
Effects of Changing Veterinary Handling Techniques on Canine Behaviour and Physiology Part 1: Physiological Measurements

1
Department of Health Management, Atlantic Veterinary College, University of Prince Edward Island, Charlottetown, PE C1A 4P3, Canada
2
Department of Applied Human Sciences, Faculty of Nursing, University of Prince Edward Island, Charlottetown, PE C1A 4P3, Canada
*
Author to whom correspondence should be addressed.
Animals 2023, 13(7), 1253; https://doi.org/10.3390/ani13071253
Submission received: 19 February 2023
/
Revised: 18 March 2023
/
Accepted: 3 April 2023
/
Published: 4 April 2023
(This article belongs to the Section Veterinary Clinical Studies)
Abstract
:Simple Summary
Canine patient stress during veterinary visits is an animal welfare and health concern. Low-stress handling, combined with cooperative and collaborative care, has been proposed to reduce patient fear; however, research investigating these techniques in a veterinary setting is lacking. The aim of this study was to determine whether targeted interventions during veterinary visits helped to prevent or reduce distress in dogs. A total of 28 dogs were examined within four visits across 8 weeks. Following the first visit, dogs were split into intervention and control groups, where the intervention group received simple low-stress handling techniques and practiced collaborative care, and the control groups experienced routine care. The interventions were selected so that they could easily be incorporated into a busy veterinary hospital. There was a greater reduction in serum cortisol, an indicator of stress, between the first and last visit in the intervention group. The intervention group had a significant reduction in a composite stress response index from the first to last visit. Our findings have important applications both for dogs who are already afraid of veterinary examination and for use in a preventative context with dogs just beginning their veterinary experience.
Abstract
Signs of distress in dogs are often normalized during routine veterinary care, creating an animal welfare concern. We sought to test whether targeted interventions during veterinary visits affect physiological indicators of stress in dogs. Some 28 dogs were examined within four visits across 8 weeks. All dogs received the same care during the first visit and were then randomized into control and intervention groups for visits 2–4. In the intervention group, 14 dogs underwent procedures designed to reduce stress and to enlist their collaboration during examination. The 14 dogs in the control group received routine care. At each visit, heart rate (HR), serum cortisol (CORT), neutrophil lymphocyte ratio (NLR), and creatine kinase (CK) were measured. A composite stress index based on the summed standardized scores for these markers was constructed. No differences in HR, NLR, and CK parameters between groups were found, and both groups had a decrease in CORT by visit four. However, the intervention group showed a greater overall decrease in CORT between the first and fourth visit than the control group (p < 0.04). The composite stress index differed between the first and fourth visits for the intervention group, but not for the control group (Intervention p = 0.03; Control p= 0.288). There was a tendency for the composite stress index to worsen at visit four vs. visit one for the control group. The findings suggest that dogs that participated in adaptive, collaborative exams and procedures designed to minimize fear had a greater reduction in stress over time compared to those receiving standard care.
1. Introduction
The welfare of dogs undergoing veterinary care has primarily been focused on achieving a basic standard of physical care that includes redressing pain. Through this lens, signs of distress have often been normalized—and in many cases, expected—as part of routine care, when instead, they should be viewed as welfare concerns. Fear has been demonstrated to begin as soon as dogs walk into a clinic. For example, a study conducted at a veterinary hospital in Germany found that fewer than half of the dogs entered the clinic calmly, and 13.3% had to be dragged or carried into the building [1]. A similar finding was highlighted in a study demonstrating that when walking into a vet clinic, 60% of dogs showed apprehensive postures and 18% showed signs of fear-related aggression [2]. Two-thirds of dogs in a veterinary waiting room spent more than 20% of the time exhibiting at least one sign of stress, and 53% exhibited four or more signs of stress [3]. Other aspects of veterinary visits including walking onto a scale and physical examination have been shown to increase stress in canine patients [1,4,5,6]. Multiple studies have shown that a majority of dogs show signs of fear while on an examination table [1,5], and a recent study found that fear responses were increased during examination that involved physical manipulations [7]. The pervasive level of fear and anxiety currently experienced by patients during veterinary visits has prompted immediate welfare concerns in addition to long term implications and consequences. Each negative event an animal experiences when at the veterinary clinic conditions them for the future negative responses to similar events, causing subsequent visits to become more difficult and time-consuming [1,8]. Dogs < 2 years old that visited the practice frequently were more fearful than older dogs that visited infrequently [1], suggesting that exposure to experiences they perceive as fearful matters to them, and that repeated exposure to veterinary practices may actually enhance fear.
Fear and anxiety can have significant physiological consequences for dogs. In many species, including dogs, distress can reduce immune function and reproductive abilities, increase the risk of contracting infectious diseases, delay healing, and have a negative effect on life span [9,10,11,12,13]. Exposure to stressors can further negatively affect treatment outcomes by causing pet guardians to delay intervention and preventative veterinary care. The stress experienced by the pet—and owner—and induced by veterinary appointments is a large contributor to decreased veterinary care [14]. A quantitative survey of 2188 dogs and cat owners found that 58% of cat owners and 38% of dog owners perceived that their animal “hates” going to the veterinarian, and 38% of cat owners and 26% of dog owners found it stressful just thinking about taking their animal to the veterinary clinic [14]. Stress responses experienced during veterinary visits affect the animal, pet guardian and veterinary staff in a variety of manifestations. These responses may include how frequently owners seek veterinary care, the negative effect of stress on the patient’s long-term health, reductions in the veterinarian’s ability to assess and accurately diagnose and treat health concerns, and the reduced safety of the veterinary staff, with an increased risk of injury associated with stressed animals [8,10,14,15].
Recently, there has been increased acknowledgment and awareness of the persistence of stress and fear in veterinary patients. With this acknowledgement, in the veterinary community, recognition of the importance of low-stress handling in the veterinary hospital and clinic has grown [15,16,17,18,19]. Some limited research has shown that dogs with positive experiences while at the veterinary clinic have been found to be less fearful than others [1]. Additionally, recent research has begun to investigate the influence of collaborative care on dog fear levels during veterinary examination [20]. Early veterinary visits set the foundation for subsequent interactions, and can have lasting effects on anxiety levels in patients [15,21]. However, data assessing the effect of the implementation of low-stress techniques within a veterinary setting and their effectiveness in reducing distress in patients are lacking. The aim of our study was to determine whether simple interventions, which could be easily implemented in any veterinary practice, affected measurements of distress at the veterinary clinic. Rather than singling out one intervention to assess, we used an examination protocol that altered most of the patterns of the standard physical exam for the intervention group, since what the dogs experience is the entire approach. Accordingly, we assayed responses to an overall pattern of changes, rather than to any of our individual interventions.
This paper is part of a larger project in which we sought to evaluate all dogs behaviourally and physiologically for their responses to the veterinary visit. To measure the physiological response to the stress of the veterinary visits, we sought an approach that would evaluate various axes of the dogs’ responses to the stressor. We chose four parameters to evaluate: heart rate (HR), serum cortisol (CORT), serum creatine (phospho)-kinase (CK/CPK), and neutrophil/lymphocyte ratio (NLR).
HR is a marker of an immediate sympathetic response [22], cortisol is a marker of an acute stress response [23], and NLR is a reliable immunological measure of chronic stress [24]. NLR is relatively unaffected by handling associated with acute stress such as blood sampling [24], and may be a good marker of sub-clinical inflammation [25]. CK can be an indicator of muscle tension and/or damage. In profound panic, acute muscle contraction and injury may be one component of the arousal and stress response associated with freezing [26], and so CK was selected as a component of a multi-modal assessment of physiological stress to evaluate any panic component [27].
2. Materials and Methods
This study was conducted from June to September 2021. Data were analyzed using SAS, Social Science Statistics (https://www.socscistatistics.com/ (accessed on 27 December 2022)), R and Excel (R Project, 2011; R version 4.1.2 (2021-11-01)—“Bird Hippie”). This research was approved by the Animal Care Committee (ACC) and the Research Ethics Board (REB) of UPEI (Joint Protocol 21-02). All dog guardians gave informed consent and could withdraw at any time.
2.1. Enrolment
A total of 30 dogs were enrolled for the study design target of 28 participants (Table 1) based on initial power calculations of 80% with a one-tailed probability of 0.1 and zbeta = 1.28. Dogs whose guardians expressed an interest in their dogs’ behaviours during veterinary visits and who were interested in making such visits as happy as possible were solicited for the study. Posters were placed in local businesses and veterinary offices within Charlottetown, Prince Edward Island, Canada and within the Atlantic Veterinary College (AVC) Veterinary Teaching Hospital (VTH) waiting room, and in the hallways of the hospital. A recruitment message was sent to AVC staff and veterinary students via the AVC dean’s office. Inclusion criteria specified that participating dogs had to be at least 6 months of age and be in good health. By requiring that dogs were 6 months of age, we guaranteed that all had had some prior veterinary experience. This is also the minimum age for pharmacological studies for behavioural medications, including those used prophylactically for veterinary evaluation. Exclusion criteria included females that were pregnant or lactating, animals that were receiving behaviour-altering medications, and those that had a history of overt aggression during veterinary examinations. Overt aggression was determined via an aggression screen within the pre-enrolment WDQ (Working Dog Questionnaire–pet version) that asked what behaviours their pet demonstrated at the veterinary clinic. Behaviours included snarling, lifting their lip, barking, growling, snapping, biting, withdrawing, or having no reaction.
Owners were told at the end of the study that the laboratory results could be sent upon request to their family veterinary clinic, and if they wished to further pursue improvement in their dog’s behaviour at the veterinary hospital, free visits would be arranged to address their dog’s concerns. Two dogs were removed from participation during the study due to frank aggression (growling, snarling, lunging, snapping) when we attempted to touch them, which prevented their safe handling. This left 28 dogs, the target number, for the control (14 dogs) and intervention (14 dogs) groups.
2.2. Questionnaire
Prior to enrolment, pet owners were asked to complete the WDQ—PET questionnaire (Figure S1). This questionnaire has been used in dogs across contexts, and when compared with provocative tests for problematic behaviours (aggression, noise reactivity, fear, and separation anxiety) has been shown to accurately portray patterns of behaviour with a low level of false negatives and false positives [28,29,30]. The questionnaire consists of 78 questions and is broken down into six parts: demographic information, reward/reinforcement-based questions, questions about reacting to the environment, general behavioural patterns, husbandry information, and general behavioural and medical history, which included response to absences and noises, ritualistic behaviour, an aggression screen, and age-related changes. The questionnaire provided scorable historical information—including if the dog was adopted or obtained as a puppy, their training history, plus scorable questionnaires for fear, anxiety and aggression. These data will be used in an analysis of behavioural responses during the veterinary examination as part of another paper in progress. The WDQ-Pet also served as check that participants met the inclusion criteria.
2.3. Study Design
The study took place from July to October of 2021 at the AVC Veterinary Teaching Hospital (VTH). The study consisted of four visits across 8 weeks, with each visit being separated by 2 weeks. Once the dog was scheduled into an appointment slot, each subsequent appointment would occur at the same time of day, in order to remain consistent with diurnal cortisol curves [31]. During each visit, a physical examination was conducted and a blood sample obtained. All dogs were weighed at each visit. All dogs were video-recorded and assessed behaviourally using a Likert scale, similar to those published [15,32,33] (Table S1), during the following events: (1) when the dog walked into the hospital, (2) when the dog was weighed, (3) as the dog entered the exam room, and (4) throughout the physical examination, during which scoring was carried out at the beginning and end of the exam.
All dogs were randomized into two treatment groups of 14 dogs each, a control and an intervention group, using an online randomization tool (Randomizer.org). Owners were unaware of the treatment assigned until the end of visit four. Both treatments were treated identically at the first visit, when every participant received the control treatment. After the initial visit, different protocols were used for each group when weighing the dog on a scale, during the physical exam and blood draw, for visits two to four, and the type of homework assigned between visits. Table 2 summarizes the major differences between each treatment group.
2.3.1. Homework Protocols
Clients in each treatment group received homework assignments with their dogs; they were asked to perform these for 5 consecutive minutes, three times a week, during the two weeks between their appointments. Written and video instructions were provided, and clients were asked to complete logbooks noting the time of starting and stopping, and any concerns or observations they had. Clients were asked to bring these logbooks to subsequent appointments. Intervention group members were given a soft blue bathmat and a Lickimat® at the end of their first visit, and they were asked to use these tools to practice parts of a physical exam with their pet. Clients were asked to touch various parts of the dog’s body (neck, abdomen, chest, legs), to encourage dogs to turn their heads to offer their ears to handle, picking up each of their feet, applying non-scented lotion to both the front and back legs where blood draws would typically occur to imitate the application of a lidocaine cream, and briefly applying pressure to leg veins. These steps were both written and demonstrated on a dog in an accompanying video. Control group members were simply asked to pet their dogs in the allotted time, and a video was provided for how to calmly pet your dog (Figures S2 and S3, Videos S1 and S2).
2.3.2. Scale Protocols
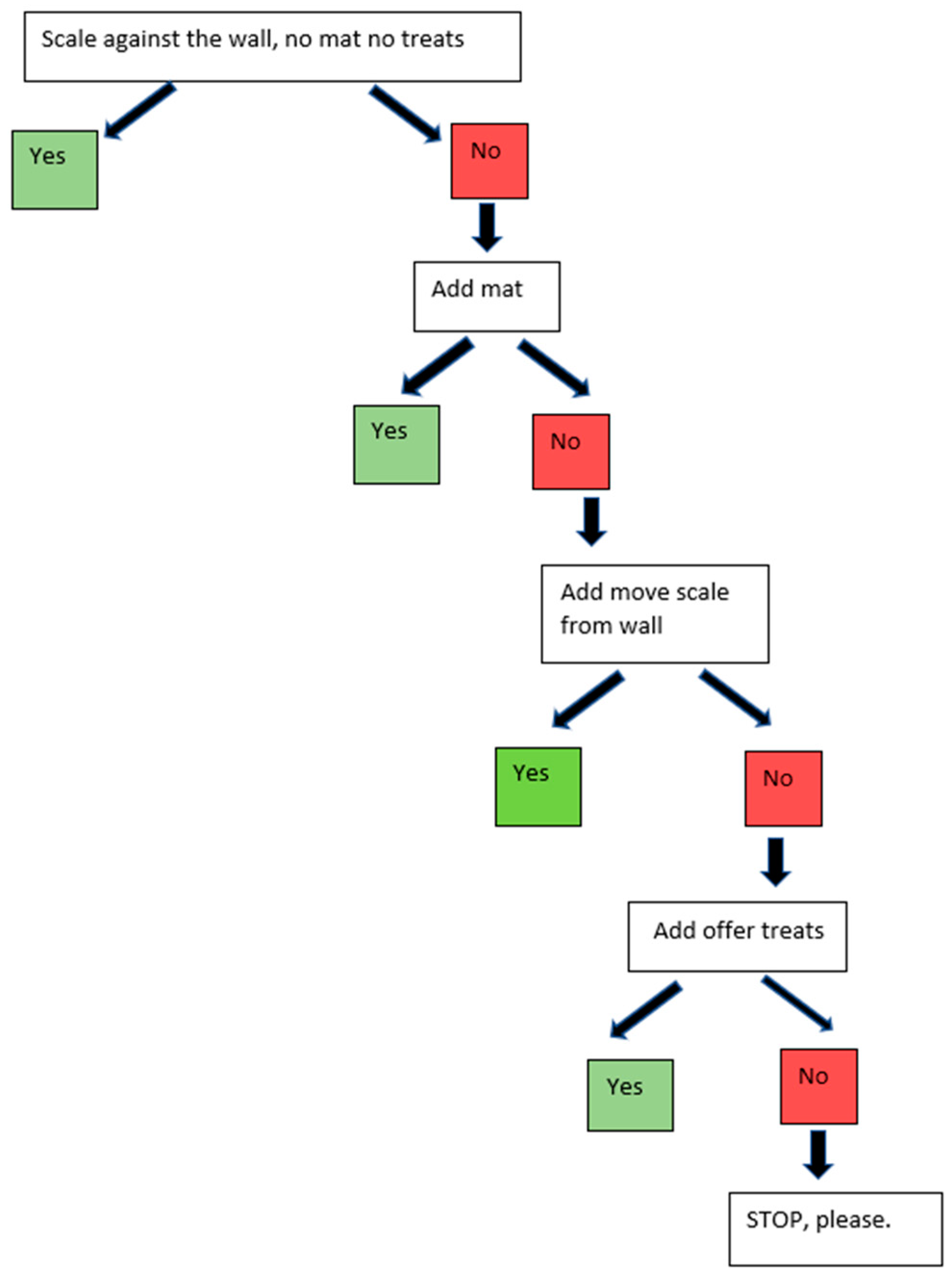
The same walk-on stainless steel scale in the same location was used for both groups and all visits. All dogs were weighed at all visits. For the control group, dogs were weighed on the scale when they first arrived for their appointment. The control group participants were asked to walk onto the bare metal scale that was placed against the wall. For the intervention group, there was a blue yoga mat on the scale, the scale was pulled away from the wall, and treats were used to lure the dog (Figure 1). If the control group dogs would not get onto the scale at any visit, the decision tree in Figure 2 was followed in a step-wise manner, and the level of intervention needed to weigh the dog was noted. Such tiered procedures are scorable for level of intervention required to obtain a weight, and thus indicate where the dog has concerns. Similar decision trees were utilized for the physical examination and blood draw portions (Figures S3 and S4).
2.3.3. Physical Exam and Blood Draw Protocols
The same exam room was used for all participants during each visit, and the physical examination and blood draw was performed by the same clinician (CS) for every participant. Both the control and intervention group received the same standardized physical examination (Table 3), which has been used in other studies assessing physical examination [32,33,40]. Owners were present throughout the physical exam and blood draw for both groups. Owners were offered chairs, and water dishes were provided for dogs. In the intervention group, the blue mat was placed in front of the owner’s chair, and they were asked to hold the Lickimat® for their pet. In both groups, owners could give treats and pets as needed, and occasionally assisted with handling (such as holding their pet in their lap if comfortable).
In the intervention group, the exam started with applying a lidocaine cream (EMLA® 2.5% lidocaine/2.5% prilocaine cream; SOLA Pharmaceuticals, Baton Rouge, LA, USA) on both the cephalic and saphenous vessel regions of the legs. For dogs that had long hair, the hair was parted to apply it to the skin. During the examination, the blue mat was placed in front of the owner and they were instructed to hold the Lickimat® for their pet (Figure 3). The Lickimat® was loaded with the dog’s preferred treats (whipped cream cheese, string cheese, Kong® cheese or liver spay, and/or freeze-dried liver or fish treats) prior to the start of the exam. All dogs in the intervention group, regardless of size, were examined on the floor, or if preferred, in their owner’s lap. For some dogs, the mat was placed on the owner’s lap for traction and comfort. Examination took place when the dog was on the mat. If they left the mat, the examination was readjusted to their preferred position to accommodate the dog’s needs. Following the physical exam, blood was drawn, and the dog was told that they were good and offered a treat. No white coat was worn for any phase of the visit for the dogs in the intervention group.
In the intervention group, a closed needle butterfly needle system (e.g., Vacutainer® Safety-LokTM blood collection and infusion set) was used to obtain the blood samples. This allowed for there to be less restraint, as the vein did not need to be held off by another team member (as is required for the open needle system routinely used in veterinary medicine), and the dog could remain in a comfortable standing position (Figure 4).
In the control group, no lidocaine was applied, no Lickimats® and food treats were used, and no soft, stabilizing blue mat was provided for the dog. Small dogs were examined on the table, and larger dogs were examined wherever clients said was routine for the dog. The clinician wore a white coat for the entirety of the visit for the dogs in the control group.
The intervention group dogs were weighed after the physical examination and blood draw were concluded, prior to exiting the reception area of the hospital into the parking lot.
All dogs, regardless of group, were offered treats at the end of the appointment while in the room, and while in the parking lot when leaving the hospital, since differential consumption of treats may be informative of the dog’s perception of the experience [41].
Because this was a study about reducing distress, a humane care exception was instituted during all appointments. If dogs became sufficiently distressed despite adjustments, further intervention such as applying lidocaine cream for the blood draw (if in the control group; N = 4) or providing anxiolytic support (Sileo®-Orion Corporation, Orion Pharma Finland, Espoo, Finland/alprazolam; N = 3 in the intervention group) was offered, with any scoring being restricted to the earlier exam. Owners were always able to withdraw from the study at any point, although none did so.
2.4. Physiological Measurements
At every visit, a blood sample was obtained to measure serum cortisol (CORT), neutrophil lymphocyte ratio (NLR), and creatine kinase (CK). At the first visit, a complete serum biochemistry and complete blood count (CBC) was obtained to ensure that the participant was healthy. The last physiological parameter measured was the dog’s heart rate (HR), which was obtained at the time of the physical exam.
CORT is considered a measure of an acute response to a stressor, reaching a peak within minutes to hours of exposure to the stressor [23]. The cortisol response can also be ongoing or chronic, and is regulated by the HPA axis. The HPA control over CORT is considered to have evolved as an adaptive homeostatic mechanism to allow recovery from stressors [23]. However, not all physiological or behavioural responses are adaptive. When such responses fail, we often see behavioural/psychiatric pathology and maladaptive responses that may signal such pathology. In such circumstances, the outcome of long-term response to stressors may be a blunted/depressed cortisol response [42,43,44,45].
Neutrophil/lymphocyte ratios (NLRs) have also been used as a measure of an individual’s response to a stressor [46,47]. Glucocorticoid (GC) increases, including increases in CORT, cause a rapid increase in neutrophils and a concomitant decrease in lymphocytes, raising the ratio. The change in leukocyte measures has been hypothesized to be adaptive in emergencies, in which combatting infection due to tissue damage is desirable [48]. Because the NLR response to GC stimulation can be delayed, NLRs may not be the most sensitive measure of short-term stressors [49], but NLRs appear to be at least constant over the duration of the stressor [48].
In general, the NLR has been found to be a reliable immunological measure of chronic stress, is relatively unaffected by handling associated with acute stress such as blood sampling or potentially confounding factors such a sex or time of day [24], and may be a good marker of sub-clinical inflammation [25]. It was used here as a complement to serum CORT measurement to provide a joint profile of relatively acute stress (the procedure) and some measure of ongoing or more chronic stress (the dog’s perception of life).
Heart rate responses, specifically tachycardia, have been used in previous studies to measure situational acute stress [50,51,52]. HR as a fear and/or stress response is due directly to activation of arousal as part of the sympathetic response originating in the locus ceruleus (LC). The LC is the primary source of norepinephrinergic (NE) neuronal activation throughout the brain in sympathetic arousal responses, and has inputs to the lateral nucleus, the basolateral nucleus and the central nucleus of the amygdala [53]. The NE produced by the LC acts to trigger somatic physiological responses to the stressor [22], largely through amygdalic stimulation. Stressors of a more ‘psychological’ nature are thought to have a more profound effect on NE release than stressors of a more physical nature such as restraint [54]. Accordingly, HR may be one measure of the individual’s perception of whether a stressor is more ‘psychological’ to the individual.
CK has been used as a plasma marker of acute muscle damage, including cardiac muscle damage [55], and muscle pain and fatigue due to exertion, acute tension, or illness [56]. In profound panic, acute muscle contraction and injury may be one component of the arousal and stress response associated with freezing [26]. Freezing with muscle contraction and increased CK has been found in dogs undergoing lactate testing for profound anxiety/panic [57].
While HR, CORT and NLR all share overlapping mechanisms initiating their response, CK evaluates a different system and is not a traditional stress response measure. It was included here to ensure that we identified any dogs experiencing panic. Table 4 summarizes the physiological markers and their specific stress measurement.
2.5. Statistical Methodology
A two-way ANOVA for repeated measures was conducted to assess differences between the control and intervention groups for HR, CORT, CK, and NLR. A Wilcoxon Mann–Whitney test was conducted to assess changes in HR, CORT, CK and NLR across the four visits within the control and intervention group.
There is no single response to any stressor. We chose three potential measures (HR, CORT, NLR) for which the physiological response to stress is well known, and one that measures muscle damage (CK). The effect on the individual is a combined measure of all response patterns. We attempted to assess the combined effect of the stress response indicators experienced by the dogs by creating a dimensionless composite index, the stress response index, that included summed standardized measures for HR, CORT and NLR, using a winsorizing process that removed extreme outliers. Paired t-tests were used to test for differences between the first and fourth visit.
3. Results
3.1. Changes between Control and Intervention Groups
There were no significant differences between the control and intervention groups for HR, CORT, CK, and NLR for each visit.
3.2. Changes within Control and Intervention Groups
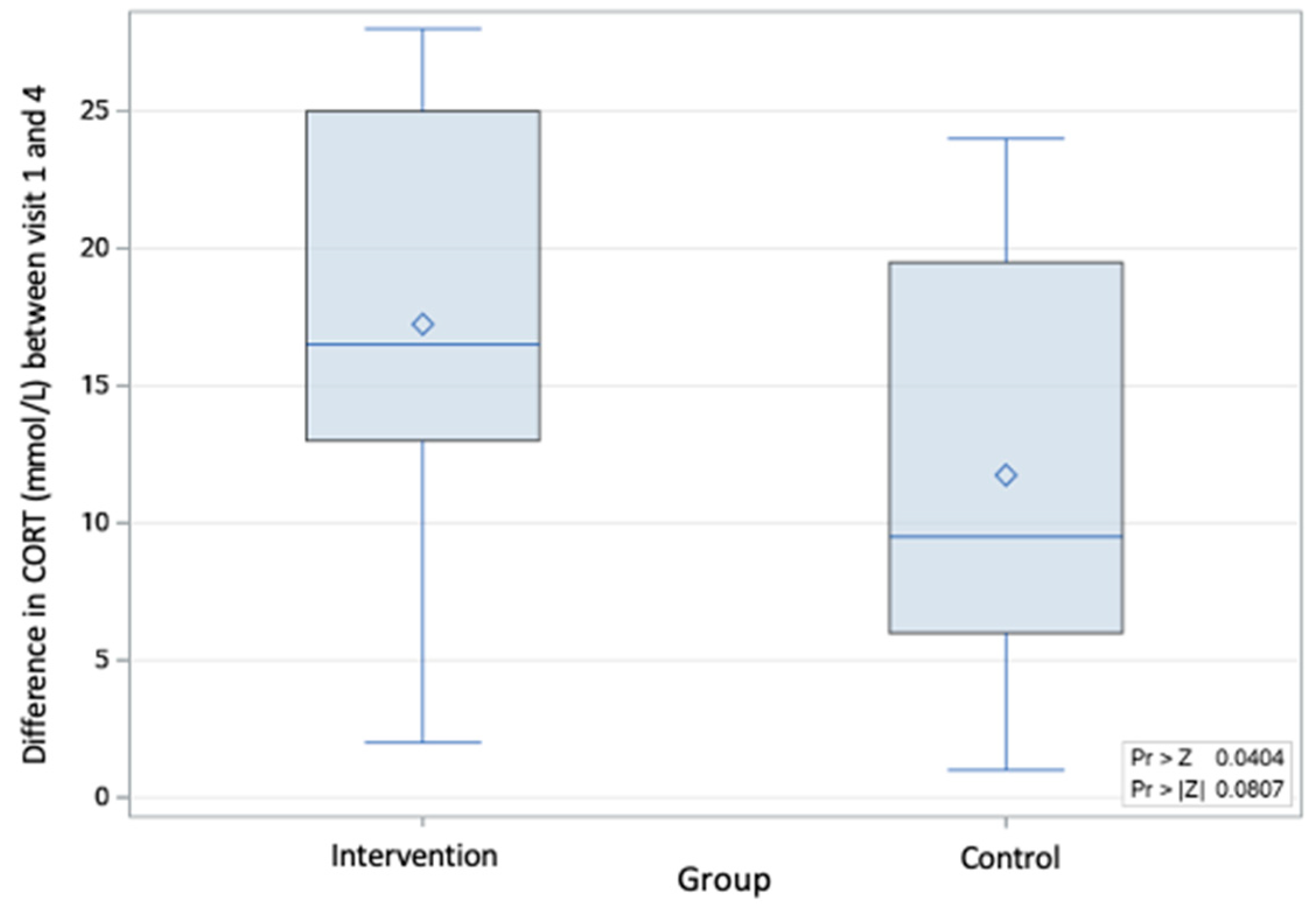
The probability associated with the overall change from the first to fourth visit in cortisol was p < 0.08 (based on a Wilcoxon Mann–Whitney test: Z = 1.75). However, when comparing the changes between the first and last visit, the intervention group had a greater reduction in serum cortisol compared to the control group, with a probability of p < 0.04 (Wilcoxon Mann–Whitney test: Z = 1.75). (Figure 5 and Figure 6).
When assessing the other physiological variables (HR, CK, NLR), there was no significant difference between the groups for the change in values from the first to the last visit. Although there was an observed decrease in HR (Wilcoxon Mann–Whitney test: Z = 0.89; p < 0.37, two-tail test; p < 0.18, one-tail test) and NLR (Wilcoxon Mann–Whitney test: Z = 0.07; p < 0.94, two-tail test; p < 0.47, two-tail test) from the first to the last visit in both groups, the differences were not statistically significant.
3.3. Stress Response Index
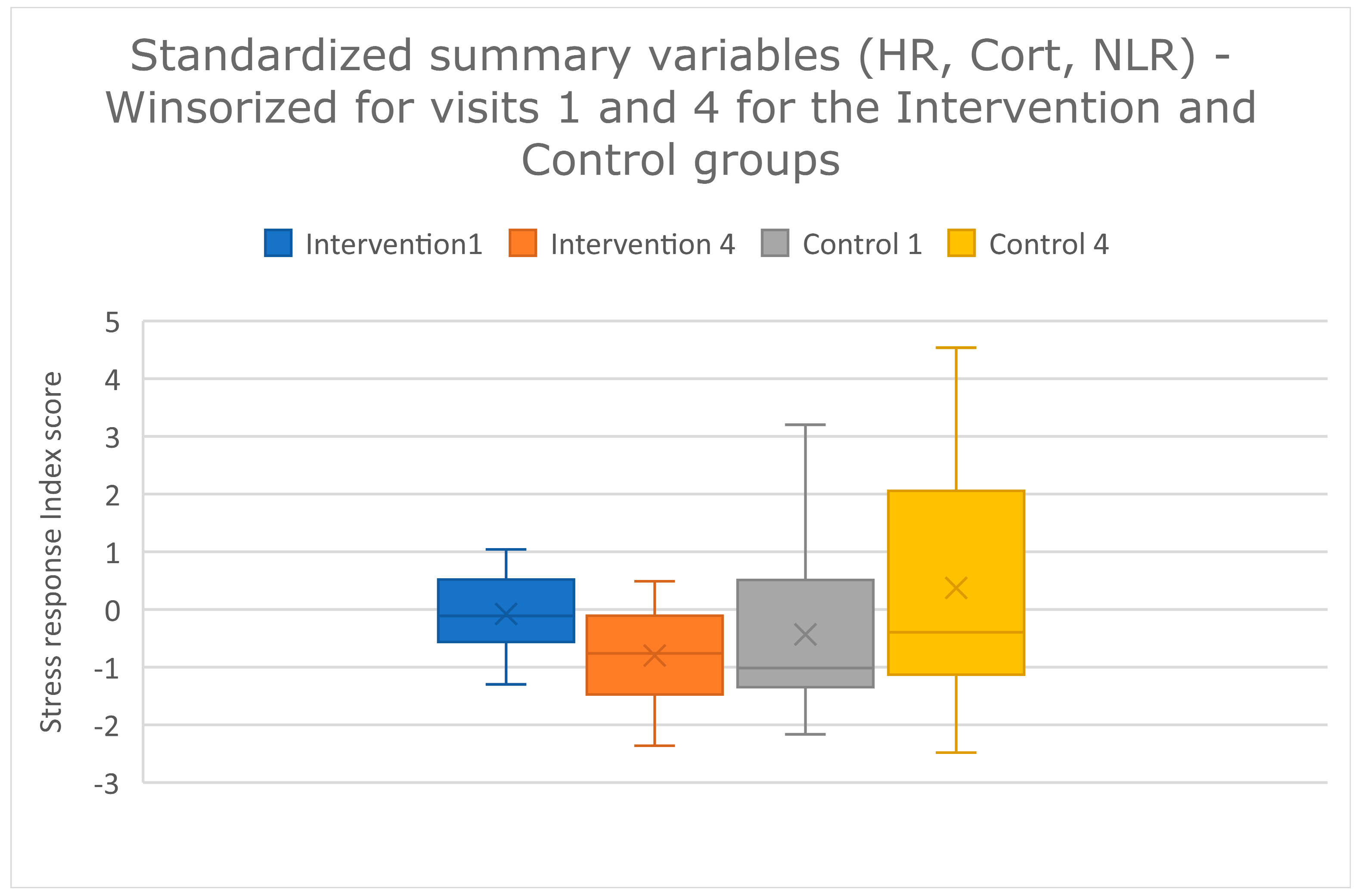
The stress response index was compared between visits one and four. The index did not differ between the first and last visit for the control group, but did differ between the first and last visit for the intervention group (paired t-tests: intervention t-value = 2.37; p = 0.027; control t-value = −1.12; p = 0.29) (Figure 7). The effect size is approximately 1, which is considered a large effect (Cohen’s d = (−0.80–−0.08)/0.72 = 0.99. Glass’s delta = (−0.80–−0.08)/0.65 = 1.12. Hedges’ g = (−0.80–−0.08)/0.73 = 0.99).
4. Discussion
The overall goal of this study was to assess whether canine patients that received a veterinary examination designed to minimize stress and fear, and that was collaborative and adaptive to the dogs’ needs, had a greater reduction in distress across four veterinary visits compared to those that received routine handling methods. The targeted low-stress interventions were simple and practical, and were specifically selected so that they could easily be implemented into a busy veterinary practice. Rather than selecting one parameter to assay, such as not wearing a white coat, we altered as much of the entire visit and examination procedure as we could to provide opportunities for adaptive and collaborative care, and pain and anxiety relief. The dog’s experience is the entire visit, not compartmentalized segments. Accordingly, we cannot attribute any of our results to any one intervention, but instead show what happened across four visits over 8 weeks.
No difference was observed between the control and intervention groups for the physiological parameters for each visit. A possible explanation is the large variability within the study population, including baseline anxiety and fear when entering the study. This led to a wide range of individual responses for all physiological values, and a large degree of overlap between each group. It is also important to note that four visits across 8 weeks is a relatively short time in the life of a dog. Regardless, both the intervention and control groups experienced a decrease in serum cortisol when the first and last visits were compared; however, the intervention group had a significantly greater reduction in serum cortisol compared to the control group, by the last visit. This finding suggests that dogs that experienced adaptive, collaborative care and low-stress intervention techniques throughout all four veterinary visits had a greater reduction in stress over time, an effect that may be magnified were such interventions routine. Serum cortisol has been used in numerous studies as a physiological measurement of acute stress in dogs [6,58,59]. It is important to note that a lack of an increase in serum cortisol in a patient does not necessarily mean that acute stress was not experienced. For example, if the animal was experiencing chronic stress, acute stress measures may be blunted [45]. In humans and animals that experience chronic stress, repeated surges of cortisol can result in cortisol dysfunction, which may include depletion of cortisol, insufficient free (unbound) cortisol, impaired cortisol secretion, and/or glucocorticoid receptor resistance [60]. Therefore, it is possible that some of the dogs in the study had blunted cortisol values while still experiencing the same level of stress of those that showed the increased serum cortisol concentration. This phenomenon will be investigated further when combining the behavioural scores and historical data, as it will hopefully help to reveal those individuals whose stress may have been undervalued in this initial data analysis.
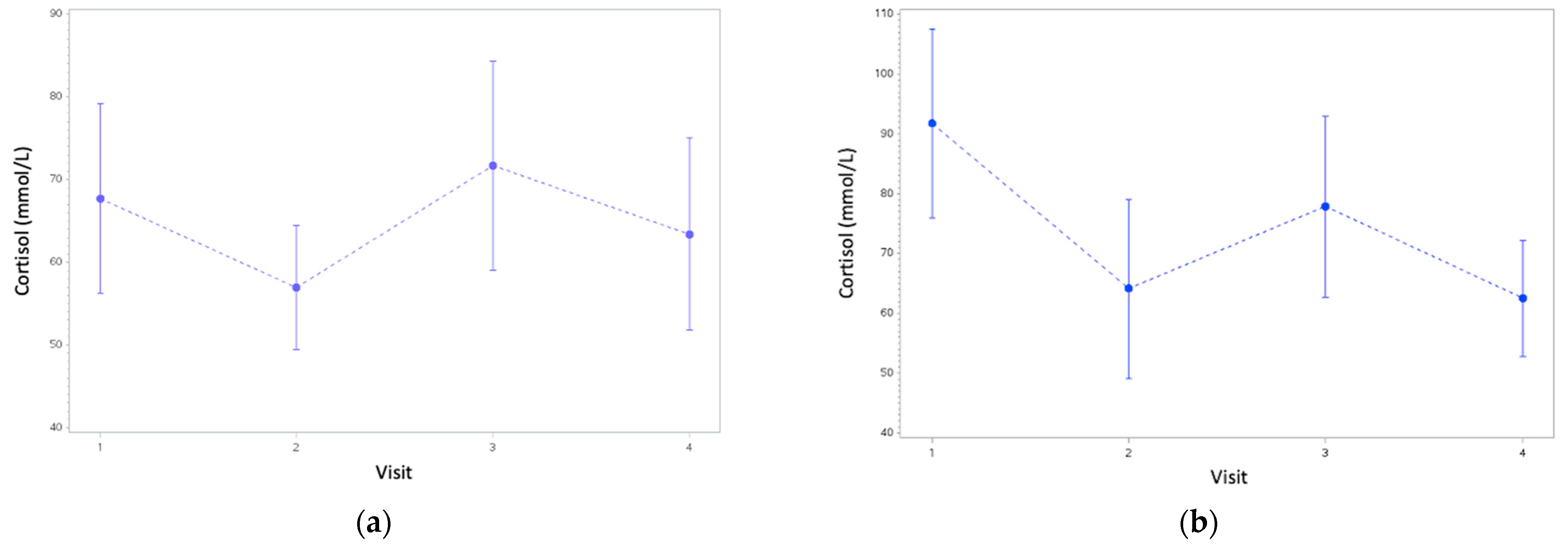
For both groups, there was an increase in serum cortisol in the second visit, followed by a decrease at the third. This may be explained by an initial period of sensitization in the dogs, followed by a period of habituation [61]. The pattern of serum cortisol over time suggests that that both groups experienced a degree of habituation across the four visits, but the effect was greater for the intervention group. The intervention group significantly improved when comparing the last visit to the first visit using the stress response index, but the control group showed a non-significant worsening of response. This result suggests that members in the control group could have been sensitized across the visits, in the absence of any of the calming techniques that the intervention group experienced.
The stress response index also differed significantly between the first and last visit, but only for the intervention group. The effect size is approximately 1, suggesting that the effect is real, and possibly important, especially since there was a non-significant pattern of the composite stress index worsening at the last visit compared with the first visit in the control group. The non-significant increase in the stress response index for the control group may suggest that when the combined effect of all physiological responses was examined, dogs may have been experiencing some sensitization to repeated visits. Composite scores may be a valuable tool for understanding the global effects of multiple integrated physiological systems.
The decision to have limited inclusion criteria was important, as the study population aimed to represent the real-life patient population found within veterinary clinics. The study groups successfully mirrored the large variety observed within the AVC setting (and most participants were drawn from AVC patients), including a wide range of breeds, sizes, and histories, in addition to varying baselines of anxiety and fear. A representative population of patients was solicited for participation rather than choosing a group of standard age, size, breed and/or background, to render the outcome more applicable to our patients. Accordingly, our results were highly variable. The size of the dogs alone ranged from a 3 kg Chihuahua to a 64 kg Labrador retriever. The dogs in the study also had a range of veterinary experiences, most of which we could not quantify, which could have contributed to their anxiety and fear. Despite the variability, greater improvement was observed in dogs that received low-stress interventions.
Because we aimed to not cause extreme duress in the study participants, some degree of an adaptive exam was available to all patients. For one participant, this meant going outside the building for the blood draw so that they would not feel confined in the exam room, and for others, this meant using other intervention methods such as lidocaine cream, even for patients in the control group (N = 4), or anxiolytic medication (alprazolam or Sileo®) (N = 3 in the intervention group) [62]. These interventions occurred when the initial treatment for their group, plus routine adjustments (including using treats, adjusting locations, providing breaks, and using other tools such as towels) as outlined in the procedure decision trees, was unsuccessful (Figures S4 and S5). The last possible intervention offered was Sileo®, an oral dexmedetomidine gel. This medication is an alpha-2 agonist that blunts the release of norepinephrine from the locus ceruleus within the brain and has been used successfully in hospital settings to reduce fear and anxiety in patients [32,33,63]. Sileo® can lower HR, so it is possible that the three participants who received it (all of whom were in the intervention group) may have experienced a very slightly lower HR as a result. In a repeated measures design, each dog acts as its own control, which is inherent in the statistical analysis. These dogs fell well within the variation for other dogs in this group at each assessment (they were not outliers) The dogs in the control group that received lidocaine cream for venepuncture may have experienced beneficial alterations in their physiological values, yet from the first to the last visit, the control group worsened. The effects of the interventions on NLR and CORT are less likely, as the laboratory effects we measured have long half-lives. Behavioural effects, not discussed here, are possible. We wanted to fully disclose this humane care usage.
For both groups, the owners were present throughout the entire appointment, including for the physical exam and blood draw. For the control group, the protocol aimed to match what patients at AVC would typically experience, but having the owner present deviated from the AVC protocol. At AVC, it is standard to remove patients from their owners and take the patient into a hospital treatment room for these procedures. Pets who are able to stay with their owners during examination or other stressful procedures show fewer and lesser signs of distress [10,18,52]. Because we allowed both groups to be with their owners, this likely affected—and lessened—the level of stress the control group members experienced, versus what is experienced by many dogs and cats routinely at veterinary clinics when separated.
Other limitations included an inability to completely blind the study. Because of the specific protocols and tools required for each group, it was impossible to blind researchers to what group the participants were assigned to. All possible actions were taken to reduce biases. The owners of the dogs did not know which group they were in until the very end, although it is possible that they surmised their group given on the homework and appointment protocols they experienced. Regardless, the laboratory technicians running the blood tests were blinded to the group status of each blood sample.
5. Conclusions
The aim of this study was to determine whether interventions affected measurements of distress at the veterinary clinic in canine patients. The initial findings from the physiological data presented suggest that patients receiving low-stress intervention techniques during veterinary visits have a greater reduction in stress over time compared to those without interventions. The use of composite scores such as the stress response index may be a valuable tool for understanding the global effects of multiple integrated physiological systems. Further analyses will investigate the relationship of these findings with behavioural scores and historical data.
Supplementary Materials
The following supporting information can be downloaded at: www.mdpi.com/article/10.3390/ani13071253/s1, Figure S1: WDQ-Pet questionnaire, Figure S2: Homework assigned for intervention group, Figure S3: Homework assigned for control group, Figure S4: Decision tree for physical examination protocol, Figure S5: Decision tree for physical examination protocol, Table S1: Likert Scale, Video S1: Group 1 Homework Video–Control, Video S2: Group 2 Homework Video–Intervention.
Author Contributions
Conceptualization K.L.O. and C.S.; formal analysis K.L.O., W.M. and C.S.; funding acquisition K.L.O.; investigation C.S. and K.L.O.; methodology C.S., K.L.O., K.P. and W.M.; project administration C.S. and K.L.O.; supervision K.L.O.; writing—original draft C.S.; writing—review and editing K.L.O., K.P. and W.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research was fully funded by a grant from the Sir James Dunn Animal Welfare Centre at the Atlantic Veterinary College to KLO (SJDAWC 2021 6009007). UPEI and VIN provided additional support to CS.
Institutional Review Board Statement
The animal study protocol was approved by the Animal Care Committee (ACC) and the Research Ethics Board (REB) of UPEI (Protocol 21-02; 19 May 2021).
Informed Consent Statement
Written informed consent was obtained from all dog owners involved in the study, and they could withdraw from the study at any time.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to the ethical agreement with the participants that only anonymized, summary data would be publicly presented.
Acknowledgments
The authors would like to thank Lickimat® for donating their product for this research study, and the student volunteers and summer research students for their assistance in the examinations and video recording. We would also like to thank the dog owners and their dogs for their participation for this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Döring, D.; Roscher, A.; Scheipl, F.; Küchenhoff, H.; Erhard, M.H. Fear-Related Behaviour of Dogs in Veterinary Practice. Vet. J. 2009, 182, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Stanford, T.L. Behavior of Dogs Entering a Veterinary Clinic. Appl. Anim. Ethol. 1981, 7, 271–279. [Google Scholar] [CrossRef]
- Mariti, C.; Raspanti, E.; Zilocchi, M.; Carlone, B.; Gazzano, A. The Assessment of Dog Welfare in the Waiting Room of a Veterinary Clinic. Anim. Welf. 2015, 24, 299–305. [Google Scholar] [CrossRef]
- Hernander, L. Factors Influencing Dogs’ Stress Level in the Waiting Room at a Veterinary Clinic; Student Report; Department of Animal Environment and Health, Swedish University of Agricultural Sciences: Skara, Sweden, 2008; ISSN 1652-280X. [Google Scholar]
- Mariti, C.; Pierantoni, L.; Sighieri, C.; Gazzano, A. Guardians’ Perceptions of Dogs’ Welfare and Behaviors Related to Visiting the Veterinary Clinic. J. Appl. Anim. Welf. Sci. 2017, 20, 24–33. [Google Scholar] [CrossRef]
- Perego, R.; Proverbio, D.; Spada, E. Increases in Heart Rate and Serum Cortisol Concentrations in Healthy Dogs Are Positively Correlated with an Indoor Waiting-Room Environment. Vet. Clin. Pathol. 2014, 43, 67–71. [Google Scholar] [CrossRef] [Green Version]
- Stellato, A.C.; Hoffman, H.; Gowland, S.; Dewey, C.E.; Widowski, T.M.; Niel, L. Effect of High Levels of Background Noise on Dog Responses to a Routine Physical Examination in a Veterinary Setting. Appl. Anim. Behav. Sci. 2019, 214, 64–71. [Google Scholar] [CrossRef]
- Stellato, A.C.; Flint, H.E.; Dewey, C.E.; Widowski, T.M.; Niel, L. Risk-Factors Associated with Veterinary-Related Fear and Aggression in Owned Domestic Dogs. Appl. Anim. Behav. Sci. 2021, 241, 105374. [Google Scholar] [CrossRef]
- Dreschel, N.A. The Effects of Fear and Anxiety on Health and Lifespan in Pet Dogs. Appl. Anim. Behav. Sci. 2010, 125, 157–162. [Google Scholar] [CrossRef]
- Edwards, P.T.; Smith, B.P.; McArthur, M.L.; Hazel, S.J. Fearful Fido: Investigating Dog Experience in the Veterinary Context in an Effort to Reduce Distress. Appl. Anim. Behav. Sci. 2019, 213, 14–25. [Google Scholar] [CrossRef]
- Moberg, G.P. Biological Response to Stress: Implications for Animal Welfare. In The Biology of Animal Stress: Basic Principles and Implications for Animal Welfare; CABI Books: Wallingford, UK, 2000; ISBN 9780851993591. [Google Scholar]
- Gouin, J.-P.; Kiecolt-Glaser, J.K. The Impact of Psychological Stress on Wound Healing: Methods and Mechanisms. Immunol. Allergy Clin. N. Am. 2011, 31, 81–93. [Google Scholar] [CrossRef] [Green Version]
- Dhabhar, F.S. Enhancing versus Suppressive Effects of Stress on Immune Function: Implications for Immunoprotection and Immunopathology. Neuroimmunomodulation 2009, 16, 300–317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Volk, J.O.; Felsted, K.E.; Thomas, J.G.; Siren, C.W. Executive Summary of the Bayer Veterinary Care Usage Study. J. Am. Vet. Med. Assoc. 2011, 238, 1275–1282. [Google Scholar] [CrossRef] [PubMed]
- Overall, K.L. Embracing Behavior as a Core Disipline: Creating the Behavior-Centered Practice. In Manual of Clinical Behavioral Medicine for Dogs and Cats; Elsevier: St. Louis, MO, USA, 2013; pp. 2–44. ISBN 978-0-323-00890-7. [Google Scholar]
- Lloyd, J. Minimising Stress for Patients in the Veterinary Hospital: Why It Is Important and What Can Be Done about It. Vet. Sci. 2017, 4, 22. [Google Scholar] [CrossRef] [Green Version]
- Riemer, S.; Heritier, C.; Windschnurer, I.; Pratsch, L.; Arhant, C.; Affenzeller, N. A Review on Mitigating Fear and Aggression in Dogs and Cats in a Veterinary Setting. Animals 2021, 11, 158. [Google Scholar] [CrossRef] [PubMed]
- Mandese, W.W.; Griffin, F.C.; Reynolds, P.S.; Blew, A.C.; Deriberprey, A.S.; Estrada, A.H. Stress in Client-owned Dogs Related to Clinical Exam Location: A Randomised Crossover Trial. J. Small Anim. Pract. 2021, 62, 82–88. [Google Scholar] [CrossRef]
- Overall, K.L. Evidence-Based Paradigm Shifts in Veterinary Behavioral Medicine. J. Am. Vet. Med. Assoc. 2019, 254, 798–807. [Google Scholar] [CrossRef]
- Stellato, A.; Jajou, S.; Dewey, C.E.; Widowski, T.M.; Niel, L. Effect of a Standardized Four-Week Desensitization and Counter-Conditioning Training Program on Pre-Existing Veterinary Fear in Companion Dogs. Animals 2019, 9, 767. [Google Scholar] [CrossRef] [Green Version]
- Godbout, M.; Frank, D. Persistence of Puppy Behaviors and Signs of Anxiety during Adulthood. J. Vet. Behav. 2011, 6, 92. [Google Scholar] [CrossRef]
- Goddard, A.W.; Ball, S.G.; Martinez, J.; Robinson, M.J.; Yang, C.R.; Russell, J.M.; Shekhar, A. Current Perspectives of the Roles of the Central Norepinephrine System in Anxiety and Depression. Depress. Anxiety 2010, 27, 339–350. [Google Scholar] [CrossRef]
- Mormède, P.; Andanson, S.; Aupérin, B.; Beerda, B.; Guémené, D.; Malmkvist, J.; Manteca, X.; Manteuffel, G.; Prunet, P.; van Reenen, C.G.; et al. Exploration of the Hypothalamic–Pituitary–Adrenal Function as a Tool to Evaluate Animal Welfare. Physiol. Behav. 2007, 92, 317–339. [Google Scholar] [CrossRef]
- Hickman, D.L. Evaluation of the Neutrophil:Lymphocyte Ratio as an Indicator of Chronic Distress in the Laboratory Mouse. Lab Anim. 2017, 46, 303–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isaac, V.; Wu, C.-Y.; Huang, C.-T.; Baune, B.T.; Tseng, C.-L.; McLachlan, C.S. Elevated Neutrophil to Lymphocyte Ratio Predicts Mortality in Medical Inpatients with Multiple Chronic Conditions. Medicine 2016, 95, e3832. [Google Scholar] [CrossRef]
- Grillon, C.; Ameli, R.; Goddard, A.; Woods, S.W.; Davis, M. Baseline and Fear-Potentiated Startle in Panic Disorder Patients. Biol. Psychiatry 1994, 35, 431–439. [Google Scholar] [CrossRef] [PubMed]
- Meltzer, H. Plasma Creatine Phosphokinase Activity, Hypothermia, and Stress. Am. J. Physiol.-Leg. Content 1971, 221, 896–901. [Google Scholar] [CrossRef]
- Overall, K.L.; Dunham, A.E.; Juarbe-Diaz, S.V. Phenotypic Determination of Noise Reactivity in 3 Breeds of Working Dogs: A Cautionary Tale of Age, Breed, Behavioral Assessment, and Genetics. J. Vet. Behav. 2016, 16, 113–125. [Google Scholar] [CrossRef] [Green Version]
- Overall, K.L.; Dunham, A.E.; Scheifele, P.; Sonstrom Malowski, K. Fear of Noises Affects Canine Problem Solving Behavior and Locomotion in Standardized Cognitive Tests. Appl. Anim. Behav. Sci. 2019, 221, 104863. [Google Scholar] [CrossRef]
- Bryant, D.A.; Dunham, A.E.; Overall, K.L. Roles for Referential Focus in Effective and Efficient Canine Signaling: Do Pet and Working Dogs Differ? J. Vet. Behav. 2018, 27, 55–66. [Google Scholar] [CrossRef]
- Kolevská, J.; Brunclík, V.; Svoboda, M. Circadian Rhythm of Cortisol Secretion in Dogs of Different Daily Activities. Acta Vet. Brno 2003, 72, 599–605. [Google Scholar] [CrossRef]
- Korpivaara, M.; Huhtinen, M.; Aspegrén, J.; Overall, K. Dexmedetomidine Oromucosal Gel Reduces Fear and Anxiety in Dogs during Veterinary Visits: A Randomised, Double-blind, Placebo-controlled Clinical Pilot Study. Vet. Rec. 2021, 189, e832. [Google Scholar] [CrossRef] [PubMed]
- Hauser, H.; Campbell, S.; Korpivaara, M.; Stefanovski, D.; Quinlan, M.; Siracusa, C. In-Hospital Administration of Dexmedetomidine Oromucosal Gel for Stress Reduction in Dogs during Veterinary Visits: A Randomized, Double-Blinded, Placebo-Controlled Study. J. Vet. Behav. 2020, 39, 77–85. [Google Scholar] [CrossRef]
- Marino, C.L.; Cober, R.E.; Iazbik, M.C.; Couto, C.G. White-Coat Effect on Systemic Blood Pressure in Retired Racing Greyhounds: Blood Pressure in Retired Racing Greyhounds. J. Vet. Intern. Med. 2011, 25, 861–865. [Google Scholar] [CrossRef]
- Haskard-Zolnierek, K.; Cobos, B.; Howard, K. White Coat Hypertension: Improving the Patient–Health Care Practitioner Relationship. Psychol. Res. Behav. Manag. 2015, 8, 133. [Google Scholar] [CrossRef] [Green Version]
- Westlund, K. To Feed or Not to Feed: Counterconditioning in the Veterinary Clinic. J. Vet. Behav. 2015, 10, 433–437. [Google Scholar] [CrossRef]
- Crisi, P.E.; De Santis, F.; Giordano, M.V.; Cerasoli, I.; Colucci, F.; Di Tommaso, M.; Luciani, A. Evaluation of Eutectic Lidocaine/Prilocaine Cream for Jugular Blood Sampling in Cats. J. Feline Med. Surg. 2021, 23, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Van Oostrom, H.; Knowles, T.G. The Clinical Efficacy of EMLA Cream for Intravenous Catheter Placement in Client-Owned Dogs. Vet. Anaesth. Analg. 2018, 45, 604–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paediatric and Neonatal Blood Sampling. In WHO Guidelines on Drawing Blood: Best Practices in Phlebotomy; World Health Organization: Geneva, Switzerland, 2010.
- Godbout, M.; Palestrini, C.; Beauchamp, G.; Frank, D. Puppy Behavior at the Veterinary Clinic: A Pilot Study. J. Vet. Behav. 2007, 2, 126–135. [Google Scholar] [CrossRef]
- Lind, A.-K.; Hydbring-Sandberg, E.; Forkman, B.; Keeling, L.J. Assessing Stress in Dogs during a Visit to the Veterinary Clinic: Correlations between Dog Behavior in Standardized Tests and Assessments by Veterinary Staff and Owners. J. Vet. Behav. 2017, 17, 24–31. [Google Scholar] [CrossRef]
- Huber, T.J.; Issa, K.; Schik, G.; Wolf, O.T. The Cortisol Awakening Response Is Blunted in Psychotherapy Inpatients Suffering from Depression. Psychoneuroendocrinology 2006, 31, 900–904. [Google Scholar] [CrossRef]
- Dauvermann, M.R.; Donohoe, G. Cortisol Stress Response in Psychosis from the High-Risk to the Chronic Stage: A Systematic Review. Ir. J. Psychol. Med. 2019, 36, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Lam, J.C.W.; Shields, G.S.; Trainor, B.C.; Slavich, G.M.; Yonelinas, A.P. Greater Lifetime Stress Exposure Predicts Blunted Cortisol but Heightened DHEA Responses to Acute Stress. Stress Health 2019, 35, 15–26. [Google Scholar] [CrossRef] [Green Version]
- Cobb, M.L.; Iskandarani, K.; Chinchilli, V.M.; Dreschel, N.A. A Systematic Review and Meta-Analysis of Salivary Cortisol Measurement in Domestic Canines. Domest. Anim. Endocrinol. 2016, 57, 31–42. [Google Scholar] [CrossRef] [PubMed]
- Beerda, B.; Schilder, M.B.H.; Bernadina, W.; Van Hooff, J.A.R.A.M.; De Vries, H.W.; Mol, J.A. Chronic Stress in Dogs Subjected to Social and Spatial Restriction. II. Hormonal and Immunological Responses. Physiol. Behav. 1999, 66, 243–254. [Google Scholar] [CrossRef] [PubMed]
- Carbillet, J.; Rey, B.; Lavabre, T.; Chaval, Y.; Merlet, J.; Débias, F.; Régis, C.; Pardonnet, S.; Duhayer, J.; Gaillard, J.-M.; et al. The Neutrophil to Lymphocyte Ratio Indexes Individual Variation in the Behavioural Stress Response of Wild Roe Deer across Fluctuating Environmental Conditions. Behav. Ecol. Sociobiol. 2019, 73, 144. [Google Scholar] [CrossRef]
- Goessling, J.M.; Kennedy, H.; Mendonça, M.T.; Wilson, A.E. A Meta-analysis of Plasma Corticosterone and Heterophil: Lymphocyte Ratios—Is There Conservation of Physiological Stress Responses over Time? Funct. Ecol. 2015, 29, 1189–1196. [Google Scholar] [CrossRef]
- Sapolsky, R.M.; Romero, L.M.; Munck, A.U. How Do Glucocorticoids Influence Stress Responses? Integrating Permissive, Suppressive, Stimulatory, and Preparative Actions*. Endocr. Rev. 2000, 21, 55–89. [Google Scholar] [CrossRef] [Green Version]
- Edwards, P.T.; Smith, B.P.; McArthur, M.L.; Hazel, S.J. At the Heart of a Dog’s Veterinary Experience: Heart Rate Responses in Dogs Vary across a Standard Physical Examination. J. Vet. Behav. 2022, 51, 23–34. [Google Scholar] [CrossRef]
- Csoltova, E.; Martineau, M.; Boissy, A.; Gilbert, C. Behavioral and Physiological Reactions in Dogs to a Veterinary Examination: Owner-Dog Interactions Improve Canine Well-Being. Physiol. Behav. 2017, 177, 270–281. [Google Scholar] [CrossRef]
- Stellato, A.C.; Dewey, C.E.; Widowski, T.M.; Niel, L. Evaluation of Associations between Owner Presence and Indicators of Fear in Dogs during Routine Veterinary Examinations. J. Am. Vet. Med. Assoc. 2020, 257, 1031–1040. [Google Scholar] [CrossRef]
- Davis, M. Neurobiology of Fear Responses: The Role of the Amygdala. J. Neuropsychiatry Clin. Neurosci. 1997, 9, 382–402. [Google Scholar] [CrossRef]
- Pacák, K.; Palkovits, M. Stressor Specificity of Central Neuroendocrine Responses: Implications for Stress-Related Disorders. Endocr. Rev. 2001, 22, 502–548. [Google Scholar] [CrossRef] [Green Version]
- Jaffe, A.S.; Garfinkel, B.T.; Ritter, C.S.; Sobel, B.E. Plasma Mb Creatine Kinase after Vigorous Exercise in Professional Athletes. Am. J. Cardiol. 1984, 53, 856–858. [Google Scholar] [CrossRef] [PubMed]
- Orsucci, D.; Trezzi, M.; Anichini, R.; Blanc, P.; Barontini, L.; Biagini, C.; Capitanini, A.; Comeglio, M.; Corsini, P.; Gemignani, F.; et al. Increased Creatine Kinase May Predict A Worse COVID-19 Outcome. J. Clin. Med. 2021, 10, 1734. [Google Scholar] [CrossRef] [PubMed]
- Overall, K.; Dunham, A.; Acland, G. Responses of Genetically Fearful Dogs to the Lactate Test: Assessment of the Test as Provocative Index and Application in Mechanistic Diagnoses. Mol. Psychiatry 1999, 4, S125. [Google Scholar]
- Yuki, M.; Aoyama, R.; Hirano, T.; Tawada, R.; Ogawa, M.; Naitoh, E.; Kainuma, D.; Nagata, N. Investigation of Serum Cortisol Concentration as a Potential Prognostic Marker in Hospitalized Dogs: A Prospective Observational Study in a Primary Care Animal Hospital. BMC Vet. Res. 2019, 15, 170. [Google Scholar] [CrossRef]
- Hekman, J.; Karas, A.; Sharp, C. Psychogenic Stress in Hospitalized Dogs: Cross Species Comparisons, Implications for Health Care, and the Challenges of Evaluation. Animals 2014, 4, 331–347. [Google Scholar] [CrossRef]
- Hannibal, K.E.; Bishop, M.D. Chronic Stress, Cortisol Dysfunction, and Pain: A Psychoneuroendocrine Rationale for Stress Management in Pain Rehabilitation. Phys. Ther. 2014, 94, 1816–1825. [Google Scholar] [CrossRef] [PubMed]
- Domjan, M. Elicited Behavior, Habituation, and Sensitization. In The Principles of Learning and Behavior; Domjan, M., Ed.; Cengage Learning: Stamford, CT, USA, 2015; pp. 29–58. ISBN 978-1-285-08856-3. [Google Scholar]
- Erickson, A.; Harbin, K.; MacPherson, J.; Rundle, K.; Overall, K.L. A Review of Pre-Appointment Medications to Reduce Fear and Anxiety in Dogs and Cats at Veterinary Visits. Can. Vet. J. 2021, 62, 952–960. [Google Scholar]
- Korpivaara, M.; Laapas, K.; Huhtinen, M.; Schöning, B.; Overall, K. Dexmedetomidine Oromucosal Gel for Noise-Associated Acute Anxiety and Fear in Dogs-a Randomised, Double-Blind, Placebo-Controlled Clinical Study. Vet. Rec. 2017, 180, 356. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
(a) Scale set up for control group and (b) intervention group. The scale procedure for the control group occurred at the beginning of the appointment; for the intervention group, it occurred at the end of the appointment.
Figure 1.
(a) Scale set up for control group and (b) intervention group. The scale procedure for the control group occurred at the beginning of the appointment; for the intervention group, it occurred at the end of the appointment.

Figure 2.
Decision tree for scale procedure for control group (noting the level at which they could be weighed at each visit).
Figure 2.
Decision tree for scale procedure for control group (noting the level at which they could be weighed at each visit).

Figure 3.
(a) Physical exam example for control group and (b) intervention group.

Figure 4.
(a) Blood collection example for control group and (b) intervention group.

Figure 5.
Non-parametric comparison assessing the change in cortisol from the first to fourth visit within the intervention and control groups. The box and whisker plots show the means (rhombus), the medians (lines), and the values for 75% of index scores (whiskers) for each group.
Figure 5.
Non-parametric comparison assessing the change in cortisol from the first to fourth visit within the intervention and control groups. The box and whisker plots show the means (rhombus), the medians (lines), and the values for 75% of index scores (whiskers) for each group.

Figure 6.
Cortisol values from the first to fourth visit for (a) the control group and (b) the intervention group.
Figure 6.
Cortisol values from the first to fourth visit for (a) the control group and (b) the intervention group.

Figure 7.
Stress response index score; Summed, standardized measures for HR, CORT and NLR for the first and last visit within the intervention and control groups, as noted in the key on the graph, after data were winsorized. The index score is on the Y axis. Groups are colour-coded by treatment (intervention v. control and visit number (1 v. 4). The box and whisker plots show the means (×), the medians (lines), and the values for 75% of index scores (whiskers) for each group.
Figure 7.
Stress response index score; Summed, standardized measures for HR, CORT and NLR for the first and last visit within the intervention and control groups, as noted in the key on the graph, after data were winsorized. The index score is on the Y axis. Groups are colour-coded by treatment (intervention v. control and visit number (1 v. 4). The box and whisker plots show the means (×), the medians (lines), and the values for 75% of index scores (whiskers) for each group.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Subject signalment, group, and study completion status (MC = male, castrated; MI = male, intact; FS = female, spayed; FI = female, intact).
Table 1.
Subject signalment, group, and study completion status (MC = male, castrated; MI = male, intact; FS = female, spayed; FI = female, intact).
| ID | Age in Months | Sex | Breed | Weight | Group | Status |
|---|---|---|---|---|---|---|
| 01 | 76 mo | MC | Dachshund | 7.2 kg | Control | Completed |
| 02 | 35 mo | FS | Chihuahua mix | 5.4 kg | Control | Withdrawn |
| 03 | 102 mo | MC | German Shepherd/Husky mix | 30.2 kg | Control | Completed |
| 04 | 46 mo | MC | Springer Spaniel mix | 19.2 kg | Intervention | Completed |
| 05 | 61 mo | FS | Beagle | 13.2 kg | Control | Completed |
| 06 | 73 mo | FS | Shih Tzu mix | 8.2 kg | Control | Completed |
| 07 | 31 mo | MC | Pitbull mix | 30.4 kg | Intervention | Completed |
| 08 | 120 mo | MC | Dalmatian | 27.0 kg | Intervention | Completed |
| 09 | 31 mo | MC | Bernese Mountain Dog | 38.8 kg | Intervention | Completed |
| 10 | 15 mo | MC | Maltese/Lhasa Apso mix | 4.6 kg | Intervention | Completed |
| 11 | 38 mo | FS | Springer Spaniel | 21.2 kg | Control | Completed |
| 12 | 48 mo | MC | Dalmatian | 29.4 kg | Intervention | Completed |
| 13 | 84 mo | FS | American Staffordshire Terrier Mix | 20.8 kg | Control | Completed |
| 14 | 24 mo | FS | Belgian Groenendael Sheepdog | 21.2 kg | Control | Completed |
| 15 | 31 mo | MC | Mastiff mix | 34.0 kg | Intervention | Completed |
| 16 | 50 mo | FS | Chihuahua mix | 3.0 kg | Intervention | Completed |
| 17 | 80 mo | FS | German Shepherd mix | 27.6 kg | Control | Completed |
| 18 | 29 mo | FS | Labradoodle | 28.8 kg | Control | Completed |
| 19 | 160 mo | MC | Golden Retriever | 38.8 kg | Intervention | Completed |
| 20 | 68 mo | MC | Poodle Dachshund mix | 11.4 kg | Intervention | Completed |
| 21 | 102 mo | MC | Labrador Retriever | 64.0 kg | Control | Completed |
| 22 | 127 mo | FS | Chihuahua mix | 4.2 kg | Control | Completed |
| 23 | 7 mo | FI | Golden Retriever | 23.6 kg | Control | Completed |
| 24 | 42 mo | MC | Labrador mix | 20.6 kg | Intervention | Completed |
| 25 | 19 mo | FS | Terrier mix | 6.6 kg | Intervention | Completed |
| 26 | 114 mo | FS | Newfoundland dog | 56.2 kg | Control | Completed |
| 27 | 62 mo | FS | Labrador Retriever | 25.0 kg | Intervention | Completed |
| 28 | 24 mo | FS | English Bulldog | 25.8 kg | Control | Withdrawn |
| 29 | 52 mo | MC | Toy Goldendoodle | 6.5 kg | Control | Completed |
| 30 | 9 mo | MI | Australian Cattle Dog | 21.5 kg | Control | Completed |
Table 2.
Study protocol summaries for control and intervention treatment.
| Control Treatment | Intervention Treatment | |
|---|---|---|
| Scale (See Figure 1) |
|
|
| Physical exam |
|
|
| Blood draw |
|
|
| Homework |
|
Table 3.
Exam structure—including order and timing or frequency—used for both intervention and control groups [32].
Table 3.
Exam structure—including order and timing or frequency—used for both intervention and control groups [32].
| Physical Examination Protocol |
|---|
| 1. Dog stroked gently from head to base of tail three times |
| 2. Hand placed over the thigh pulse point for 30 s |
| 3. Lidocaine (2.5% lidocaine/2.5% prilocaine) put on legs (two saphenous and one cephalic) for intervention dogs (control dogs are just touched in these areas) |
| 4. Auscultation of heart and lungs 15 s from each side of the chest |
| 5. Manual manipulation of lymph nodes (in order submandibular, prescapular, popliteal) |
| 6. Gentle abdominal palpation undertaken for 15 s |
| 7. Each paw lifted for 5 s for testing placement; first hind limbs and then fore limbs |
| 8. Lifting of upper lips (control of the oral mucous membranes) |
| 9. Observation of external ear canals for 5 s each (without an otoscope) |
| 10. Ear thermometer placed in position until reading |
| 11. Eyes examined directly (observation of the conjunctiva, checking of the cornea) for 5 s each |
| 12. Venepuncture |
| 13. Gently put your hand on the dog’s back and tell them they are good |
| 14. Remove from table and give treat, or if the dog is on the floor, just give the treat (note whether the dog takes the treat on record) |
| 15. Walk client to parking lot and give treat mid-way to car (note response on record) |
Table 4.
List of selected physiological markers and what specific component of a stress response each evaluates.
Table 4.
List of selected physiological markers and what specific component of a stress response each evaluates.
| Physiological Marker | Stress Measurement |
|---|---|
| Serum cortisol | Acute stress |
| Neutrophil lymphocyte ratio | Chronic stress associated with inflammation |
| Heart rate | Acute stress—immediate sympathetic response |
| Creatine kinase | Muscle damage associated with panic response |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Squair, C.; Proudfoot, K.; Montelpare, W.; Overall, K.L. Effects of Changing Veterinary Handling Techniques on Canine Behaviour and Physiology Part 1: Physiological Measurements. Animals 2023, 13, 1253. https://doi.org/10.3390/ani13071253
AMA Style
Squair C, Proudfoot K, Montelpare W, Overall KL. Effects of Changing Veterinary Handling Techniques on Canine Behaviour and Physiology Part 1: Physiological Measurements. Animals. 2023; 13(7):1253. https://doi.org/10.3390/ani13071253
Chicago/Turabian StyleSquair, Camille, Kathryn Proudfoot, William Montelpare, and Karen L. Overall. 2023. "Effects of Changing Veterinary Handling Techniques on Canine Behaviour and Physiology Part 1: Physiological Measurements" Animals 13, no. 7: 1253. https://doi.org/10.3390/ani13071253
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.