
Expanding the Trauma-Informed Care Measurement Toolkit: An Evaluation of the Attitudes Related to Trauma-Informed Care (ARTIC-45) Scale with SUD Workers in PIMH

 , , and
, , and
Abstract
:1. Introduction
2. Literature Review
2.1. TIC in Practice
2.2. Introduction to the ARTIC
3. Methods
3.1. Participants
3.2. Procedures
3.3. Measures
3.4. Data Analysis
3.4.1. Quantitative
3.4.2. Qualitative
4. Results
4.1. Item Analysis
4.2. Cronbach’s Alpha
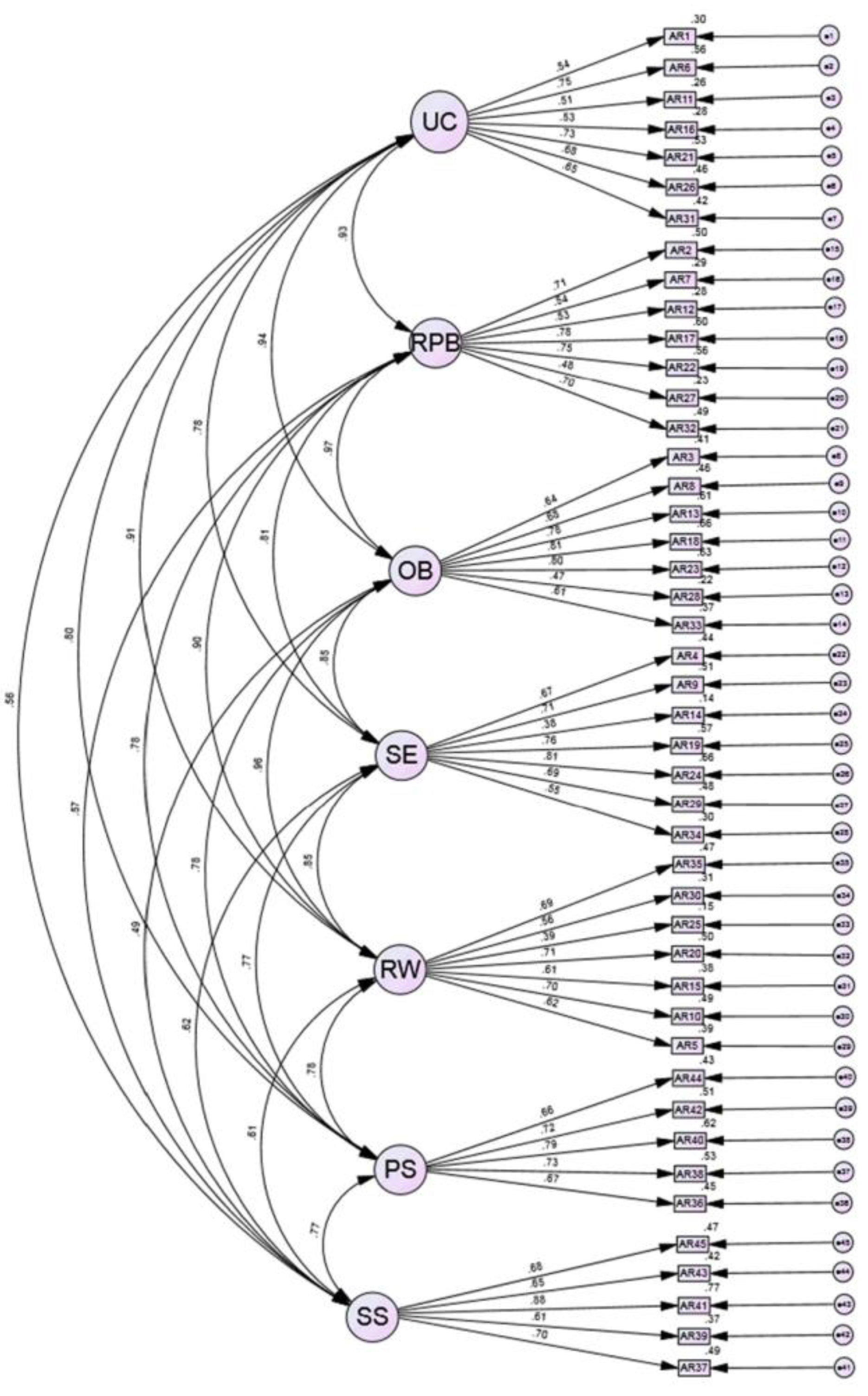
4.3. Confirmatory Factor Analysis
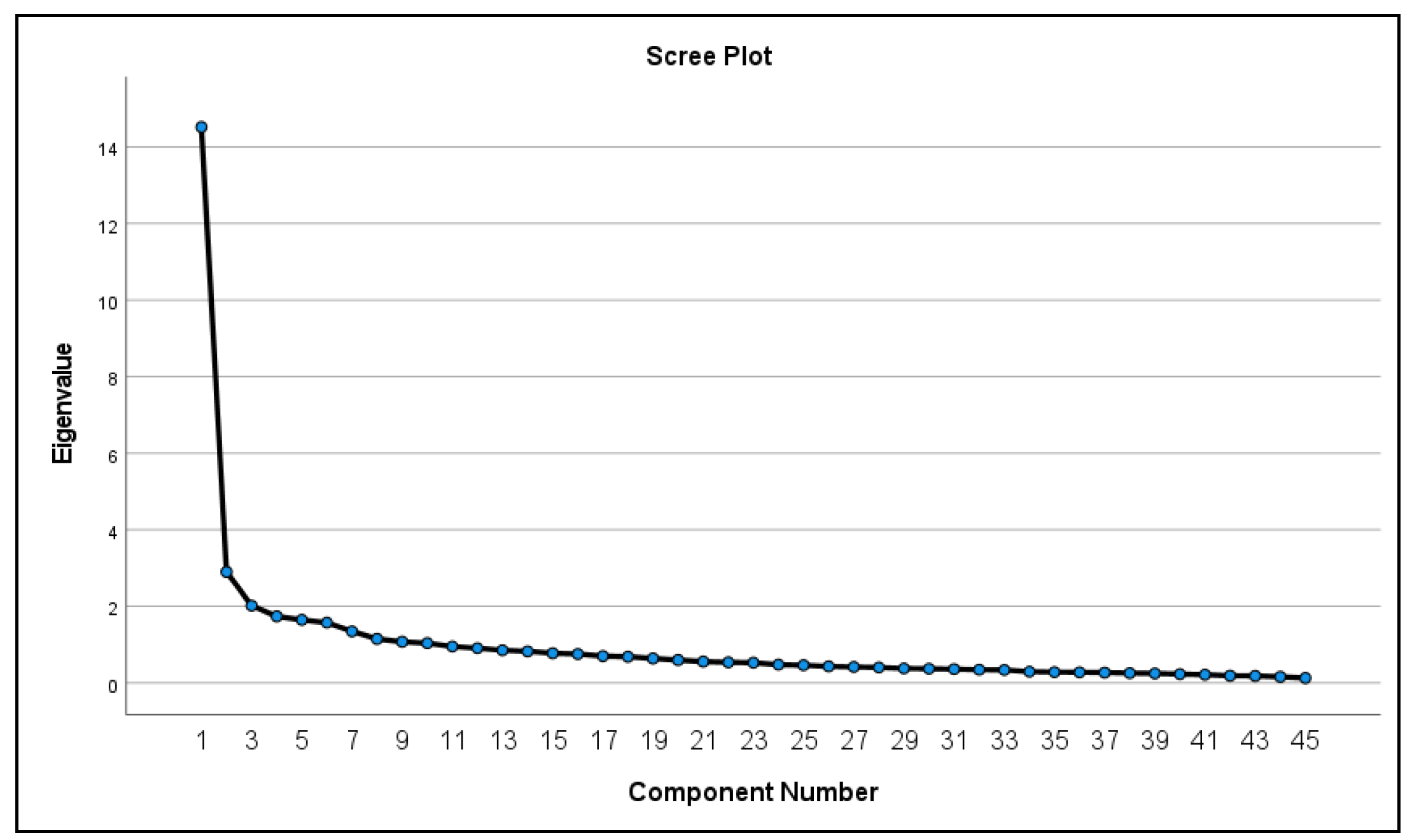
4.4. Exploratory Factor Analysis and Sensitivity Analyses
4.5. Qualitative Analysis
5. Discussion
6. Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Felitti, V.J.; Anda, R.F.; Nordenberg, D.; Williamson, D.F.; Spitz, A.M.; Edwards, V.; Koss, M.P.; Marks, J.S. Relationship of Childhood Abuse and Household Dysfunction to Many of the Leading Causes of Death in Adults: The Adverse Childhood Experiences (ACE) Study. Am. J. Prev. Med. 1998, 14, 245–258. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; McLaughlin, K.A.; Green, J.G.; Gruber, M.J.; Sampson, N.A.; Zaslavsky, A.M.; Aguilar-Gaxiola, S.; Alhamzawi, A.O.; Alonso, J.; Angermeyer, M.; et al. Childhood adversities and adult psychopathology in the WHO World Mental Health Surveys. Br. J. Psychiatry 2010, 197, 378–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Racine, N.; Eirich, R.; Dimitropoulos, G.; Hartwick, C.; Madigan, S. Development of trauma symptoms following adversity in childhood: The moderating role of protective factors. Child Abuse Negl. 2020, 101, 104375. [Google Scholar] [CrossRef] [PubMed]
- Becker-Blease, K.A. As the world becomes trauma-informed, work to do. J. Trauma Dissociation 2017, 18, 131–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Champine, R.B.; Lang, J.M.; Nelson, A.M.; Hanson, R.F.; Tebes, J.K. Systems Measures of a Trauma-Informed Approach: A Systematic Review. Am. J. Community Psychol. 2019, 64, 418–437. [Google Scholar] [CrossRef]
- Donisch, K.; Bray, C.; Gewirtz, A. Child welfare, juvenile justice, mental health, and education providers’ conceptualizations of trauma-informed practice. Child Maltreatment 2016, 21, 125–134. [Google Scholar] [CrossRef]
- Hanson, R.F.; Lang, J. A critical look at trauma-informed care among agencies and systems serving maltreated youth and their families. Child Maltreatment 2016, 21, 95–100. [Google Scholar] [CrossRef]
- Bailey, C.; Klas, A.; Cox, R.; Bergmeier, H.; Avery, J.; Skouteris, H. Systematic review of organisation-wide, trauma-informed care models in out-of-home care (Oo HC) settings. Health Soc. Care Community 2019, 27, e10–e22. [Google Scholar] [CrossRef] [Green Version]
- Substance Abuse and Mental Health Services Administration, [SAMHSA]. SAMHSA’s Concept of Trauma and Guidance for a Trauma-Informed Approach; SMA 15-4884; Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2014; p. 27. Available online: https://www.nasmhpd.org/sites/default/files/SAMHSA_Concept_of_Trauma_and_Guidance.pdf (accessed on 21 April 2023).
- Substance Abuse and Mental Health Services Administration, [SAMHSA]. Resources for Child Trauma-Informed Care; Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2021. Available online: https://www.samhsa.gov/childrens-awareness-day/past-events/2018/child-traumatic-stress-resources (accessed on 21 April 2023).
- Wall, L.; Higgins, D.; Hunter, C. Trauma-informed care in child/family welfare services. AIFS 2016, 37, 2–19. Available online: https://aifs.gov.au/sites/default/files/publication-documents/cfca37-trauma-informed-practice_0.pdf (accessed on 10 April 2023).
- Fraser, J.G.; Griffin, J.; Barto, B.; Lo, C.; Wenz-Gross, M.; Spinazzola, J.; Bodian, R.A.; Nisenbaum, J.M.; Bartlett, J. Implementation of a workforce initiative to build trauma-informed child welfare practice and services: Findings from the Massachusetts Child Trauma Project. Child. Youth Serv. Rev. 2014, 44, 233–242. [Google Scholar] [CrossRef]
- Ko, S.; Ford, J.; Kassam-Adams, N.; Berkowitz, S.; Wilson, C.; Wong, M.; Brymer, M.J.; Layne, C. Trauma-informed systems: Child welfare, education, first responders, health care, juvenile justice. Prof. Psychol. Res. Pract. 2008, 39, 396–404. [Google Scholar] [CrossRef] [Green Version]
- Lowenthal, A. Trauma-informed care implementation in the child-and youth-serving sectors: A scoping review. Int. J. Child Adolesc. Resil. 2020, 7, 178–194. [Google Scholar] [CrossRef]
- Bosk, E.A. Creating A Parallel Process: A New Methodological Framework for Conducting Trauma-Informed Evaluation and Research (TIER) in Mental Health Settings. Eval. Program Plann. 2023, 97, 102229. [Google Scholar] [CrossRef]
- Hanson, R.F.; Lang, J.M.; Fraser, J.G.; Agosti, J.R.; Ake, G.S.; Donisch, K.M.; Gewirtz, A.H. Trauma-informed care: Definitions and statewide initiatives. In The APSAC Handbook on Child Maltreatment, 4th ed.; Klika, J.B., Conte, J.R., Eds.; SAGE Publications: Los Angeles, CA, USA, 2018; pp. 272–291. [Google Scholar]
- Lang, J.; Campbell, K.; Shanley, P.; Crusto, C.; Connell, C. Building Capacity for Trauma-Informed Care in the Child Welfare System: Initial Results of a Statewide Implementation. Child Maltreatment 2016, 21, 113–124. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, K.; Murray, K.; Ake, G. Trauma-Informed Care for Children in the Child Welfare System: An Initial Evaluation of a Trauma-Informed Parenting Workshop. Child Maltreatment 2016, 21, 147–155. [Google Scholar] [CrossRef]
- Wathen, C.N.; Schmitt, B.; MacGregor, J.C. Measuring trauma-(and violence-) informed care: A scoping review. Trauma Violence Abus. 2023, 24, 261–277. [Google Scholar] [CrossRef]
- Baker, C.N.; Brown, S.M.; Wilcox, P.D.; Overstreet, S.; Arora, P. Development and Psychometric Evaluation of the Attitudes Related to Trauma-Informed Care (ARTIC) Scale. Sch. Ment. Health 2016, 8, 61–76. [Google Scholar] [CrossRef]
- Parker, J.; Olson, S.; Bunde, J. The Impact of Trauma-Based Training on Educators. J. Child Adolesc. Trauma 2019, 13, 217–227. [Google Scholar] [CrossRef]
- Stokes, Y.; Jacob, J.-D.; Squires, J.; Vandyk, A. Using the ARTIC-35 to Measure Nurses’ Attitudes Related to Trauma-Informed Care. J. Nurs. Meas. 2020, 28, 185–199. [Google Scholar] [CrossRef]
- Kataoka, M.; Kotake, R.; Asaoka, H.; Miyamoto, Y.; Nishi, D. Reliability and Validity of the Japanese Version of the Attitudes Related to Trauma-Informed Care (ARTIC-10) Scale. Int. J. Trauma Nurs. 2022, 29, 312–318. [Google Scholar] [CrossRef]
- Baker, C.N.; Brown, S.M.; Overstreet, S.; Wilcox, P. Validation of the Attitudes Related to Trauma-Informed Care Scale (ARTIC). Psychol. Trauma-US 2021, 13, 505–513. [Google Scholar] [CrossRef]
- Thirkle, S.; Kennedy, A.; Sice, P. Instruments for exploring trauma-informed care. J. Health Hum. Serv. Adm. 2021, 44, 30–44. [Google Scholar]
- Bloom, S.L. Advancing a national cradle-to-grave-to-cradle public health agenda. J. Trauma Dissociation 2016, 17, 383–396. [Google Scholar] [CrossRef]
- Murphy, K.; Moore, K.A.; Redd, Z.; Malm, K. Trauma-informed child welfare systems and children’s well-being: A longitudinal evaluation of KVC’s bridging the way home initiative. Child. Youth Serv. Rev. 2017, 75, 23–34. [Google Scholar] [CrossRef]
- Reeves, E. A synthesis of the literature on trauma-informed care. Issues Ment. Health Nurs. 2015, 36, 698–709. [Google Scholar] [CrossRef]
- Brown, S.; Baker, C.; Wilcox, P. Risking connection trauma training: A pathway toward trauma-informed care in child congregate care settings. J. Psychol. Trauma 2012, 4, 507–515. [Google Scholar] [CrossRef] [Green Version]
- Green, B.; Saunders, P.; Power, E.; Dass-Brailsford, P.; Schelbert, K.; Giller, E.; Wissow, L.; Hurtado de Mendoza, A.; Mete, M. Trauma-Informed Medical Care: Patient Response to a Primary Care Provider Communication Training. J. Loss Trauma 2016, 21, 147–159. [Google Scholar] [CrossRef] [Green Version]
- Greenwald, R.; Siradas, L.; Schmitt, T.A.; Reslan, S.; Fierle, J.; Sande, B. Implementing trauma-informed treatment for youth in a residential facility: First-year outcomes. Resid. Treat. Child. Youth 2012, 29, 141–153. [Google Scholar] [CrossRef]
- Guarino, K.M. Trauma-Informed Care for Families Experiencing Homelessness. In Supporting Families Experiencing Homelessness: Current Practices and Future Directions; Haskett, M.E., Perlman, S., Cowan, B.A., Eds.; Springer: New York, NY, USA, 2014; pp. 121–143. [Google Scholar]
- Hodgdon, H.B.; Kinniburgh, K.; Gabowitz, D.; Blaustein, M.E.; Spinazzola, J. Development and implementation of trauma-informed programming in youth residential treatment centers using the ARC framework. J. Fam. Violence 2013, 28, 679–692. [Google Scholar] [CrossRef]
- Beyerlein, B.A.; Bloch, E. Need for Trauma-Informed Care within the Foster Care System. Child Welf. 2014, 93, 7–22. [Google Scholar]
- Bruce, M.M.; Kassam-Adams, N.; Rogers, M.; Anderson, K.M.; Sluys, K.P.; Richmond, T.S. Trauma Providers’ Knowledge, Views and Practice of Trauma-Informed Care. J. Trauma Nurs. 2018, 25, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Kramer, T.L.; Sigel, B.A.; Conners-Burrow, N.A.; Savary, P.E.; Tempel, A. A statewide introduction of trauma-informed care in a child welfare system. Child. Youth Serv. Rev. 2013, 35, 19–24. [Google Scholar] [CrossRef]
- De Leon, G. Therapeutic communities for substance abuse: Overview of approach and effectiveness. Psychol. Addict. Behav. 1989, 3, 140–147. [Google Scholar] [CrossRef]
- Saakvitne, K.W.; Gamble, S.; Pearlman, L.A.; Tabor Lev, B. Risking Connection: A Training Curriculum for Working with Survivors of Childhood Abuse; Sidran Press: Baltimore, MD, USA, 2001. [Google Scholar]
- DeVellis, R. Scale Development: Theory and Applications, 4th ed.; SAGE Publications: Los Angeles, CA, USA, 2017. [Google Scholar]
- Woods, S.; Hampson, S. Measuring the Big Five with single items using a bipolar response scale. Eur. J. Personal. 2005, 19, 373–390. [Google Scholar] [CrossRef]
- Kinniburgh, K.J.; Blaustein, M.; Spinazzola, J.; Van der Kolk, B.A. Attachment, self-regulation, and competency. Psychiatr. Ann. 2005, 35, 424–430. [Google Scholar] [CrossRef] [Green Version]
- Byrne, B.M. Structural Equation Modeling with AMOS: Basic Concepts, Applications, and Programming; Routledge: Abingdon, UK, 2016. [Google Scholar]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Goretzko, D.; Pham, T.T.H.; Bühner, M. Exploratory factor analysis: Current use, methodological developments and recommendations for good practice. Curr. Psychol. 2021, 40, 3510–3521. [Google Scholar] [CrossRef]
- Marsh, H.W.; Morin, A.J.; Parker, P.D.; Kaur, G. Exploratory Structural Equation Modeling: An Integration of the Best Features of Exploratory and Confirmatory Factor Analysis. Annu. Rev. Clin. Psychol. 2014, 10, 85–110. [Google Scholar] [CrossRef] [Green Version]
- Costello, A.B.; Osborne, J. Best practices in exploratory factor analysis: Four recommendations for getting the most from your analysis. Pract. Assess. Res. Eval. 2005, 10, 7. [Google Scholar]
- Fabrigar, L.R.; Wegener, D.T.; MacCallum, R.C.; Strahan, E.J. Evaluating the Use of Exploratory Factor Analysis in Psychological Research. Psychol. Methods 1999, 4, 272–299. [Google Scholar] [CrossRef]
- Reise, S.P.; Ainsworth, A.T.; Haviland, M.G. Item response theory: Fundamentals, applications, and promise in psychological research. Curr. Dir.Psychol. Sci. 2005, 14, 95–101. [Google Scholar] [CrossRef]
- Raykov, T. Coefficient alpha and composite reliability with interrelated nonhomogeneous items. Appl. Psychol. Meas. 1998, 22, 375–385. [Google Scholar] [CrossRef]
- Tasaki, K.; Shin, J. Japanese response bias: Cross-level and cross-national comparisons on response styles. Jpn. J. Educ. Psychol. 2017, 88, 32–42. (In Japanese) [Google Scholar] [CrossRef] [Green Version]
- Bardwell, W.A.; Dimsdale, J.E. The Impact of Ethnicity and Response Bias on the Self-Report of Negative Affect. J. Appl. Biobehav. Res. 2001, 6, 27–38. [Google Scholar] [CrossRef]
- Boer, D.; Hanke, K.; He, J. On detecting systematic measurement error in cross-cultural research: A review and critical reflection on equivalence and invariance tests. J. Cross Cult. Psychol. 2018, 49, 713–734. [Google Scholar] [CrossRef]
- Khadjesari, Z.; Boufkhed, S.; Vitoratou, S.; Schatte, L.; Ziemann, A.; Daskalopoulou, C.; Uglik-Marucha, E.; Sevaldis, N.; Hull, L. Implementation outcome instruments for use in physical healthcare settings: A systematic review. Implement. Sci. 2020, 15, 1–16. [Google Scholar] [CrossRef]
- Raykov, T.; Shrout, P.E. Reliability of scales with general structure: Point and interval estimation using a structural equation modeling approach. Struct. Equ. Model. 2002, 9, 195–212. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Mean or % (n) | |
|---|---|
| Sex | |
| Male | 18.1 (42) |
| Female | 81.9 (190) |
| Race | |
| Black or African American | 16.4 (37) |
| Asian | 3.1 (7) |
| Latino | 16.4 (37) |
| Multiracial | 5.8 (13) |
| White | 58.4 (132) |
| Hispanic | |
| Hispanic | 19.6 (44) |
| Not Hispanic | 80.4 (180) |
| Education Level | |
| Completed HS or GED | 7 (16) |
| Some College | 10.4 (24) |
| Completed College | 20.4 (47) |
| Some Masters Completed | 6.5 (15) |
| Masters Completed | 52.6 (121) |
| Completed PhD or equivalent | 3 (7) |
| Annual Income | |
| <USD 20,000 | 2.27 (6) |
| USD 20,000–USD 40,000 | 32.4 (73) |
| USD 40,000–USD 60,000 | 41.8 (94) |
| USD 60,000–USD 80,000 | 14.2 (32) |
| USD 80,000+ | 8.9 (20) |
| ARTIC 45 Original Constructs | Constructs following Qual Content Analysis |
|---|---|
| Underlying causes of problem behavior and symptoms | Organizational support for provision of TIC |
| Responses to problem behavior and symptoms | Trauma theory |
| On-the-job behavior | Reflective functioning on the job |
| Self-efficacy at work | Worker efficacy |
| Reactions to the work | Relationships with clients |
| Personal support of TIC | Efficacy of TIC |
| System-wide support of TIC | Importance of consequences |
| Beliefs about clients | |
| Secondary traumatic stress |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mendez, A.; Bosk, E.A.; Keller, A.; Williams-Butler, A.; Hardan, T.; Ruisard, D.J.; MacKenzie, M.J. Expanding the Trauma-Informed Care Measurement Toolkit: An Evaluation of the Attitudes Related to Trauma-Informed Care (ARTIC-45) Scale with SUD Workers in PIMH. Behav. Sci. 2023, 13, 471. https://doi.org/10.3390/bs13060471
Mendez A, Bosk EA, Keller A, Williams-Butler A, Hardan T, Ruisard DJ, MacKenzie MJ. Expanding the Trauma-Informed Care Measurement Toolkit: An Evaluation of the Attitudes Related to Trauma-Informed Care (ARTIC-45) Scale with SUD Workers in PIMH. Behavioral Sciences. 2023; 13(6):471. https://doi.org/10.3390/bs13060471
Chicago/Turabian StyleMendez, Alicia, Emily A. Bosk, Amanda Keller, Abigail Williams-Butler, Tareq Hardan, Debra J. Ruisard, and Michael J. MacKenzie. 2023. "Expanding the Trauma-Informed Care Measurement Toolkit: An Evaluation of the Attitudes Related to Trauma-Informed Care (ARTIC-45) Scale with SUD Workers in PIMH" Behavioral Sciences 13, no. 6: 471. https://doi.org/10.3390/bs13060471