
Suicidal Attempts among Secondary School-Going Adolescents in Kilimanjaro Region, Northern Tanzania
 and
and
Abstract
:1. Introduction
2. Methodology
2.1. Study Design and Settings
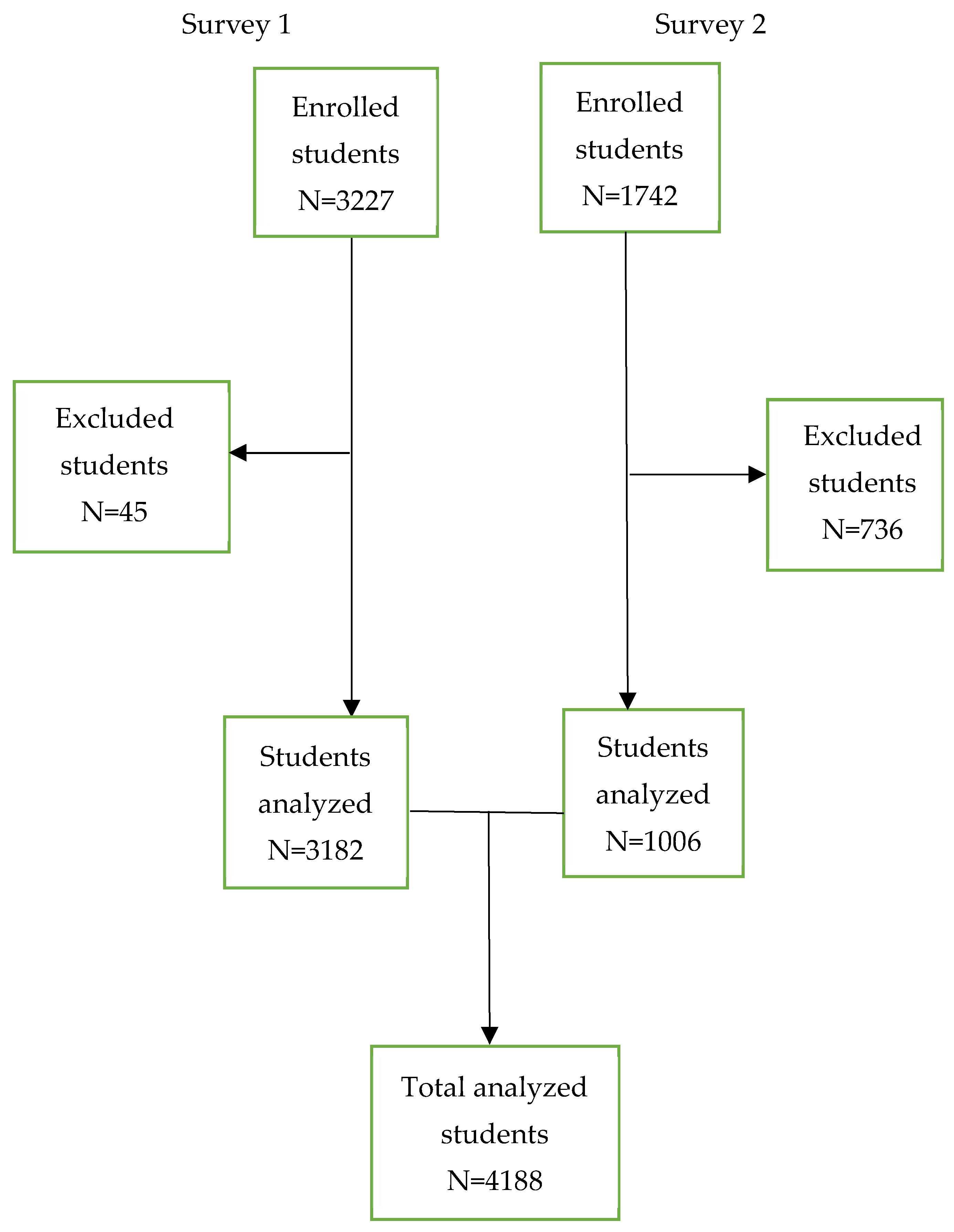
2.2. Study Population and Sampling
2.3. Data Collection
2.4. Instrument Measures
2.5. Statistical Analysis
3. Results
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Suicide; World Health Organization: Geneva, Switzerland, 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/suicide (accessed on 1 September 2022).
- World Health Organization. Suicide in the World: Global Health Estimates. 2019. Available online: https://apps.who.int/iris/handle/10665/326948 (accessed on 1 September 2022).
- UNICEF. Invest More in Mental Health. 2021. Available online: https://www.unicef.org/montenegro/en/stories/unicef-invest-more-mental-health (accessed on 17 March 2023).
- McKinnon, B.; Gariépy, G.; Sentenac, M.; Elgar, F.J. Adolescent suicidal behaviors in 32 low- and middle-income countries. Bull. World Health Organ. 2016, 94, 340–350F. [Google Scholar] [CrossRef] [PubMed]
- McLoughlin, A.B.; Gould, M.S.; Malone, K.M. Global trends in teenage suicide: 2003–2014. QJM 2015, 108, 765–780. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Preventing suicide. CMAJ 2014, 143, 609–610. [Google Scholar]
- Haagsma, J.A.; Graetz, N.; Bolliger, I.; Naghavi, M.; Higashi, H.; Mullany, E.C. The global burden of injury: Incidence, mortality, disability-adjusted life years and time trends from the Global Burden of Disease study 2013. INJ Prev. 2015, 22, 3–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pengpid, S.; Peltzer, K. Prevalence and correlates of past 12-month suicide attempt among in-school adolescents in Guatemala. Psychol. Res. Behav. Manag. 2019, 12, 523–529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cluver, L.; Orkin, M.; Boyes, M.E.; Sherr, L. Child and adolescent suicide attempts, suicidal behavior, and adverse childhood experiences in South Africa: A prospective study. J. Adolesc. Health 2015, 57, 52–59. [Google Scholar] [CrossRef]
- Shaikh, M.A.; Lloyd, J.; Acquah, E.; Celedonia, K.L.; Wilson, M.L. Suicide attempts and behavioral correlates among a nationally representative sample of school-attending adolescents in the Republic of Malawi. BMC Public Health 2016, 16, 843. [Google Scholar] [CrossRef] [Green Version]
- Shayo, F.K.; Lawala, P.S. Does bullying predict suicidal behaviors among in-school adolescents? A cross-sectional finding from Tanzania as an example of a low-income country. BMC Psychiatry 2009, 19, 400. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.; Nkomola, P.; Xue, Q.; Lin, X.; Xie, X.; Hou, F. Health Risk Behaviors and Suicide Attempt among Adolescents in China and Tanzania: A school-based study of countries along the Belt and Road. Child. Youth Serv. Rev. 2020, 118, 105335. [Google Scholar] [CrossRef]
- Nyandindi, U.S. Tanzania Global School-Based Student Health Survey Report; WHO Document; The United Republic of Tanzania, Ministry of Health and Social Welfare: Dodoma, Tanzania, 2017. [Google Scholar]
- Nyundo, A.; Manu, A.; Regan, M.; Ismail, A.; Chukwu, A.; Dessie, Y. Factors associated with depressive symptoms and suicidal ideation and behaviors amongst sub-Saharan African adolescents aged 10-19 years: Cross-sectional study. Trop. Med. Int. Health 2020, 25, 54–69. [Google Scholar] [CrossRef]
- Campisi, S.C.; Carducci, B.; Akseer, N.; Zasowski, C.; Szatmari, P.; Bhutta, Z.A. Suicidal behaviors among adolescents from 90 countries: A pooled analysis of the global school-based student health survey. BMC Public Health 2020, 20, 1102. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Preventing Suicide: LIVE LIFE Implementation; World Health Organization: Geneva, Switzerland, 2022. Available online: https://www.who.int/publications/i/item/WHO-MSD-UNC-MHE-22.02 (accessed on 1 September 2022).
- Pengpid, S.; Peltzer, K. Single and multiple suicide attempts: Prevalence and correlates in school-going adolescents in Jamaica in 2017. Int. J. Disabil. Hum. Dev. 2020, 19, 659–665. [Google Scholar]
- National Bureau of Statistics (NBS). The 2022 Population and Housing Census, Preliminary Report, Tanzania; National Bureau of Statistics (NBS): Dodoma, Tanzania, 2022.
- MOEST. Tanzania Mainland Education Sector Performance Report (2018/2019), Tanzania; MOEST: Dodoma, Tanzania, 2019. [Google Scholar]
- Mavura, R.A.; Nyaki, A.Y.; Leyaro, B.J.; Mamseri, R.; George, J.; Ngocho, J.S. Prevalence of substance use and associated factors among secondary school adolescents in Kilimanjaro region, northern Tanzania. PLoS ONE 2022, 17, e0274102. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Adolescent and Young Adult Health; World Health Organization: Geneva, Switzerland, 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/adolescents-health-risks-and-solutions (accessed on 5 September 2022).
- MoHCDGEC. Tanzania Mainland Global School-Based Student Health Survey Country Report, Tanzania; MoHCDGEC: Dodoma, Tanzania, 2017. [Google Scholar]
- WHO. GSHS Questionnaire; World Health Organization: Geneva, Switzerland, 2021. Available online: https://www.who.int/teams/noncommunicable-diseases/surveillance/systems-tools/global-school-based-student-health-survey/questionnaire (accessed on 21 November 2022).
- Wasserman, D.; Carli, V.; Losue, M.; Javed, A.; Herrmann, H. Suicide prevention in childhood and adolescence: A narrative review of current knowledge on risk and protective factors and effectiveness of interventions. Asian Psychiatry 2021, 13, e12452. [Google Scholar] [CrossRef]
- Makoye, K. Suicide Rates Rise Sharply in Tanzania Amid Economic, Social Woes. 2021. Available online: https://www.aa.com.tr/en/africa/suicide-rates-rise-sharply-in-tanzania-amid-economic-social-woes/2360130# (accessed on 13 December 2022).
- Dunlavy, A.C.; Aquah, E.O.; Wilson, M.L. Suicidal ideation among school-attending adolescents in Dar es Salaam, Tanzania. Tanzan. J. Health Res 2015, 17, 1–9. Available online: https://www.ajol.info/index.php/thrb/article/view/102996 (accessed on 13 December 2022).
- Liu, X.; Huang, Y.; Liu, Y. Prevalence, distribution, and associated factors of suicide attempts in young adolescents: School-based data from 40 low-income and middle-income countries. PLoS ONE 2018, 13, e0207823. [Google Scholar] [CrossRef] [Green Version]
- Darré, T.; Consuela, K.C.; Saka, B.; Djiwa, T.; Ekouévi, K.D.; Napo-Koura, G. Suicidal ideation and suicide attempts in subjects aged 15-19 in Lomé (Togo). BMC Res. Notes 2019, 12, 187. [Google Scholar] [CrossRef]
- Balzer, B.W.R.; Duke, S.A.; Hawke, C.I.; Steinbeck, K.S. The effects of estradiol on mood and behavior in human female adolescents: A systematic review. Eur. J. Pediatr. 2015, 174, 289–298. [Google Scholar] [CrossRef] [Green Version]
- Pandey, A.R.; Bista, B.; Dhungana, R.R. Factors associated with suicidal ideation and suicidal attempts among adolescent students in Nepal: Findings from Global School-based Students Health Survey. PLoS ONE 2019, 14, e0210383. [Google Scholar] [CrossRef] [Green Version]
- Aboagye, R.G.; Ahinkorah, B.O.; Seidu, A.A.; Okyere, J.; Frimpong, J.B. In-school adolescents’ loneliness, social support, and suicidal ideation in sub-Saharan Africa: Leveraging Global School Health data to advance mental health focus in the region. PLoS ONE 2022, 17, e0275660. [Google Scholar] [CrossRef]
- Erzen, E.; Çikrikci, Ö. The effect of loneliness on depression: A meta-analysis. Int. J. Soc. Psychiatry 2018, 64, 427–435. [Google Scholar] [CrossRef] [PubMed]
- Badarch, J.; Chuluunbaatar, B.; Batbaatar, S.; Paulik, E. Suicide Attempts among School-Attending Adolescents in Mongolia: Associated Factors and Gender Differences. Int. J. Environ. Res. Public Health 2022, 19, 2991. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.J.; Yu, Y.; Wilcox, H.C.; Kang, C.; Wang, K.; Wang, C.; Wu, Y.; Chen, R. Global risks of suicidal behaviors and being bullied and their association in adolescents: School-based health survey in 83 countries. EClinicalMedicine 2020, 19, 100253. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variables | Overall n (%) | Survey 1 n (%) | Survey 2 n (%) | p-Value |
|---|---|---|---|---|
| Age (years) | <0.001 | |||
| 13–15 | 2733 (65.3) | 2692 (84.6) | 41 (4.1) | |
| 16–17 | 1455 (34.7) | 490 (15.4) | 965 (95.9) | |
| Median (IQR), Mean (SD) | 15 (14, 16) | 14 (1.0) | 17 (16, 17) | |
| Sex | <0.001 | |||
| Male | 1848 (44.1) | 1494 (47.0) | 354 (35.2) | |
| Female | 2340 (55.9) | 1688 (53.0) | 652 (64.8) | |
| Schooling district * | <0.001 | |||
| Moshi municipality | 933 (22.5) | 662 (20.8) | 271 (28.0) | |
| Moshi district council | 1658 (40.0) | 1324 (41.6) | 334 (34.5) | |
| Hai district council | 646 (15.6) | 523 (16.4) | 123 (12.7) | |
| Siha district council | 912 (22.0) | 673 (21.2) | 239 (24.7) | |
| Ever been worried * | <0.001 | |||
| No | 3638 (88.9) | 2795 (90.6) | 843 (84.0) | |
| Yes | 452 (11.1) | 291 (9.4) | 161 (16.0) | |
| Ever been lonely | <0.001 | |||
| No | 3860 (92.2) | 2966 (93.2) | 894 (88.9) | |
| Yes | 328 (7.8) | 216 (6.8) | 112 (11.1) | |
| Current substances use * † | <0.001 | |||
| No | 566 (50.2) | 250 (37.9) | 316 (67.5) | |
| Yes | 561 (49.8) | 409 (62.1) | 152 (32.5) | |
| Ever had sex * | 0.399 | |||
| No | 3784 (90.5) | 2886 (90.7) | 898 (89.8) | |
| Yes | 398 (9.5) | 296 (9.3) | 102 (10.2) | |
| Ever missed class * | <0.001 | |||
| No | 3277 (78.5) | 2571 (80.9) | 703 (70.9) | |
| Yes | 896 (21.5) | 607 (19.1) | 289 (29.1) | |
| Number of close friends * | 0.290 | |||
| No friends | 363 (8.7) | 285 (9.0) | 78 (7.9) | |
| >1 friend | 3798 (91.3) | 2888 (91.0) | 910 (92.1) | |
| Ever been physically attacked * | 0.002 | |||
| No | 3208 (76.8) | 2408 (75.7) | 800 (80.4) | |
| Yes | 968 (23.2) | 773 (24.3) | 195 (19.6) | |
| Ever engaged in a physical fight * | <0.001 | |||
| No | 3363 (80.3) | 2449 (77.0) | 914 (90.9) | |
| Yes | 824 (19.7) | 733 (23.0) | 91 (9.1) | |
| Ever been bullied * | <0.001 | |||
| No | 3688 (88.1) | 2748 (86.4) | 940 (93.7) | |
| Yes | 497 (11.9) | 434 (13.6) | 63 (6.3) | |
| Food insecurity * | <0.001 | |||
| No | 3885 (92.8) | 2924 (91.9) | 961 (95.7) | |
| Yes | 301 (7.2) | 258 (8.1) | 43 (4.3) | |
| Parental engagement * | 0.058 | |||
| No | 2156 (51.6) | 1666 (52.4) | 490 (49.0) | |
| Yes | 2025 (48.4) | 1514 (47.6) | 511 (51.0) | |
| Survey year (Overall) | 4188 | 3182 (76.0) | 1006 (24.0) |
| Variable | Overall n (%) | Survey 1 n (%) | Survey 2 n (%) | p-Value |
|---|---|---|---|---|
| Ever attempted suicide | ||||
| No | 4051 (96.7) | 3087 (97.0) | 964 (95.8) | 0.065 |
| Yes | 137 (3.3) | 95 (3.0) | 42 (4.2) | |
| Ever had suicidal Ideation * | ||||
| No | 3912 (93.5) | 2989 (93.9) | 923 (92.2) | 0.053 |
| Yes | 271 (6.5) | 193 (6.1) | 78 (7.8) | |
| Ever made suicidal Plan * | ||||
| No | 4007 (95.7) | 3055 (96.0) | 952 (94.9) | 0.135 |
| Yes | 178 (4.3) | 127 (4.0) | 51 (5.1) |
| Variables | Overall | Survey 1 | Survey 2 | |||
|---|---|---|---|---|---|---|
| AOR (95% CI) | p-Value | AOR (95% CI) | p-Value | AOR (95% CI) | p-Value | |
| Age (years) | ||||||
| 13–15 | 1 | 1 | 1 | |||
| 16–17 | 1.0 (0.6, 1.7) | 0.924 | 1.6 (0.7, 3.9) | 0.277 | 0.7 (0.1, 8.0) | 0.775 |
| Sex | ||||||
| Male | 1 | 1 | 1 | |||
| Female | 2.8 (1.5, 5.1) | 0.001 | 3.1 (1.5, 6.5) | 0.002 | 2.9 (0.9, 9.3) | 0.078 |
| Ever felt lonely (Yes) | 2.2 (1.1, 4.3) | 0.020 | 2.4 (1.0, 5.7) | 0.055 | 1.9 (0.7, 5.5) | 0.215 |
| Ever been worried (Yes) | 1.9 (1.1, 3.5) | 0.033 | 2.0 (0.9, 4.3) | 0.087 | 2.2 (0.8, 6.1) | 0.112 |
| Current substance use (Yes) | 1.8 (1.0, 3.3) | 0.058 | 1.7 (0.7, 3.7) | 0.230 | 1.8 (0.7, 4.5) | 0.218 |
| Ever had sex (Yes) | 1.5 (0.8, 2.9) | 0.235 | 1.0 (0.4, 2.3) | 0.901 | 3.4 (1.1, 10.7) | 0.037 |
| Ever physically attacked (Yes) | 1.1 (0.6, 1.9) | 0.789 | 0.9 (0.4, 1.8) | 0.708 | 1.6 (0.6, 4.2) | 0.360 |
| Ever engaged in a physical fight (Yes) | 1.2 (0.6, 2.2) | 0.590 | 1.2 (0.6, 2.5) | 0.579 | 1.0 (0.3, 3.4) | 0.955 |
| Ever bullied (Yes) | 2.2 (1.2, 4.1) | 0.016 | 2.1 (1.0, 4.5) | 0.056 | 2.4 (0.8, 7.7) | 0.130 |
| Parental engagement (Yes) | 1.2 (0.7, 2.1) | 0.454 | 1.3 (0.7, 2.6) | 0.451 | 1.2 (0.5, 2.9) | 0.709 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shirima, J.; Mhando, L.; Mavura, R.; Mboya, I.B.; Ngocho, J.S. Suicidal Attempts among Secondary School-Going Adolescents in Kilimanjaro Region, Northern Tanzania. Behav. Sci. 2023, 13, 288. https://doi.org/10.3390/bs13040288
Shirima J, Mhando L, Mavura R, Mboya IB, Ngocho JS. Suicidal Attempts among Secondary School-Going Adolescents in Kilimanjaro Region, Northern Tanzania. Behavioral Sciences. 2023; 13(4):288. https://doi.org/10.3390/bs13040288
Chicago/Turabian StyleShirima, Jackline, Lisbeth Mhando, Rehema Mavura, Innocent B. Mboya, and James S. Ngocho. 2023. "Suicidal Attempts among Secondary School-Going Adolescents in Kilimanjaro Region, Northern Tanzania" Behavioral Sciences 13, no. 4: 288. https://doi.org/10.3390/bs13040288