
Regulation of Gut Microbiota through Breast Milk Feeding Benefits Language and Cognitive Development of Preterm Toddlers

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Data Collection
2.3. Language and Cognitive Developmental Tests
2.4. Fecal Sample Collection
2.5. 16S rRNA Gene Amplicon Sequencing
2.6. Statistical Analyses
3. Results
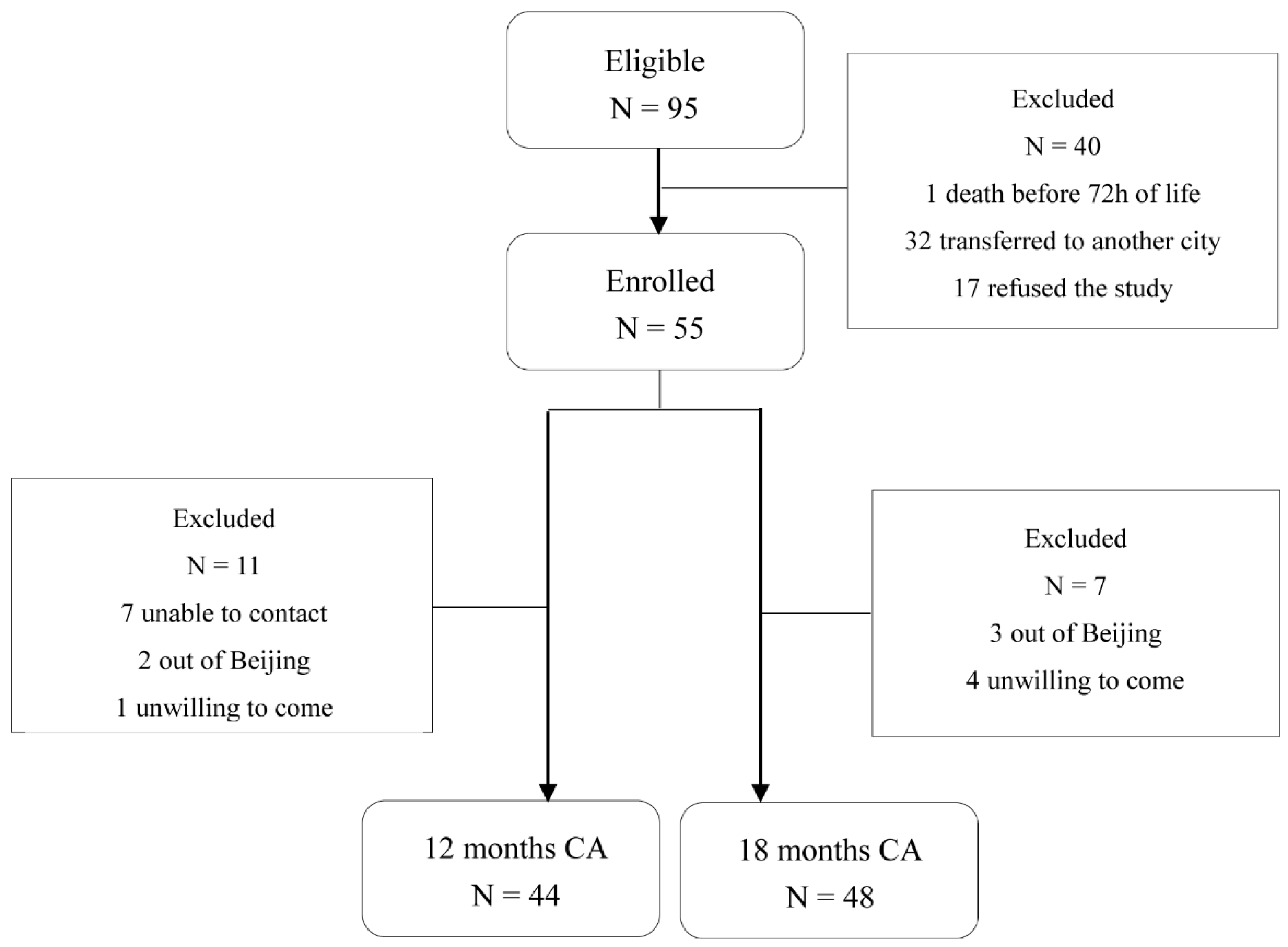
3.1. Study Population
3.2. Feeding Group
3.3. Neurodevelopment Outcome
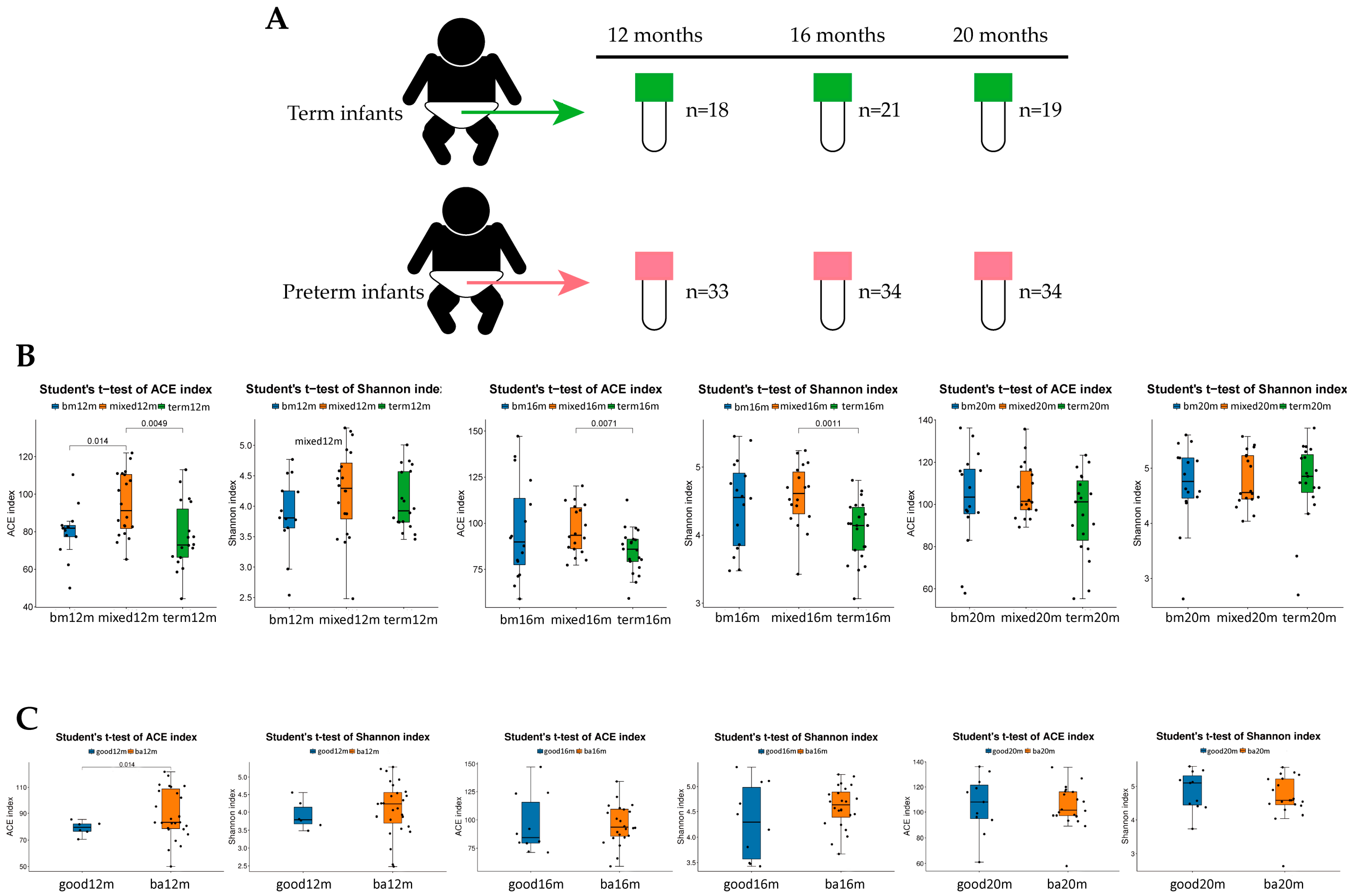
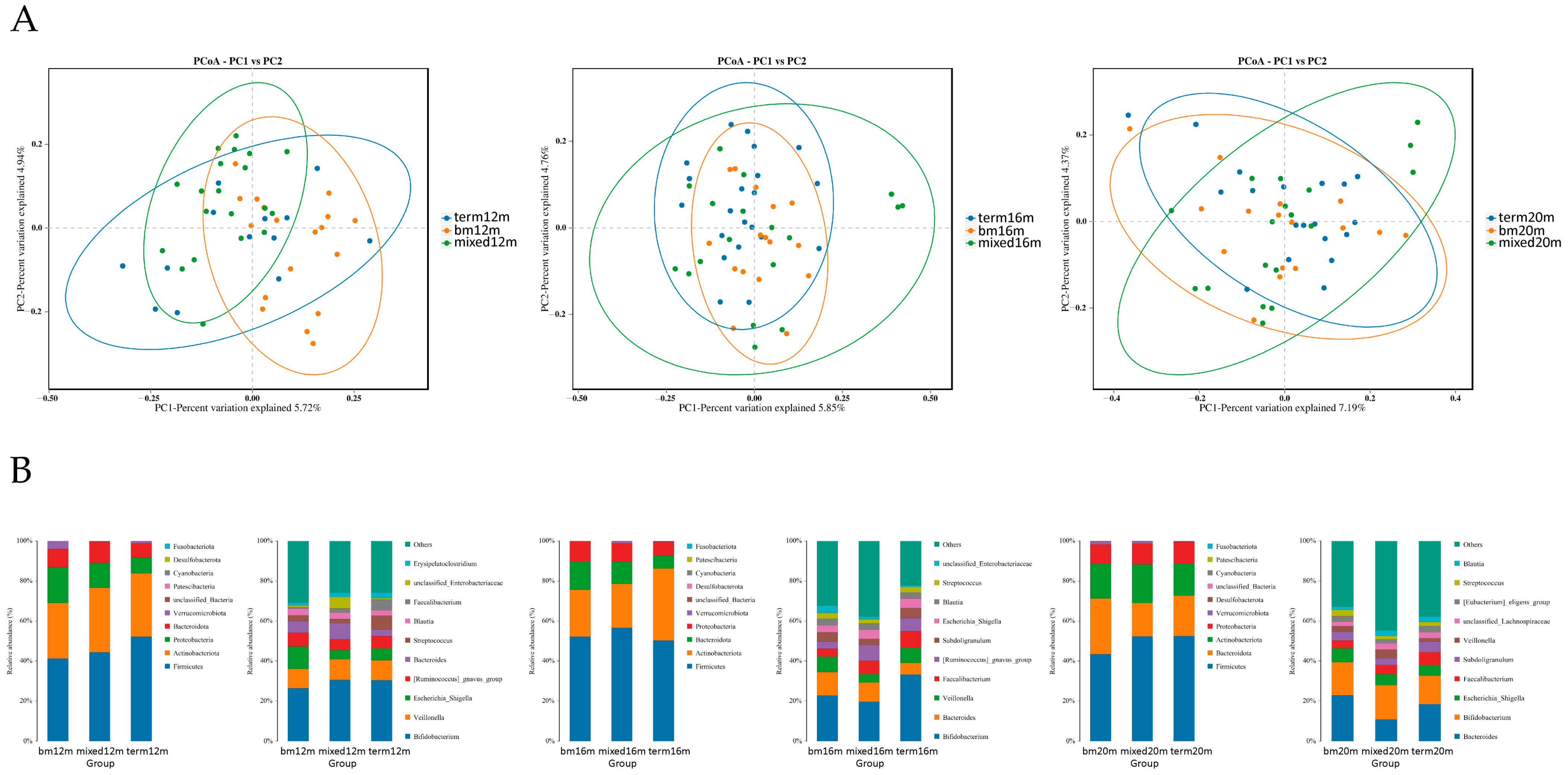
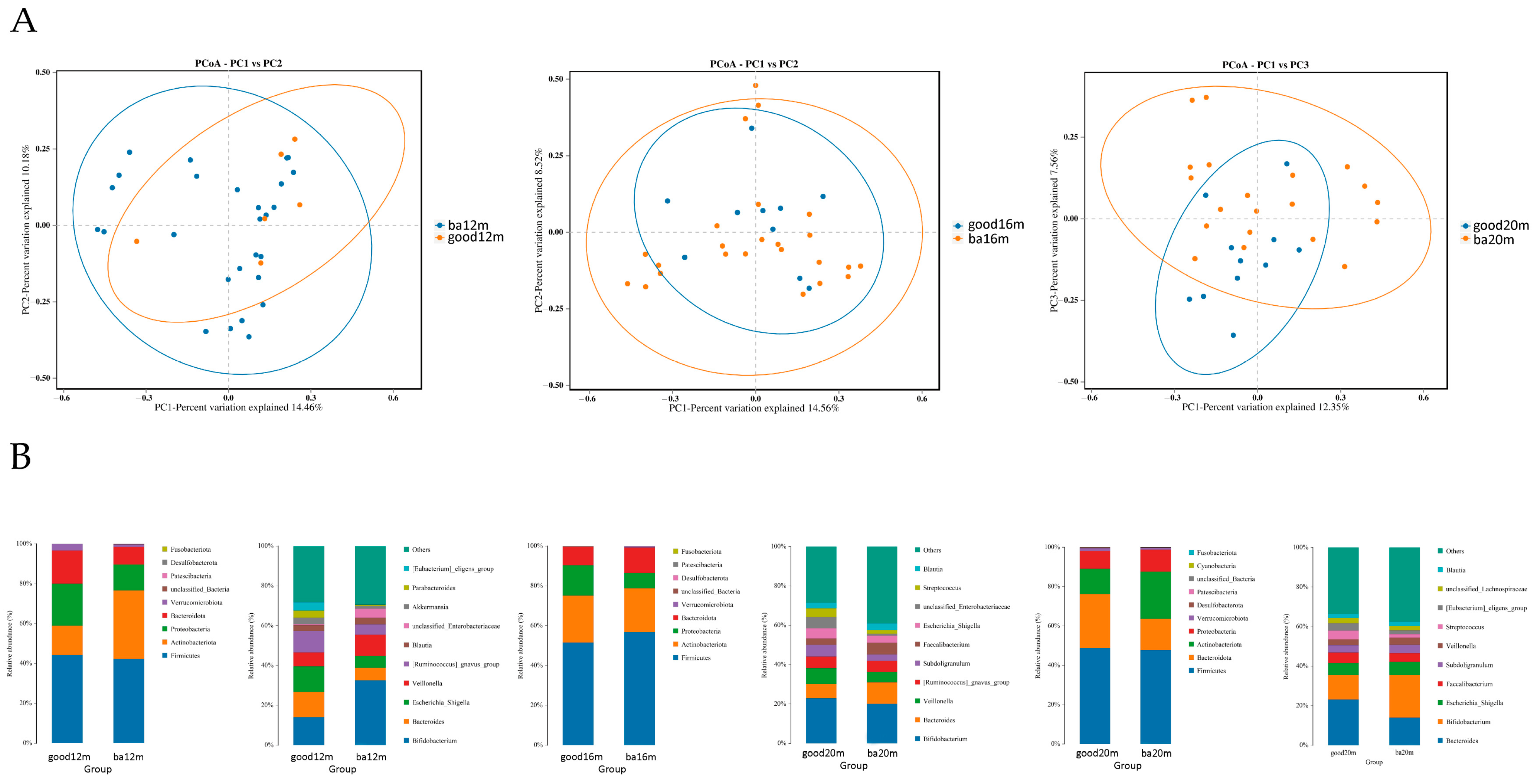
3.4. Gut Microbiota Diversity and Composition Varied by Sampling Time and Neurodevelopment Outcome
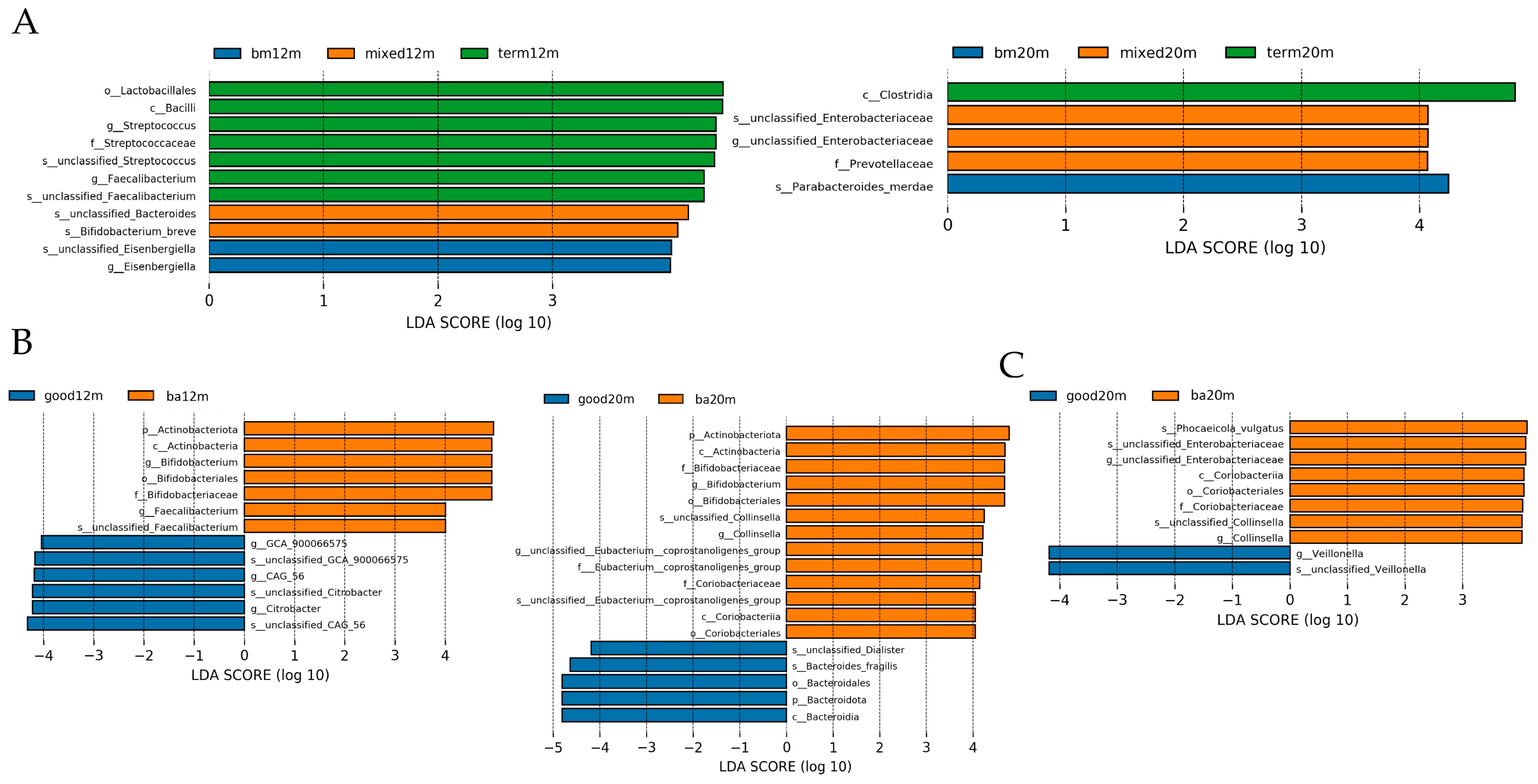
3.5. Linear Discriminant Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pierrat, V.; Marchand-Martin, L.; Marret, S.; Arnaud, C.; Benhammou, V.; Cambonie, G.; Debillon, T.; Dufourg, M.N.; Gire, C.; Goffinet, F.; et al. Neurodevelopmental outcomes at age 5 among children born preterm: EPIPAGE-2 cohort study. BMJ 2021, 373, n741. [Google Scholar] [CrossRef] [PubMed]
- Agostoni, C. LC-PUFA content in human milk: Is it always optimal? Acta Paediatr. 2005, 94, 1532–1534. [Google Scholar] [CrossRef] [PubMed]
- Einloft, P.R.; Garcia, P.C.; Piva, J.P.; Schneider, R.; Fiori, H.H.; Fiori, R.M. Supplemented vs. unsupplemented human milk on bone mineralization in very low birth weight preterm infants: A randomized clinical trial. Osteoporos. Int. 2015, 26, 2265–2271. [Google Scholar] [CrossRef]
- Cormack, B.E.; Harding, J.E.; Miller, S.P.; Bloomfield, F.H. The Influence of Early Nutrition on Brain Growth and Neu-rodevelopment in Extremely Preterm Babies: A Narrative Review. Nutrients 2019, 11, 2029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodrigues, C.; Zeitlin, J.; Zemlin, M.; Wilson, E.; Pedersen, P.; Barros, H. Never-breastfed children face a higher risk of suboptimal cognition at 2 years of corrected age: A multinational cohort of very preterm children. Matern. Child Nutr. 2022, 18, e13347. [Google Scholar] [CrossRef] [PubMed]
- Furman, L.; Wilson-Costello, D.; Friedman, H.; Taylor, H.G.; Minich, N.; Hack, M. The effect of neonatal maternal milk feeding on the neurodevelopmental outcome of very low birth weight infants. J. Dev. Behav. Pediatr. 2004, 25, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Pinelli, J.; Saigal, S.; Atkinson, S.A. Effect of breastmilk consumption on neurodevelopmental outcomes at 6 and 12 months of age in VLBW infants. Adv. Neonatal Care 2003, 3, 76–87. [Google Scholar] [CrossRef] [PubMed]
- Agirman, G.; Hsiao, E.Y. SnapShot: The microbiota-gut-brain axis. Cell 2021, 184, 2524. [Google Scholar] [CrossRef]
- Bayley, N. Bayley Scales of Infant and Toddler Development, 3rd ed.; Harcourt Assessment: San Antonio, TX, USA, 2006. [Google Scholar]
- Callahan, B.J.; McMurdie, P.J.; Rosen, M.J.; Han, A.W.; Johnson, A.J.; Holmes, S.P. DADA2: High-resolution sample inference from Illumina amplicon data. Nat. Methods 2016, 13, 581–583. [Google Scholar] [CrossRef] [Green Version]
- Bolyen, E.; Rideout, J.R.; Dillon, M.R.; Bokulich, N.A.; Abnet, C.C.; Al-Ghalith, G.A.; Alexander, H.; Alm, E.J.; Arumu-gam, M.; Asnicar, F.; et al. Reproducible, interactive, scalable and extensible microbiome data science using QIIME 2. Nat. Biotechnol. 2019, 37, 852–857. [Google Scholar] [CrossRef]
- Vohr, B.R. Neurodevelopmental outcomes of extremely preterm infants. Clin. Perinatol. 2014, 41, 241–255. [Google Scholar] [CrossRef] [PubMed]
- Cerasani, J.; Ceroni, F.; De Cosmi, V.; Mazzocchi, A.; Morniroli, D.; Roggero, P.; Mosca, F.; Agostoni, C.; Giannì, M.L. Human Milk Feeding and Preterm Infants’ Growth and Body Composition: A Literature Review. Nutrients 2020, 12, 1155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacobi-Polishook, T.; Collins, C.T.; Sullivan, T.R.; Simmer, K.; Gillman, M.W.; Gibson, R.A.; Makrides, M.; Belfort, M.B. Human milk intake in preterm infants and neurodevelopment at 18 months corrected age. Pediatr. Res. 2016, 80, 486–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bier, J.A.; Oliver, T.; Ferguson, A.E.; Vohr, B.R. Human milk improves cognitive and motor development of premature infants during infancy. J. Hum. Lact. 2002, 18, 361–367. [Google Scholar] [CrossRef] [PubMed]
- Gibertoni, D.; Corvaglia, L.; Vandini, S.; Rucci, P.; Savini, S.; Alessandroni, R.; Sansavini, A.; Fantini, M.P.; Faldella, G. Positive effect of human milk feeding during NICU hospitalization on 24 month neurodevelopment of very low birth weight infants: An Italian cohort study. PLoS ONE 2015, 10, e116552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patra, K.; Hamilton, M.; Johnson, T.J.; Greene, M.; Dabrowski, E.; Meier, P.P.; Patel, A.L. NICU Human Milk Dose and 20-Month Neurodevelopmental Outcome in Very Low Birth Weight Infants. Neonatology 2017, 112, 330–336. [Google Scholar] [CrossRef]
- Ruys, C.A.; Bröring, T.; van Schie, P.; van de Lagemaat, M.; Rotteveel, J.; Finken, M.; Oostrom, K.J.; Lafeber, H.N. Neurodevelopment of children born very preterm and/or with a very low birth weight: 8-Year follow-up of a nutritional RCT. Clin. Nutr. ESPEN 2019, 30, 190–198. [Google Scholar] [CrossRef]
- Lapidaire, W.; Lucas, A.; Clayden, J.D.; Clark, C.; Fewtrell, M.S. Human milk feeding and cognitive outcome in preterm infants: The role of infection and NEC reduction. Pediatr. Res. 2021, 91, 1207–1214. [Google Scholar] [CrossRef]
- Stewart, C.J.; Ajami, N.J.; O’Brien, J.L.; Hutchinson, D.S.; Smith, D.P.; Wong, M.C.; Ross, M.C.; Lloyd, R.E.; Doddap-aneni, H.; Metcalf, G.A.; et al. Temporal development of the gut microbiome in early childhood from the TEDDY study. Nature 2018, 562, 583–588. [Google Scholar] [CrossRef] [Green Version]
- Abrahamsson, T.R.; Jakobsson, H.E.; Andersson, A.F.; Björkstén, B.; Engstrand, L.; Jenmalm, M.C. Low gut microbiota diversity in early infancy precedes asthma at school age. Clin. Exp. Allergy 2014, 44, 842–850. [Google Scholar] [CrossRef] [Green Version]
- Kostic, A.D.; Gevers, D.; Siljander, H.; Vatanen, T.; Hyötyläinen, T.; Hämäläinen, A.M.; Peet, A.; Tillmann, V.; Pöhö, P.; Mattila, I.; et al. The dynamics of the human infant gut microbiome in development and in progression toward type 1 diabetes. Cell Host Microbe 2015, 17, 260–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finegold, S.M.; Dowd, S.E.; Gontcharova, V.; Liu, C.; Henley, K.E.; Wolcott, R.D.; Youn, E.; Summanen, P.H.; Granpeesheh, D.; Dixon, D.; et al. Pyrosequencing study of fecal microflora of autistic and control children. Anaerobe 2010, 16, 444–453. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Ling, Z.; Zhang, Y.; Mao, H.; Ma, Z.; Yin, Y.; Wang, W.; Tang, W.; Tan, Z.; Shi, J.; et al. Altered fecal microbiota composition in patients with major depressive disorder. Brain Behav. Immun. 2015, 48, 186–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carlson, A.L.; Xia, K.; Azcarate-Peril, M.A.; Goldman, B.D.; Ahn, M.; Styner, M.A.; Thompson, A.L.; Geng, X.; Gilmore, J.H.; Knickmeyer, R.C. Infant Gut Microbiome Associated with Cognitive Development. Biol. Psychiatry 2018, 83, 148–159. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Neupane, A.; Vo, R.; White, J.; Wang, X.; Marzano, S.L. Comparing Gut Microbiome in Mothers’ Own Breast Milk- and Formula-Fed Moderate-Late Preterm Infants. Front. Microbiol. 2020, 11, 891. [Google Scholar] [CrossRef]
- Aguilar-Lopez, M.; Wetzel, C.; MacDonald, A.; Ho, T.; Donovan, S.M. Human Milk-Based or Bovine Milk-Based Fortifiers Differentially Impact the Development of the Gut Microbiota of Preterm Infants. Front. Pediatr. 2021, 9, 719096. [Google Scholar] [CrossRef] [PubMed]
- Fehr, K.; Moossavi, S.; Sbihi, H.; Boutin, R.; Bode, L.; Robertson, B.; Yonemitsu, C.; Field, C.J.; Becker, A.B.; Mandhane, P.J.; et al. Breastmilk Feeding Practices Are Associated with the Co-Occurrence of Bacteria in Mothers’ Milk and the Infant Gut: The CHILD Cohort Study. Cell. Host Microbe 2020, 28, 285–297. [Google Scholar] [CrossRef]
- Guzzardi, M.A.; Ederveen, T.; Rizzo, F.; Weisz, A.; Collado, M.C.; Muratori, F.; Gross, G.; Alkema, W.; Iozzo, P. Ma-ternal pre-pregnancy overweight and neonatal gut bacterial colonization are associated with cognitive development and gut microbiota composition in pre-school-age offspring. Brain Behav. Immun. 2022, 100, 311–320. [Google Scholar] [CrossRef]
- Jia, J.; Xun, P.; Wang, X.; He, K.; Tang, Q.; Zhang, T.; Wang, Y.; Tang, W.; Lu, L.; Yan, W.; et al. Impact of Postnatal Antibiotics and Parenteral Nutrition on the Gut Microbiota in Preterm Infants During Early Life. JPEN J. Parenter. Enteral Nutr. 2020, 44, 639–654. [Google Scholar] [CrossRef]
- Tamana, S.K.; Tun, H.M.; Konya, T.; Chari, R.S.; Field, C.J.; Guttman, D.S.; Becker, A.B.; Moraes, T.J.; Turvey, S.E.; Subbarao, P.; et al. Bacteroides-dominant gut microbiome of late infancy is associated with enhanced neurodevelopment. Gut Microbes 2021, 13, 1930875. [Google Scholar] [CrossRef]
- Groer, M.W.; Luciano, A.A.; Dishaw, L.J.; Ashmeade, T.L.; Miller, E.; Gilbert, J.A. Development of the preterm infant gut microbiome: A research priority. Microbiome 2014, 2, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiciński, M.; Sawicka, E.; Gębalski, J.; Kubiak, K.; Malinowski, B. Human Milk Oligosaccharides: Health Benefits, Po-tential Applications in Infant Formulas, and Pharmacology. Nutrients 2020, 12, 266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cong, X.; Judge, M.; Xu, W.; Diallo, A.; Janton, S.; Brownell, E.A.; Maas, K.; Graf, J. Influence of Feeding Type on Gut Microbiome Development in Hospitalized Preterm Infants. Nurs. Res. 2017, 66, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Jakobsson, H.E.; Abrahamsson, T.R.; Jenmalm, M.C.; Harris, K.; Quince, C.; Jernberg, C.; Björkstén, B.; Engstrand, L.; Andersson, A.F. Decreased gut microbiota diversity, delayed Bacteroidetes colonisation and reduced Th1 responses in infants delivered by caesarean section. Gut 2014, 63, 559–566. [Google Scholar] [CrossRef] [Green Version]
- Tremaroli, V.; Bäckhed, F. Functional interactions between the gut microbiota and host metabolism. Nature 2012, 489, 242–249. [Google Scholar] [CrossRef]
- Deoni, S.C.; Dean, D.R.; Piryatinsky, I.; O’Muircheartaigh, J.; Waskiewicz, N.; Lehman, K.; Han, M.; Dirks, H. Breast-feeding and early white matter development: A cross-sectional study. Neuroimage 2013, 82, 77–86. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.C.; Chen, Y.J.; Huang, C.C.; Shieh, C.C. Concentrated Preterm Formula as a Liquid Human Milk Fortifier at Initia-tion Stage in Extremely Low Birth Weight Preterm Infants: Short Term and 2-year Follow-up Outcomes. Nutrients 2020, 12, 2229. [Google Scholar] [CrossRef]
- Quigley, M.; Embleton, N.D.; McGuire, W. Formula versus donor breast milk for feeding preterm or low birth weight infants. Cochrane Database Syst. Rev. 2018, 6, D2971. [Google Scholar] [CrossRef]
- Barrett, E.; Ross, R.P.; O’Toole, P.W.; Fitzgerald, G.F.; Stanton, C. Aminobutyric acid production by culturable bacteria from the human intestine. J. Appl. Microbiol. 2012, 113, 411–417. [Google Scholar] [CrossRef]
- Pärtty, A.; Kalliomäki, M.; Wacklin, P.; Salminen, S.; Isolauri, E. A possible link between early probiotic intervention and the risk of neuropsychiatric disorders later in childhood: A randomized trial. Pediatr. Res. 2015, 77, 823–828. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Preterm Toddlers n = 55 | Term Toddlers n = 22 | p Value | ||
|---|---|---|---|---|
| Male | n (%) | 27 (49.1) | 9 (40.9) | 0.516 |
| Gestational age, week | median (IQR) | 35 (33–36) | 39 (38–40) | 0.000 |
| Birth weight, g | mean (SD) | 2015.73 (422.78) | 3636.95 (500.19) | 0.000 |
| Type of feeding | 0.000 | |||
| Breast milk feeding | n (%) | 25 (45.5) | 22 (100) | |
| Mixed feeding | n (%) | 27 (49.1) | 0 (0) | |
| Formula feeding | n (%) | 3 (5.5) | 0 (0) |
| 12 Months CA N = 44 | 18 Months CA N = 48 | p Value | ||
|---|---|---|---|---|
| Male | n (%) | 22 (50) | 20 (43) | 0.423 |
| Gestational age, week | median (IQMR) | 35 (34–36) | 35 (32–36) | 0.213 |
| Birth weight, g | mean (SD) | 2117.8 (331.4) | 2004.3 (425.6) | 0.159 |
| Head circumference, cm | median (IQR) | 32 (30, 32.88) | 31 (30, 32.5) | 0.367 |
| Length, cm | mean (SD) | 44.6 (2.9) | 43.9 (3.3) | 0.264 |
| 1 min Apgar score | median (IQR) | 10 (9–10) | 10 (9–10) | 0.153 |
| 5 min Apgar score | median (IQR) | 10 (10–10) | 10 (10–10) | 0.107 |
| 10 min Apgar score | median (IQR) | 10 (10–10) | 10 (10–10) | 0.107 |
| Hospitalization days | median (IQR) | 10 (8–16) | 11(8–25.5) | 0.200 |
| Caesarean delivery | n (%) | 35 (79.5) | 36 (75) | 0.604 |
| Neonatal purulent meningitis | n (%) | 4 (9.0) | 4 (8.3) | 0.898 |
| Intracranial hemorrhage | n (%) | 0.600 | ||
| Grade 1 | n (%) | 2 (4.5) | 3 (6.3) | |
| Grade 2 | n (%) | 1 (2.3) | 2 (4.2) | |
| Grade 4 | n (%) | 1 (2.3) | 1 (2.1) | |
| Sepsis | n (%) | 4 (9.0) | 11 (22.91) | 0.073 |
| Maternal history of disease | ||||
| Gestational hypertension | n (%) | 17 (38.6) | 17 (35.4) | 0.749 |
| Gestational diabetes | n (%) | 7 (15.9) | 7 (14.6) | 0.860 |
| Maternal education | 0.871 | |||
| <12 years | n (%) | 0 | 1 (2.1) | |
| High school | n (%) | 3 (6.8) | 4 (8.3) | |
| Associate’s degree | n (%) | 5 (11.4) | 4 (8.3) | |
| Bachelor’s degree | n (%) | 27 (61.4) | 30 (62.5) | |
| Graduate degree | n (%) | 9 (20.5) | 9 (18.8) | |
| Average family income, CNY | 0.940 | |||
| CNY 50,000–100,000 | n (%) | 5 (11.4) | 7 (14.6) | |
| CNY 100,000–200,000 | n (%) | 13 (29.5) | 15 (31.2) | |
| CNY 200,000–400,000 | n (%) | 14 (31.8) | 12 (25.0) | |
| CNY 400,000–600,000 | n (%) | 5 (11.4) | 7 (14.6) | |
| CNY >600,000 | n (%) | 7 (15.9) | 7 (14.6) | |
| Feeding mode | 0.357 | |||
| Breast milk feeding | n (%) | 16 (36.4) | 23 (47.9) | |
| Mixed feeding | n (%) | 25 (56.8) | 22 (45.8) | |
| Formula feeding | n (%) | 3 (6.8) | 3 (6.25) | |
| Pure breast milk feeding duration during first 6 months | 0.445 | |||
| Breast milk feeding | median [IQR] | 5 (4–6) | 5 (4–6) | |
| Mixed feeding | median [IQR] | 0 (0–0) | 0 (0–0) | |
| Time of weaning | ||||
| Breast milk feeding | mean (SD) | 12 (6) | 13 (8) | 0.409 |
| Mixed feeding | mean (SD) | 10 (6) | 8 (6) | 0.707 |
| 12 Months CA | Breast Milk Feeding n = 16 | Formula or Mixed Feeding n = 28 | p Value |
|---|---|---|---|
| Bayley index score (median (IQR)) | |||
| Cognitive | 110 (96.25,110) | 102.5 (90,110) | 0.507 |
| Language | 86 (79,97) | 77 (71.75,79) | 0.008 |
| Motor | 88 (85,91) | 88 (85,91) | 0.672 |
| 18 Months CA | Breast Milk Feeding n = 23 | Formula or Mixed Feeding n = 25 | p Value |
|---|---|---|---|
| Bayley index score (mean ± SD) | |||
| Cognitive | 107.17 ± 10.85 | 99.00 ± 9.24 | 0.007 |
| Language | 106.05 ± 14.68 | 90.58 ± 12.25 | 0.000 |
| Motor | 102.04 ± 6.22 | 98.00 ± 8.22 | 0.062 |
| Language Composite Score at 12 Months CA | Language Composite Score at 18 Months CA | Cognitive Composite Score at 18 Months CA | ||||
|---|---|---|---|---|---|---|
| B (95%CI) | p | B (95%CI) | p | B (95%CI) | p | |
| Feeding mode | 10.121 (2.54, 17.70) | 0.011 | 12.46 (3.18, 21.73) | 0.010 | 8.41 (2.11, 14.71) | 0.010 |
| Gestational age | −0.94 (−4.84, 2.96) | 0.625 | −3.40 (−7.39, 5.91) | 0.093 | 0.25 (−2.51, 3.02) | 0.854 |
| Birth weight | −0.02 (−0.04, 0.01) | 0.150 | 0.00 (−0.02, 0.03) | 0.733 | −0.02 (−0.04, 0.00) | 0.053 |
| Neonatal purulent meningitis | 1.76 (−27.24, 30.76) | 0.902 | −1.86 (−25.60,21.88) | 0.875 | 10.83 (−5.28, 26.95) | 0.181 |
| Intracranial hemorrhage | −4.78 (−11.70,2.16) | 0.170 | −1.54 (−7.77, 4.70) | 0.620 | 0.60 (−3.73,4.94) | 0.780 |
| Sepsis | 10.42 (−10.31, 31.15) | 0.313 | 0.97 (−2.19, 4.12) | 0.539 | 0.59 (−1.61,2.79) | 0.591 |
| Antibiotics use duration | −0.45 (−1.47, 0.58) | 0.378 | −0.49 (−1.35, 0.38) | 0.263 | −0.53 (−1.12,0.07) | 0.083 |
| Siblings | −2.08 (−9.80, 5.64) | 0.586 | 2.70 (−6.83, 12.21) | 0.570 | −1.27 (−7.83,5.30) | 0.697 |
| Maternal BMI | −0.87 (−2.06, 0.33) | 0.149 | −0.66 (2.34, 1.02) | 0.432 | 0.43 (−0.74,1.59) | 0.464 |
| Family income | −0.11 (−0.32, 0.10) | 0.283 | 0.04 (−0.23, 0.31) | 0.769 | 0.00 (−0.19, 0.19) | 0.996 |
| Maternal education | −1.33 (−6.39, 3.73) | 0.595 | 1.15 (−4.26, 6.56) | 0.668 | 2.49 (−1.23,6.22) | 0.183 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, S.; Huang, K.; Liu, R.; Sun, J.; Yin, C. Regulation of Gut Microbiota through Breast Milk Feeding Benefits Language and Cognitive Development of Preterm Toddlers. Microorganisms 2023, 11, 866. https://doi.org/10.3390/microorganisms11040866
Guo S, Huang K, Liu R, Sun J, Yin C. Regulation of Gut Microbiota through Breast Milk Feeding Benefits Language and Cognitive Development of Preterm Toddlers. Microorganisms. 2023; 11(4):866. https://doi.org/10.3390/microorganisms11040866
Chicago/Turabian StyleGuo, Shan, Kaikun Huang, Ruixia Liu, Jing Sun, and Chenghong Yin. 2023. "Regulation of Gut Microbiota through Breast Milk Feeding Benefits Language and Cognitive Development of Preterm Toddlers" Microorganisms 11, no. 4: 866. https://doi.org/10.3390/microorganisms11040866