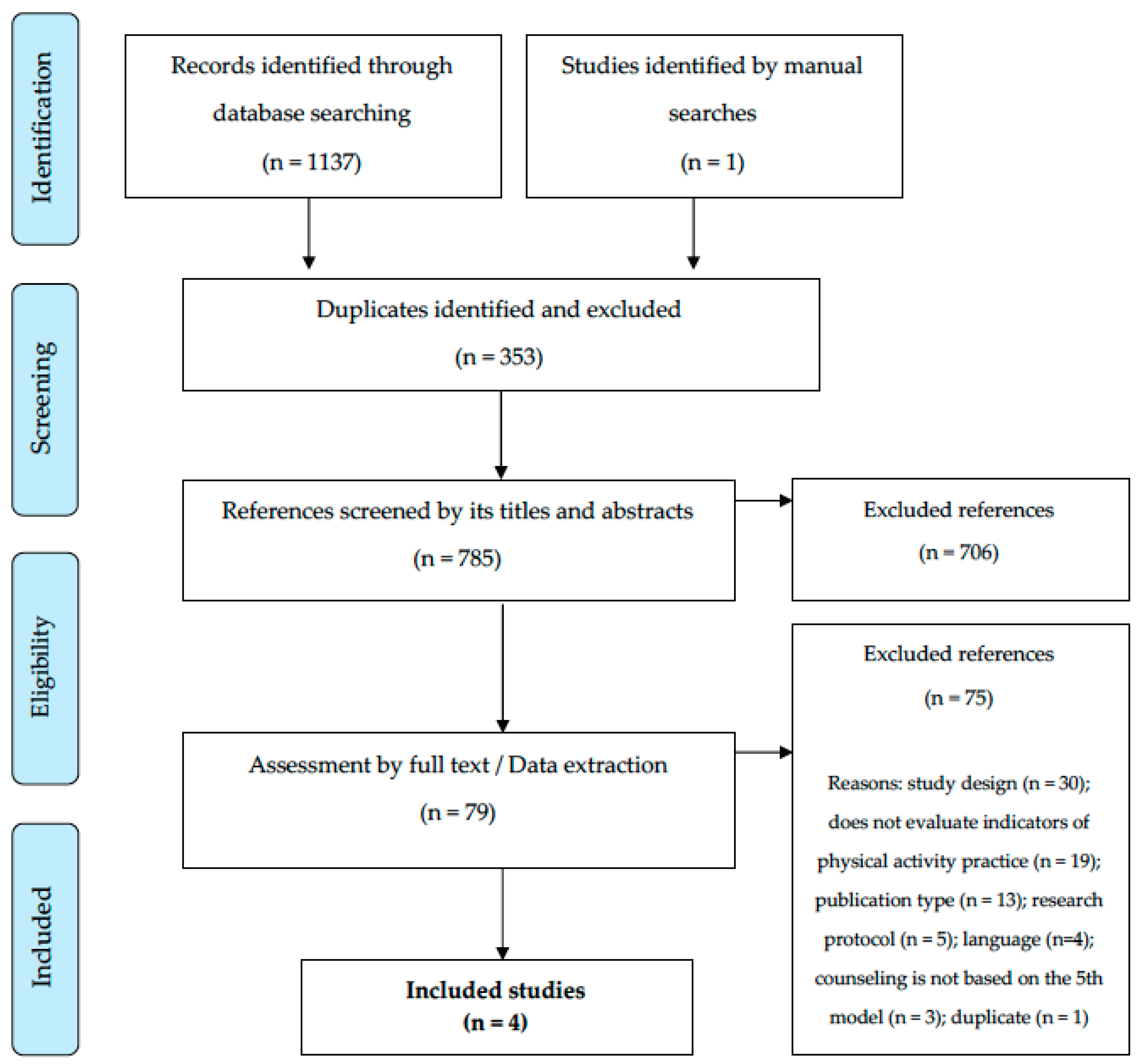
2. Materials and Methods
- “Population”: adults, between 18 and 59 years of age, without impeding conditions for the practice of physical activity;
- “Interventions”: the provision of 5A model counselling-based interventions about physical activity, regardless of the duration, the professional nucleus that implemented it and the support of other strategies (e.g., preparation of materials, offer of practical activities);
- “Comparators”: who preferably did not receive care, or who received standard care, without offering physical activity counseling based on the 5A model;
- “Outcome”: physical activity indicators (e.g., increase in the amount of physical activity, number of steps per day/week, proportion of people meeting the recommendation, self-efficacy for physical activity, etc.), preferably the total, or in leisure time or as a form of transport;
- “Study design”: intervention studies without restrictions regarding the presence of a control group and randomized allocation between groups.
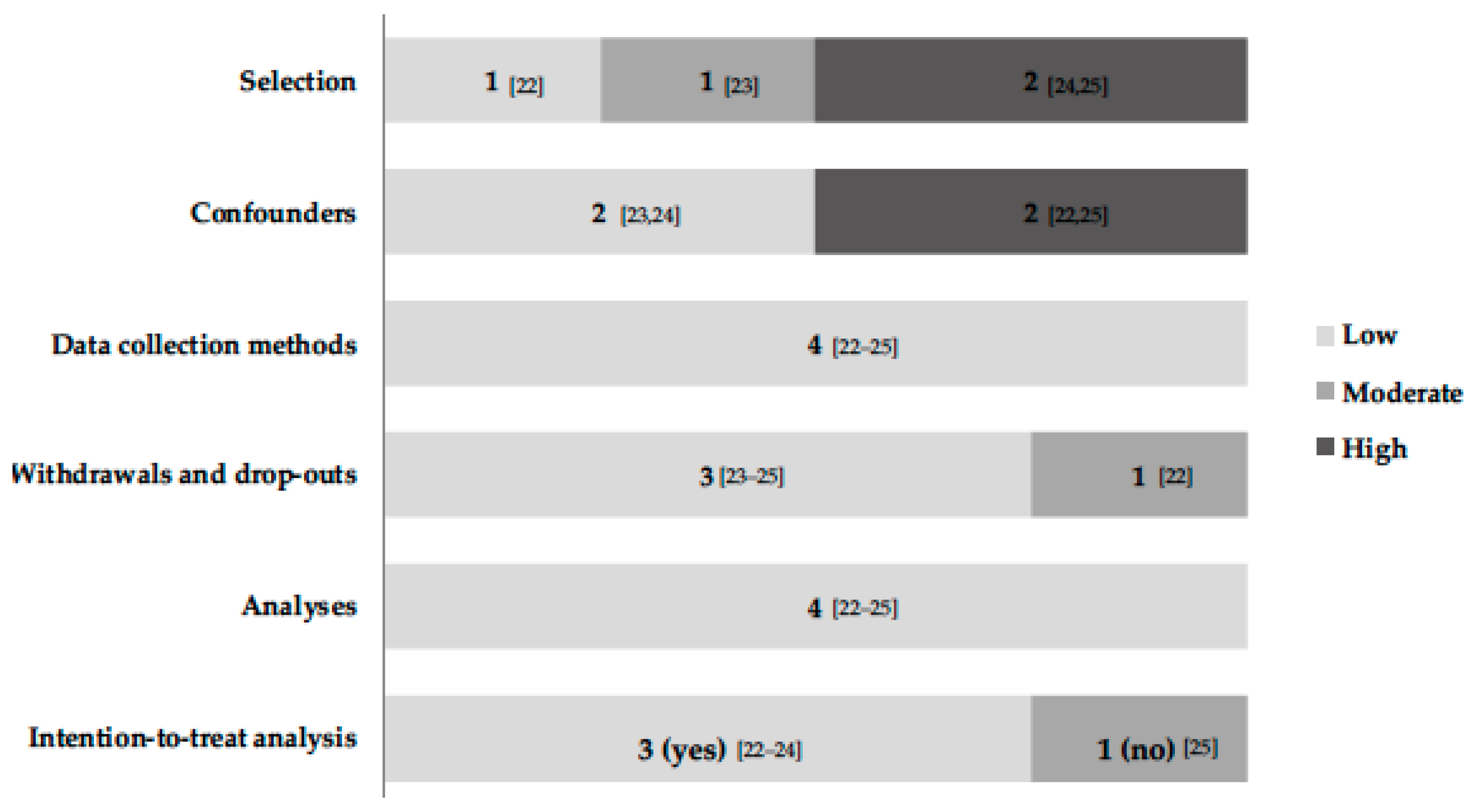
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- DiPietro, L.; Al-Ansari, S.S.; Biddle, S.J.H.; Borodulin, K.; Bull, F.C.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; et al. Advancing the global physical activity agenda: Recommendations for future research by the 2020 WHO physical activity and sedentary behavior guidelines development group. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 143. [Google Scholar] [CrossRef] [PubMed]
- Vagetti, G.C.; Barbosa Filho, V.C.; Moreira, N.B.; Oliveira, V.; Mazzardo, O.; Campos, W. Association between physical activity and quality of life in the elderly: A systematic review, 2000–2012. Braz. J. Psychiatry 2014, 36, 76–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hyde, A.L.; Maher, J.P.; Elavsky, S. Enhancing our understanding of physical activity and wellbeing with a lifespan perspective. Int. J. Wellbeing 2013, 3, 98–115. [Google Scholar] [CrossRef] [Green Version]
- Samitz, G.; Egger, M.; Zwahlen, M. Domains of physical activity and all-cause mortality: Systematic review and dose-response meta-analysis of cohort studies. Int. J. Epidemiol. 2011, 40, 1382–1400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giles-Corti, B.; Donovan, R.J. The relative influence of individual, social and physical environment determinants of physical activity. Soc. Sci. Med. 2002, 54, 1793–1812. [Google Scholar] [CrossRef]
- Heath, G.W.; Parra, D.C.; Sarmiento, O.L.; Andersen, L.B.; Owen, N.; Goenka, S.; Montes, F.; Brownson, R.C.; Lancet Physical Activity Series Working Group. Evidence-based intervention in physical activity: Lessons from around the world. Lancet 2012, 380, 272–281. [Google Scholar] [CrossRef] [Green Version]
- Baker, P.R.; Francis, D.P.; Soares, J.; Weightman, A.L.; Foster, C. Community wide interventions for increasing physical activity. Cochrane Database Syst. Rev. 2015, 1, CD008366. [Google Scholar] [CrossRef] [Green Version]
- Garrett, S.; Elley, C.R.; Rose, S.B.; O’Dea, D.; Lawton, B.A.; Dowell, A.C. Are physical activity interventions in primary care and the community cost-effective? A systematic review of the evidence. Br. J. Gen. Pract. 2011, 61, e125–e133. [Google Scholar] [CrossRef] [Green Version]
- Vijay, G.C.; Wilson, E.C.; Suhrcke, M.; Hardeman, W.; Sutton, S.; VBI Programme Team. Are brief interventions to increase physical activity cost-effective? A systematic review. Br. J. Sports Med. 2016, 50, 408–417. [Google Scholar]
- Ainsworth, B.E.; Youmans, C.P. Tools for physical activity counseling in medical practice. Obes. Res. 2002, 10 (Suppl. 1), 69S–75S. [Google Scholar] [CrossRef] [Green Version]
- Gagliardi, A.R.; Abdallah, F.; Faulkner, G.; Ciliska, D.; Hicks, A. Factors contributing to the effectiveness of physical activity counselling in primary care: A realist systematic review. Patient Educ. Couns. 2015, 98, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Carroll, J.K.; Fiscella, K.; Epstein, R.M.; Sanders, M.R.; Williams, G.C. A 5A’s communication intervention to promote physical activity in underserved populations. BMC Health Serv. Res. 2012, 12, 374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alahmed, Z.; Lobelo, F. Physical activity promotion in Saudi Arabia: A critical role for clinicians and the health care system. J. Epidemiol. Glob. Health 2018, 7 (Suppl. 1), S7–S15. [Google Scholar] [CrossRef] [PubMed]
- Vallis, M.; Piccinini-Vallis, H.; Sharma, A.M.; Freedhoff, Y. Clinical review: Modified 5 As: Minimal intervention for obesity counseling in primary care. Can. Fam. Physician 2013, 59, 27–31. [Google Scholar] [PubMed]
- Moattari, M.; Ghobadi, A.; Beigi, P.; Pishdad, G. Impact of self-management on metabolic control indicators of diabetes patients. J. Diabetes Metab. Disord. 2012, 11, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Welzel, F.D.; Bär, J.; Stein, J.; Löbner, M.; Pabst, A.; Luppa, M.; Grochtdreis, T.; Kersting, A.; Blüher, M.; Luck-Sikorski, C.; et al. Using a brief web-based 5A intervention to improve weight management in primary care: Results of a cluster-randomized controlled trial. BMC Fam. Pract. 2021, 22, 61. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ. 2021, 372, n160. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J. Cochrane Handbook for Systematic Reviews of Interventions Version 6.3. 2022. Available online: https://www.training.cochrane.org/handbook (accessed on 8 March 2023).
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [Green Version]
- Review Manager (RevMan) [Computer Program], Version 5.4; The Cochrane Collaboration: London, UK, 2020.
- Guerra, P.H.; Soares, H.F.; Mafra, A.B.; Czarnobai, I.; Cruz, G.A.; Weber, W.V.; Farias, J.C.H.; Loch, M.R.; Ribeiro, E.H.C. Educational interventions for physical activity among Brazilian adults: Systematic review. Rev. Saude. Publica. 2021, 55, 110. [Google Scholar] [CrossRef]
- Galaviz, K.I.; Estabrooks, P.A.; Ulloa, E.J.; Lee, R.E.; Janssen, I.; López, Y.; Taylor, J.; Ortiz-Hernández, L.; Lévesque, L. Evaluating the effectiveness of physician counseling to promote physical activity in Mexico: An effectiveness-implementation hybrid study. Transl. Behav. Med. 2017, 7, 731–740. [Google Scholar] [CrossRef] [Green Version]
- Reed, J.R.; Estabrooks, P.; Pozehl, B.; Heelan, K.; Wichman, C. Effectiveness of the 5A’s model for changing physical activity behaviors in rural adults recruited from Primary Care Clinics. J. Phys. Act. Health 2019, 16, 1138–1146. [Google Scholar] [CrossRef] [PubMed]
- Viglione, C.; Bouwman, D.; Rahman, N.; Fang, Y.; Beasley, J.M.; Sherman, S.; Pi-Sunyer, X.; Wylie-Rosett, J.; Tenner, C.; Jay, M. A technology-assisted health coaching intervention vs. enhanced usual care for Primary Care-based obesity treatment: A randomized controlled trial. BMC Obes. 2019, 6, 4. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Yin, G.; Li, G.; Liang, W.; Wei, Q. Efficacy of physical activity counseling plus sleep restriction therapy on the patients with chronic insomnia. Neuropsychiatr. Dis. Treat. 2015, 11, 2771–2778. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World. Geneva. 2018. Available online: https://apps.who.int/iris/bitstream/handle/10665/272722/9789241514187-eng.pdf. (accessed on 8 March 2023).
- Prochaska, J.O.; DiClemente, C.C. Stages of change in the modification of problem behaviors. Prog. Behav. Modif. 1992, 28, 183–218. [Google Scholar] [PubMed]
- Costa, E.F.; Guerra, P.H.; Santos, T.I.; Florindo, A.A. Systematic review of physical activity promotion by community health workers. Prev. Med. 2015, 81, 114–121. [Google Scholar] [CrossRef]
- Wilcox, S.; Castro, C.; King, A.C.; Housemann, R.; Brownson, R.C. Determinants of leisure time physical activity in rural compared with urban older and ethnically diverse women in the United States. J. Epidemiol. Community Health 2000, 54, 667–672. [Google Scholar] [CrossRef] [Green Version]
- Florindo, A.A.; Mielke, G.I.; Gomes, G.A.; Ramos, L.R.; Bracco, M.M.; Parra, D.C.; Simoes, E.J.; Lobelo, F.; Hallal, P.C. Physical activity counseling in primary health care in Brazil: A national study on prevalence and associated factors. BMC Public Health 2013, 13, 794. [Google Scholar] [CrossRef] [Green Version]
- Füzéki, E.; Weber, T.; Groneberg, D.A.; Banzer, W. Physical Activity Counseling in Primary Care in Germany-An Integrative Review. Int. J. Environ. Res. Public Health 2020, 17, 5625. [Google Scholar] [CrossRef]
- Lugones-Sanchez, C.; Crutzen, R.; Recio-Rodriguez, J.I.; Garcia-Ortiz, L. Establishing the relevance of psychological determinants regarding physical activity in people with overweight and obesity. Int. J. Clin. Health Psychol. 2021, 21, 100250. [Google Scholar] [CrossRef]
- Panagiotakos, D.B.; Pitsavos, C.; Lentzas, Y.; Skoumas, Y.; Papadimitriou, L.; Zeimbekis, A.; Stefanadis, C. Determinants of physical inactivity among men and women from Greece: A 5-year follow-up of the ATTICA study. Ann. Epidemiol. 2008, 18, 387–394. [Google Scholar] [CrossRef]
- Sialino, L.D.; Picavet, H.S.J.; Wijnhoven, H.A.H.; Loyen, A.; Verschuren, W.M.M.; Visser, M.; Schaap, L.S.; van Oostrom, S.H. Exploring the difference between men and women in physical functioning: How do sociodemographic, lifestyle- and health-related determinants contribute? BMC Geriatr. 2022, 22, 610. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Reference | Country | Mean Age (% of Women) | Sample Characteristics | Main Objective |
|---|---|---|---|---|
| Galaviz et al., 2017 [22] | México | 49 (77) | Adults who do not meet physical activity recommendations, but without clinical impediments. | Increase the use of the 5A model in counseling and observe whether the intervention provided an increase in users’ physical activity. |
| Reed et al., 2019 [23] | United States | 48 (80) | Inactive adults assisted by a primary health care unit located in a rural setting. | Test the use of the 5A model in counseling to increase physical activity. |
| Viglione et al., 2019 [24] | United States | 55 (33) | Veterans with a BMI ≥ 30 kg/m2 or between 25 and 29.9 km/m2 diagnosed with a comorbidity (hypertension, obstructive sleep apnea, high cholesterol, prediabetes, and metabolic syndrome). | Determine the feasibility and acceptability of a technology-based method compared to usual care. Test the impact of this method on weight, diet, and physical activity. |
| Wang et al., 2015 [25] | China | 40 (65) | Adults with chronic insomnia. | Verify the effects of a counseling-based intervention on physical activity and sleep restriction. |
| Reference | Study Design | Professionals Who Implemented the Intervention | Study Protocol |
|---|---|---|---|
| Galaviz et al., 2017 [22] | Effectiveness-implementation hybrid study. | General practitioners working in the public health service. | Previously trained physicians offered counseling based on the 5A model in regular consultations. |
| Reed et al., 2019 [23] | Randomized Controlled Trial. | Nurses and Researchers. | Elaborating action plans to improve self-regulation and sending motivational weekly text messages. |
| Viglione et al., 2019 [24] | Randomized Controlled Trial. | Health professionals and students. | Delivery of educational material and counseling (face-to-face and remote). |
| Wang et al., 2015 [25] | Randomized Controlled Trial, | Psychologists. | Offer of four weekly counseling sessions, adjustment of prescription and sleep restriction strategy. |
| Reference | Tools Used to Assess Physical Activity | Intervention Group | Control Group | Physical Activity Indicator (Time in Which the Assessment Took Place) | Result |
|---|---|---|---|---|---|
| Galaviz et al., 2017 [22] | Questionnaire GLTEQ | 228 * | 231 | Physical activity score (6 months post-intervention). | Data were not statistically significant (numbers were not presented in the report). |
| Number of people classified as physically active (6 months post-intervention). | Data were not statistically significant (numbers were not presented in the report). | ||||
| Reed et al., 2019 [23] | Questionnaire GLTEQ; Fitbit Charge 2 | 29 | 30 | Assessment by questionnaire (4 months). | 8.1 (95%CI = 0.1; 16.1) |
| Weekly number of steps (4 months). | 1266 (95%CI = −520; 3052) | ||||
| Active weekly minutes (4 months). | 42 (95%CI = −102; 186) | ||||
| Viglione et al., 2019 [24] | PaffenbargerPhysical Activity Questionnaire | 21 | 22 | Self-efficacy for physical activity (3 months). | −1.1 (95%CI = −6.8; 4.7); |
| Self-efficacy for physical activity (6 months). | 2.1 (95%CI = −4.5; 8.8) | ||||
| Self-efficacy for physical activity (12 months). | −2.2 (95%CI = −9.1; 4.1) | ||||
| Wang et al., 2015 [25] | IPAQ Long version | 35 | 36 | Daily number of steps (4 months). | 2231 (95%CI = 474; 3987) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guerra, P.H.; Sposito, L.A.C.; da Costa, F.F.; Fermino, R.C.; Papini, C.B.; Rech, C.R. Effectiveness of the 5A Counseling Model-Based Interventions on Physical Activity Indicators in Adults: A Systematic Review. Behav. Sci. 2023, 13, 476. https://doi.org/10.3390/bs13060476
Guerra PH, Sposito LAC, da Costa FF, Fermino RC, Papini CB, Rech CR. Effectiveness of the 5A Counseling Model-Based Interventions on Physical Activity Indicators in Adults: A Systematic Review. Behavioral Sciences. 2023; 13(6):476. https://doi.org/10.3390/bs13060476
Chicago/Turabian StyleGuerra, Paulo Henrique, Letícia Aparecida Calderão Sposito, Filipe Ferreira da Costa, Rogério César Fermino, Camila Bosquiero Papini, and Cassiano Ricardo Rech. 2023. "Effectiveness of the 5A Counseling Model-Based Interventions on Physical Activity Indicators in Adults: A Systematic Review" Behavioral Sciences 13, no. 6: 476. https://doi.org/10.3390/bs13060476