
Beta-Lactams Toxicity in the Intensive Care Unit: An Underestimated Collateral Damage?


Abstract
:Key Points
- The risk of neurotoxicity differs widely among beta-lactam antibiotics.
- The occurrence of a neurological and/or psychiatric sign in patients treated with beta-lactams, especially in the event of renal insufficiency or underlying brain abnormalities, should lead physicians to suspect some degree of neurotoxicity.
- High beta-lactam exposure is common in ICU patients and is associated with an increased risk of neurotoxicity.
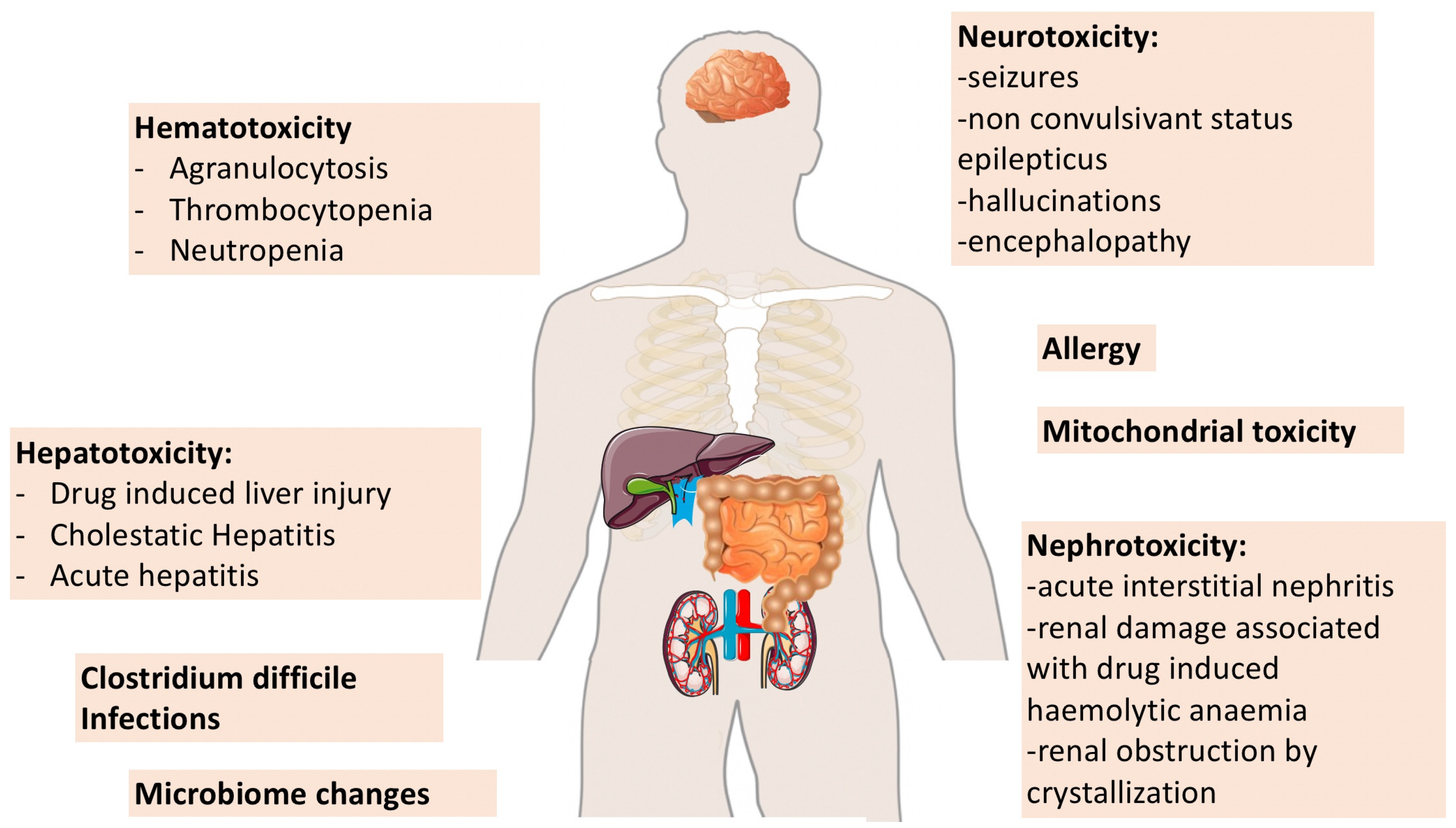
- Nephrotoxicity related to beta-lactams is mainly characterized by the occurrence of acute interstitial nephritis, renal damage associated with drug induced hemolytic anemia and renal obstruction by crystallization.
- Therapeutic drug monitoring and well-defined toxicity thresholds may help in the future to better tailor beta-lactam dosing regimens in ICU patients.
1. Introduction
2. Literature Search
3. Beta-Lactam Neurotoxicity
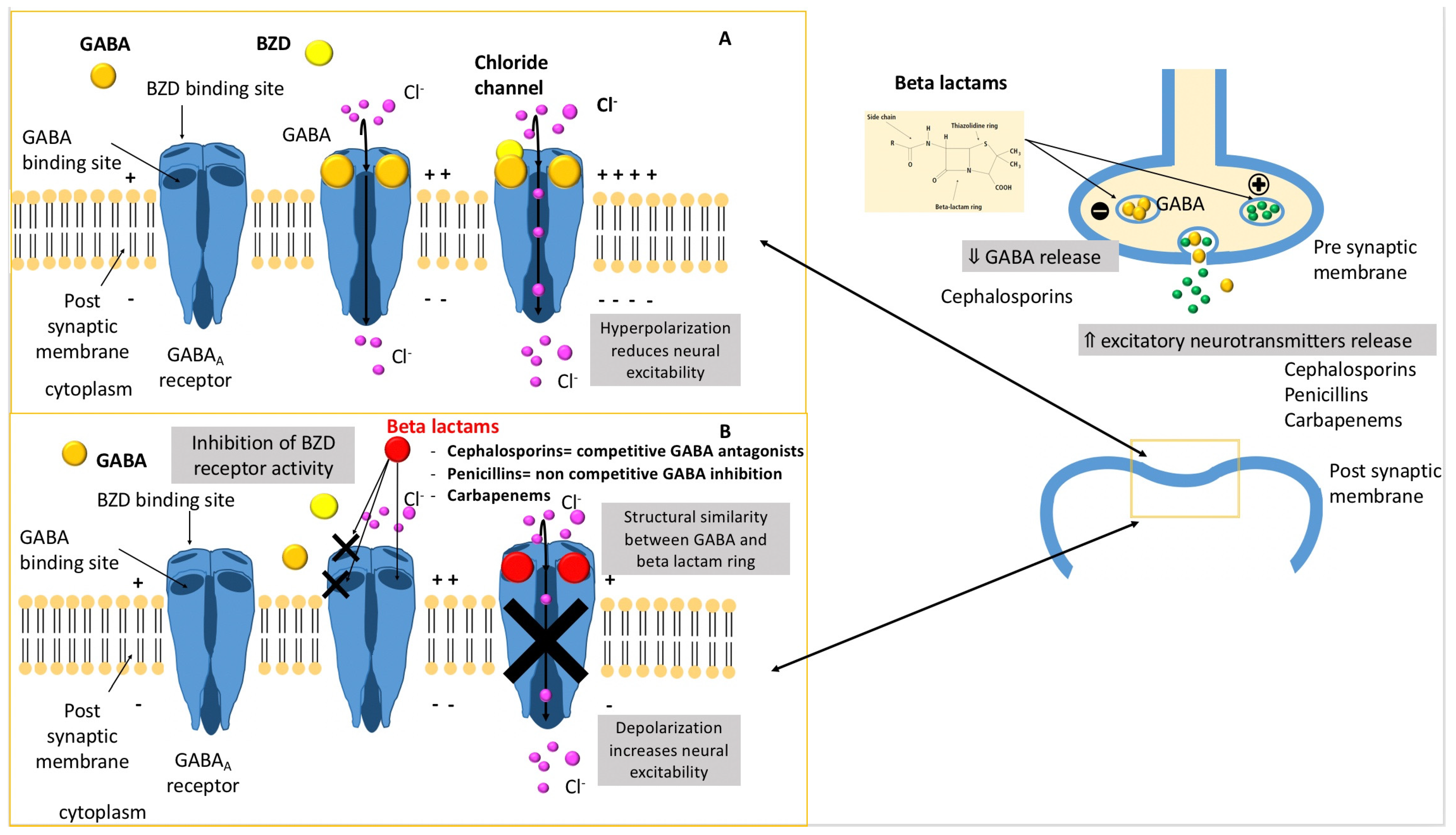
3.1. Physiopathology
- A decrease in gamma-aminobutyric acid (GABA) neuroinhibitory tone through the concentration-dependent inhibition of subunits of the GABAA receptor complex in a competitive (cephalosporins) or non-competitive (penicillins) way. Indeed, the activation of GABAA receptor by endogenous GABA results in an intracellular influx of chloride ions, creating an inhibitory postsynaptic potential that increases the threshold for the generation of an action potential.
- A decrease in the GABA release from nerve terminals.
- The inhibition of the activity of benzodiazepine receptors.
- Direct antagonistic action at the GABAA receptor complex.
3.2. Clinical Manifestations
3.3. Electroencephalogram (EEG)
3.4. Prevalence of Neurotoxicity
3.5. Neurotoxicity Risk Factors
3.5.1. Variable Risk According to Beta-Lactam Molecules
3.5.2. Renal Impairment
3.5.3. Underlying Brain Abnormalities
3.5.4. Advanced Age
4. Perspectives to Limit Beta-Lactam Neurotoxicity: Therapeutic Drug Monitoring
5. Beta-Lactam Nephrotoxicity
5.1. Acute Interstitial Nephritis
5.2. Nephropathy Associated with Hemolytic Anemia
5.3. Crystal (Obstructive) Nephropathy
5.4. AKI and Drug Association
6. Other Beta-Lactam-Related Adverse Events
7. Future Perspectives
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ICU | Intensive care unit |
| CNS | Central nervous system |
| GABA | Gamma-aminobutyric acid |
| EEG | Electroencephalography |
| MIC | Minimal inhibitory concentration |
| TDM | Therapeutic drug monitoring |
References
- Deshayes, S.; Coquerel, A.; Verdon, R. Neurological adverse effects attributable to beta-lactam antibiotics: A literature review. Drug Saf. 2017, 40, 1171–1198. [Google Scholar] [CrossRef]
- Lagace-Wiens, P.; Rubinstein, E. Adverse reactions to beta-lactam antimicrobials. Expert Opin. Drug Saf. 2012, 11, 381–399. [Google Scholar] [CrossRef] [PubMed]
- Arulkumaran, N.; Routledge, M.; Schlebusch, S.; Lipman, J.; Conway Morris, A. Antimicrobial-associated harm in critical care: A narrative review. Intensive Care Med. 2020, 46, 225–235. [Google Scholar] [CrossRef]
- Vardakas, K.Z.; Kalimeris, G.D.; Triarides, N.A.; Falagas, M.E. An update on adverse drug reactions related to beta-lactam antibiotics. Expert Opin. Drug Saf. 2018, 17, 499–508. [Google Scholar] [CrossRef] [PubMed]
- Barreto, E.F.; Webb, A.J.; Pais, G.M.; Rule, A.D.; Jannetto, P.J.; Scheetz, M.H. Setting the beta-lactam therapeutic range for critically ill patients: Is there a floor or even a ceiling? Crit. Care Explor. 2021, 3, e0446. [Google Scholar] [CrossRef]
- Imani, S.; Buscher, H.; Marriott, D.; Gentili, S.; Sandaradura, I. Too much of a good thing: A retrospective study of beta-lactam concentration-toxicity relationships. J. Antimicrob. Chemother. 2017, 72, 2891–2897. [Google Scholar] [CrossRef]
- Chow, K.M.; Hui, A.C.; Szeto, C.C. Neurotoxicity induced by beta-lactam antibiotics: From bench to bedside. Eur. J. Clin. Microbiol. Infect. Dis. 2005, 24, 649–653. [Google Scholar] [CrossRef] [PubMed]
- Grill, M.F.; Maganti, R.K. Neurotoxic effects associated with antibiotic use: Management considerations. Br. J. Clin. Pharmacol. 2011, 72, 381–393. [Google Scholar] [CrossRef] [Green Version]
- Sugimoto, M.; Uchida, I.; Mashimo, T.; Yamazaki, S.; Hatano, K.; Ikeda, F.; Mochizuki, Y.; Terai, T.; Matsuoka, N. Evidence for the involvement of GABA(A) receptor blockade in convulsions induced by cephalosporins. Neuropharmacology 2003, 45, 304–314. [Google Scholar] [CrossRef]
- Wallace, K.L. Antibiotic-induced convulsions. Crit. Care Clin. 1997, 13, 741–762. [Google Scholar] [CrossRef]
- Gutnick, M.J.; Prince, D.A. Penicillinase and the convulsant action of penicillin. Neurology 1971, 21, 759–764. [Google Scholar] [CrossRef]
- Lindquist, C.E.; Dalziel, J.E.; Cromer, B.A.; Birnir, B. Penicillin blocks human alpha 1 beta 1 and alpha 1 beta 1 gamma 2S GABAA channels that open spontaneously. Eur. J. Pharmacol. 2004, 496, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Grill, M.F.; Maganti, R. Cephalosporin-induced neurotoxicity: Clinical manifestations, potential pathogenic mechanisms, and the role of electroencephalographic monitoring. Ann. Pharmacother. 2008, 42, 1843–1850. [Google Scholar] [CrossRef]
- Fugate, J.E.; Kalimullah, E.A.; Hocker, S.E.; Clark, S.L.; Wijdicks, E.F.; Rabinstein, A.A. Cefepime neurotoxicity in the intensive care unit: A cause of severe, underappreciated encephalopathy. Crit. Care 2013, 17, R264. [Google Scholar] [CrossRef] [Green Version]
- Wanleenuwat, P.; Suntharampillai, N.; Iwanowski, P. Antibiotic-induced epileptic seizures: Mechanisms of action and clinical considerations. Seizure 2020, 81, 167–174. [Google Scholar] [CrossRef]
- Ilechukwu, S.T. Acute psychotic reactions and stress response syndromes following intramuscular aqueous procaine penicillin. Br. J. Psychiatry 1990, 156, 554–559. [Google Scholar] [CrossRef] [PubMed]
- Appa, A.A.; Jain, R.; Rakita, R.M.; Hakimian, S.; Pottinger, P.S. Characterizing cefepime neurotoxicity: A systematic review. In Open Forum Infectious Diseases; Oxford University Press: Oxford, UK, 2017; Volume 4, p. ofx170. [Google Scholar] [CrossRef] [Green Version]
- Payne, L.E.; Gagnon, D.J.; Riker, R.R.; Seder, D.B.; Glisic, E.K.; Morris, J.G.; Fraser, G.L. Cefepime-induced neurotoxicity: A systematic review. Crit. Care 2017, 21, 276. [Google Scholar] [CrossRef] [Green Version]
- Li, H.T.; Lee, C.H.; Wu, T.; Cheng, M.Y.; Tseng, W.J.; Chang, C.W.; Hsieh, H.Y.; Chiang, H.I.; Lin, C.Y.; Chang, B.L.; et al. Clinical, electroencephalographic features and prognostic factors of cefepime-induced neurotoxicity: A retrospective study. Neurocrit. Care 2019, 31, 329–337. [Google Scholar] [CrossRef]
- Beumier, M.; Casu, G.S.; Hites, M.; Wolff, F.; Cotton, F.; Vincent, J.L.; Jacobs, F.; Taccone, F.S. Elevated beta-lactam concentrations associated with neurological deterioration in ICU septic patients. Minerva Anestesiol. 2015, 81, 497–506. [Google Scholar] [PubMed]
- Schliamser, S.E.; Cars, O.; Norrby, S.R. Neurotoxicity of beta-lactam antibiotics: Predisposing factors and pathogenesis. J. Antimicrob. Chemother. 1991, 27, 405–425. [Google Scholar] [CrossRef] [PubMed]
- Walker, A.E.; Johnson, H.C. Convulsive factor in commercial penicillin. Arch. Surg. 1945, 50, 69–73. [Google Scholar] [CrossRef]
- Nau, R.; Sorgel, F.; Eiffert, H. Penetration of drugs through the blood-cerebrospinal fluid/blood-brain barrier for treatment of central nervous system infections. Clin. Microbiol. Rev. 2010, 23, 858–883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Sarro, A.; Ammendola, D.; Zappala, M.; Grasso, S.; De Sarro, G.B. Relationship between structure and convulsant properties of some beta-lactam antibiotics following intracerebroventricular microinjection in rats. Antimicrob. Agents Chemother. 1995, 39, 232–237. [Google Scholar] [CrossRef] [Green Version]
- Sutter, R.; Ruegg, S.; Tschudin-Sutter, S. Seizures as adverse events of antibiotic drugs: A systematic review. Neurology 2015, 85, 1332–1341. [Google Scholar] [CrossRef] [PubMed]
- Huwyler, T.; Lenggenhager, L.; Abbas, M.; Ing Lorenzini, K.; Hughes, S.; Huttner, B.; Karmime, A.; Uckay, I.; von Dach, E.; Lescuyer, P.; et al. Cefepime plasma concentrations and clinical toxicity: A retrospective cohort study. Clin. Microbiol. Infect. 2017, 23, 454–459. [Google Scholar] [CrossRef] [Green Version]
- Linden, P. Safety profile of meropenem: An updated review of over 6000 patients treated with meropenem. Drug Saf. 2007, 30, 657–668. [Google Scholar] [CrossRef] [PubMed]
- Cannon, J.P.; Lee, T.A.; Clark, N.M.; Setlak, P.; Grim, S.A. The risk of seizures among the carbapenems: A meta-analysis. J. Antimicrob. Chemother. 2014, 69, 2043–2055. [Google Scholar] [CrossRef] [PubMed]
- Park, M.K.; Lim, K.S.; Kim, T.E.; Han, H.K.; Yi, S.J.; Shin, K.H.; Cho, J.Y.; Shin, S.G.; Jang, I.J.; Yu, K.S. Reduced valproic acid serum concentrations due to drug interactions with carbapenem antibiotics: Overview of 6 cases. Ther. Drug Monit. 2012, 34, 599–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gatti, M.; Raschi, E.; De Ponti, F. Serious adverse events with novel beta-lactam/beta-lactamase inhibitor combinations: A large-scale pharmacovigilance analysis. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 1169–1176. [Google Scholar] [CrossRef]
- Chatellier, D.; Jourdain, M.; Mangalaboyi, J.; Ader, F.; Chopin, C.; Derambure, P.; Fourrier, F. Cefepime-induced neurotoxicity: An underestimated complication of antibiotherapy in patients with acute renal failure. Intensive Care Med. 2002, 28, 214–217. [Google Scholar] [CrossRef]
- Zhang, J.; Huang, C.; Li, H.; Yao, Q.; Xu, J.; Yuan, J.; Qian, J.; Bao, B. Antibiotic-induced neurotoxicity in dialysis patients: A retrospective study. Ren. Fail. 2013, 35, 901–905. [Google Scholar] [CrossRef]
- Quinton, M.C.; Bodeau, S.; Kontar, L.; Zerbib, Y.; Maizel, J.; Slama, M.; Masmoudi, K.; Lemaire-Hurtel, A.S.; Bennis, Y. Neurotoxic concentration of piperacillin during continuous infusion in critically ill patients. Antimicrob. Agents Chemother. 2017, 61. [Google Scholar] [CrossRef] [Green Version]
- Calandra, G.; Lydick, E.; Carrigan, J.; Weiss, L.; Guess, H. Factors predisposing to seizures in seriously ill infected patients receiving antibiotics: Experience with imipenem/cilastatin. Am. J. Med. 1988, 84, 911–918. [Google Scholar] [CrossRef]
- Khan, A.; DeMott, J.M.; Varughese, C.; Hammond, D.A. Effect of cefepime on neurotoxicity development in critically ill adults with renal dysfunction. Chest 2020, 158, 157–163. [Google Scholar] [CrossRef]
- Barbhaiya, R.H.; Knupp, C.A.; Forgue, S.T.; Matzke, G.R.; Guay, D.R.; Pittman, K.A. Pharmacokinetics of cefepime in subjects with renal insufficiency. Clin. Pharmacol. Ther. 1990, 48, 268–276. [Google Scholar] [CrossRef] [PubMed]
- Mattappalil, A.; Mergenhagen, K.A. Neurotoxicity with antimicrobials in the elderly: A review. Clin. Ther. 2014, 36, 1489–1511 e1484. [Google Scholar] [CrossRef] [PubMed]
- Abdul-Aziz, M.H.; Alffenaar, J.C.; Bassetti, M.; Bracht, H.; Dimopoulos, G.; Marriott, D.; Neely, M.N.; Paiva, J.A.; Pea, F.; Sjovall, F.; et al. Antimicrobial therapeutic drug monitoring in critically ill adult patients: A position paper. Intensive Care Med. 2020, 46, 1127–1153. [Google Scholar] [CrossRef] [PubMed]
- Tabah, A.; De Waele, J.; Lipman, J.; Zahar, J.R.; Cotta, M.O.; Barton, G.; Timsit, J.F.; Roberts, J.A. The Working Group for Antimicrobial Use in the ICU within the Infection Section of the European Society of Intensive Care Medicine (ESICM). The ADMIN-ICU survey: A survey on antimicrobial dosing and monitoring in ICUs. J. Antimicrob. Chemother. 2015, 70, 2671–2677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, G.; Brinkman, A.; Benefield, R.J.; Carlier, M.; De Waele, J.J.; El Helali, N.; Frey, O.; Harbarth, S.; Huttner, A.; McWhinney, B.; et al. An international, multicentre survey of beta-lactam antibiotic therapeutic drug monitoring practice in intensive care units. J. Antimicrob. Chemother. 2014, 69, 1416–1423. [Google Scholar] [CrossRef] [Green Version]
- Scaglione, F.; Esposito, S.; Leone, S.; Lucini, V.; Pannacci, M.; Ma, L.; Drusano, G.L. Feedback dose alteration significantly affects probability of pathogen eradication in nosocomial pneumonia. Eur. Respir. J. 2009, 34, 394–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richter, D.C.; Frey, O.; Rohr, A.; Roberts, J.A.; Koberer, A.; Fuchs, T.; Papadimas, N.; Heinzel-Gutenbrunner, M.; Brenner, T.; Lichtenstern, C.; et al. Therapeutic drug monitoring-guided continuous infusion of piperacillin/tazobactam significantly improves pharmacokinetic target attainment in critically ill patients: A retrospective analysis of four years of clinical experience. Infection 2019, 47, 1001–1011. [Google Scholar] [CrossRef] [Green Version]
- Neely, M.N.; Kato, L.; Youn, G.; Kraler, L.; Bayard, D.; van Guilder, M.; Schumitzky, A.; Yamada, W.; Jones, B.; Minejima, E. Prospective trial on the use of trough concentration versus area under the curve to determine therapeutic vancomycin dosing. Antimicrob. Agents Chemother. 2018, 62. [Google Scholar] [CrossRef] [Green Version]
- McDonald, C.; Cotta, M.O.; Little, P.J.; McWhinney, B.; Ungerer, J.P.; Lipman, J.; Roberts, J.A. Is high-dose beta-lactam therapy associated with excessive drug toxicity in critically ill patients? Minerva Anestesiol. 2016, 82, 957–965. [Google Scholar] [PubMed]
- Lamoth, F.; Buclin, T.; Pascual, A.; Vora, S.; Bolay, S.; Decosterd, L.A.; Calandra, T.; Marchetti, O. High cefepime plasma concentrations and neurological toxicity in febrile neutropenic patients with mild impairment of renal function. Antimicrob. Agents Chemother. 2010, 54, 4360–4367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guilhaumou, R.; Benaboud, S.; Bennis, Y.; Dahyot-Fizelier, C.; Dailly, E.; Gandia, P.; Goutelle, S.; Lefeuvre, S.; Mongardon, N.; Roger, C.; et al. Optimization of the treatment with beta-lactam antibiotics in critically ill patients-guidelines from the French Society of Pharmacology and Therapeutics (Societe Francaise de Pharmacologie et Therapeutique-SFPT) and the French Society of Anaesthesia and Intensive Care Medicine (Societe Francaise d’Anesthesie et Reanimation-SFAR). Crit. Care 2019, 23, 104. [Google Scholar] [CrossRef] [Green Version]
- Duarte, C.G.; Preuss, H.G. Assessment of renal function—Glomerular and tubular. Clin. Lab. Med. 1993, 13, 33–52. [Google Scholar] [CrossRef]
- Jensen, J.U.; Hein, L.; Lundgren, B.; Bestle, M.H.; Mohr, T.; Andersen, M.H.; Thornberg, K.J.; Loken, J.; Steensen, M.; Fox, Z.; et al. Kidney failure related to broad-spectrum antibiotics in critically ill patients: Secondary end point results from a 1200 patient randomised trial. BMJ Open 2012, 2, e000635. [Google Scholar] [CrossRef] [PubMed]
- Rutter, W.C.; Burgess, D.R.; Talbert, J.C.; Burgess, D.S. Acute kidney injury in patients treated with vancomycin and piperacillin-tazobactam: A retrospective cohort analysis. J. Hosp. Med. 2017, 12, 77–82. [Google Scholar] [CrossRef] [Green Version]
- Muriithi, A.K.; Leung, N.; Valeri, A.M.; Cornell, L.D.; Sethi, S.; Fidler, M.E.; Nasr, S.H. Biopsy-proven acute interstitial nephritis, 1993-2011: A case series. Am. J. Kidney Dis. 2014, 64, 558–566. [Google Scholar] [CrossRef]
- Nast, C.C. Medication-induced interstitial nephritis in the 21st century. Adv. Chronic Kidney Dis. 2017, 24, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Markowitz, G.S.; Perazella, M.A. Drug-induced renal failure: A focus on tubulointerstitial disease. Clin. Chim. Acta 2005, 351, 31–47. [Google Scholar] [CrossRef] [PubMed]
- Perazella, M.A. Diagnosing drug-induced AIN in the hospitalized patient: A challenge for the clinician. Clin. Nephrol. 2014, 81, 381–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moledina, D.G.; Perazella, M.A. Drug-induced acute interstitial nephritis. Clin. J. Am. Soc. Nephrol. 2017, 12, 2046–2049. [Google Scholar] [CrossRef]
- Clarkson, M.R.; Giblin, L.; O’Connell, F.P.; O’Kelly, P.; Walshe, J.J.; Conlon, P.; O’Meara, Y.; Dormon, A.; Campbell, E.; Donohoe, J. Acute interstitial nephritis: Clinical features and response to corticosteroid therapy. Nephrol. Dial. Transpl. 2004, 19, 2778–2783. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez, E.; Gutierrez, E.; Galeano, C.; Chevia, C.; de Sequera, P.; Bernis, C.; Parra, E.G.; Delgado, R.; Sanz, M.; Ortiz, M.; et al. Early steroid treatment improves the recovery of renal function in patients with drug-induced acute interstitial nephritis. Kidney Int. 2008, 73, 940–946. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raza, M.N.; Hadid, M.; Keen, C.E.; Bingham, C.; Salmon, A.H. Acute tubulointerstitial nephritis, treatment with steroid and impact on renal outcomes. Nephrology 2012, 17, 748–753. [Google Scholar] [CrossRef] [PubMed]
- Garratty, G.; Arndt, P.A. Drugs that have been shown to cause drug-induced immune hemolytic anemia or positive direct antiglobulin tests: Some interesting findings since 2007. Immunohematology 2014, 30, 66–79. [Google Scholar] [CrossRef] [PubMed]
- Arndt, P.A. Drug-induced immune hemolytic anemia: The last 30 years of changes. Immunohematology 2014, 30, 44–54. [Google Scholar] [CrossRef]
- Mayer, B.; Bartolmas, T.; Yurek, S.; Salama, A. Variability of findings in drug-induced immune haemolytic anaemia: Experience over 20 years in a single centre. Transfus. Med. Hemother. 2015, 42, 333–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Northrop, M.S.; Agarwal, H.S. Ceftriaxone-induced hemolytic anemia: Case report and review of literature. J. Pediatr. Hematol. Oncol. 2015, 37, e63–e66. [Google Scholar] [CrossRef] [PubMed]
- Neuman, G.; Boodhan, S.; Wurman, I.; Koren, G.; Bitnun, A.; Kirby-Allen, M.; Ito, S. Ceftriaxone-induced immune hemolytic anemia. Ann. Pharmacother. 2014, 48, 1594–1604. [Google Scholar] [CrossRef]
- Deuel, J.W.; Schaer, C.A.; Boretti, F.S.; Opitz, L.; Garcia-Rubio, I.; Baek, J.H.; Spahn, D.R.; Buehler, P.W.; Schaer, D.J. Hemoglobinuria-related acute kidney injury is driven by intrarenal oxidative reactions triggering a heme toxicity response. Cell Death Dis. 2016, 7, e2064. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rifkind, J.M.; Mohanty, J.G.; Nagababu, E. The pathophysiology of extracellular hemoglobin associated with enhanced oxidative reactions. Front. Physiol. 2014, 5, 500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garratty, G. Drug-induced immune hemolytic anemia. Hematol. Am. Soc. Hematol. Educ. Program. 2009. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Yu, D. Adverse drug reactions during ceftriaxone treatment can cause severe hemolysis. Pediatr. Allergy Immunol. 2014, 25, 101–102. [Google Scholar] [CrossRef] [PubMed]
- Vehapoglu, A.; Goknar, N.; Tuna, R.; Cakir, F.B. Ceftriaxone-induced hemolytic anemia in a child successfully managed with intravenous immunoglobulin. Turk. J. Pediatr. 2016, 58, 216–219. [Google Scholar] [CrossRef] [Green Version]
- Leicht, H.B.; Weinig, E.; Mayer, B.; Viebahn, J.; Geier, A.; Rau, M. Ceftriaxone-induced hemolytic anemia with severe renal failure: A case report and review of literature. BMC Pharmacol. Toxicol. 2018, 19, 67. [Google Scholar] [CrossRef]
- Shahrbaf, F.G.; Assadi, F. Drug-induced renal disorders. J. Renal Inj. Prev. 2015, 4, 57–60. [Google Scholar] [CrossRef]
- Mulay, S.R.; Anders, H.J. Crystal nephropathies: Mechanisms of crystal-induced kidney injury. Nat. Rev. Nephrol. 2017, 13, 226–240. [Google Scholar] [CrossRef]
- Chutipongtanate, S.; Thongboonkerd, V. Ceftriaxone crystallization and its potential role in kidney stone formation. Biochem. Biophys. Res. Commun. 2011, 406, 396–402. [Google Scholar] [CrossRef]
- Kimata, T.; Kaneko, K.; Takahashi, M.; Hirabayashi, M.; Shimo, T.; Kino, M. Increased urinary calcium excretion caused by ceftriaxone: Possible association with urolithiasis. Pediatr. Nephrol. 2012, 27, 605–609. [Google Scholar] [CrossRef] [PubMed]
- Mousseaux, C.; Rafat, C.; Letavernier, E.; Frochot, V.; Kerroumi, Y.; Zeller, V.; Luque, Y. Acute kidney injury after high doses of amoxicillin. Kidney Int. Rep. 2021, 6, 830–834. [Google Scholar] [CrossRef] [PubMed]
- Zeller, V.; Puyraimond-Zemmour, D.; Sene, T.; Lidove, O.; Meyssonnier, V.; Ziza, J.M. Amoxicillin crystalluria, an emerging complication with an old and well-known antibiotic. Antimicrob. Agents Chemother. 2016, 60, 3248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vodovar, D.; Thomas, L.; Mongardon, N.; Lepeule, R.; Lebrun-Vignes, B.; Biour, M.; Netzer, F.; Haouache, H.; Le Beller, C.; Dhonneur, G. Dramatic increase of amoxicillin-induced crystal nephropathy found in a cohort study of French pharmacovigilance centers. Antimicrob. Agents Chemother. 2018, 62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avci, Z.; Koktener, A.; Uras, N.; Catal, F.; Karadag, A.; Tekin, O.; Degirmencioglu, H.; Baskin, E. Nephrolithiasis associated with ceftriaxone therapy: A prospective study in 51 children. Arch. Dis. Child. 2004, 89, 1069–1072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, X.; Wu, R.; Huang, X.; Zhang, Y. Noncontrast multidetector-row computed tomography scanning for detection of radiolucent calculi in acute renal insufficiency caused by bilateral ureteral obstruction of ceftriaxone crystals. J. X-ray Sci. Technol. 2012, 20, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Hammond, D.A.; Smith, M.N.; Li, C.; Hayes, S.M.; Lusardi, K.; Bookstaver, P.B. Systematic review and meta-analysis of acute kidney injury associated with concomitant vancomycin and piperacillin/tazobactam. Clin. Infect. Dis. 2017, 64, 666–674. [Google Scholar] [CrossRef]
- Blevins, A.M.; Lashinsky, J.N.; McCammon, C.; Kollef, M.; Micek, S.; Juang, P. Incidence of acute kidney injury in critically ill patients receiving vancomycin with concomitant piperacillin-tazobactam, cefepime, or meropenem. Antimicrob. Agents Chemother. 2019, 63. [Google Scholar] [CrossRef] [Green Version]
- Hundeshagen, G.; Herndon, D.N.; Capek, K.D.; Branski, L.K.; Voigt, C.D.; Killion, E.A.; Cambiaso-Daniel, J.; Sljivich, M.; De Crescenzo, A.; Mlcak, R.P.; et al. Co-administration of vancomycin and piperacillin-tazobactam is associated with increased renal dysfunction in adult and pediatric burn patients. Crit. Care 2017, 21, 318. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Beta-Lactam | Relative Pro-Convulsive Activity (Reference: Penicillin G = 100) |
|---|---|
| Cefazolin | 294 |
| Cefepime | 160 |
| Penicillin G | 100 |
| Imipenem | 71 |
| Aztreonam | 42 |
| Ampicillin | 21 |
| Ceftazidime | 17 |
| Meropenem | 16 |
| Ceftriaxone | 12 |
| Piperacillin | 11 |
| Cefotaxime | 8.8 |
| Cefoxitine | 1.8 |
| Beta-Lactam | Toxicity Threshold | Clinical Signs |
|---|---|---|
| Flucloxacillin [6] | Cmin > 125.1 mg/L | Seizures |
| Confusion | ||
| Myoclonia | ||
| Amoxicillin [46] | Css < 8 × MIC | Psychotic symptoms |
| Ceftazidime [46] | Css < 8 × MIC | Encephalopathy |
| Confusion, disturbed vigilance | ||
| Cefepime [45] | Cmin > 20 mg/L | Encephalopathy |
| Confusion, disturbed vigilance | ||
| Piperacillin tazobactam [6,20,33] | Css > 157.2 mg/L (pip taz CI) Cmin > 64 (pip taz)–361(pip alone) mg/L | Seizures |
| Hallucinations | ||
| Imipenem [46] | Css < 8 × MIC | Seizures |
| Confusion | ||
| Myoclonia | ||
| Meropenem [6] | Cmin > 64 mg/L | Seizures |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roger, C.; Louart, B. Beta-Lactams Toxicity in the Intensive Care Unit: An Underestimated Collateral Damage? Microorganisms 2021, 9, 1505. https://doi.org/10.3390/microorganisms9071505
Roger C, Louart B. Beta-Lactams Toxicity in the Intensive Care Unit: An Underestimated Collateral Damage? Microorganisms. 2021; 9(7):1505. https://doi.org/10.3390/microorganisms9071505
Chicago/Turabian StyleRoger, Claire, and Benjamin Louart. 2021. "Beta-Lactams Toxicity in the Intensive Care Unit: An Underestimated Collateral Damage?" Microorganisms 9, no. 7: 1505. https://doi.org/10.3390/microorganisms9071505