
Gender Disparities after Transcatheter Aortic Valve Replacement with Newer Generation Transcatheter Heart Valves: A Systematic Review and Meta-Analysis

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Inclusion Criteria
- (1)
- Studies that were cohort studies (prospective or retrospective), case–control studies, or randomized controlled trials (RCTs) that reported and compared mortality rates between female and male patients undergoing TAVR with newer generation THVs.
- (2)
- Relative risk (RR), odds ratio (OR), hazard ratio (HR) with 95% confidence intervals (CI), or sufficient raw data to calculate the effect size of mortality rate differences between female and male patients undergoing TAVR with newer generation THVs.
2.3. Data Extraction and Quality Assessment Tool
2.4. Outcomes and Definitions
2.5. Statistical Analysis
3. Results
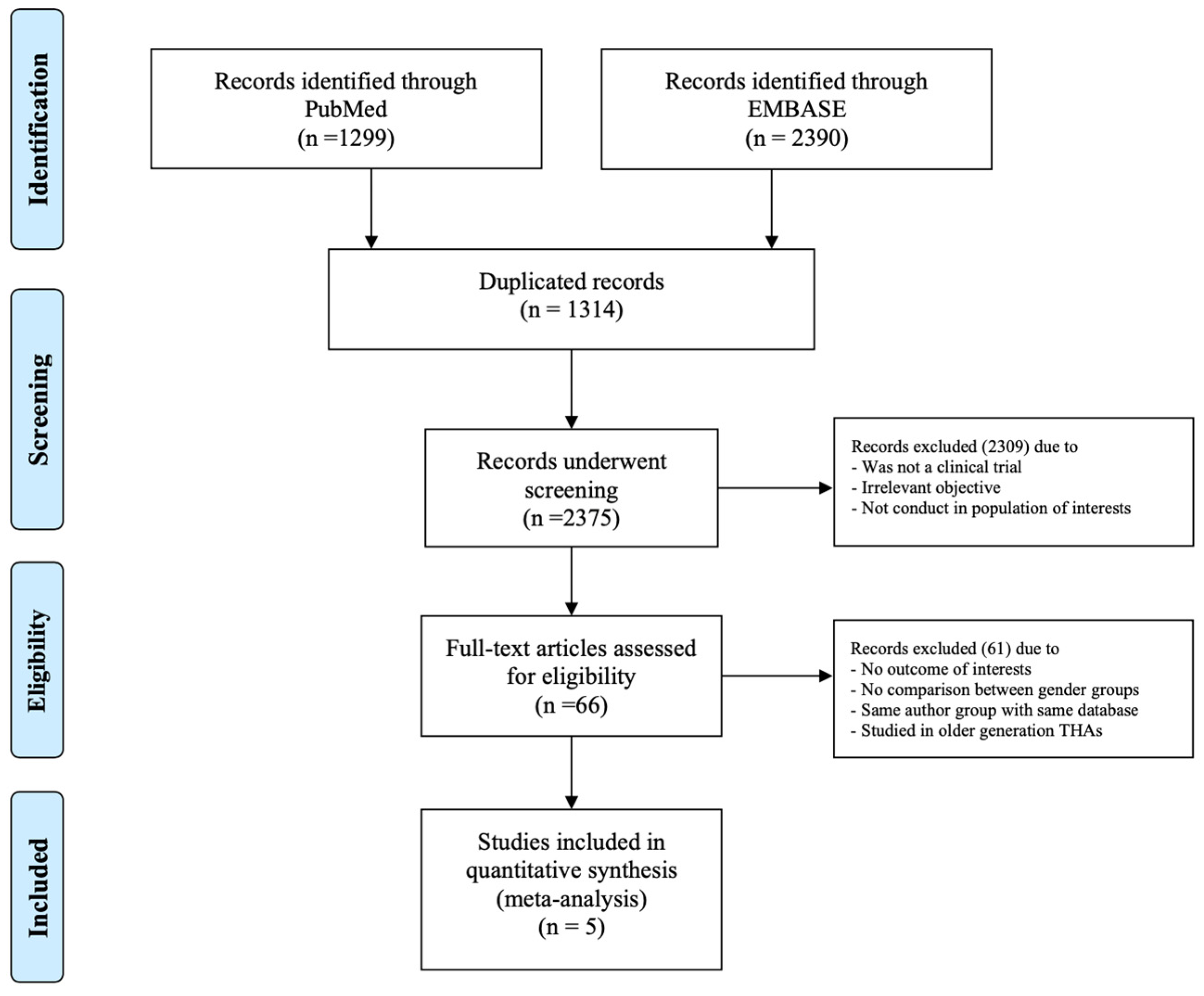
3.1. Literature Search
3.2. Description of Included Studies
3.3. Quality Assessment Tool
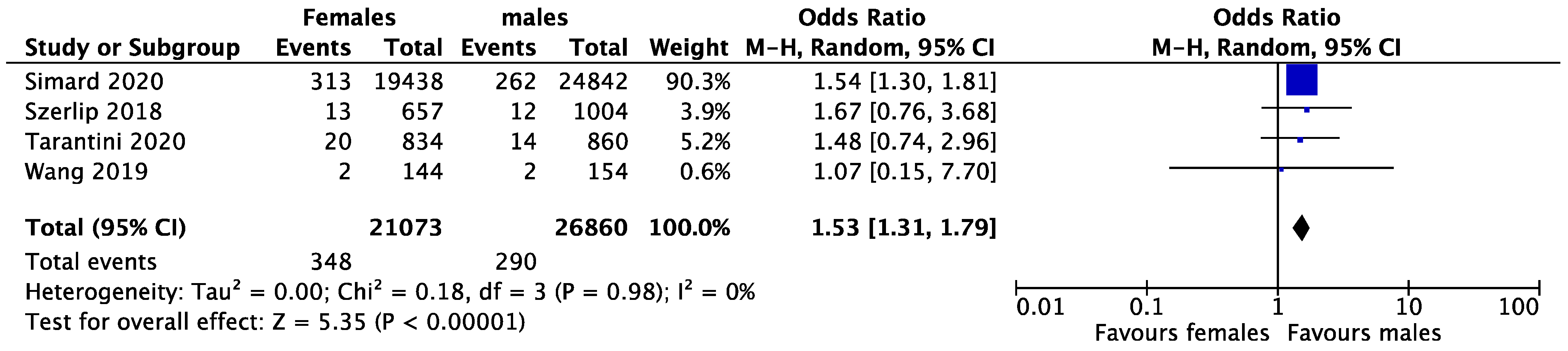
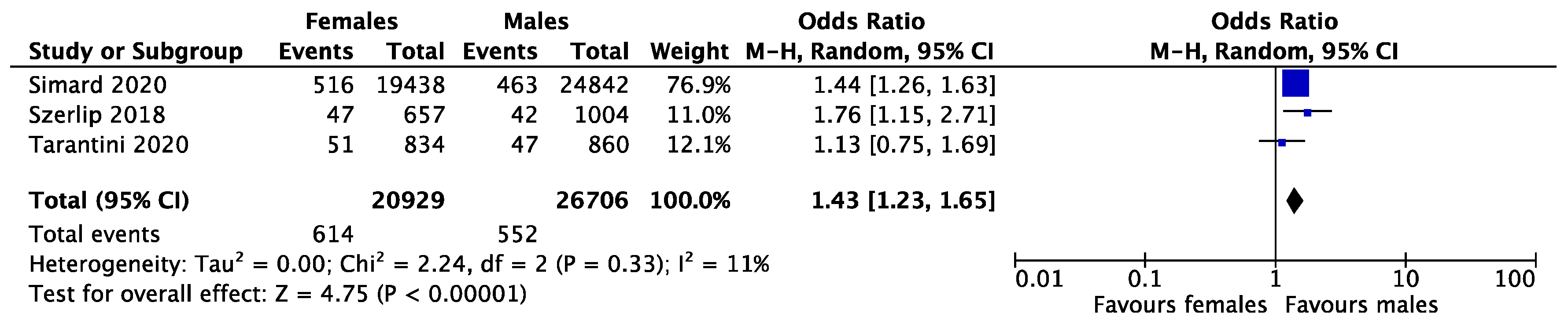
3.4. Meta-Analysis Results
3.4.1. Sensitivity Analysis
3.4.2. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Al-Lamee, R.; Broyd, C.; Parker, J.; Davies, J.E.; Mayet, J.; Sutaria, N.; Ariff, B.; Unsworth, B.; Cousins, J.; Bicknell, C.; et al. Influence of gender on clinical outcomes following transcatheter aortic valve implantation from the UK transcatheter aortic valve implantation registry and the National Institute for Cardiovascular Outcomes Research. Am. J. Cardiol. 2014, 113, 522–528. [Google Scholar] [CrossRef] [PubMed]
- Hayashida, K.; Morice, M.C.; Chevalier, B.; Hovasse, T.; Romano, M.; Garot, P.; Farge, A.; Donzeau-Gouge, P.; Bouvier, E.; Cormier, B.; et al. Sex-related differences in clinical presentation and outcome of transcatheter aortic valve implantation for severe aortic stenosis. J. Am. Coll. Cardiol. 2012, 59, 566–571. [Google Scholar] [CrossRef]
- Katz, M.; Carlos Bacelar Nunes Filho, A.; Caixeta, A.; Antonio Carvalho, L.; Sarmento-Leite, R.; Alves Lemos Neto, P.; Eduardo Koenig São Thiago, L.; Dias Dourado Oliveira, A.; Antonio Marino, M.; Tadeu Tumelero, R.; et al. Gender-related differences on short- and long-term outcomes of patients undergoing transcatheter aortic valve implantation. Catheter. Cardiovasc. Interv. 2017, 89, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Gaglia, M.A., Jr.; Lipinski, M.J.; Torguson, R.; Gai, J.; Ben-Dor, I.; Bernardo, N.L.; Satler, L.F.; Pichard, A.D.; Waksman, R. Comparison in Men Versus Women of Co-morbidities, Complications, and Outcomes After Transcatheter Aortic Valve Implantation for Severe Aortic Stenosis. Am. J. Cardiol. 2016, 118, 1692–1697. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, S.A.; Morice, M.C.; Gilard, M.; Leon, M.B.; Webb, J.G.; Dvir, D.; Rodés-Cabau, J.; Tamburino, C.; Capodanno, D.; D’Ascenzo, F.; et al. Revisiting Sex Equality with Transcatheter Aortic Valve Replacement Outcomes: A Collaborative, Patient-Level Meta-Analysis of 11,310 Patients. J. Am. Coll. Cardiol. 2015, 66, 221–228. [Google Scholar] [CrossRef]
- Saad, M.; Nairooz, R.; Pothineni, N.V.K.; Almomani, A.; Kovelamudi, S.; Sardar, P.; Katz, M.; Abdel-Wahab, M.; Bangalore, S.; Kleiman, N.S.; et al. Long-Term Outcomes with Transcatheter Aortic Valve Replacement in Women Compared With Men: Evidence From a Meta-Analysis. JACC Cardiovasc. Interv. 2018, 11, 24–35. [Google Scholar] [CrossRef]
- Sherwood, M.W.; Xiang, K.; Matsouaka, R.; Li, Z.; Vemulapalli, S.; Vora, A.N.; Fanaroff, A.; Harrison, J.K.; Thourani, V.H.; Holmes, D.; et al. Incidence, Temporal Trends, and Associated Outcomes of Vascular and Bleeding Complications in Patients Undergoing Transfemoral Transcatheter Aortic Valve Replacement: Insights From the Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Therapies Registry. Circ. Cardiovasc. Interv. 2020, 13, e008227. [Google Scholar] [CrossRef]
- Sattar, Y.; Prakash, P.; Almas, T.; Mir, T.; Titus, A.; Ahmad, S.; Khan, M.S.; Aggarwal, A.; Ullah, W.; Alhharbi, A.; et al. Cardiovascular Outcomes of Older versus Newer Generation Transcatheter Aortic Valve Replacement Recipients: A Systematic Review & Meta-analysis. Curr. Probl. Cardiol. 2023, 48, 101467. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. 2011. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 15 January 2023).
- Furfaro, E.; Nicolini, L.; Della Vecchia, A.; Di Grazia, C.; Raiola, A.M.; Varaldo, R.; Ferrando, F.; Barisione, G.; Bruzzone, B.; Angelucci, E.; et al. Hepatitis E Virus Infection in an Italian Cohort of Hematopoietic Stem Cell Transplantation Recipients: Seroprevalence and Infection. Biol. Blood Marrow Transplant. 2020, 26, 1355–1362. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Begg, C.B.; Mazumdar, M. Operating Characteristics of a Rank Correlation Test for Publication Bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629. [Google Scholar] [CrossRef] [PubMed]
- Patsopoulos, N.A.; Evangelou, E.; Ioannidis, J.P. Sensitivity of between-study heterogeneity in meta-analysis: Proposed metrics and empirical evaluation. Int. J. Epidemiol. 2008, 37, 1148–1157. [Google Scholar] [CrossRef]
- Simard, T.; Alqahtani, F.; Hibbert, B.; Mamas, M.A.; El-Hajj, S.; Harris, A.H.; Hohmann, S.F.; Alkhouli, M. Sex-specific in-hospital outcomes of transcatheter aortic valve replacement with third generation transcatheter heart valves. Catheter. Cardiovasc. Interv. 2021, 98, 176–183. [Google Scholar] [CrossRef]
- Szerlip, M.; Gualano, S.; Holper, E.; Squiers, J.J.; White, J.M.; Doshi, D.; Williams, M.R.; Hahn, R.T.; Webb, J.G.; Svensson, L.G.; et al. Sex-Specific Outcomes of Transcatheter Aortic Valve Replacement with the SAPIEN 3 Valve: Insights From the PARTNER II S3 High-Risk and Intermediate-Risk Cohorts. JACC Cardiovasc. Interv. 2018, 11, 13–20. [Google Scholar] [CrossRef]
- Tarantini, G.; Baumgartner, H.; Frank, D.; Husser, O.; Bleiziffer, S.; Rudolph, T.; Jeger, R.; Fraccaro, C.; Hovorka, T.; Wendler, O. Four-year mortality in women and men after transfemoral transcatheter aortic valve implantation using the SAPIEN 3. Catheter. Cardiovasc. Interv. 2021, 97, 876–884. [Google Scholar] [CrossRef]
- Wang, T.Y.; Gracia, E.; Callahan, S.; Bilfinger, T.; Tannous, H.; Pyo, R.; Kort, S.; Skopicki, H.; Weinstein, J.; Patel, N.; et al. Gender Disparities in Management and Outcomes Following Transcatheter Aortic Valve Implantation with Newer Generation Transcatheter Valves. Am. J. Cardiol. 2019, 123, 1489–1493. [Google Scholar] [CrossRef]
- Novotny, S.; Kort, S.; Tannous, H.; Pyo, R.; Gracia, E.; Wang, T.Y.; Callahan, S.; Skopicki, H.; Bilfinger, T.; Parikh, P.B. Predictors of 1-Year Mortality in Men Versus Women Undergoing Transfemoral Transcatheter Aortic Valve Implantation. Am. J. Cardiol. 2023, 186, 1–4. [Google Scholar] [CrossRef]
- Simmonds, M. Quantifying the risk of error when interpreting funnel plots. Syst. Rev. 2015, 4, 24. [Google Scholar] [CrossRef]
- Debray, T.P.A.; Moons, K.G.M.; Riley, R.D. Detecting small-study effects and funnel plot asymmetry in meta-analysis of survival data: A comparison of new and existing tests. Res. Synth. Methods 2018, 9, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Leon, M.B.; Smith, C.R.; Mack, M.; Miller, D.C.; Moses, J.W.; Svensson, L.G.; Tuzcu, E.M.; Webb, J.G.; Fontana, G.P.; Makkar, R.R.; et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N. Engl. J. Med. 2010, 363, 1597–1607. [Google Scholar] [CrossRef] [PubMed]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., 3rd; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021, 143, e35–e71. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; Baumann, P.; Manthey, J.; Hoffmann, M.; Schuler, G.; Mehmel, H.C.; Schmitz, W.; Kübler, W. The effect of aortic valve replacement on survival. Circulation 1982, 66, 1105–1110. [Google Scholar] [CrossRef]
- Iung, B.; Cachier, A.; Baron, G.; Messika-Zeitoun, D.; Delahaye, F.; Tornos, P.; Gohlke-Bärwolf, C.; Boersma, E.; Ravaud, P.; Vahanian, A. Decision-making in elderly patients with severe aortic stenosis: Why are so many denied surgery? Eur. Heart J. 2005, 26, 2714–2720. [Google Scholar] [CrossRef] [PubMed]
- Leon, M.B.; Smith, C.R.; Mack, M.J.; Makkar, R.R.; Svensson, L.G.; Kodali, S.K.; Thourani, V.H.; Tuzcu, E.M.; Miller, D.C.; Herrmann, H.C.; et al. Transcatheter or Surgical Aortic-Valve Replacement in Intermediate-Risk Patients. N. Engl. J. Med. 2016, 374, 1609–1620. [Google Scholar] [CrossRef]
- Pibarot, P.; Salaun, E.; Dahou, A.; Avenatti, E.; Guzzetti, E.; Annabi, M.S.; Toubal, O.; Bernier, M.; Beaudoin, J.; Ong, G.; et al. Echocardiographic Results of Transcatheter Versus Surgical Aortic Valve Replacement in Low-Risk Patients: The PARTNER 3 Trial. Circulation 2020, 141, 1527–1537. [Google Scholar] [CrossRef]
- Mack, M.J.; Leon, M.B.; Thourani, V.H.; Makkar, R.; Kodali, S.K.; Russo, M.; Kapadia, S.R.; Malaisrie, S.C.; Cohen, D.J.; Pibarot, P.; et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1695–1705. [Google Scholar] [CrossRef]
- Leon, M.B.; Mack, M.J.; Hahn, R.T.; Thourani, V.H.; Makkar, R.; Kodali, S.K.; Alu, M.C.; Madhavan, M.V.; Chau, K.H.; Russo, M.; et al. Outcomes 2 Years After Transcatheter Aortic Valve Replacement in Patients at Low Surgical Risk. J. Am. Coll. Cardiol. 2021, 77, 1149–1161. [Google Scholar] [CrossRef]
- Fassa, A.A.; Himbert, D.; Vahanian, A. Mechanisms and management of TAVR-related complications. Nat. Rev. Cardiol. 2013, 10, 685–695. [Google Scholar] [CrossRef]
- Arnold, S.V.; Manandhar, P.; Vemulapalli, S.; Kosinski, A.; Desai, N.D.; Bavaria, J.E.; Carroll, J.D.; Mack, M.J.; Thourani, V.H.; Cohen, D.J. Impact of short-term complications of transcatheter aortic valve replacement on longer-term outcomes: Results from the STS/ACC Transcatheter Valve Therapy Registry. Eur. Heart J. Qual. Care Clin. Outcomes 2021, 7, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Toggweiler, S.; Gurvitch, R.; Leipsic, J.; Wood, D.A.; Willson, A.B.; Binder, R.K.; Cheung, A.; Ye, J.; Webb, J.G. Percutaneous aortic valve replacement: Vascular outcomes with a fully percutaneous procedure. J. Am. Coll. Cardiol. 2012, 59, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Pibarot, P.; Hahn, R.T.; Weissman, N.J.; Arsenault, M.; Beaudoin, J.; Bernier, M.; Dahou, A.; Khalique, O.K.; Asch, F.M.; Toubal, O.; et al. Association of Paravalvular Regurgitation With 1-Year Outcomes After Transcatheter Aortic Valve Replacement with the SAPIEN 3 Valve. JAMA Cardiol. 2017, 2, 1208–1216. [Google Scholar] [CrossRef] [PubMed]
- Alvarado, T.; Rivero, F.; Diego, G.; García-Guimaraes, M.; Salamanca, J.; Díez-Villanueva, P.; Cuesta, J.; Antuña, P.; Jiménez-Borreguero, J.; Alfonso, F. Transcatheter aortic valve replacement using the new Evolut-Pro system: A prospective comparison with the Evolut-R device. J. Thorac. Dis. 2021, 13, 4023–4032. [Google Scholar] [CrossRef]
- De Torres-Alba, F.; Kaleschke, G.; Diller, G.P.; Vormbrock, J.; Orwat, S.; Radke, R.; Reinke, F.; Fischer, D.; Reinecke, H.; Baumgartner, H. Changes in the Pacemaker Rate After Transition from Edwards SAPIEN XT to SAPIEN 3 Transcatheter Aortic Valve Implantation: The Critical Role of Valve Implantation Height. JACC Cardiovasc. Interv. 2016, 9, 805–813. [Google Scholar] [CrossRef]
- Caponcello, M.G.; Banderas, L.M.; Ferrero, C.; Bramlage, C.; Thoenes, M.; Bramlage, P. Gender differences in aortic valve replacement: Is surgical aortic valve replacement riskier and transcatheter aortic valve replacement safer in women than in men? J. Thorac. Dis. 2020, 12, 3737–3746. [Google Scholar] [CrossRef]
- Freitas-Ferraz, A.B.; Tirado-Conte, G.; Dagenais, F.; Ruel, M.; Al-Atassi, T.; Dumont, E.; Mohammadi, S.; Bernier, M.; Pibarot, P.; Rodés-Cabau, J. Aortic Stenosis and Small Aortic Annulus. Circulation 2019, 139, 2685–2702. [Google Scholar] [CrossRef]
- Barbanti, M.; Binder, R.K.; Freeman, M.; Wood, D.A.; Leipsic, J.; Cheung, A.; Ye, J.; Tan, J.; Toggweiler, S.; Yang, T.H.; et al. Impact of low-profile sheaths on vascular complications during transfemoral transcatheter aortic valve replacement. EuroIntervention 2013, 9, 929–935. [Google Scholar] [CrossRef]
- Hayashida, K.; Lefèvre, T.; Chevalier, B.; Hovasse, T.; Romano, M.; Garot, P.; Mylotte, D.; Uribe, J.; Farge, A.; Donzeau-Gouge, P.; et al. Transfemoral Aortic Valve Implantation: New Criteria to Predict Vascular Complications. JACC Cardiovasc. Interv. 2011, 4, 851–858. [Google Scholar] [CrossRef]
- Aurigemma, G.; Battista, S.; Orsinelli, D.; Sweeney, A.; Pape, L.; Cuénoud, H. Abnormal left ventricular intracavitary flow acceleration in patients undergoing aortic valve replacement for aortic stenosis. A marker for high postoperative morbidity and mortality. Circulation 1992, 86, 926–936. [Google Scholar] [CrossRef]
- Orsinelli, D.A.; Aurigemma, G.P.; Battista, S.; Krendel, S.; Gaasch, W.H. Left ventricular hypertrophy and mortality after aortic valve replacement for aortic stenosis. A high risk subgroup identified by preoperative relative wall thickness. J. Am. Coll. Cardiol. 1993, 22, 1679–1683. [Google Scholar] [CrossRef] [PubMed]
- Pugh, M.E.; Hemnes, A.R. Pulmonary hypertension in women. Expert Rev. Cardiovasc. Ther. 2010, 8, 1549–1558. [Google Scholar] [CrossRef] [PubMed]
- Alushi, B.; Beckhoff, F.; Leistner, D.; Franz, M.; Reinthaler, M.; Stähli, B.E.; Morguet, A.; Figulla, H.R.; Doenst, T.; Maisano, F.; et al. Pulmonary Hypertension in Patients With Severe Aortic Stenosis: Prognostic Impact After Transcatheter Aortic Valve Replacement: Pulmonary Hypertension in Patients Undergoing TAVR. JACC Cardiovasc. Imaging 2019, 12, 591–601. [Google Scholar] [CrossRef] [PubMed]
- Kjønås, D.; Dahle, G.; Schirmer, H.; Malm, S.; Eidet, J.; Aaberge, L.; Steigen, T.; Aakhus, S.; Busund, R.; Rösner, A. Predictors of early mortality after transcatheter aortic valve implantation. Open Heart 2019, 6, e000936. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study (First Author, Year) | Country | Study Type | Number of Patients | Age (Mean ± SD) | CAD (%) | AF (%) | DM (%) | HTN (%) | Stroke/TIA (%) | CKD (%) | Follow-Up (Year) | Access (%) | Valve (%) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | F | M | F | M | F | M | F | M | F | M | F | M | F | M | F | M | TF | Non-TF | Balloon | Self- Expanding | ||||
| Novotny, 2022 * | USA | P | 297 | 144 | 153 | 81 ± 8 | 79 ± 9 | 16.7 | 30.1 | 27.1 | 45.1 | 34.3 | 43.1 | N/A | N/A | 16.7 | 14.4 | N/A | N/A | 1 | 100 | 0 | 78 | 22 |
| Simard, 2021 | USA | P | 44,280 | 19,438 | 24,842 | 79.8 ± 9.2 | 78.3 ± 9.8 | 61 | 76.9 | 33.9 | 37.4 | 38.9 | 42.2 | N/A | N/A | 13 | 13.1 | 32 | 39.6 | During hospitalization | 99.2 | 0.8 | N/A | N/A |
| Szerlip, 2018 | USA | P after PARTNER II S3 trial | 1661 | 657 | 1004 | 82.5 ± 7.2 | 82 ± 7 | 58.9 | 80.5 | N/A | N/A | 31.2 | 35.2 | 92.7 | 93.1 | 16.4 | 18.4 | 6.5 | 10.9 | 1 | 86.9 | 13.1 | 100 | 0 |
| Tarantini, 2020 | European countries | P | 1694 | 834 | 860 | 82.7 ± 6.29 | 80.8 ± 6.91 | 39.8 | 57.6 | 19.9 | 24.8 | 27.2 | 30.2 | 82.3 | 80.8 | N/A | N/A | N/A | N/A | 4 | 100 | 0 | 100 | 0 |
| Wang, 2019 * | USA | P | 298 | 144 | 154 | 81 ± 8 | 79 ± 9 | 16.7 | 30.5 | 27.1 | 44.8 | 34.3 | 43.5 | N/A | N/A | 16.7 | 14.3 | N/A | N/A | During hospitalization | 99.7 | 0.3 | 78.2 | 21.8 |
| Total | N/A | N/A | 47,933 | 21,073 | 26,860 | 80 ± 9.1 | 78.5 ± 9.4 | 44 | 61 | 23.5 | 34.8 | 32.8 | 37.8 | 87.5 | 87 | 15.4 | 15.2 | 25.3 | 4.8 | N/A | 97 | 3.6 | 98.2 | 1.8 |
| p-value | N/A | N/A | N/A | 0.08 | 0.01 | 0.06 | 0.5 | 0.8 | 0.5 | 0.3 | N/A | <0.001 | <0.001 | |||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trongtorsak, A.; Thangjui, S.; Adhikari, P.; Shrestha, B.; Kewcharoen, J.; Navaravong, L.; Kanjanauthai, S.; Attanasio, S.; Saudye, H.A. Gender Disparities after Transcatheter Aortic Valve Replacement with Newer Generation Transcatheter Heart Valves: A Systematic Review and Meta-Analysis. Med. Sci. 2023, 11, 33. https://doi.org/10.3390/medsci11020033
Trongtorsak A, Thangjui S, Adhikari P, Shrestha B, Kewcharoen J, Navaravong L, Kanjanauthai S, Attanasio S, Saudye HA. Gender Disparities after Transcatheter Aortic Valve Replacement with Newer Generation Transcatheter Heart Valves: A Systematic Review and Meta-Analysis. Medical Sciences. 2023; 11(2):33. https://doi.org/10.3390/medsci11020033
Chicago/Turabian StyleTrongtorsak, Angkawipa, Sittinun Thangjui, Pabitra Adhikari, Biraj Shrestha, Jakrin Kewcharoen, Leenhapong Navaravong, Somsupha Kanjanauthai, Steve Attanasio, and Hammad A. Saudye. 2023. "Gender Disparities after Transcatheter Aortic Valve Replacement with Newer Generation Transcatheter Heart Valves: A Systematic Review and Meta-Analysis" Medical Sciences 11, no. 2: 33. https://doi.org/10.3390/medsci11020033