
With or without the Mask: Age Differences in Perceived Trustworthiness and Health during the COVID-19 Pandemic
 , , , , , , , and
, , , , , , , and
Abstract
:General Overview
1. Study 1—Trustworthiness
1.1. Introduction
1.2. Materials and Methods
1.2.1. Participants
1.2.2. Study Design
1.2.3. Facial Stimuli
1.2.4. Fear of COVID-19 Questionnaire
1.2.5. Lack of Trust Questionnaire
1.2.6. Procedure
1.2.7. Statistical Analyses
1.3. Results
1.4. Discussion
2. Study 2—Health
2.1. Introduction
2.2. Materials and Methods
2.2.1. Procedure
2.2.2. Statistical Analyses
2.3. Results
2.4. Discussion
3. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mahase, E. China Coronavirus: WHO Declares International Emergency as Death Toll Exceeds 200. BMJ 2020, 368, m408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, Y.; Ma, N.; Witt, C.; Rapp, S.; Wild, P.S.; Andreae, M.O.; Pöschl, U.; Su, H. Face Masks Effectively Limit the Probability of SARS-CoV-2 Transmission. Science 2021, 372, 1439–1443. [Google Scholar] [CrossRef] [PubMed]
- Sommerstein, R.; Fux, C.A.; Vuichard-Gysin, D.; Abbas, M.; Marschall, J.; Balmelli, C.; Troillet, N.; Harbarth, S.; Schlegel, M.; Widmer, A.; et al. Risk of SARS-CoV-2 Transmission by Aerosols, the Rational Use of Masks, and Protection of Healthcare Workers from COVID-19. Antimicrob. Resist. Infect. Control 2020, 9, 100. [Google Scholar] [CrossRef]
- Saladino, V.; Algeri, D.; Auriemma, V. The Psychological and Social Impact of COVID-19: New Perspectives of Well-Being. Front. Psychol. 2020, 11, 2550. [Google Scholar] [CrossRef]
- Sukul, P.; Bartels, J.; Fuchs, P.; Trefz, P.; Remy, R.; Rührmund, L.; Kamysek, S.; Schubert, J.K.; Miekisch, W. Effects of COVID-19 Protective Face-Masks and Wearing Durations onto Respiratory-Haemodynamic Physiology and Exhaled Breath Constituents. Eur. Respir. J. 2022, 60, 2200009. [Google Scholar] [CrossRef]
- Litwinowicz, K.; Choroszy, M.; Ornat, M.; Wróbel, A.; Waszczuk, E. Bayesian Network Meta-Analysis of Face Masks’ Impact on Human Physiology. Sci. Rep. 2022, 12, 5823. [Google Scholar] [CrossRef]
- Ginszt, M.; Zieliński, G.; Szkutnik, J.; Wójcicki, M.; Baszczowski, M.; Litko-Rola, M.; Zielińska, D.; Różyło-Kalinowska, I. The Difference in Electromyographic Activity While Wearing a Medical Mask in Women with and without Temporomandibular Disorders. Int. J. Environ. Res. Public Health 2022, 19, 15559. [Google Scholar] [CrossRef]
- Ginszt, M.; Zieliński, G.; Szkutnik, J.; Wójcicki, M.; Baszczowski, M.; Litko-Rola, M.; Rózyło-Kalinowska, I.; Majcher, P. The Effects of Wearing a Medical Mask on the Masticatory and Neck Muscle Activity in Healthy Young Women. J. Clin. Med. 2022, 11, 303. [Google Scholar] [CrossRef]
- Di Crosta, A.; Palumbo, R.; Marchetti, D.; Ceccato, I.; La Malva, P.; Maiella, R.; Cipi, M.; Roma, P.; Mammarella, N.; Verrocchio, M.C.; et al. Individual Differences, Economic Stability, and Fear of Contagion as Risk Factors for PTSD Symptoms in the COVID-19 Emergency. Front. Psychol. 2020, 11, 567367. [Google Scholar] [CrossRef]
- Palumbo, R.; Adams, R.B.; Hess, U.; Kleck, R.E.; Zebrowitz, L. Age and Gender Differences in Facial Attractiveness, but Not Emotion Resemblance, Contribute to Age and Gender Stereotypes. Front. Psychol. 2017, 8, 1704. [Google Scholar] [CrossRef] [Green Version]
- Zebrowitz, L.A.; Franklin, R.G.; Palumbo, R. Ailing Voters Advance Attractive Congressional Candidates. Evol. Psychol. 2015, 13, 147470491501300. [Google Scholar] [CrossRef] [Green Version]
- Koster, E.H.W.; Verschuere, B.; Burssens, B.; Custers, R.; Crombez, G. Attention for Emotional Faces under Restricted Awareness Revisited: Do Emotional Faces Automatically Attract Attention? Emotion 2007, 7, 285–295. [Google Scholar] [CrossRef]
- Ruffman, T.; Henry, J.D.; Livingstone, V.; Phillips, L.H. A Meta-Analytic Review of Emotion Recognition and Aging: Implications for Neuropsychological Models of Aging. Neurosci. Biobehav. Rev. 2008, 32, 863–881. [Google Scholar] [CrossRef]
- Filippini, C.; Di Crosta, A.; Palumbo, R.; Perpetuini, D.; Cardone, D.; Ceccato, I.; Di Domenico, A.; Merla, A. Automated Affective Computing Based on Bio-Signals Analysis and Deep Learning Approach. Sensors 2022, 22, 1789. [Google Scholar] [CrossRef] [PubMed]
- Kamatani, M.; Ito, M.; Miyazaki, Y.; Kawahara, J.I. Effects of Masks Worn to Protect Against COVID-19 on the Perception of Facial Attractiveness. i-Perception 2021, 12, 20416695211027920. [Google Scholar] [CrossRef] [PubMed]
- Olivera-La Rosa, A.; Chuquichambi, E.G.; Ingram, G.P.D. Keep Your (Social) Distance: Pathogen Concerns and Social Perception in the Time of COVID-19. Personal. Individ. Differ. 2020, 166, 110200. [Google Scholar] [CrossRef] [PubMed]
- Cannito, L.; Anzani, S.; Bortolotti, A.; Palumbo, R.; Ceccato, I.; Di Crosta, A.; Di Domenico, A.; Palumbo, R. Temporal Discounting of Money and Face Masks During the COVID-19 Pandemic: The Role of Hoarding Level. Front. Psychol. 2021, 12, 642102. [Google Scholar] [CrossRef] [PubMed]
- Ceccato, I.; Di Crosta, A.; La Malva, P.; Cannito, L.; Mammarella, N.; Palumbo, R.; Palumbo, R.; Di Domenico, A. Public Opinion in Vaccine Allocation Priority: Who Comes First? Psychol. Health 2021, 1–21. [Google Scholar] [CrossRef]
- Colautti, L.; Cancer, A.; Magenes, S.; Antonietti, A.; Iannello, P. Risk-Perception Change Associated with COVID-19 Vaccine’s Side Effects: The Role of Individual Differences. Int. J. Environ. Res. Public Health 2022, 19, 1189. [Google Scholar] [CrossRef]
- Ceccato, I.; Palumbo, R.; Di Crosta, A.; Marchetti, D.; La Malva, P.; Maiella, R.; Marin, A.; Mammarella, N.; Verrocchio, M.C.; Di Domenico, A. “What’s next?” Individual Differences in Expected Repercussions of the COVID-19 Pandemic. Personal. Individ. Differ. 2021, 174, 110674. [Google Scholar] [CrossRef]
- Cannito, L.; Ceccato, I.; Bortolotti, A.; Di Crosta, A.; La Malva, P.; Palumbo, R.; Di Domenico, A.; Palumbo, R. Exploring Vaccine Hesitancy: The Twofold Role of Critical Thinking. Curr. Psychol. 2022, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Ceccato, I.; Di Crosta, A.; Palumbo, R.; Marchetti, D.; La Malva, P.; Maiella, R.; Marin, A.; Mammarella, N.; Verrocchio, M.C.; Di Domenico, A. Data on the Effects of COVID-19 Pandemic on People’s Expectations about Their Future. Data Brief 2021, 35, 106892. [Google Scholar] [CrossRef] [PubMed]
- Biermann, M.; Schulze, A.; Unterseher, F.; Atanasova, K.; Watermann, P.; Krause-Utz, A.; Stahlberg, D.; Bohus, M.; Lis, S. Trustworthiness Appraisals of Faces Wearing a Surgical Mask during the COVID-19 Pandemic in Germany: An Experimental Study. PLoS ONE 2021, 16, e0251393. [Google Scholar] [CrossRef] [PubMed]
- Ceccato, I.; Palumbo, R.; Di Crosta, A.; La Malva, P.; Marchetti, D.; Maiella, R.; Verrocchio, M.C.; Marin, A.; Mammarella, N.; Palumbo, R.; et al. Age-Related Differences in the Perception of COVID-19 Emergency during the Italian Outbreak. Aging Ment. Health 2021, 25, 1305–1313. [Google Scholar] [CrossRef]
- Rosi, A.; van Vugt, F.T.; Lecce, S.; Ceccato, I.; Vallarino, M.; Rapisarda, F.; Vecchi, T.; Cavallini, E. Risk Perception in a Real-World Situation (COVID-19): How It Changes From 18 to 87 Years Old. Front. Psychol. 2021, 12, 646558. [Google Scholar] [CrossRef]
- Cartaud, A.; Quesque, F.; Coello, Y. Wearing a Face Mask against COVID-19 Results in a Reduction of Social Distancing. PLoS ONE 2020, 15, e0243023. [Google Scholar] [CrossRef]
- Zebrowitz, L.A.; Franklin, R.G.; Hillman, S.; Boc, H. Older and Younger Adults’ First Impressions from Faces: Similar in Agreement but Different in Positivity. Psychol. Aging 2013, 28, 202–212. [Google Scholar] [CrossRef] [Green Version]
- Rhodes, M.G.; Anastasi, J.S. The Own-Age Bias in Face Recognition: A Meta-Analytic and Theoretical Review. Psychol. Bull. 2012, 138, 146–174. [Google Scholar] [CrossRef]
- Carstensen, L.L.; Fung, H.H.; Charles, S.T. Socioemotional Selectivity Theory and the Regulation of Emotion in the Second Half of Life. Motiv. Emot. 2003, 27, 103–123. [Google Scholar] [CrossRef]
- Löckenhoff, C.E.; Carstensen, L.L. Socioemotional Selectivity Theory, Aging, and Health: The Increasingly Delicate Balance between Regulating Emotions and Making Tough Choices. J. Pers. 2004, 72, 1395–1424. [Google Scholar] [CrossRef]
- Mammarella, N.; Fairfield, B.; Frisullo, E.; Di Domenico, A. Saying It with a Natural Child’s Voice! When Affective Auditory Manipulations Increase Working Memory in Aging. Aging Ment. Health 2013, 17, 853–862. [Google Scholar] [CrossRef]
- Ceccato, I.; La Malva, P.; Di Crosta, A.; Palumbo, R.; Gatti, M.; Momi, D.; Logrieco, M.G.M.; Fasolo, M.; Mammarella, N.; Borella, E.; et al. “When Did You See It?” The Effect of Emotional Valence on Temporal Source Memory in Aging. Cogn. Emot. 2022, 36, 987–994. [Google Scholar] [CrossRef]
- Di Crosta, A.; Ceccato, I.; Marchetti, D.; Malva, P.L.; Maiella, R.; Cannito, L.; Cipi, M.; Mammarella, N.; Palumbo, R.; Verrocchio, M.C.; et al. Psychological Factors and Consumer Behavior during the COVID-19 Pandemic. PLoS ONE 2021, 16, e0256095. [Google Scholar] [CrossRef] [PubMed]
- Federico, G.; Ferrante, D.; Marcatto, F.; Brandimonte, M.A. How the Fear of COVID-19 Changed the Way We Look at Human Faces. PeerJ 2021, 9, e11380. [Google Scholar] [CrossRef]
- Moye, M.J.; Henkin, A.B.; Egley, R.J. Teacher-principal Relationships: Exploring Linkages between Empowerment and Interpersonal Trust. J. Educ. Adm. 2005, 43, 260–277. [Google Scholar] [CrossRef]
- Sofer, C.; Dotsch, R.; Wigboldus, D.H.J.; Todorov, A. What Is Typical Is Good: The Influence of Face Typicality on Perceived Trustworthiness. Psychol. Sci. 2015, 26, 39–47. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Chen, Z.; Liu, X.; Qi, Y. Perceiving the Facial Trustworthiness: Facial Age, Emotional Expression, and Attractiveness. Q. J. Exp. Psychol. 2022, 75, 818–829. [Google Scholar] [CrossRef] [PubMed]
- Fiske, S.T.; Cuddy, A.J.; Glick, P.; Xu, J. A model of (often mixed) stereotype content: Competence and warmth respectively follow from perceived status and competition. In Social Cognition; Routledge: Oxfordshire, UK, 2018; pp. 162–214. [Google Scholar]
- Bailey, P.E.; Leon, T. A Systematic Review and Meta-Analysis of Age-Related Differences in Trust. Psychol. Aging 2019, 34, 674–685. [Google Scholar] [CrossRef]
- Tokuda, Y.; Jimba, M.; Yanai, H.; Fujii, S.; Inoguchi, T. Interpersonal Trust and Quality-of-Life: A Cross-Sectional Study in Japan. PLoS ONE 2008, 3, e3985. [Google Scholar] [CrossRef] [Green Version]
- Alijanzadeh, M.; Ahorsu, D.K.; Alimoradi, Z.; Mahmoudi, N.; Griffiths, M.D.; Lin, C.-Y.; Liu, H.-K.; Pakpour, A.H. Fear of COVID-19 and Trust in the Healthcare System Mediates the Association between Individual’s Risk Perception and Preventive COVID-19 Behaviours among Iranians. Int. J. Environ. Res. Public Health 2021, 18, 12146. [Google Scholar] [CrossRef]
- Lin, C.-Y.; Alimoradi, Z.; Ehsani, N.; Ohayon, M.M.; Chen, S.-H.; Griffiths, M.D.; Pakpour, A.H. Suicidal Ideation during the COVID-19 Pandemic among A Large-Scale Iranian Sample: The Roles of Generalized Trust, Insomnia, and Fear of COVID-19. Healthcare 2022, 10, 93. [Google Scholar] [CrossRef]
- Marini, M.; Ansani, A.; Paglieri, F.; Caruana, F.; Viola, M. The Impact of Facemasks on Emotion Recognition, Trust Attribution and Re-Identification. Sci. Rep. 2021, 11, 5577. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool for Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Ebner, N.C.; Riediger, M.; Lindenberger, U. FACES—A Database of Facial Expressions in Young, Middle-Aged, and Older Women and Men: Development and Validation. Behav. Res. Methods 2010, 42, 351–362. [Google Scholar] [CrossRef]
- Siegrist, M.; Earle, T.C.; Gutscher, H. Test of a Trust and Confidence Model in the Applied Context of Electromagnetic Field (EMF) Risks. Risk Anal. 2003, 23, 705–716. [Google Scholar] [CrossRef]
- Siegrist, M.; Keller, C.; Kiers, H.A.L. A New Look at the Psychometric Paradigm of Perception of Hazards. Risk Anal. 2005, 25, 211–222. [Google Scholar] [CrossRef] [PubMed]
- Statistics, S. IBM SPSS Statistics for Windows, Version 27.0; IBM Corp: Armonk, NY, USA, 2020. [Google Scholar]
- Fell, L. Trust and COVID-19: Implications for Interpersonal, Workplace, Institutional, and Information-Based Trust. Digit. Gov. Res. Pract. 2020, 2, 10:1–10:5. [Google Scholar] [CrossRef]
- Di Crosta, A.; La Malva, P.; Manna, C.; Marin, A.; Palumbo, R.; Verrocchio, M.C.; Cortini, M.; Mammarella, N.; Di Domenico, A. The Chieti Affective Action Videos Database, a Resource for the Study of Emotions in Psychology. Sci. Data 2020, 7, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- La Malva, P.; Ceccato, I.; Di Crosta, A.; Marin, A.; Fasolo, M.; Palumbo, R.; Mammarella, N.; Palumbo, R.; Di Domenico, A. Updating the Chieti Affective Action Videos Database with Older Adults. Sci. Data 2021, 8, 272. [Google Scholar] [CrossRef]
- Mather, M.; Carstensen, L.L. Aging and Motivated Cognition: The Positivity Effect in Attention and Memory. Trends Cogn. Sci. 2005, 9, 496–502. [Google Scholar] [CrossRef]
- Mather, M.; Knight, M. Goal-Directed Memory: The Role of Cognitive Control in Older Adults’ Emotional Memory. Psychol. Aging 2005, 20, 554–570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mammarella, N.; Gatti, M.; Ceccato, I.; Di Crosta, A.; Di Domenico, A.; Palumbo, R. The Protective Role of Neurogenetic Components in Reducing Stress-Related Effects during Spaceflights: Evidence from the Age-Related Positive Memory Approach. Life 2022, 12, 1176. [Google Scholar] [CrossRef] [PubMed]
- Henderson, A.J.; Holzleitner, I.J.; Talamas, S.N.; Perrett, D.I. Perception of Health from Facial Cues. Philos. Trans. R Soc. Lond. B Biol. Sci. 2016, 371, 20150380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zebrowitz, L.A.; Montepare, J.M. Social Psychological Face Perception: Why Appearance Matters. Soc. Personal. Psychol. Compass 2008, 2, 1497–1517. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Younger Adults (YAs) | Older Adults (OAs) | |||||||
|---|---|---|---|---|---|---|---|---|
| Mask | No-Mask | Pre-COVID | Statistics | Mask | No-Mask | Pre-COVID | Statistics | |
| M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | |||
| Age | 22.40 (4.12) | 21.00 (2.49) | 21.5 (1.70) | F(2,77) = 1.59, p = 0.210 | 73.90 (7.66) | 72.17 (7.41) | 72.30 (6.05) | F(2.77) = 0.51, p = 0.601 |
| Education | 3.03 (0.56) | 3.10 (0.31) | t(58) = −0.58, p = 0.426 | 2.00 (1.02) | 2.37 (1.25) | t(58) = −1.25, p = 0.200 | ||
| Lack of trust | 3.50 (0.63) | 3.40 (0.54) | t(58) = 0.61, p = 0.472 | 3.48 (0.57) | 3.31 (0.83) | t(58) = 0.88, p = 0.077 | ||
| Belief in contagion | 53.33 (21.83) | 59.33 (18.92) | t(58) = −1.14, p = 0.260 | 45.92 (22.90) | 49.93 (21.61) | t(58) = −0.70, p = 0.880 | ||
| Consequences of contagion | 37.62 (17.47) | 42.86 (21.72) | t(58) = −1.03, p = 0.307 | 59.36 (20.56) | 54.44 (24.24) | t(58) = 0.85, p = 0.212 | ||
| Trustworthiness ratings | 4.33 (0.60) | 3.55 (0.58) | 4.22 (0.60) | F(2,77) = 11.91, p < 0.001 | 4.65 (0.83) | 4.16 (0.84) | 4.32 (0.66) | F(2.77) = 2.88, p = 0.063 |
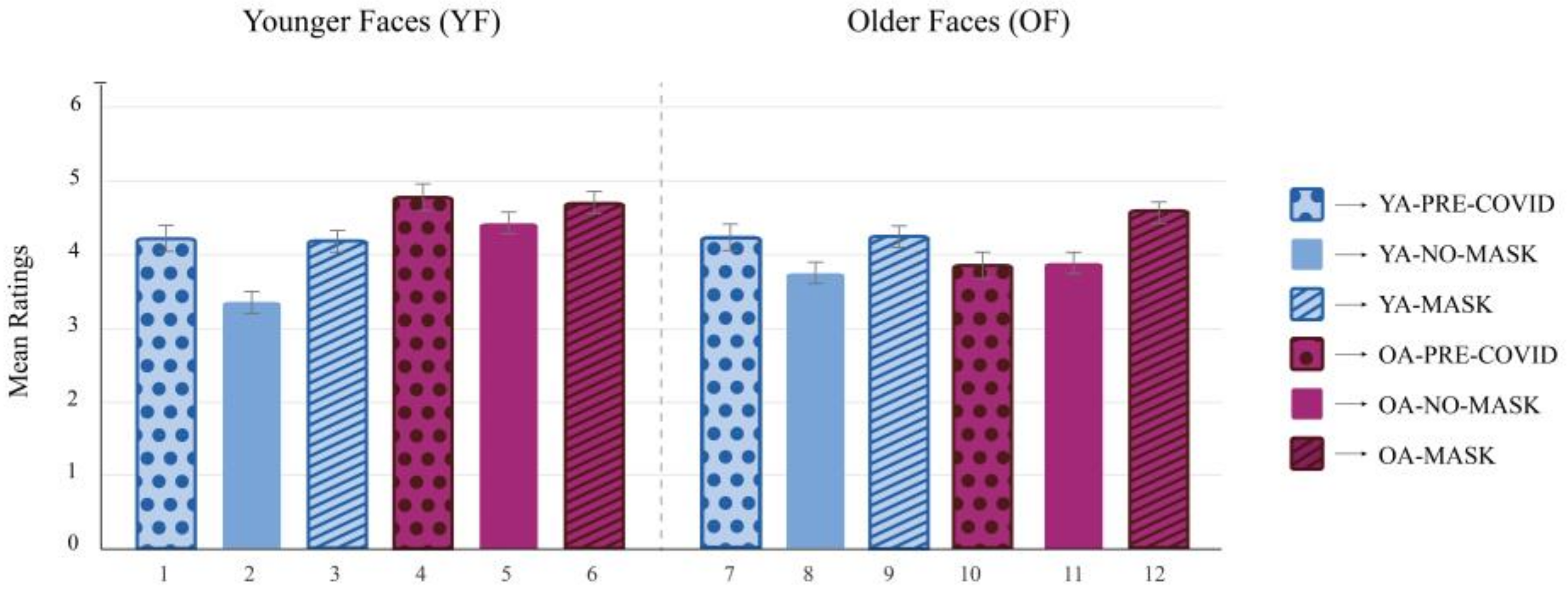
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M (SE) | 4.22 (0.18) | 3.35 (0.15) | 4.19 (0.15) | 4.78 (0.18) | 4.43 (0.15) | 4.70 (0.15) | 4.22 (0.18) | 3.75 (0.15) | 4.25 (0.15) | 3.86 (0.18) | 3.90 (0.15) | 4.60 (0.15) |
| 1 | 0.01 | 0.999 | 0.562 | 0.999 | 0.664 | 0.999 | 0.68 | 0.999 | 0.957 | 0.965 | 0.906 | |
| 2 | 0.003 | <0.001 | <0.001 | <0.001 | 0.011 | 0.197 | 0.001 | 0.576 | 0.267 | <0.001 | ||
| 3 | 0.332 | 0.994 | 0.392 | 0.999 | 0.606 | 0.999 | 0.953 | 0.96 | 0.737 | |||
| 4 | 0.939 | 0.999 | 0.554 | 0.001 | 0.512 | <0.001 | 0.009 | 0.999 | ||||
| 5 | 0.98 | 0.999 | 0.053 | 0.999 | 0.367 | 0.013 | 0.999 | |||||
| 6 | 0.655 | <0.001 | 0.603 | 0.016 | 0.007 | 0.999 | ||||||
| 7 | 0.688 | 0.999 | 0.959 | 0.967 | 0.901 | |||||||
| 8 | 0.396 | 0.999 | 0.999 | 0.003 | ||||||||
| 9 | 0.863 | 0.863 | 0.893 | |||||||||
| 10 | 0.999 | 0.065 | ||||||||||
| 11 | 0.038 |
| Model 1 YAs in the No-Mask Condition Evaluating YFs | Model 2 OAs in the No-Mask Condition Evaluating OFs | |||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Step 1 | Step 2 | Step 3 | Step 1 | Step 2 | Step 3 | |||||||||||||||||||
| B | SE | t | p | B | SE | t | p | B | SE | t | p | B | SE | t | p | B | SE | t | p | B | SE | t | p | |
| Gender | 0.08 | 0.27 | −0.32 | 0.752 | −0.06 | 0.28 | −0.23 | 0.823 | 0.00 | 0.24 | 0.01 | 0.994 | 0.11 | 0.26 | 0.44 | .965 | 0.15 | 0.27 | 0.58 | 0.954 | 0.73 | 0.23 | 0.32 | 0.755 |
| Education | 0.48 | 0.43 | 1.12 | 0.271 | 0.48 | 0.44 | 1.10 | 0.281 | 0.38 | 0.38 | 1.00 | 0.326 | −0.17 | 0.40 | −0.42 | .677 | −0.17 | 0.41 | −0.41 | 0.682 | −0.26 | 0.36 | −0.72 | 0.480 |
| Lack of trust | −0.11 | 0.24 | −0.45 | 0.659 | 0.06 | 0.21 | 0.30 | 0.766 | −0.02 | 0.23 | −0.08 | 0.934 | 0.13 | 0.21 | −0.65 | 0.524 | ||||||||
| Belief in contagion | −0.02 | 0.01 | −3.00 | 0.006 | −0.02 | 0.01 | −2.71 | 0.012 | ||||||||||||||||
| Consequences of contagion | −0.00 | 0.01 | −0.22 | .827 | −0.00 | 0.01 | −0.23 | 0.824 | ||||||||||||||||
| R2 | 0.05 | 0.05 | 0.38 | 0.01 | 0.01 | 0.31 | ||||||||||||||||||
| ΔR2 | 0.05 | 0.01 | 0.37 | 0.01 | 0.00 | 0.30 | ||||||||||||||||||
| F for ΔR2 | 0.63 | 0.20 | 63.19 | 0.09 | 0.01 | 5.19 | ||||||||||||||||||
| p for ΔR2 | 0.539 | 0.659 | 0.006 | 0.914 | 0.934 | 0.013 | ||||||||||||||||||
| Younger Adults (YAs) | Older Adults (OAs) | |||||||
|---|---|---|---|---|---|---|---|---|
| Mask | No-Mask | Pre-COVID | Statistics | Mask | No-Mask | Pre-COVID | Statistics | |
| M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | |||
| Age | 21.83 (3.69) | 22.33 (4.44) | 21.75 (1.83) | F(2,77) = 0.203, p = 0.817 | 72.90 (6.21) | 72.40 (6.53) | 72.30 (6.05) | F(2.77) = 0.513, p = 0.601 |
| Education | 3.17 (0.53) | 3.10 (0.48) | t(58) = −0.510, p = 0.156 | 2.17 (1.26) | 2.13 (1.22) | t(58) = 0.104, p = 0.918 | ||
| Health Status | 4.33 (0.55) | 4.00 (0.95) | t(58) = 1.670, p = 0.037 | 3.60 (0.81) | 3.40 (0.86) | t(58) = 0.928, p = 0.357 | ||
| Belief in contagion | 49.53 (22.70) | 56.17 (19.50) | t(58) = −1.217, p = 0.552 | 43.33 (26.71) | 45.67 (21.92) | t(58) = −0.371, p = 0.712 | ||
| Consequences of contagion | 44.12 (17.73) | 45.29 (16.15) | t(58) = −0.268, p = 0.566 | 59.79 (25.51) | 54.44 (24.24) | t(58) = 0.845, p = 0.212 | ||
| Health ratings | 3.79 (0.43) | 3.63 (0.31) | 4.36 (0.45) | F(2,77) = 21.413, p < 0.001 | 4.51(0.54) | 4.78 (0.58) | 4.73 (0.75) | F(2,77) = 1.564, p < 0.216 |
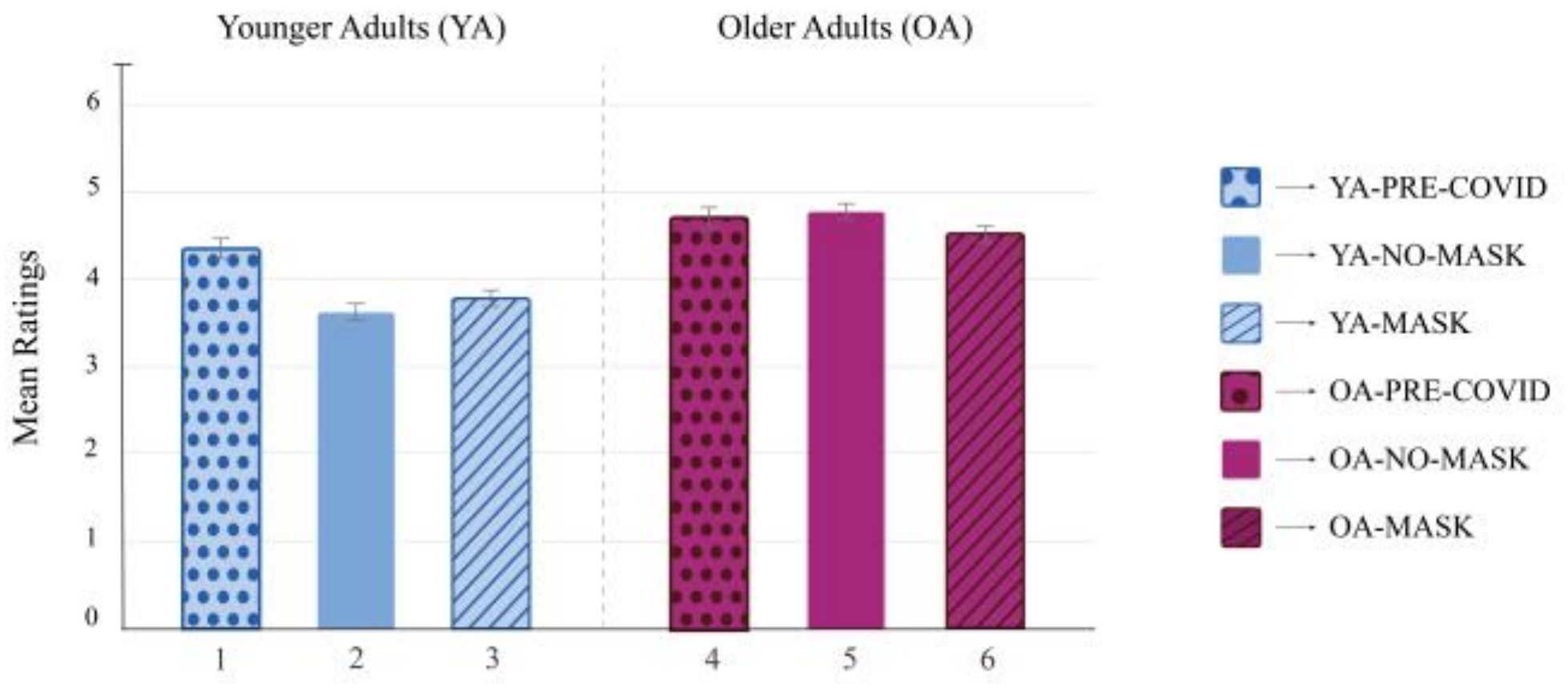
| 1 | 2 | 3 | 4 | 5 | 6 | |
|---|---|---|---|---|---|---|
| M (SE) | 4.36 (0.11) | 3.63 (0.09) | 3,79 (0.09) | 4.73 (0.11) | 4.78 (0.09) | 4.51 (0.09) |
| 1 | <0.001 | 0.002 | 0.198 | 0.051 | 0.901 | |
| 2 | 0.855 | <0.001 | <0.001 | <0.001 | ||
| 3 | <0.001 | <0.001 | <0.001 | |||
| 4 | 0.999 | 0.69 | ||||
| 5 | 0.34 |
| Step 1 | Step 2 | Step 3 | Step 4 | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B | SE | t | p | B | SE | t | p | B | SE | t | p | B | SE | t | p | |
| Gender | −0.14 | 0.1 | −1.397 | 0.165 | −0.137 | 0.101 | −1.365 | 0.175 | −0.136 | 0.101 | −1.353 | 0.179 | −0.087 | 0.094 | −0.93 | 0.354 |
| Age group | 0.019 | 0.002 | 9.324 | <0.001 | 0.019 | 0.002 | 9.311 | <0.001 | 0.018 | 0.002 | 8.698 | <0.001 | 0.017 | 0.002 | 8.612 | <0.001 |
| Education | 0.069 | 0.05 | 1.397 | 0.165 | 0.071 | 0.05 | 1.415 | 0.162 | 0.081 | 0.051 | 1.59 | 0.115 | 0.065 | 0.048 | 1.358 | 0.177 |
| Condition | 0.055 | 0.089 | 0.616 | 0.539 | 0.041 | 0.09 | 0.449 | 0.654 | 0.054 | 0.086 | 0.625 | 0.534 | ||||
| Health status | −0.056 | 0.058 | −0.959 | 0.343 | −0.08 | 0.054 | −1.463 | 0.146 | ||||||||
| Belief in contagion | −0.008 | 0.002 | −4.002 | <0.001 | ||||||||||||
| Consequences of contagion | −0.003 | 0.002 | −1.135 | 0.259 | ||||||||||||
| ΔR2 | 0.493 | 0.002 | 0.004 | 0.081 | ||||||||||||
| F for ΔR2 | 37.61 | 0.38 | 0.92 | 10.78 | ||||||||||||
| p for ΔR2 | <0.001 | 0.539 | 0.340 | <0.001 | ||||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Crosta, A.; Ceccato, I.; Bartolini, E.; La Malva, P.; Gatti, M.; D’Intino, E.; Cannito, L.; Marin, A.; Palumbo, R.; Mammarella, N.; et al. With or without the Mask: Age Differences in Perceived Trustworthiness and Health during the COVID-19 Pandemic. Behav. Sci. 2023, 13, 195. https://doi.org/10.3390/bs13030195
Di Crosta A, Ceccato I, Bartolini E, La Malva P, Gatti M, D’Intino E, Cannito L, Marin A, Palumbo R, Mammarella N, et al. With or without the Mask: Age Differences in Perceived Trustworthiness and Health during the COVID-19 Pandemic. Behavioral Sciences. 2023; 13(3):195. https://doi.org/10.3390/bs13030195
Chicago/Turabian StyleDi Crosta, Adolfo, Irene Ceccato, Emanuela Bartolini, Pasquale La Malva, Matteo Gatti, Eleonora D’Intino, Loreta Cannito, Anna Marin, Riccardo Palumbo, Nicola Mammarella, and et al. 2023. "With or without the Mask: Age Differences in Perceived Trustworthiness and Health during the COVID-19 Pandemic" Behavioral Sciences 13, no. 3: 195. https://doi.org/10.3390/bs13030195