
Effect of Sub-Inhibitory Concentrations of Nitrofurantoin, Ciprofloxacin, and Trimethoprim on In Vitro Biofilm Formation in Uropathogenic Escherichia coli (UPEC)
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Susceptibility of UPEC to Antimicrobials
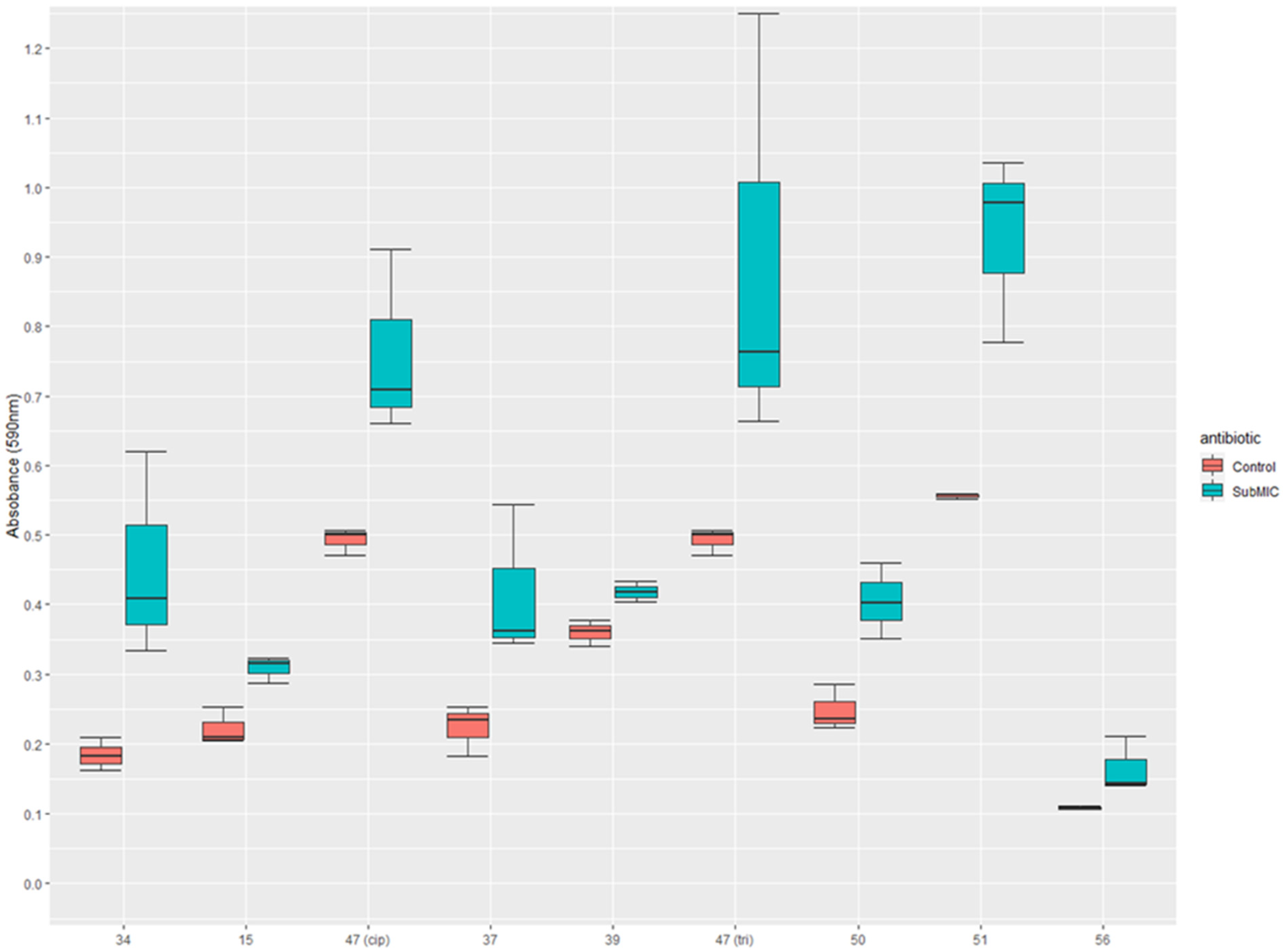
3.2. The Effect of Sub-Inhibitory Concentrations of Antibiotics on Biofilm Formation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tandogdu, Z.; Wagenlehner, F.M.E. Global Epidemiology of Urinary Tract Infections. Curr. Opin. Infect. Dis. 2016, 29, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Terlizzi, M.E.; Gribaudo, G.; Maffei, M.E. UroPathogenic Escherichia Coli (UPEC) Infections: Virulence Factors, Bladder Responses, Antibiotic, and Non-Antibiotic Antimicrobial Strategies. Front. Microbiol. 2017, 8, 1566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geerlings, S.E. Clinical Presentations and Epidemiology of Urinary Tract Infections. In Urinary Tract Infections: Molecular Pathogenesis and Clinical Management; John Wiley & Sons: Hoboken, NJ, USA, 2016; pp. 27–40. [Google Scholar] [CrossRef]
- Foxman, B. Urinary Tract Infection Syndromes. Occurrence, Recurrence, Bacteriology, Risk Factors, and Disease Burden. Infect. Dis. Clin. N. Am. 2014, 28, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Callan, A.; O’Shea, E.; Galvin, S.; Duane, S.; Corry, O.; SIMPle Team, T.; Vellinga, A. The Economic Cost of Urinary Tract Infections in The Community: Results From Ireland. Value Health 2014, 17, A468. [Google Scholar] [CrossRef] [PubMed]
- Bonkat, G.; Bartoletti, R.; Bruyere, F.; Cai, T.; Geerlings, S.E.; Koves, B.; Schubert, S.; Wagenlehner, F. EAU Guidelines on Urological Infections. Eur. Assoc. Urol. 2022. Available online: https://uroweb.org/guidelines/urological-infections/chapter/the-guideline (accessed on 4 November 2022).
- Blango, M.G.; Mulvey, M.A. Persistence of Uropathogenic Escherichia coli in the Face of Multiple Antibiotics. Antimicrob. Agents Chemother. 2010, 54, 1855–1863. [Google Scholar] [CrossRef] [Green Version]
- Soto, S.M.; Smithson, A.; Horcajada, J.P.; Martinez, J.A.; Mensa, J.P.; Vila, J. Implication of Biofilm Formation in the Persistence of Urinary Tract Infection Caused by Uropathogenic Escherichia coli. Clin. Microbiol. Infect. 2006, 12, 1034–1036. [Google Scholar] [CrossRef] [Green Version]
- Szczuka, E.; Jabłońska, L.; Kaznowski, A. Effect of Subinhibitory Concentrations of Tigecycline and Ciprofloxacin on the Expression of Biofilm-Associated Genes and Biofilm Structure of Staphylococcus epidermidis. Microbiology 2017, 163, 712–718. [Google Scholar] [CrossRef]
- Gümüş, D.; Kalaycı-Yüksek, F.; Yörük, E.; Uz, G.; Çelik, E.; Arslan, C.; Aydın, E.M.; Canlı, C.; Anğ-Küçüker, M. Alterations of Growth Rate and Gene Expression Levels of UPEC by Antibiotics at Sub-MIC. Folia Microbiol. 2018, 63, 451–457. [Google Scholar] [CrossRef] [PubMed]
- Rafaque, Z.; Abid, N.; Liaqat, N.; Afridi, P.; Siddique, S.; Masood, S.; Kanwal, S.; Dasti, J.I. In-Vitro Investigation of Antibiotics Efficacy against Uropathogenic Escherichia coli Biofilms and Antibiotic Induced Biofilm Formation at Subminimum Inhibitory Concentration of Ciprofloxacin. Infect. Drug Resist. 2020, 13, 2801–2810. [Google Scholar] [CrossRef]
- Dong, G.; Li, J.; Chen, L.; Bi, W.; Zhang, X.; Liu, H.; Zhi, X.; Zhou, T.; Cao, J. Effects of Sub-Minimum Inhibitory Concentrations of Ciprofloxacin on Biofilm Formation and Virulence Factors of Escherichia coli. Brazilian J. Infect. Dis. 2019, 23, 15–21. [Google Scholar] [CrossRef]
- Smanthong, N.; Tavichakorntrakool, R.; Saisud, P.; Prasongwatana, V.; Sribenjalux, P.; Lulitanond, A.; Tunkamnerdthai, O.; Wongkham, C.; Boonsiri, P. Biofilm Formation in Trimethoprim/Sulfamethoxazole-Susceptible and Trimethoprim/Sulfamethoxazole-Resistant Uropathogenic Escherichia coli. Asian Pac. J. Trop. Biomed. 2015, 5, 485–487. [Google Scholar] [CrossRef] [Green Version]
- Gandee, L.; Hsieh, J.T.; Sperandio, V.; Moreira, C.G.; Lai, C.H.; Zimmern, P.E. The Efficacy of Immediate versus Delayed Antibiotic Administration on Bacterial Growth and Biofilm Production of Selected Strains of Uropathogenic Escherichia Coli and Pseudomonas Aeruginosa. Int. Braz J. Urol 2015, 41, 67–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naves, P.; del Prado, G.; Huelves, L.; Gracia, M.; Ruiz, V.; Blanco, J.; Dahbi, G.; Blanco, M.; del Carmen Ponte, M.; Soriano, F. Correlation between Virulence Factors and in Vitro Biofilm Formation by Escherichia coli Strains. Microb. Pathog. 2008, 45, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Sung, B.H.; Lee, C.H.; Yu, B.J.; Lee, J.H.; Lee, J.Y.; Kim, M.S.; Blattner, F.R.; Kim, S.C. Development of a Biofilm Production-Deficient Escherichia coli Strain as a Host for Biotechnological Applications. Appl. Environ. Microbiol. 2006, 72, 3336–3342. [Google Scholar] [CrossRef] [Green Version]
- Schön, T.; Werngren, J.; Machado, D.; Borroni, E.; Wijkander, M.; Lina, G.; Mouton, J.; Matuschek, E.; Kahlmeter, G.; Giske, C.; et al. Antimicrobial Susceptibility Testing of Mycobacterium tuberculosis Complex Isolates—the EUCAST Broth Microdilution Reference Method for MIC Determination. Clin. Microbiol. Infect. 2020, 26, 1488–1492. [Google Scholar] [CrossRef]
- EUCAST. European Committee on Antimicrobial Susceptibility Testing (EUCAST). Available online: Http://Www.Eucast.Org (accessed on 28 October 2022).
- RStudio Team. R Studio: Integrated Development for R; RStudio, PBC: Boston, MA, USA, 2020. [Google Scholar]
- Kot, B. Antibiotic Resistance among Uropathogenic Escherichia coli. Polish J. Microbiol. 2019, 68, 403–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Grady, M.C.; Barry, L.; Corcoran, G.D.; Hooton, C.; Sleator, R.D.; Lucey, B. Empirical Treatment of Urinary Tract Infections: How Rational Are Our Guidelines? J. Antimicrob. Chemother. 2018, 74, 214–217. [Google Scholar] [CrossRef]
- Nordmann, P.; Poirel, L.; Mueller, L. Rapid Detection of Fosfomycin Resistance in Escherichia coli. J. Clin. Microbiol. 2019, 57, 16–20. [Google Scholar] [CrossRef] [Green Version]
- Cepas, V.; López, Y.; Muñoz, E.; Rolo, D.; Ardanuy, C.; Martí, S.; Xercavins, M.; Horcajada, J.P.; Bosch, J.; Soto, S.M. Relationship between Biofilm Formation and Antimicrobial Resistance in Gram-Negative Bacteria. Microb. Drug Resist. 2019, 25, 72–79. [Google Scholar] [CrossRef]
- Behzadi, P.; Urbán, E.; Gajdács, M. Association between Biofilm-Production and Antibiotic Resistance in Uropathogenic Escherichia coli (UPEC): An In Vitro Study. Diseases 2020, 8, 17. [Google Scholar] [CrossRef]
- Costerton, J.W. Bacterial Biofilms: A Common Cause of Persistent Infections. Science 1999, 284, 1318–1322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sepandj, F.; Ceri, H.; Gibb, A.; Read, R.; Olson, M. Minimum Inhibitory Concentration (MIC) versus Minimum Biofilm Eliminating Concentration (MBEC) in Evaluation of Antibiotic Sensitivity of Gram-Negative Bacilli Causing Peritonitis. Perit. Dial. Int. 2004, 24, 65–67. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Reardon, C.P.; Read, N.; Thorpe, S.; Evans, A.; Todd, N.; Van Der Woude, M.; Krauss, T.F. Attachment and Antibiotic Response of Early-Stage Biofilms Studied Using Resonant Hyperspectral Imaging. NPJ Biofilms Microbiomes 2020, 6, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Romero, D.; Traxler, M.F.; López, D.; Kolter, R. Antibiotics as Signal Molecules. Chem. Rev. 2011, 111, 5492–5505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balagué, C.; Fernández, L.; Pérez, J.; Grau, R. Effect of Ciprofloxacin on Adhesive Properties of Non-P Mannose-Resistant Uropathogenic Escherichia coli Isolates. J. Antimicrob. Chemother. 2003, 51, 401–404. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Preston, J.F.; Romeo, T. The PgaABCD Locus of Escherichia Coli Promotes the Synthesis of a Polysaccharide Adhesin Required for Biofilm Formation. J. Bacteriol. 2004, 186, 2724–2734. [Google Scholar] [CrossRef] [Green Version]
- Katongole, P.; Nalubega, F.; Florence, N.C.; Asiimwe, B.; Andia, I. Biofilm Formation, Antimicrobial Susceptibility and Virulence Genes of Uropathogenic Escherichia Coli Isolated from Clinical Isolates in Uganda. BMC Infect. Dis. 2020, 20, 1–6. [Google Scholar] [CrossRef]
- Davari Abad, E.; Khameneh, A.; Vahedi, L. Identification Phenotypic and Genotypic Characterization of Biofilm Formation in Escherichia coli Isolated from Urinary Tract Infections and Their Antibiotics Resistance. BMC Res. Notes 2019, 12, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Emody, L.; Kerényi, M.; Nagy, G. Virulence Factors of Uropathogenic Escherichia coli. Int. J. Antimicrob. Agents 2003, 22 (Suppl. S2), 29–33. [Google Scholar] [CrossRef]
- Rich, S.N.; Klann, E.M.; Almond, C.R.; Larkin, E.M.; Nicolette, G.; Ball, J.D. Associations between Antibiotic Prescriptions and Recurrent Urinary Tract Infections in Female College Students. Epidemiol. Infect. 2019, 147, e119. [Google Scholar] [CrossRef]


{kind=link}
| Resistance | Effect on Biofilm Formation | Strains in Phenotype |
|---|---|---|
| Resistant to none | None | 1, 5, 18, 23, 58, ATCC 25922 |
| N↓ C↓ T↓ | 20, 41, 43, 46, 55 | |
| C↓ T↓ | 3, 10, 12, 52 | |
| N↑ C↑ | 2, 60 | |
| N↓ T↓ | 45, MG1655 K12 | |
| C↓ | 13, 59 | |
| T↓ | 7, 8 | |
| N↑ T↑ C↓ | 4, 36 | |
| N↓ | 27 | |
| N↓ C↓ T↑ | 29 | |
| N↑ C↑ T↑ | 38 | |
| N↓ C↑ T↓ | 40 | |
| N↑ C↓ T↓ | 62 | |
| N↓ T↑ | 28 | |
| N↓ C↑ | 31 | |
| N↑ C↓ | 61 | |
| Trimethoprim | N↓ C↓ T↓ | 11, 22, 30 |
| N↑ C↓ T↑ | 50 | |
| N↓ T↑ | 39 | |
| N↓ C↓ | 44 | |
| C↓ T↑ | 51 | |
| C↓ T↓ | 53 | |
| N↑ T↑ | 37 | |
| N↓ | 33 | |
| N↑ | 9 | |
| C↓ | 16 | |
| None | 32 | |
| Ciprofloxacin | N↓ C↓ T↓ | 42 |
| C↑ | 15 | |
| N↓ | 24 | |
| None | 25 | |
| Ciprofloxacin and Trimethoprim | N↓ C↓ T↓ | 35, 54 |
| None | 17, 57 | |
| N↑ T↑ | 47 | |
| C↑ T↑ | 56 | |
| C↓ | 48 | |
| Resistant to all | N↓ C↓ T↓ | 49 |
| N↑ C↓ | 34 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Whelan, S.; O’Grady, M.C.; Corcoran, G.D.; Finn, K.; Lucey, B. Effect of Sub-Inhibitory Concentrations of Nitrofurantoin, Ciprofloxacin, and Trimethoprim on In Vitro Biofilm Formation in Uropathogenic Escherichia coli (UPEC). Med. Sci. 2023, 11, 1. https://doi.org/10.3390/medsci11010001
Whelan S, O’Grady MC, Corcoran GD, Finn K, Lucey B. Effect of Sub-Inhibitory Concentrations of Nitrofurantoin, Ciprofloxacin, and Trimethoprim on In Vitro Biofilm Formation in Uropathogenic Escherichia coli (UPEC). Medical Sciences. 2023; 11(1):1. https://doi.org/10.3390/medsci11010001
Chicago/Turabian StyleWhelan, Shane, Mary Claire O’Grady, Gerard Daniel Corcoran, Karen Finn, and Brigid Lucey. 2023. "Effect of Sub-Inhibitory Concentrations of Nitrofurantoin, Ciprofloxacin, and Trimethoprim on In Vitro Biofilm Formation in Uropathogenic Escherichia coli (UPEC)" Medical Sciences 11, no. 1: 1. https://doi.org/10.3390/medsci11010001