

Factors Affecting Survival and Local Control in Patients with Bone Metastases Treated with Radiotherapy
Abstract
:1. Introduction
2. Materials and Methods
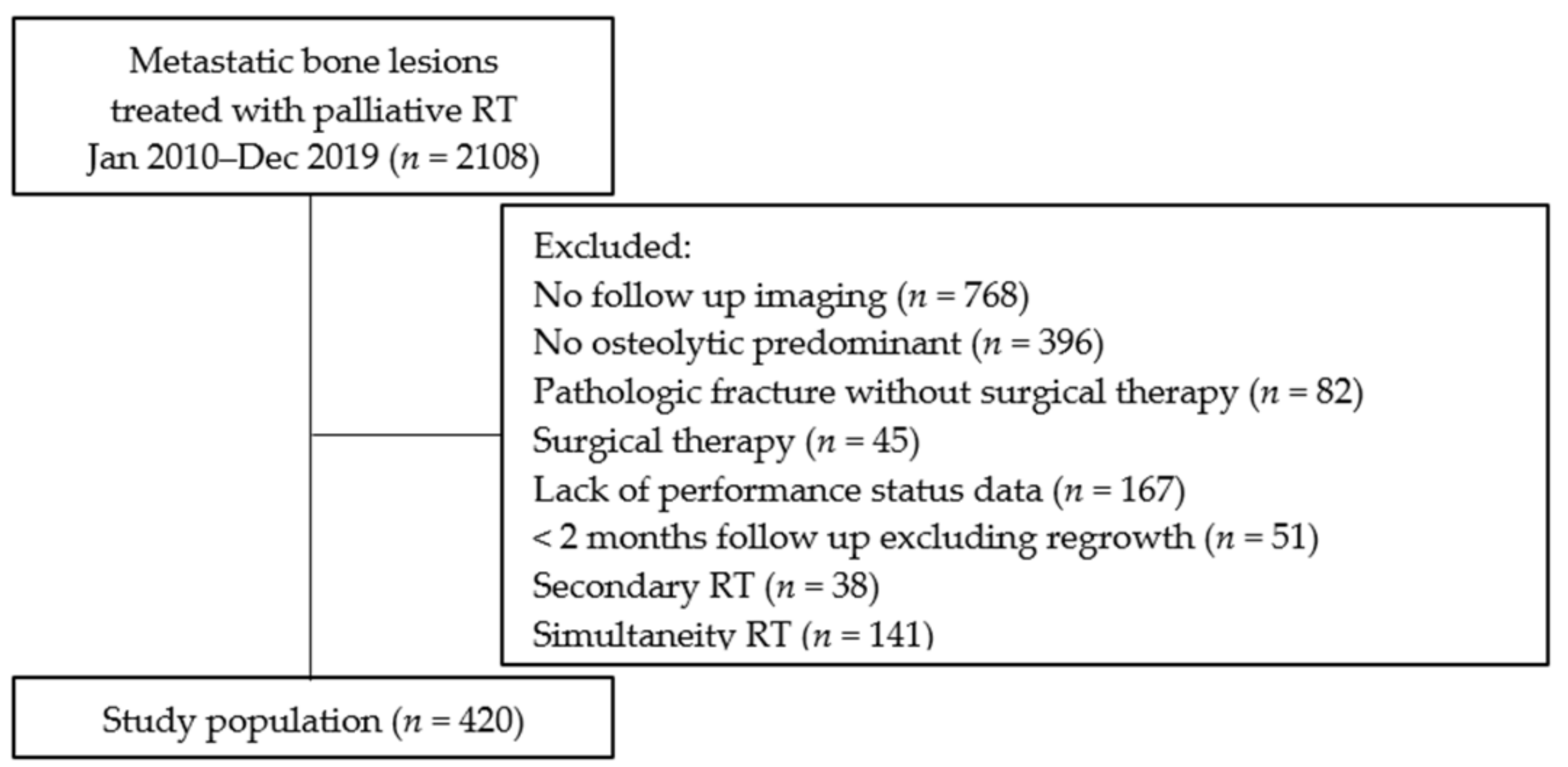
2.1. Study Protocol and Lesions
2.2. Classification of Laboratory Data and Primary Tumor Sites
2.3. Radiotherapy
2.4. Evaluation of CT Image
2.5. Statistical Analysis
3. Results
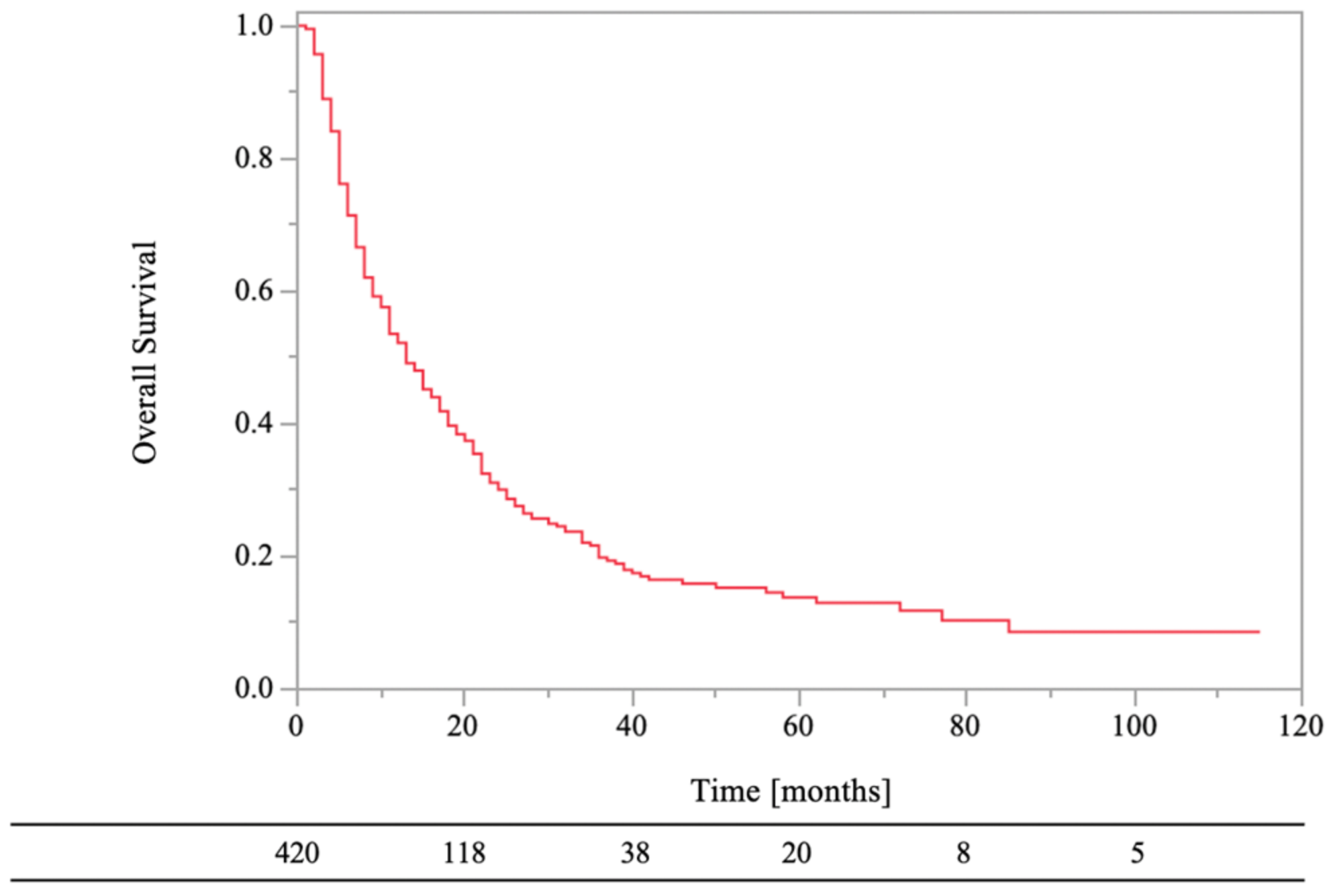
3.1. The Factors Affecting Survival Rates
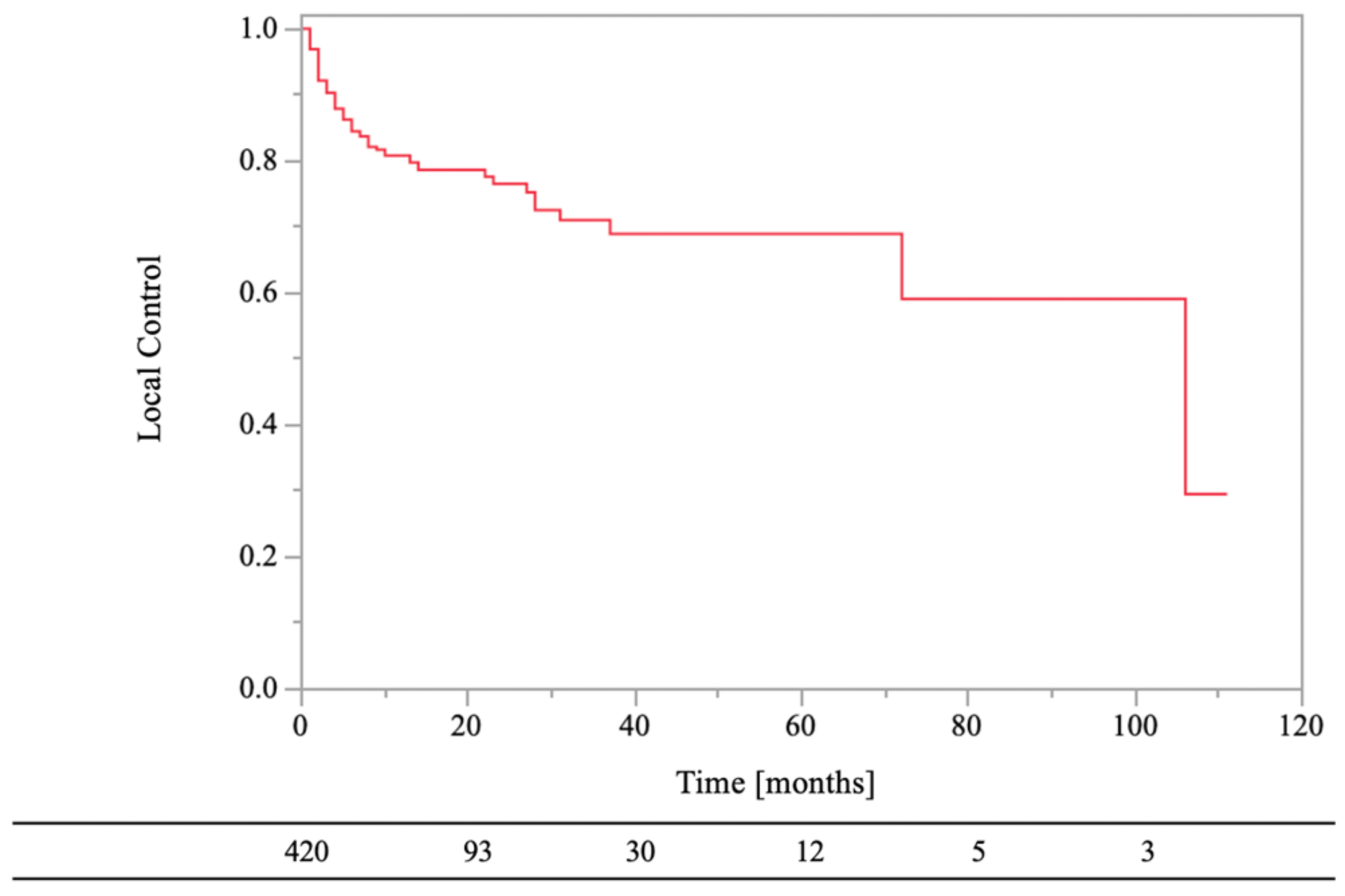
3.2. The Factors Affecting LC Rates
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nystrom, J.S.; Weiner, J.M.; Heffelfinger-Juttner, J.; Irwin, L.E.; Bateman, J.R.; Wolf, R.M. Metastatic and histologic presentations in unknown primary cancer. Semin. Oncol. 1977, 4, 53–58. [Google Scholar] [PubMed]
- Greco, T.; Fulchignoni, C.; Cianni, L.; Maccauro, G.; Perisano, C. Surgical management of tibial metastases: A systematic review. Acta Biomed. 2022, 92, e2021552. [Google Scholar] [PubMed]
- Coleman, R.E. Metastatic bone disease: Clinical features, pathophysiology and treatment strategies. Cancer Treat. Rev. 2001, 27, 165–176. [Google Scholar] [CrossRef] [PubMed]
- De Felice, F.; Piccioli, A.; Musio, D.; Tombolini, V. The role of radiation therapy in bone metastases management. Oncotarget 2017, 8, 25691–25699. [Google Scholar] [CrossRef] [PubMed]
- Perisano, C.; Greco, T.; Fulchignoni, C.; Maccauro, G.; Perisano, C. The IlluminOss(R) System: A solution in elderly patients with upper limbs bone metastases. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 119–126. [Google Scholar] [PubMed]
- Lutz, S.; Balboni, T.; Jones, J.; Lo, S.; Petit, J.; Rich, S.E.; Wong, R.; Hahn, C. Palliative radiation therapy for bone metastases: Update of an ASTRO Evidence-Based Guideline. Pract. Radiat. Oncol. 2017, 7, 4–12. [Google Scholar] [CrossRef] [PubMed]
- Oldenburger, E.; Brown, S.; Willmann, J.; van der Velden, J.M.; Spalek, M.; van der Linden, Y.M.; Kazmierska, J.; Menten, J.; Andratschke, N.; Hoskin, P. ESTRO ACROP guidelines for external beam radiotherapy of patients with complicated bone metastases. Radiother. Oncol. 2022, 173, 240–253. [Google Scholar] [CrossRef]
- Van der Velden, J.; Willmann, J.; Spalek, M.; Oldenburger, E.; Brown, S.; Kazmierska, J.; Andratschke, N.; Menten, J.; van der Linden, Y.; Hoskin, P. ESTRO ACROP guidelines for external beam radiotherapy of patients with uncomplicated bone metastases. Radiother. Oncol. 2022, 173, 197–206. [Google Scholar] [CrossRef]
- Chow, E.; Zeng, L.; Salvo, N.; Dennis, K.; Tsao, M.; Lutz, S. Update on the systematic review of palliative radiotherapy trials for bone metastasis. Clin. Oncol. 2012, 24, 113–124. [Google Scholar] [CrossRef]
- Olson, R.A.; Tiwana, M.S.; Barnes, M.; Kiraly, A.; Beecham, K.; Miller, S.; Hoegler, D.; Olivotto, I. Use of single- versus multiple-fraction palliative radiation therapy for bone metastases: Population-based analysis of 16,898 courses in a Canadian province. Int. J. Radiat. Oncol. Biol. Phys. 2014, 89, 1092–1099. [Google Scholar] [CrossRef]
- Logan, J.K.; Jiang, J.; Shih, Y.T.; Lei, X.; Xu, Y.; Hoffman, K.E.; Giordano, S.H.; Smith, B.D. Trends in Radiation for Bone Metastasis During a Period of Multiple National Quality Improvement Initiatives. J. Oncol. Pract. 2019, 15, e356–e368. [Google Scholar] [CrossRef]
- Steenland, E.; Leer, J.W.; van Houwelingen, H.; Post, W.J.; van den Hout, W.B.; Kievit, J.; de Haes, H.; Martijn, H.; Oei, B.; Vonk, E.; et al. The effect of a single fraction compared to multiple fractions on painful bone metastases: A global analysis of the Dutch Bone Metastasis Study. Radiother. Oncol. 1999, 52, 101–109. [Google Scholar] [CrossRef]
- Rich, S.E.; Chow, R.; Raman, S.; Liang Zeng, K.; Lutz, S.; Lam, H.; Silva, M.F.; Chow, E. Update of the systematic review of palliative radiation therapy fractionation for bone metastases. Radiother. Oncol. 2018, 126, 547–557. [Google Scholar] [CrossRef]
- Katagiri, H.; Okada, R.; Takagi, T.; Takahashi, M.; Murata, H.; Harada, H.; Nishimura, T.; Asakura, H.; Ogawa, H. New prognostic factors and scoring system for patients with skeletal metastasis. Cancer Med. 2014, 3, 1359–1367. [Google Scholar] [CrossRef] [PubMed]
- Tokuhashi, Y.; Matsuzaki, H.; Oda, H.; Oshima, M.; Ryu, J. A revised scoring system for preoperative evaluation of metastatic spine tumor prognosis. Spine 2005, 30, 2186–2191. [Google Scholar] [CrossRef] [PubMed]
- Bollen, L.; van der Linden, Y.M.; Pondaag, W.; Fiocco, M.; Pattynama, B.P.; Marijnen, C.A.; Nelissen, R.G.; Peul, W.C.; Dijkstra, P.D. Prognostic factors associated with survival in patients with symptomatic spinal bone metastases: A retrospective cohort study of 1043 patients. Neuro Oncol. 2014, 16, 991–998. [Google Scholar] [CrossRef] [PubMed]
- Westhoff, P.G.; de Graeff, A.; Monninkhof, E.M.; Bollen, L.; Dijkstra, S.P.; van der Steen-Banasik, E.M.; van Vulpen, M.; Leer, J.W.; Marijnen, C.A.; van der Linden, Y.M.; et al. An easy tool to predict survival in patients receiving radiation therapy for painful bone metastases. Int. J. Radiat. Oncol. Biol. Phys. 2014, 90, 739–747. [Google Scholar] [CrossRef] [PubMed]
- Willeumier, J.J.; van der Linden, Y.M.; van der Wal, C.W.P.G.; Jutte, P.C.; van der Velden, J.M.; Smolle, M.A.; van der Zwaal, P.; Koper, P.; Bakri, L.; de Pree, I.; et al. An easy-to-use prognostic model for survival estimation for patients with symptomatic long bone metastases. J. Bone Jt. Surg. Am. 2018, 100, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Makita, K.; Hamamoto, Y.; Kanzaki, H.; Kataoka, M.; Yamamoto, S.; Nagasaki, K.; Ishikawa, H.; Takata, N.; Tsuruoka, S.; Uwatsu, K.; et al. Local control of bone metastases treated with external beam radiotherapy in recent years: A multicenter retrospective study. Radiat. Oncol. 2021, 16, 225. [Google Scholar] [CrossRef]
- Gerszten, P.C.; Mendel, E.; Yamada, Y. Radiotherapy and radiosurgery for meta-static spine disease: What are the options, indications, and outcomes? Spine 2009, 34, S78–S92. [Google Scholar] [CrossRef]
- Hartsell, W.F.; Scott, C.B.; Bruner, D.W.; Scarantino, C.W.; Ivker, R.A.; Roach, M.; Suh, J.H.; Demas, W.F.; Movsas, B.; Petersen, I.A.; et al. Randomized trial of short versus long-course radiotherapy for palliation of painful bone metastases. J. Natl. Cancer Inst. 2005, 97, 798–804. [Google Scholar] [CrossRef] [PubMed]
- Takenaka, Y.; Oya, R.; Kitamiura, T.; Ashida, N.; Shimizu, K.; Takemura, K.; Yamamoto, Y.; Uno, A. Prognostic role of neutrophil-to-lymphocyte ratio in head and neck cancer: A meta-analysis. Head Neck 2018, 40, 647–655. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Du, Y.; Huang, Z.; Xu, J.; Qiu, T.; Wang, J.; Wang, T.; Zhu, W.; Liu, P. Prognostic value of PLR in various cancers: A meta-analysis. PLoS ONE 2014, 9, e101119. [Google Scholar] [CrossRef]
- Yen, H.K.; Yen, H.K.; Hu, M.H.; Zijlstra, H.; Groot, O.Q.; Hsieh, H.C.; Yang, J.J.; Karhade, A.V.; Chen, P.C.; Chen, Y.H.; et al. Prognostic significance of lab data and performance comparison by validating survival prediction models for patients with spinal metastases after radiotherapy. Radiother. Oncol. 2022, 175, 159–166. [Google Scholar] [CrossRef]
- Makita, K.; Hamamoto, Y.; Takata, N.; Ishikawa, H.; Tsuruoka, S.; Uwatsu, K.; Hato, N.; Kido, T. Prognostic significance of inflammatory response markers for locally advanced squamous cell carcinoma of the external auditory canal and middle ear. J. Radiat. Res. 2021, 62, 662–668. [Google Scholar] [CrossRef] [PubMed]
- Leithner, A.; Radl, R.; Gruber, G.; Hochegger, M.; Leithner, K.; Welkerling, H.; Rehak, P.; Windhager, R. Predictive value of seven preoperative prognostic scoring systems for spinal metastases. Eur. Spine J. 2008, 17, 1488–1495. [Google Scholar] [CrossRef] [PubMed]
- Ciray, I.; Lindman, H.; Aström, K.G. Early response of breast cancer bone metastases to chemotherapy evaluated with MR imaging. Acta Radiol. 2001, 42, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Tokito, T.; Shukuya, T.; Akamatsu, H.; Taira, T.; Ono, A.; Kenmotsu, H.; Naito, T.; Murakami, H.; Takahashi, T.; Endo, M.; et al. Efficacy of bevacizumab-containing chemotherapy for non-squamous non-small cell lung cancer with bone metastases. Cancer Chemother. Pharmacol. 2013, 71, 1493–1498. [Google Scholar] [CrossRef]
- Rades, D.; Hakim, S.G.; Bajrovic, A.; Karstens, J.H.; Veninga, T.; Rudat, V.; Schild, S.E. Impact of zoledronic acid on control of metastatic spinal cord compression. Strahlenther. Onkol. 2012, 188, 910–916. [Google Scholar] [CrossRef]
- Vassiliou, V.; Kalogeropoulou, C.; Christopoulos, C.; Solomou, E.; Leotsinides, M.; Kardamakis, D. Combination ibandronate and radiotherapy for the treatment of bone metastases: Clinical evaluation and radiologic assessment. Int. J. Radiat. Oncol. Biol. Phys. 2007, 67, 264–272. [Google Scholar] [CrossRef]
- Makita, K.; Hamamoto, Y.; Tsuruoka, S.; Takata, N.; Urashima, Y.; Miyagawa, M.; Mochizuki, T. Treatment intensity and control rates in combining external-beam radiotherapy and radioactive iodine therapy for metastatic or recurrent differentiated thyroid cancer. Int. J. Clin. Oncol. 2020, 25, 691–697. [Google Scholar] [CrossRef] [PubMed]
- Rades, D.; Panzner, A.; Rudat, V.; Karstens, J.H.; Schild, S.E. Dose escalation of radiotherapy for metastatic spinal cord compression (MSCC) in patients with relatively favorable survival prognosis. Strahlenther. Onkol. 2011, 187, 729–735. [Google Scholar] [CrossRef] [PubMed]
- Li, K.K.; Chow, E.; Chiu, H.; Bradley, N.; Doyle, M.; Barnes, E.A.; Tsao, M.; Sinclair, E.; Danjoux, C. Effectiveness of palliative Radiotherapy in the Treatment of Bone Metastases Employing the Brief Pain Inventory. J. Cancer Pain Symptom Palliation 2006, 2, 19–29. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Factors | No. of Cases | % | |
|---|---|---|---|
| age | <70 years | 275 | 65.5 |
| ≥70 years | 145 | 34.5 | |
| sex | male | 240 | 57.1 |
| female | 180 | 42.9 | |
| ECOG PS | <3 | 341 | 81.2 |
| ≥3 | 79 | 18.8 | |
| laboratory data before RT | normal | 130 | 31.0 |
| abnormal | 290 | 60.0 | |
| primary tumor sites | lung | 146 | 34.8 |
| breast | 71 | 16.9 | |
| head and neck | 19 | 4.5 | |
| esophagus | 11 | 2.6 | |
| hepatobiliary/pancreatic | 46 | 11.0 | |
| renal/ureter | 37 | 8.8 | |
| colorectal | 19 | 4.5 | |
| gynecological | 16 | 3.8 | |
| non-epithelial | 13 | 3.1 | |
| others | 42 | 10.0 | |
| RT sites | vertebral | 230 | 54.8 |
| pelvis | 99 | 23.6 | |
| rib | 33 | 7.9 | |
| others | 58 | 13.8 | |
| RT dose (BED10) | median: 39.0 Gy (14.4–71.7 Gy) | ||
| 14.4 Gy | 7 | 1.7 | |
| >14.4 Gy, <39.0 Gy | 36 | 8.6 | |
| 39.0 Gy | 261 | 62.1 | |
| >39.0 Gy | 116 | 27.6 | |
| bone cortex destruction | yes | 310 | 73.8 |
| no | 110 | 26.2 | |
| aTs before RT | yes | 232 | 55.2 |
| no | 188 | 44.8 | |
| aTs after RT | yes | 301 | 71.7 |
| no | 119 | 28.3 | |
| BMAs after RT | yes | 276 | 65.7 |
| no | 144 | 34.3 | |
| 0.5-Year (%) | 1-Year (%) | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | ||||
| age | <70 years vs. ≥70 years | 72 vs. 71 | 53 vs. 52 | 1.05 (0.83–1.33) | 0.68 | - | - |
| sex | female vs. male | 82 vs. 63 | 64 vs. 43 | 1.50 (1.19–1.89) | <0.01 | 1.38 (1.09–1.76) | <0.01 |
| ECOG PS | <3 vs. ≥3 | 74 vs. 59 | 55 vs. 38 | 1.38 (1.05–1.81) | 0.02 | 1.38 (1.04–1.82) | 0.03 |
| laboratory data before RT | normal vs. abnormal | 89 vs. 63 | 68 vs. 45 | 1.62 (1.26–2.07) | <0.01 | 1.59 (1.23–2.04) | <0.01 |
| primary tumor sites | low risk vs. high risk | 74 vs. 64 | 56 vs. 42 | 1.43 (1.11–1.84) | <0.01 | 1.28 (0.99–1.66) | 0.06 |
| bone cortex destruction | yes vs. no | 72 vs. 71 | 51 vs. 55 | 0.95 (0.73–1.23) | 0.68 | - | - |
| RT dose (BED10) | ≥39.0 Gy vs. <39.0 Gy | 75 vs. 37 | 56 vs. 21 | 2.30 (1.62–3.27) | <0.01 | 2.15 (1.50–3.07) | <0.01 |
| aTs before RT | yes vs. no | 70 vs. 73 | 51 vs. 53 | 0.90 (0.72–1.14) | 0.39 | - | - |
| aTs after RT | yes vs. no | 77 vs. 56 | 57 vs. 40 | 1.69 (1.31–2.18) | <0.01 | 1.57 (1.20–2.05) | <0.01 |
| BMAs after RT | yes vs. no | 77 vs. 61 | 57 vs. 43 | 1.48 (1.17–1.88) | <0.01 | 1.29 (1.00–1.65) | 0.05 |
| 0.5-Year (%) | 1-Year (%) | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | ||||
| age | <70 years vs. ≥70 years | 89 vs. 77 | 84 vs. 74 | 1.79 (1.15–2.79) | 0.01 | 1.52 (0.96–2.39) | 0.07 |
| sex | female vs. male | 88 vs. 81 | 85 vs. 77 | 1.59 (1.00–2.51) | 0.05 | - | - |
| ECOG PS | <3 vs. ≥3 | 85 vs. 83 | 81 vs. 81 | 1.06 (0.58–1.92) | 0.85 | - | - |
| laboratory data before RT | normal vs. abnormal | 94 vs. 80 | 90 vs. 76 | 2.07 (1.22–3.51) | 0.01 | 2.16 (1.26–3.73) | <0.01 |
| primary tumor sites | low risk vs. high risk | 90 vs. 70 | 89 vs. 56 | 4.34 (2.78–6.78) | <0.01 | 4.15 (2.64–6.52) | <0.01 |
| bone cortex destruction | yes vs. no | 81 vs. 94 | 79 vs. 86 | 0.54 (0.30–0.98) | 0.04 | 0.59 (0.33–1.08) | 0.09 |
| RT dose (BED10) | ≥39.0 Gy vs. <39.0 Gy | 85 vs. 75 | 82 vs. 66 | 1.67 (0.82–3.34) | 0.16 | - | - |
| aTs before RT | yes vs. no | 85 vs. 83 | 81 vs. 81 | 0.98 (0.63–1.53) | 0.94 | - | - |
| aTs after RT | yes vs. no | 89 vs. 70 | 86 vs. 64 | 2.54 (1.61–4.02) | <0.01 | 1.63 (0.98–2.71) | 0.06 |
| BMAs after RT | yes vs. no | 89 vs. 76 | 86 vs. 70 | 2.35 (1.51–3.67) | <0.01 | 1.85 (1.15–2.98) | 0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Makita, K.; Hamamoto, Y.; Kanzaki, H.; Nagasaki, K.; Takata, N.; Tsuruoka, S.; Uwatsu, K.; Kido, T. Factors Affecting Survival and Local Control in Patients with Bone Metastases Treated with Radiotherapy. Med. Sci. 2023, 11, 17. https://doi.org/10.3390/medsci11010017
Makita K, Hamamoto Y, Kanzaki H, Nagasaki K, Takata N, Tsuruoka S, Uwatsu K, Kido T. Factors Affecting Survival and Local Control in Patients with Bone Metastases Treated with Radiotherapy. Medical Sciences. 2023; 11(1):17. https://doi.org/10.3390/medsci11010017
Chicago/Turabian StyleMakita, Kenji, Yasushi Hamamoto, Hiromitsu Kanzaki, Kei Nagasaki, Noriko Takata, Shintaro Tsuruoka, Kotaro Uwatsu, and Teruhito Kido. 2023. "Factors Affecting Survival and Local Control in Patients with Bone Metastases Treated with Radiotherapy" Medical Sciences 11, no. 1: 17. https://doi.org/10.3390/medsci11010017