

The Effects of Repeated Attachment Security Priming on Social Anxiety and Attention Bias: A Randomized Controlled Trial

Abstract
:1. Introduction
2. Method
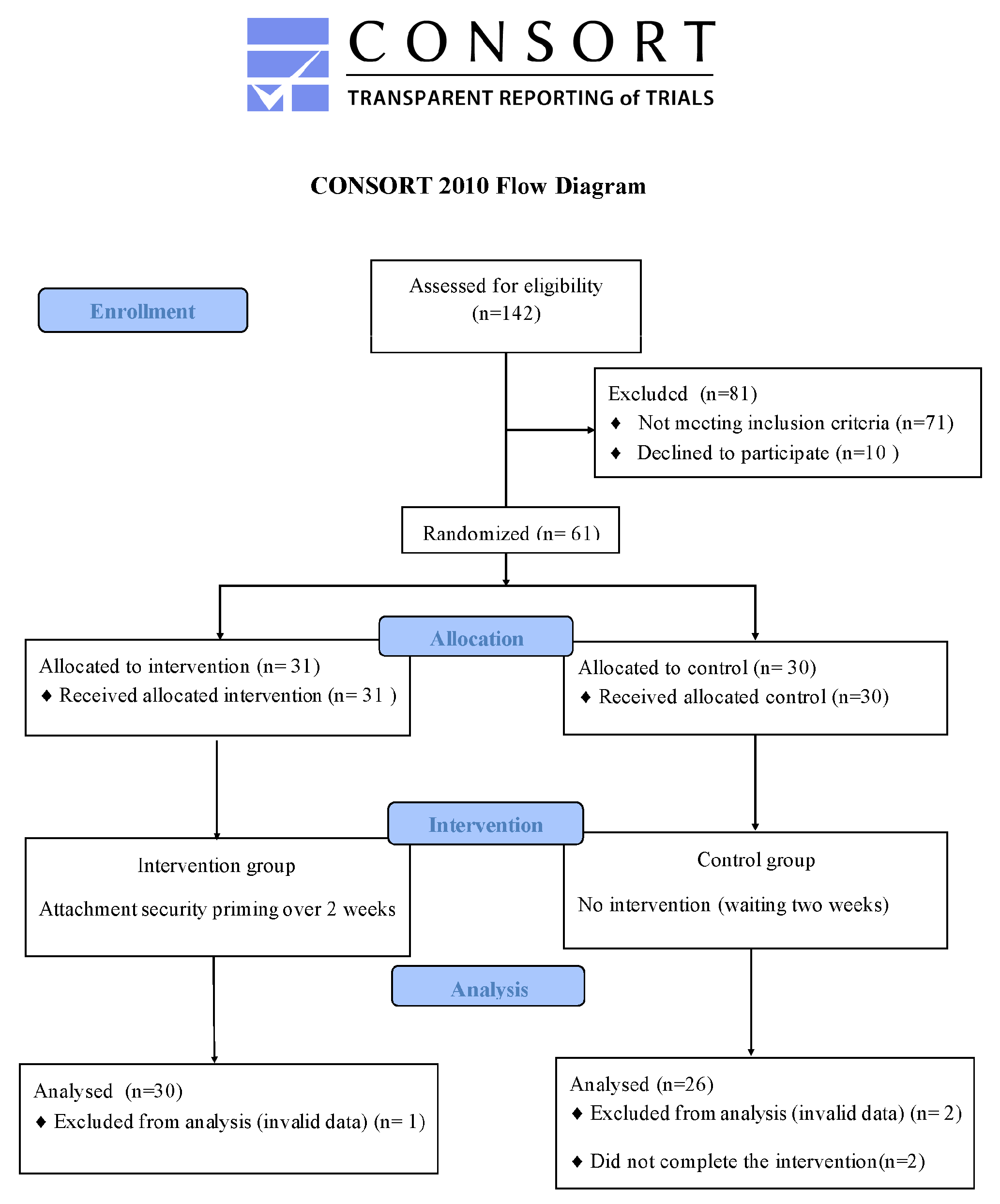
2.1. Study Design
2.2. Participants
2.3. Questionnaires
2.3.1. Experience of Close Relationship-Short, ECR-S
2.3.2. Interaction Anxiety Scale, IAS
2.4. Procedures
2.5. Attachment Security Priming
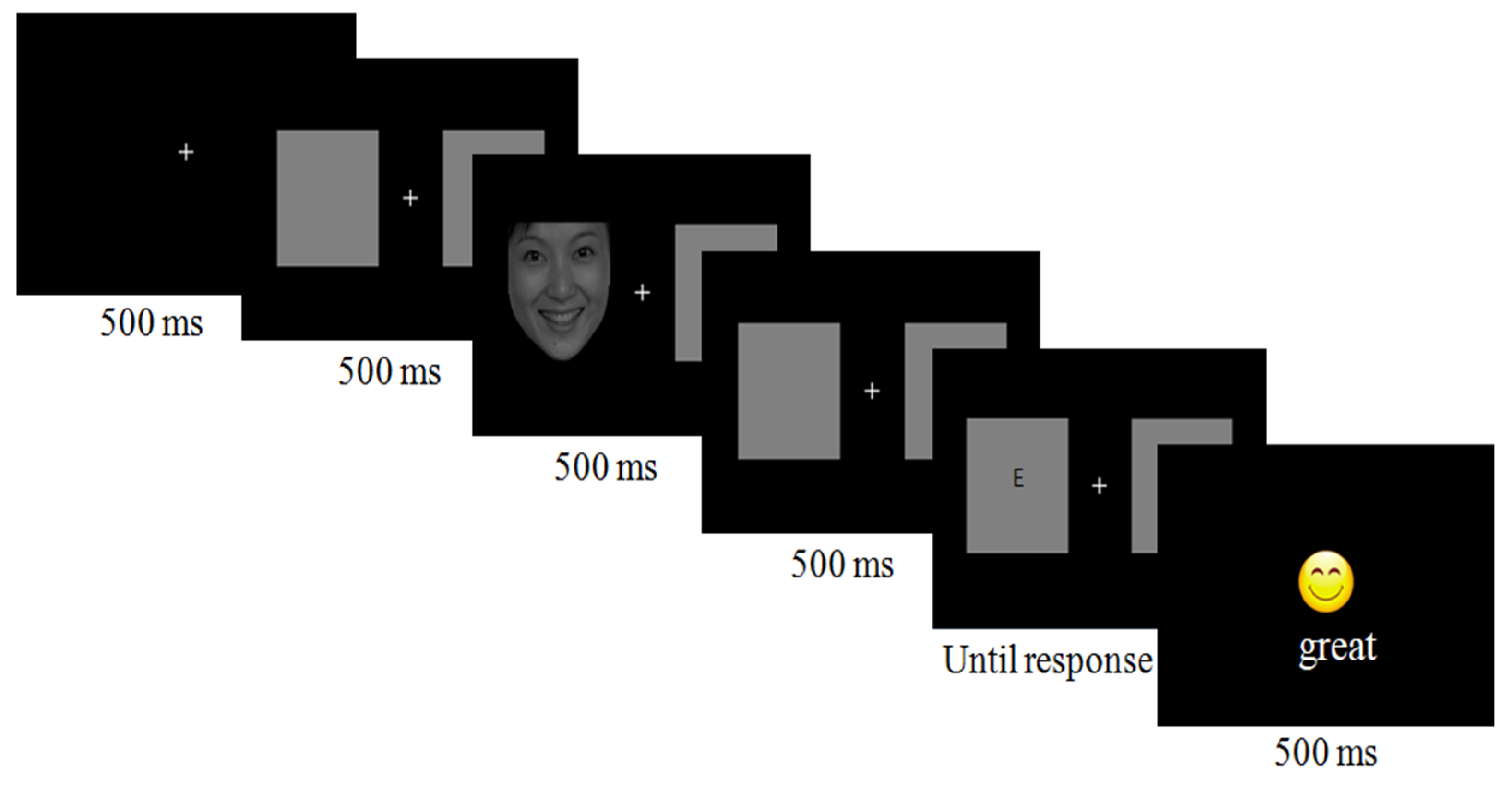
2.6. Spatial Cueing Task
2.7. Data Analysis
3. Results
3.1. Descriptive Statistics
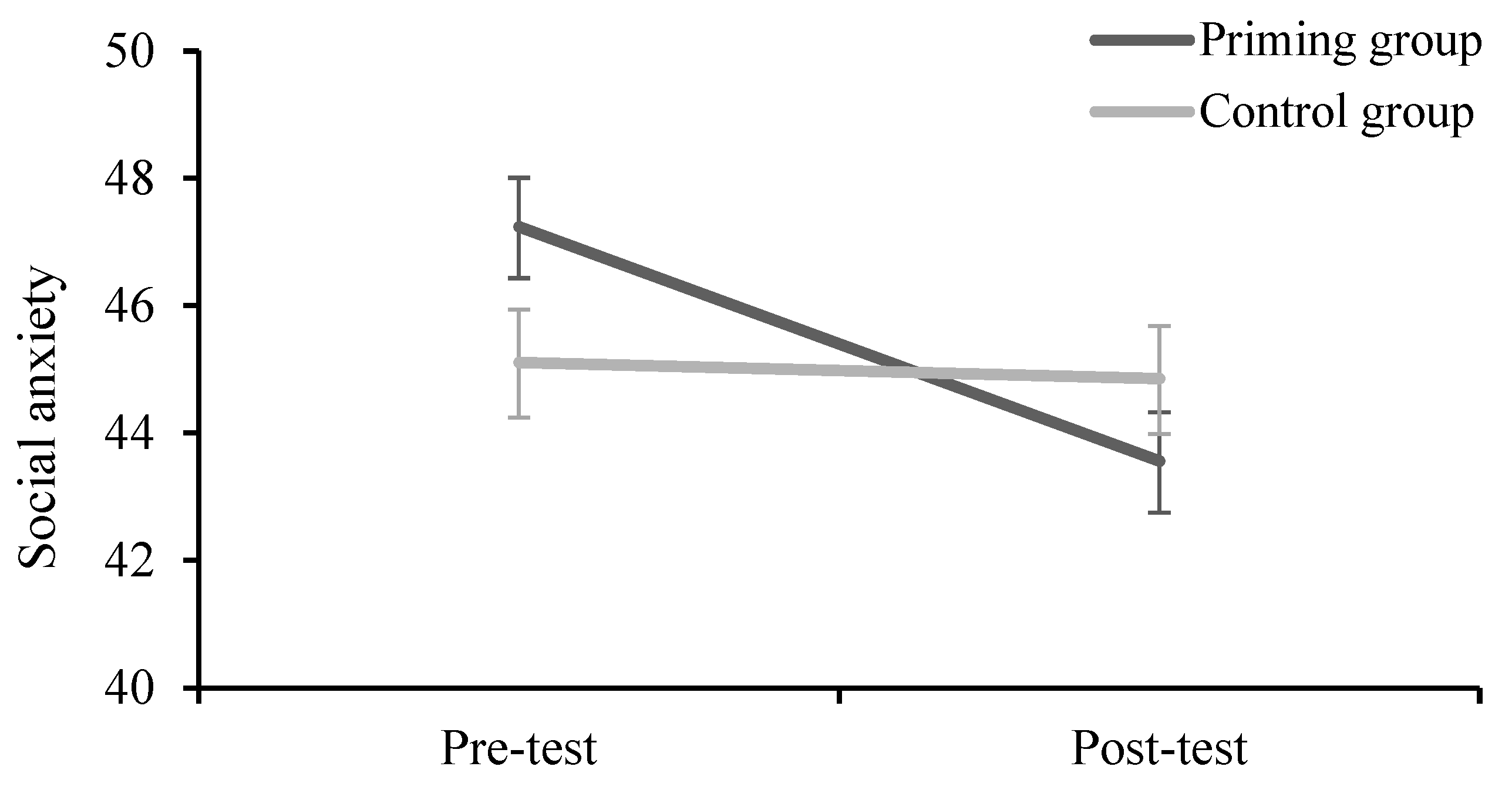
3.2. Social Anxiety
3.3. Attention Bias
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Adams, G.C.; Balbuena, L.; Meng, X.; Asmundson, G.J. When social anxiety and depression go together: A population study of comorbidity and associated consequences. J. Affect. Disord. 2016, 206, 48–54. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Johnston, L.D.; O’Malley, P.M.; Bachman, J.G.; Schulenberg, J.E.; Miech, R.A. Monitoring the Future National Survey Results on Drug Use, 1975–2014: Volume II, College Students and Adults Ages 19–55; Institute for Social Research, University of Michigan: Ann Arbor, MI, USA, 2015. [Google Scholar]
- Hakami, R.M.; Mahfouz, M.S.; Adawi, A.M.; Mahha, A.J.; Athathi, A.J.; Daghreeri, H.H.; Najmi, H.H.; Areeshi, N.A. Social anxiety disorder and its impact in undergraduate students at Jazan University, Saudi Arabia. Ment. Illn. 2017, 9, 7274. [Google Scholar] [CrossRef] [PubMed]
- Costello, E.J.; Egger, H.L.; Angold, A. The developmental epidemiology of anxiety disorders: Phenomenology, prevalence, and comorbidity. Child Adolesc. Psychiatr. Clin. 2005, 14, 631–648. [Google Scholar] [CrossRef] [PubMed]
- Buckner, J.D.; Schmidt, N.B.; Lang, A.R.; Small, J.W.; Schlauch, R.C.; Lewinsohn, P.M. Specificity of social anxiety disorder as a risk factor for alcohol and cannabis dependence. J. Psychiatr. Res. 2008, 42, 230–239. [Google Scholar] [CrossRef] [PubMed]
- Buckner, J.D.; Eggleston, A.M.; Schmidt, N.B. Social anxiety and problematic alcohol consumption: The mediating role of drinking motives and situations. Behav. Ther. 2006, 37, 381–391. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C. Lifetime co-morbidities between social phobia and mood disorders in the US National Comorbidity Survey. Psychol. Med. 1999, 29, 555–567. [Google Scholar] [CrossRef]
- Stein, M.B.; Stein, D.J. Social anxiety disorder. Lancet 2008, 371, 1115–1125. [Google Scholar] [CrossRef]
- Hofmann, S.G.; Wu, J.Q.; Boettcher, H.; Sturm, J. Effect of pharmacotherapy for anxiety disorders on quality of life: A meta-analysis. Qual. Life Res. 2014, 23, 1141–1153. [Google Scholar] [CrossRef]
- Koszycki, D.; Benger, M.; Shlik, J.; Bradwejn, J. Randomized trial of a meditation-based stress reduction program and cognitive behavior therapy in generalized social anxiety disorder. Behav. Res. Ther. 2007, 45, 2518–2526. [Google Scholar] [CrossRef]
- Leichsenring, F.; Salzer, S.; Beutel, M.E.; Herpertz, S.; Hiller, W.; Hoyer, J.; Huesing, J.; Joraschky, P.; Nolting, B.; Poehlmann, K. Psychodynamic therapy and cognitive-behavioral therapy in social anxiety disorder: A multicenter randomized controlled trial. Am. J. Psychiatry 2013, 170, 759–767. [Google Scholar] [CrossRef]
- Stangier, U.; Schramm, E.; Heidenreich, T.; Berger, M.; Clark, D.M. Cognitive therapy vs interpersonal psychotherapy in social anxiety disorder: A randomized controlled trial. Arch. Gen. Psychiatry 2011, 68, 692–700. [Google Scholar] [CrossRef] [PubMed]
- Barkowski, S.; Schwartze, D.; Strauss, B.; Burlingame, G.M.; Barth, J.; Rosendahl, J. Efficacy of group psychotherapy for social anxiety disorder: A meta-analysis of randomized-controlled trials. J. Anxiety Disord. 2016, 39, 44–64. [Google Scholar] [CrossRef] [PubMed]
- Butler, R.M.; O’Day, E.B.; Swee, M.B.; Horenstein, A.; Heimberg, R.G. Cognitive behavioral therapy for social anxiety disorder: Predictors of treatment outcome in a quasi-naturalistic setting. Behav. Ther. 2021, 52, 465–477. [Google Scholar] [CrossRef] [PubMed]
- Evans, R.; Clark, D.M.; Leigh, E. Are young people with primary social anxiety disorder less likely to recover following generic CBT compared to young people with other primary anxiety disorders? A systematic review and meta-analysis. Behav. Cogn. Psychother. 2020, 49, 352–369. [Google Scholar] [CrossRef] [PubMed]
- Olfson, M.; Guardino, M.; Struening, E.; Schneier, F.R.; Hellman, F.; Klein, D.F. Barriers to the treatment of social anxiety. Am. J. Psychiatry 2000, 157, 521–527. [Google Scholar] [CrossRef]
- Griffiths, K.M. Towards a framework for increasing help-seeking for social anxiety disorder. Aust. N. Z. J. Psychiatry 2008, 47, 899–903. [Google Scholar] [CrossRef]
- Vertue, F. From adaptive emotion to dysfunction: An attachment perspective on social anxiety disorder. Personal. Soc. Psychol. Rev. 2003, 7, 170–191. [Google Scholar] [CrossRef]
- Ainsworth, M.D.S. Infancy in Uganda: Infant Care and the Growth of Love; Johns Hopkins University Press: Baltimore, MD, USA, 1967. [Google Scholar]
- Bowlby, J. A Secure Base: Clinical Applications of Attachment Theory; Routledge: London, UK, 1988. [Google Scholar]
- Mikulincer, M.; Shaver, P.R. Attachment in Adulthood: Structure, Dynamics, and Change; Guilford Press: New York, NY, USA, 2007. [Google Scholar]
- Ainsworth, M.D.S.; Blehar, M.C.; Waters, E.; Wall, S. Patterns of Attachment: A Psychological Study of the Strange Situation; Erlbaum: Hillsdale, NJ, USA, 1978. [Google Scholar]
- Brennan, K.A.; Clark, C.L.; Shaver, P.R. Self-report measurement of adult attachment: An integrative overview. In Attachment Theory and Close Relationships; The Guilford Press: New York, NY, USA, 1998. [Google Scholar]
- Zheng, L.; Luo, Y.; Chen, X. Different effects of attachment anxiety and attachment avoidance on depressive symptoms: A meta-analysis. J. Soc. Pers. Relatsh. 2020, 37, 3028–3050. [Google Scholar] [CrossRef]
- Ein-Dor, T.; Doron, G. Psychopathology and attachment. In Attachment Theory and Research: New Directions and Emerging Themes; Simpson, J.A., Rholes, W.S., Eds.; Guilford Press: New York, NY, USA, 2015; pp. 346–373. [Google Scholar]
- Aderka, I.M.; Weisman, O.; Shahar, G.; Gilboa-Schechtman, E. The roles of the social rank and attachment systems in social anxiety. Personal. Individ. Differ. 2009, 47, 284–288. [Google Scholar] [CrossRef]
- Manes, S.; Nodop, S.; Altmann, U.; Gawlytta, R.; Dinger, U.; Dymel, W.; Ehrenthal, J.C.; Joraschky, P.; Nolting, B.; Petrowski, K. Social anxiety as a potential mediator of the association between attachment and depression. J. Affect. Disord. 2016, 205, 264–268. [Google Scholar] [CrossRef]
- Michail, M.; Birchwood, M. Social anxiety in first-episode psychosis: The role of childhood trauma and adult attachment. J. Affect. Disord. 2014, 163, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Gajwani, R.; Patterson, P.; Birchwood, M. Attachment: Developmental pathways to affective dysregulation in young people at ultra-high risk of developing psychosis. Br. J. Clin. Psychol. 2013, 52, 424–437. [Google Scholar] [CrossRef] [PubMed]
- Mikulincer, M.; Gillath, O.; Halevy, V.; Avihou, N.; Avidan, S.; Eshkoli, N. Attachment theory and rections to others’ needs: Evidence that activiation of the sense of attachment security promotes empathic responses. J. Personal. Soc. Psychol. 2001, 81, 1205–1224. [Google Scholar] [CrossRef]
- Mikulincer, M.; Shaver, P.R. Boosting attachment security to promote mental health, prosocial values, and inter-group tolerance. Psychol. Inq. 2007, 18, 139–156. [Google Scholar] [CrossRef]
- Lahat, E.; Mikulincer, M.; Lifshin, U.; Shaver, P.R. Mothers never retire: Contextual priming of working models of mother affects adults’ representations of self and romantic partners. J. Personal. 2020, 88, 501–514. [Google Scholar] [CrossRef]
- Boag, E.M.; Carnelley, K.B. Attachment and prejudice: The mediating role of empathy. Br. J. Soc. Psychol. 2016, 55, 337–356. [Google Scholar] [CrossRef]
- Troyer, D.; Greitemeyer, T. The impact of attachment orientations on empathy in adults: Considering the mediating role of emotion regulation strategies and negative affectivity. Personal. Individ. Differ. 2018, 122, 198–205. [Google Scholar] [CrossRef]
- Bucci, S.; Roberts, N.H.; Danquah, A.N.; Berry, K. Using attachment theory to inform the design and delivery of mental health services: A systematic review of the literature. Psychol. Psychother. Theory Res. Pract. 2015, 88, 1–20. [Google Scholar] [CrossRef]
- Carnelley, K.B.; Otway, L.J.; Rowe, A.C. The effects of attachment priming on depressed and anxious mood. Clin. Psychol. Sci. 2015, 4, 433–450. [Google Scholar] [CrossRef]
- Carnelley, K.B.; Bejinaru, M.M.; Otway, L.; Baldwin, D.S.; Rowe, A.C. Effects of repeated attachment security priming in outpatients with primary depressive disorders. J. Affect. Disord. 2018, 234, 201–206. [Google Scholar] [CrossRef]
- Rapee, R.M.; Heimberg, R.G. A cognitive-behavioral model of anxiety in social phobia. Behav. Res. Ther. 1997, 35, 741–756. [Google Scholar] [CrossRef] [PubMed]
- Dong, X.; Gao, C.; Guo, C.; Li, W.; Cui, L. Time course of attention bias in social anxiety: The effects of spatial frequencies and individual threats. Psychophysiology 2020, 57, e13617. [Google Scholar] [CrossRef] [PubMed]
- Staugaard, S.R.; Rosenberg, N.K. Processing of emotional faces in social phobia. Ment. Illn. 2011, 3, 14–20. [Google Scholar] [CrossRef]
- Wong, Q.J.; Rapee, R.M. The aetiology and maintenance of social anxiety disorder: A synthesis of complementary theoretical models and formulation of a new integrated model. J. Affect. Disord. 2016, 203, 84–100. [Google Scholar] [CrossRef] [PubMed]
- Mogg, K.; Philippot, P.; Bradley, B.P. Selective attention to angry faces in clinical social phobia. J. Abnorm. Psychol. 2004, 113, 160–165. [Google Scholar] [CrossRef] [PubMed]
- Pishyar, R.; Harris, L.M.; Menzies, R.G. Attention bias for words and faces in social anxiety. Anxiety Stress Coping 2004, 17, 23–36. [Google Scholar] [CrossRef]
- Byrow, Y.; Peters, L. The influence of attention biases and adult attachment style on treatment outcome for adults with social anxiety disorder. J. Affect. Disord. 2017, 217, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Davis, M.L.; Rosenfield, D.; Bernstein, A.; Zvielli, A.; Reinecke, A.; Beevers, C.G.; Koster, E.H.; Smits, J.A. Attention bias dynamics and symptom severity during and following CBT for social anxiety disorder. J. Consult. Clin. Psychol. 2016, 84, 795–802. [Google Scholar] [CrossRef]
- Gillath, O.; Selcuk, E.; Shaver, P.R. Moving toward a secure attachment style: Can repeated security priming help? Soc. Personal. Psychol. Compass 2008, 2, 1651–1666. [Google Scholar] [CrossRef]
- Leary, M.R.; Kowalski, R.M. The interaction anxiousness scale: Construct and criterion-related validity. J. Personal. Assess. 1993, 61, 136–146. [Google Scholar] [CrossRef]
- Wang, J.; Chen, J.Z. The Chinese Version of the Experiences in Close Relationship Scale (ECR)-Short Form: Reliability, Validity. Sci. Soc. Psychol. 2013, 28, 106–111. [Google Scholar]
- Peng, C.Z.; Gong, Y.X.; Zhu, X.Z. The Adaptation of Interaction Anxiousness Scale in Chinese Undergraduate Students. Chin. Ment. Health J. 2004, 18, 39–41. [Google Scholar]
- Fredrickson, B.L.; Cohn, M.A.; Coffey, K.A.; Pek, J.; Finkel, S.M. Open hearts build lives: Positive emotions, induced through loving-kindness meditation, build consequential personal resources. J. Personal. Soc. Psychol. 2008, 95, 1045. [Google Scholar] [CrossRef] [PubMed]
- Mikulincer, M.; Shaver, P.R. Attachment theory and intergroup bias: Evidence that priming the secure base schema attenuates negative reactions to out-groups. J. Personal. Soc. Psychol. 2001, 81, 97–115. [Google Scholar] [CrossRef]
- Hudson, N.W.; Fraley, R.C. Moving toward greater security: The effects of repeatedly priming attachment security and anxiety. J. Res. Personal. 2018, 74, 147–157. [Google Scholar] [CrossRef]
- Wang, Y.; Luo, Y.J. Standardization and Assessment of College Students’ Facial Expression of Emotion. Chin. J. Clin. Psychol. 2005, 13, 396–398. [Google Scholar]
- Posner, M.I. Orienting of attention. Q. J. Exp. Psychol. 1980, 32, 3–25. [Google Scholar] [CrossRef]
- Yiend, J.; Mathews, A.; Burns, T.; Dutton, K.; Fernández-Martín, A.; Georgiou, G.A.; Luckie, M.; Rose, A.; Russo, R.; Fox, E. Mechanisms of selective attention in generalized anxiety disorder. Clin. Psychol. Sci. 2015, 3, 758–771. [Google Scholar] [CrossRef]
- Carnelley, K.B.; Rowe, A.C. Repeated priming of attachment security influences later views of self and relationships. Pers. Relatsh. 2007, 14, 307–320. [Google Scholar] [CrossRef]
- Wilkinson, L.L.; Rowe, A.C.; Heath, G.H. Eating me up inside: Priming attachment security and anxiety, and their effects on snacking. J. Soc. Pers. Relatsh. 2013, 30, 795–804. [Google Scholar] [CrossRef]
- McGuire, A.; Gillath, O.; Jackson, Y.; Ingram, R. Attachment security priming as a potential intervention for depressive symptoms. J. Soc. Clin. Psychol. 2018, 37, 44–68. [Google Scholar] [CrossRef]
- Wieser, M.J.; Hambach, A.; Weymar, M. Neurophysiological correlates of attention bias for emotional faces in socially anxious individuals–Evidence from a visual search task and N2pc. Biol. Psychol. 2018, 132, 192–201. [Google Scholar] [CrossRef] [PubMed]
- Wells, A.; Clark, D.M.; Salkovskis, P.; Ludgate, J.; Hackmann, A.; Gelder, M. Social phobia: The role of in-situation safety behaviors in maintaining anxiety and negative beliefs. Behav. Ther. 1995, 26, 153–161. [Google Scholar] [CrossRef]
- Boettcher, J.; Leek, L.; Matson, L.; Holmes, E.A.; Browning, M.; MacLeod, C.; Andersson, G.; Carlbring, P. Internet-based attention bias modification for social anxiety: A randomised controlled comparison of training towards negative and training towards positive cues. PLoS ONE 2013, 8, e71760. [Google Scholar] [CrossRef] [PubMed]
- McNally, R.J.; Enock, P.M.; Tsai, C.; Tousian, M. Attention bias modification for reducing speech anxiety. Behav. Res. Ther. 2013, 51, 882–888. [Google Scholar] [CrossRef]
- Haller, S.P.; Cohen Kadosh, K.; Lau, J. A developmental angle to understanding the mechanisms of biased cognitions in social anxiety. Front. Hum. Neurosci. 2014, 7, 846. [Google Scholar] [CrossRef]
- Waters, A.M.; Mogg, K.; Bradley, B.P. Direction of threat attention bias predicts treatment outcome in anxious children receiving cognitive-behavioural therapy. Behav. Res. Ther. 2012, 50, 428–434. [Google Scholar] [CrossRef]
- Heeren, A.; Mogoase, C.; Philippot, P.; McNally, R.J. Attention bias modification for social anxiety: A systematic review and meta-analysis. Clin. Psychol. Rev. 2015, 40, 76–90. [Google Scholar] [CrossRef]
- Rietdijk, J.; Ising, H.K.; Dragt, S.; Klaassen, R.; Nieman, D.; Wunderink, L.; Cuijpers, P.; Linszen, D.; van der Gaag, M. Depression and social anxiety in help-seeking patients with an ultra-high risk for developing psychosis. Psychiatry Res. 2013, 209, 309–313. [Google Scholar] [CrossRef]
- Charles-Sire, V.; Guéguen, N.; Pascual, A.; Meineri, S. Words as environmental cues: The effect of the word “loving” on compliance to a blood donation request. J. Psychol. 2012, 146, 455–470. [Google Scholar] [CrossRef]
- Gros, D.F.; Simms, L.J.; Antony, M.M.; McCabe, R.E. Development and psychometric evaluation of the Multidimensional Assessment of Social Anxiety (MASA). J. Clin. Psychol. 2012, 68, 432–447. [Google Scholar] [CrossRef] [PubMed]
- Meynadasy, M.; Clancy, K.; Ke, Z.; Simon, J.; Wu, W.; Li, W. Impaired early visual categorization of fear in social anxiety. Psychophysiology 2020, 57, e13509. [Google Scholar] [CrossRef] [PubMed]
- Iacobucci, D.; Posavac, S.S.; Kardes, F.R.; Schneider, M.J.; Popovich, D.L. The median split: Robust, refined, and revived. J. Consum. Psychol. 2015, 25, 690–704. [Google Scholar] [CrossRef]
- Gillath, O.; Karantzas, G. Attachment security priming: A systematic review. Curr. Opin. Psychol. 2019, 25, 86–95. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Priming Group (n = 30) | Control Group (n = 26) | T | p | |||
|---|---|---|---|---|---|---|
| M | SD | M | SD | |||
| Age | 22.10 | 4.33 | 21.73 | 2.34 | 0.388 | 0.699 |
| Pre-IAS | 47.03 | 9.26 | 45.34 | 7.60 | 1.704 | 0.094 |
| ECR-AV | 35.0 | 10.0 | 31.0 | 9.3 | 1.552 | 0.127 |
| ECR-AN | 29.2 | 11.0 | 31.0 | 8.0 | −0.693 | 0.491 |
| Time | Cue Validity | Cue Emotion | Priming Group (n = 30) | Control Group (n = 26) | ||
|---|---|---|---|---|---|---|
| M | SD | M | SD | |||
| Pre-test | Valid | Happy | 564.63 | 104.82 | 569.00 | 92.27 |
| Neutral | 568.07 | 100.55 | 569.46 | 101.52 | ||
| Disgust | 565.80 | 110.93 | 565.62 | 83.94 | ||
| Invalid | Happy | 553.07 | 93.00 | 554.51 | 105.35 | |
| Neutral | 543.23 | 98.52 | 552.68 | 84.10 | ||
| Disgust | 546.52 | 98.07 | 557.27 | 87.25 | ||
| Post-test | Valid | Happy | 538.37 | 112.19 | 527.67 | 79.10 |
| Neutral | 538.97 | 125.51 | 548.85 | 88.28 | ||
| Disgust | 534.17 | 113.43 | 537.88 | 89.22 | ||
| Invalid | Happy | 525.03 | 108.48 | 523.94 | 89.89 | |
| Neutral | 512.61 | 95.06 | 535.54 | 84.96 | ||
| Disgust | 514.76 | 116.58 | 525.07 | 104.96 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, S.; Tao, Y.; Chen, Y.; Zhang, P.; Liu, X. The Effects of Repeated Attachment Security Priming on Social Anxiety and Attention Bias: A Randomized Controlled Trial. Behav. Sci. 2023, 13, 420. https://doi.org/10.3390/bs13050420
Zhang S, Tao Y, Chen Y, Zhang P, Liu X. The Effects of Repeated Attachment Security Priming on Social Anxiety and Attention Bias: A Randomized Controlled Trial. Behavioral Sciences. 2023; 13(5):420. https://doi.org/10.3390/bs13050420
Chicago/Turabian StyleZhang, Shuang, Yanqiang Tao, Yunxiang Chen, Peng Zhang, and Xiangping Liu. 2023. "The Effects of Repeated Attachment Security Priming on Social Anxiety and Attention Bias: A Randomized Controlled Trial" Behavioral Sciences 13, no. 5: 420. https://doi.org/10.3390/bs13050420