

Prevalence of Oral Pathogen Slackia exigua among Clinical Orthodontic and Non-Orthodontic Saliva Samples

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Approval
2.2. Original Study Sample Collection Protocol
2.3. DNA Isolation and Analysis
2.4. qPCR Screening
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Poco, S.E., Jr.; Nakazawa, F.; Ikeda, T.; Sato, M.; Sato, T.; Hoshino, E. Eubacterium exiguum sp. nov., isolated from human oral lesions. Int. J. Syst. Bacteriol. 1996, 46, 1120–1124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wade, W.G.; Downes, J.; Dymock, D.; Hiom, S.J.; Weightman, A.J.; Dewhirst, F.E.; Paster, B.J.; Tzellas, N.; Coleman, B. The family Coriobacteriaceae: Reclassification of Eubacterium exiguum (Poco et al. 1996) and Peptostreptococcus heliotrinreducens (Lanigan 1976) as Slackia exigua gen. nov., comb. nov. and Slackia heliotrinireducens gen. nov., comb. nov., and Eubacterium lentum (Prevot 1938) as Eggerthella lenta gen. nov., comb. nov. Int. J. Syst. Bacteriol. 1999, 49 Pt 2, 595–600. [Google Scholar] [PubMed]
- Nakazawa, F.; Sato, M.; Poco, S.E.; Hashimura, T.; Ikeda, T.; Kalfas, S.; Sundqvist, G.; Hoshino, E. Description of Mogibacterium pumilum gen. nov., sp. nov. and Mogibacterium vescum gen. nov., sp. nov., and reclassification of Eubacterium timidum (Holdeman et al. 1980) as Mogibacterium timidum gen. nov., comb. nov. Int. J. Syst. Evol. Microbiol. 2000, 50 Pt 2, 679–688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakazawa, F.; Hoshino, E. DNA-DNA relatedness and phylogenetic positions of Slackia exigua, Slackia heliotrinireducens, Eggerthella lenta, and other related bacteria. Oral Microbiol. Immunol. 2004, 19, 343–346. [Google Scholar] [CrossRef]
- Jin, J.S.; Kitahara, M.; Sakamoto, M.; Hattori, M.; Benno, Y. Slackia equolifaciens sp. nov., a human intestinal bacterium capable of producing equol. Int. J. Syst. Evol. Microbiol. 2010, 60 Pt 8, 1721–1724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, K.S.; Rowlinson, M.C.; Bennion, R.; Liu, C.; Talan, D.; Summanen, P.; Finegold, S.M. Characterization of Slackia exigua isolated from human wound infections, including abscesses of intestinal origin. J. Clin. Microbiol. 2010, 48, 1070–1075. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanner, A.C.; Kent, R.L., Jr.; Holgerson, P.L.; Hughes, C.V.; Loo, C.Y.; Kanasi, E.; Chalmers, N.I.; Johansson, I. Microbiota of severe early childhood caries before and after therapy. J. Dent. Res. 2011, 90, 1298–1305. [Google Scholar] [CrossRef] [Green Version]
- Zakaria, M.N.; Takeshita, T.; Shibata, Y.; Maeda, H.; Wada, N.; Akamine, A.; Yamashita, Y. Microbial community in persistent apical periodontitis: A 16S rRNA gene clone library analysis. Int. Endod. J. 2015, 48, 717–728. [Google Scholar] [CrossRef]
- Heller, D.; Helmerhorst, E.J.; Gower, A.C.; Siqueira, W.L.; Paster, B.J.; Oppenheim, F.G. Microbial Diversity in the Early In Vivo-Formed Dental Biofilm. Appl. Environ. Microbiol. 2016, 82, 1881–1888. [Google Scholar] [CrossRef] [Green Version]
- Hiranmayi, K.V.; Sirisha, K.; Ramoji Rao, M.V.; Sudhakar, P. Novel Pathogens in Periodontal Microbiology. J. Pharm. Bioallied. Sci. 2017, 9, 155–163. [Google Scholar] [CrossRef]
- Fakhruddin, K.S.; Ngo, H.C.; Samaranayake, L.P. Cariogenic microbiome and microbiota of the early primary dentition: A contemporary overview. Oral Dis. 2019, 25, 982–995. [Google Scholar] [CrossRef] [PubMed]
- Karasneh, J.A.; Al Habashneh, R.A.; Marzouka, N.A.; Thornhill, M.H. Effect of cigarette smoking on subgingival bacteria in healthy subjects and patients with chronic periodontitis. BMC Oral Health 2017, 17, 64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holmer, J.; Aho, V.; Eriksdotter, M.; Paulin, L.; Pietiäinen, M.; Auvinen, P.; Schultzberg, M.; Pussinen, P.J.; Buhlin, K. Subgingival microbiota in a population with and without cognitive dysfunction. J. Oral Microbiol. 2021, 13, 1854552. [Google Scholar] [CrossRef]
- Skeie, M.S.; Sen, A.; Dahllöf, G.; Fagerhaug, T.N.; Høvik, H.; Klock, K.S. Dental caries at enamel and dentine level among European adolescents—A systematic review and meta-analysis. BMC Oral Health 2022, 22, 620. [Google Scholar] [CrossRef] [PubMed]
- Oikonomou, E.; Foros, P.; Tagkli, A.; Rahiotis, C.; Eliades, T.; Koletsi, D. Impact of Aligners and Fixed Appliances on Oral Health during Orthodontic Treatment: A Systematic Review and Meta-Analysis. Oral Health Prev. Dent. 2021, 19, 659–672. [Google Scholar]
- Zhai, M.; Wang, M.; Li, L.; Liu, B.; Wei, F. Periodontal Parameters in Fixed Labial and Lingual Orthodontic Treatment: A Systematic Review and Meta-Analysis. Oral Health Prev. Dent. 2022, 20, 475–484. [Google Scholar] [PubMed]
- Mester, A.; Onisor, F.; Mesaros, A.S. Periodontal Health in Patients with Self-Ligating Brackets: A Systematic Review of Clinical Studies. J. Clin. Med. 2022, 11, 2570. [Google Scholar] [CrossRef]
- Shen, L.H.; Xiao, E.; Wang, E.B.; Zheng, H.; Zhang, Y. High-Throughput Sequencing Analysis of Microbial Profiles in the Dry Socket. J. Oral Maxillofac. Surg. 2019, 77, 1548–1556. [Google Scholar] [CrossRef]
- Kim, H.J.; Ahn, D.H.; Yu, Y.; Han, H.; Kim, S.Y.; Joo, J.Y.; Chung, J.; Na, H.S.; Lee, J.Y. Microbial profiling of peri-implantitis compared to the periodontal microbiota in health and disease using 16S rRNA sequencing. J. Periodontal. Implant Sci. 2023, 53, 69–84. [Google Scholar] [CrossRef]
- Lee, M.Y.; Kim, M.H.; Lee, W.I.; Kang, S.Y. Septic shock caused by Slackia exigua in a patient with diabetes. Anaerobe 2022, 73, 102498. [Google Scholar] [CrossRef]
- Lim, K.R.; Son, J.S.; Moon, S.Y. A case of Slackia exigua bacteremia associated with pyometra in a patient with poor dentition. Anaerobe 2022, 73, 102477. [Google Scholar] [CrossRef] [PubMed]
- Brzezinski, A.; Mennona, S.; Imbergamo, C.; Brzezinska, K.; Kayiaros, S. A Rare Case of Periprosthetic Joint Infection Caused by a Periodontal Pathogen, Slackia exigua: A Case Report. JBJS Case Connect. 2021, 22, 11. [Google Scholar] [CrossRef] [PubMed]
- McDaniel, J.; McDaniel, S.; Samiano, B.J.; Marrujo, M.; Kingsley, K.; Howard, K.M. Microbial Screening Reveals Oral Site-Specific Locations of the Periodontal Pathogen Selenomonas noxia. Curr. Issues Mol. Biol. 2021, 43, 353–364. [Google Scholar] [CrossRef] [PubMed]
- McDaniel, S.; McDaniel, J.; Howard, K.M.; Kingsley, K. Molecular Screening and Analysis Reveal Novel Oral Site-Specific Locations for the Cariogenic Pathogen Scardovia wiggsiae. Dent. J. 2021, 9, 73. [Google Scholar] [CrossRef]
- Davis, J.E.; Freel, N.; Findley, A.; Tomlin, K.; Howard, K.M.; Seran, C.C.; Cruz, P.; Kingsley, K. A molecular survey of S. mutans and P. gingivalis oral microbial burden in human saliva using relative endpoint polymerase chain reaction (RE-PCR) within the population of a Nevada dental school revealed disparities among minorities. BMC Oral Health 2012, 27, 34. [Google Scholar] [CrossRef] [Green Version]
- Shen, C.; Clawson, J.B.; Simpson, J.; Kingsley, K. Oral Prevalence of Akkermansia muciniphila Differs among Pediatric and Adult Orthodontic and Non-Orthodontic Patients. Microorganisms 2023, 11, 112. [Google Scholar] [CrossRef]
- Farronato, G.; Giannini, L.; Galbiati, G.; Cannalire, P.; Martinelli, G.; Tubertini, I.; Maspero, C. Oral tissues and orthodontic treatment: Common side effects. Minerva Stomatol. 2013, 62, 431–446. [Google Scholar]
- Do Nascimento, L.E.; de Souza, M.M.; Azevedo, A.R.; Maia, L.C. Are self-ligating brackets related to less formation of Streptococcus mutans colonies? A systematic review. Dent. Press J. Orthod. 2014, 19, 60–68. [Google Scholar] [CrossRef]
- Mavi, J.; Kingsley, K. Analysis of a Pediatric Dental School Patient Population Revealed Increasing Trends of Limited English Proficiency (LEP) Patients: Implications for Pediatric Dental Public Health and Access to Care. Pediatr. Rep. 2022, 14, 276–287. [Google Scholar] [CrossRef]
- Ozuna, J.; Barborka, B.; Abubakr, N.H. A Retrospective Evaluation of the Prevalence of Cracked Teeth Among an Adult Population in Nevada. Eur. Endod. J. 2021, 6, 160–163. [Google Scholar]
- Anwar, D.S.; Mohd Yusof, M.Y.P.; Ahmad, M.S.; Md Sabri, B.A. Family Influences on the Dental Caries Status of Children with Special Health Care Needs: A Systematic Review. Children 2022, 9, 1855. [Google Scholar] [CrossRef] [PubMed]
- Crego-Ruiz, M.; Jorba-García, A. Assessment of the periodontal health status and gingival recession during orthodontic treatment with clear aligners and fixed appliances: A systematic review and meta-analysis. Med. Oral Patol. Oral Cir. Bucal. 2023, 15, 25760. [Google Scholar] [CrossRef] [PubMed]
- Jervøe-Storm, P.M.; Eberhard, J.; Needleman, I.; Worthington, H.V.; Jepsen, S. Full-mouth treatment modalities (within 24 hours) for periodontitis in adults. Cochrane Database Syst Rev. 2022, 6, CD004622. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Demographic | Study Sample | Clinic Population | Statistical Analysis |
|---|---|---|---|
| Sex | |||
| Female | n = 132/266 (49.6%) | 49.1% | X2 = 0.100, d.f. = 1 |
| Male | n = 134/266 (50.4%) | 50.9% | p = 0.7518 |
| Race/Ethnicity | |||
| White | n = 93/266 (34.9%) | 34.6% | X2 = 0.040, d.f. = 1 |
| Minority | n = 173/266 (65.1%) | 65.4% | p = 0.8422 |
| Hispanic | n = 151/266 (56.7%) | 58.6% | |
| Age | |||
| Pediatric n = 141 | 13.1 years (Average) 7–17 years (Range) | 10.4 years (Average) 0–17 years (Range) | Two-tailed t-test p = 0.021 |
| Adult n = 125 | 40.6 years (Average) 18–77 years (Range) | 42.3 years (Average) 18–89 years (Range) | Two-tailed t-test p = 0.038 |
| Study Samples | DNA Concentration [ng/uL] | DNA Purity A260:A280 Ratio |
|---|---|---|
| Pediatric patient samples | Average: 481.2 ng/uL +/− 55.1 Range: 127.2–769.1 ng/uL | Average: 1.73 Range: 1.69–1.82 |
| Adult patient samples | Average: 455.3 ng/uL +/− 61.2 Range: 189.5–776.2 ng/uL | Average: 1.75 Range: 1.66–1.85 |
| Demographic | Slackia exigua (SE)-Positive | Slackia exigua (SE)-Negative | Statistical Analysis |
|---|---|---|---|
| Sex | |||
| Male | n = 59/134 (44.0%) | n = 75/134 (56.0%) | X2 = 0.1440, d.f. = 1 |
| Female | n = 52/132 (39.4%) | n = 80/132 (60.6%) | p = 0.2301 |
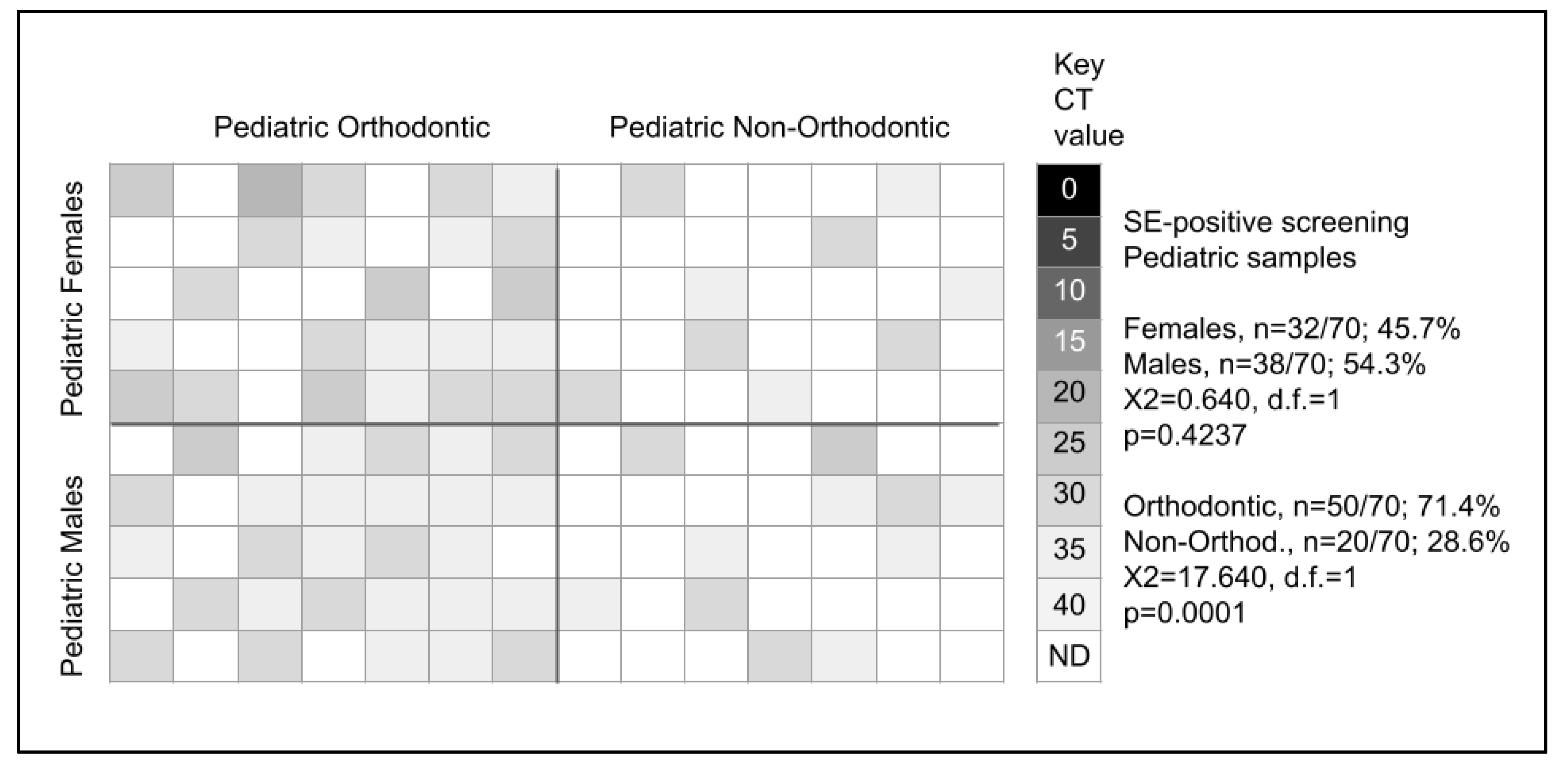
| Pediatric Male | n = 38/71 (53.5%) | n = 33/71 (46.5%) | X2 = 0.640, d.f. = 1 |
| Pediatric Female | n = 32/70 (45.7%) | n = 38/71 (53.5%) | p = 0.4237 |
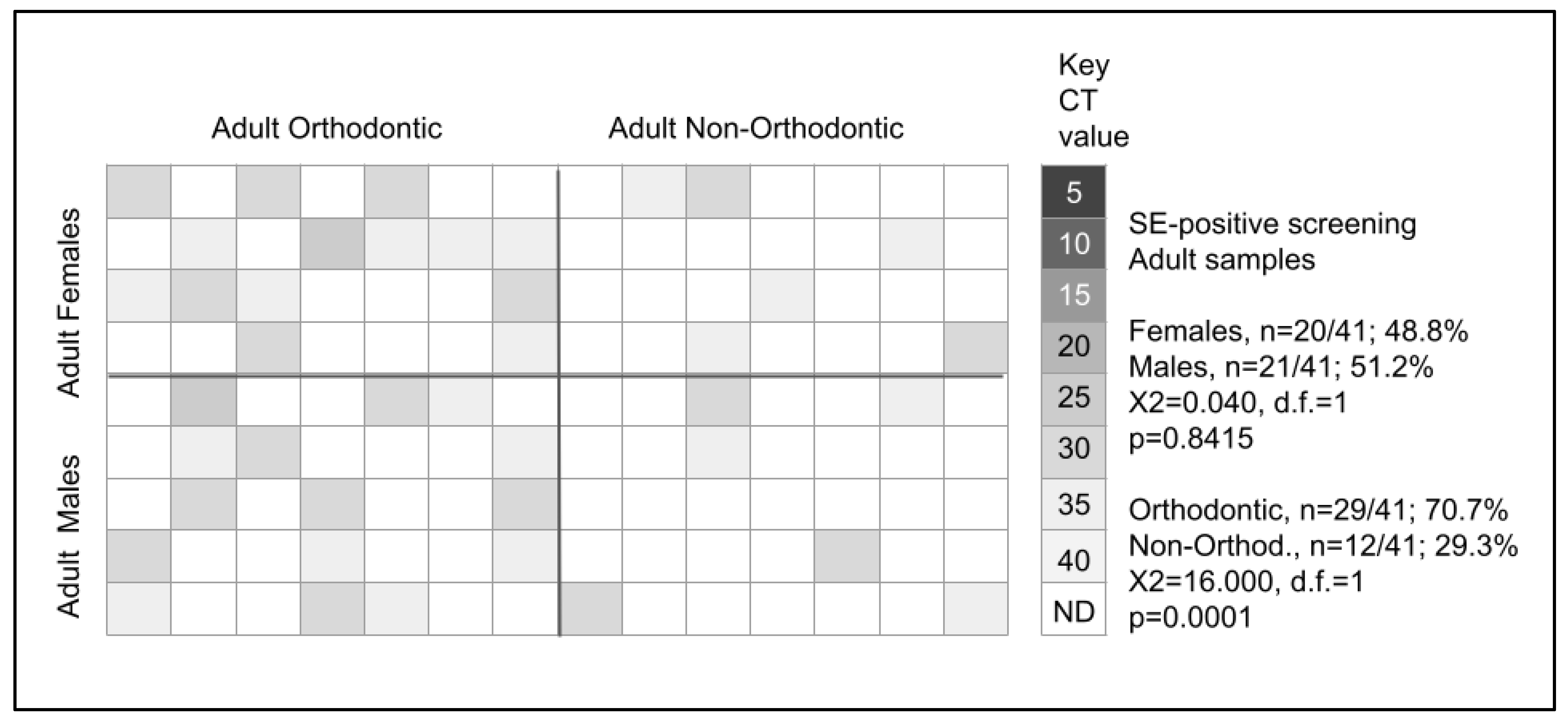
| Adult Male | n = 21/63 (33.3%) | n = 42/63 (66.7%) | X2 = 0.030, d.f. = 1 |
| Adult Female | n = 20/62 (32.3%) | n = 42/62 (67.7%) | p = 0.8633 |
| Age | |||
| Adult | n = 41/125 (32.8%) | n = 84/125 (67.2%) | X2 = 11.560, d.f. = 1 |
| Pediatric | n = 70/141 (49.6%) | n = 71/141 (50.4%) | p = 0.0007 |
| Adult Orthodontic | n = 29/60 (48.3%) | n = 31/60 (51.7%) | X2 = 16.006, d.f. = 1 |
| Pediatric Orthodontic | n = 50/70 (71.4%) | n = 20/70 (28.6%) | p = 0.001 |
| Adult Non-Orthodontic | n = 12/65 (18.4%) | n = 53/65 (81.6%) | X2 = 4.960, d.f. = 1 |
| Pediatric Non-Orthodontic | n = 20/71 (28.2%) | n = 51/71 (71.8%) | p = 0.0259 |
| Orthodontic status | |||
| Orthodontic | n = 79/130 (60.8%) | n = 51/130 (39.2%) | X2 = 54.000, d.f. = 1 |
| Non-orthodontic | n = 32/136 (23.5%) | n = 104/136 (76.5%) | p = 0.0001 |
| Male Orthodontic | n = 42/65 (64.6%) | n = 23/65 (35.4%) | X2 = 2.611, d.f. = 1 |
| Female Orthodontic | n = 37/65 (56.9%) | n = 28/65 (43.1%) | p = 0.1061 |
| Male Non-Orthodontic | n = 17/69 (24.6%) | n = 52/69 (75.4%) | X2 = 0.524, d.f. = 1 |
| Female Non-Orthodontic | n = 15/67 (22.4%) | n = 52/67 (77.6%) | p = 0.4689 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shen, C.; Simpson, J.; Clawson, J.B.; Lam, S.; Kingsley, K. Prevalence of Oral Pathogen Slackia exigua among Clinical Orthodontic and Non-Orthodontic Saliva Samples. Microorganisms 2023, 11, 867. https://doi.org/10.3390/microorganisms11040867
Shen C, Simpson J, Clawson JB, Lam S, Kingsley K. Prevalence of Oral Pathogen Slackia exigua among Clinical Orthodontic and Non-Orthodontic Saliva Samples. Microorganisms. 2023; 11(4):867. https://doi.org/10.3390/microorganisms11040867
Chicago/Turabian StyleShen, Ching, Justin Simpson, James Brigham Clawson, Steven Lam, and Karl Kingsley. 2023. "Prevalence of Oral Pathogen Slackia exigua among Clinical Orthodontic and Non-Orthodontic Saliva Samples" Microorganisms 11, no. 4: 867. https://doi.org/10.3390/microorganisms11040867