
Seroprevalence and Risk Factors of Lyme Borreliosis in The Netherlands: A Population-Based Cross-Sectional Study
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Laboratory Analysis
2.3. Data Analysis
3. Results
3.1. Study Population
3.2. Laboratory Analysis
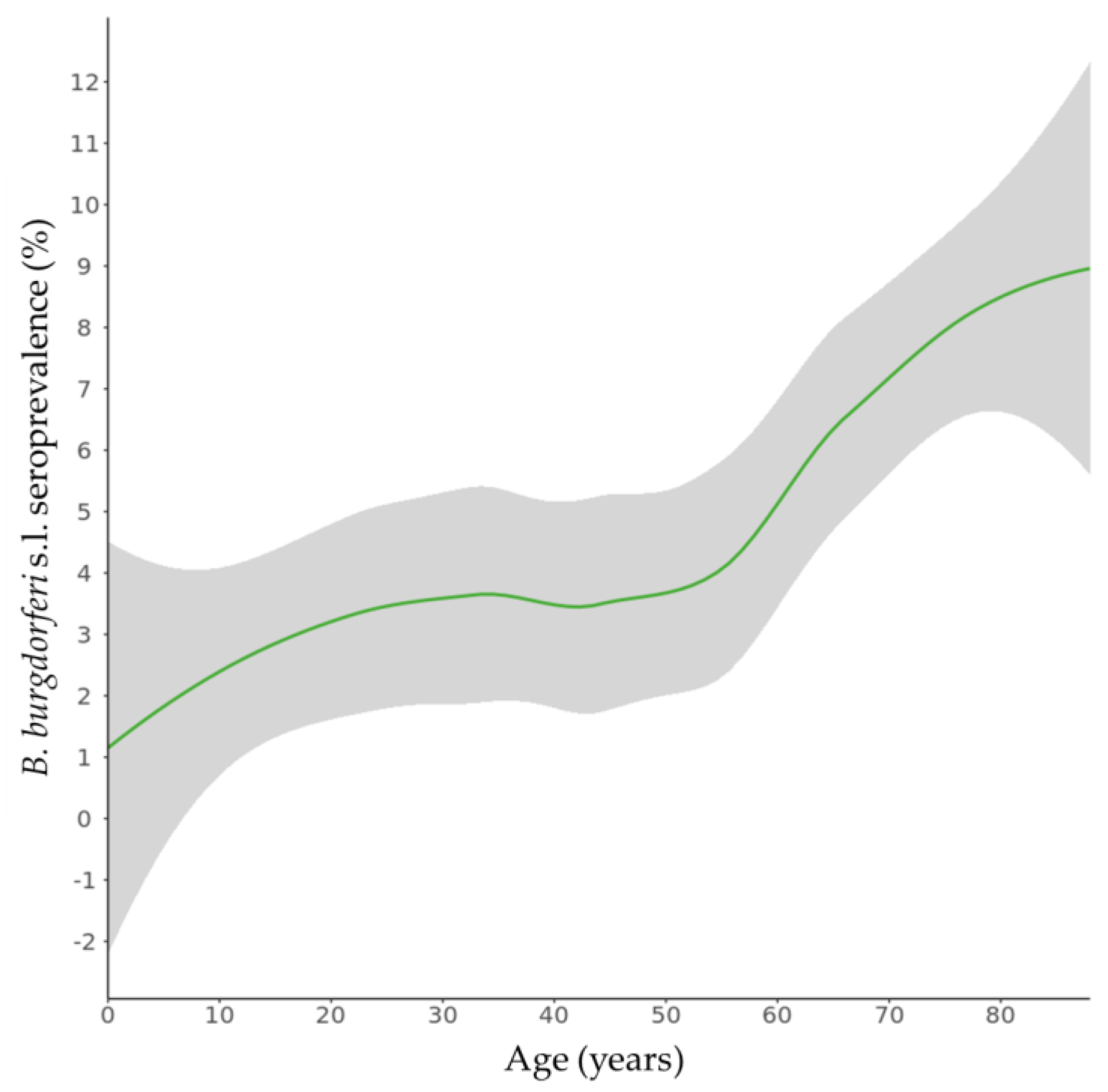
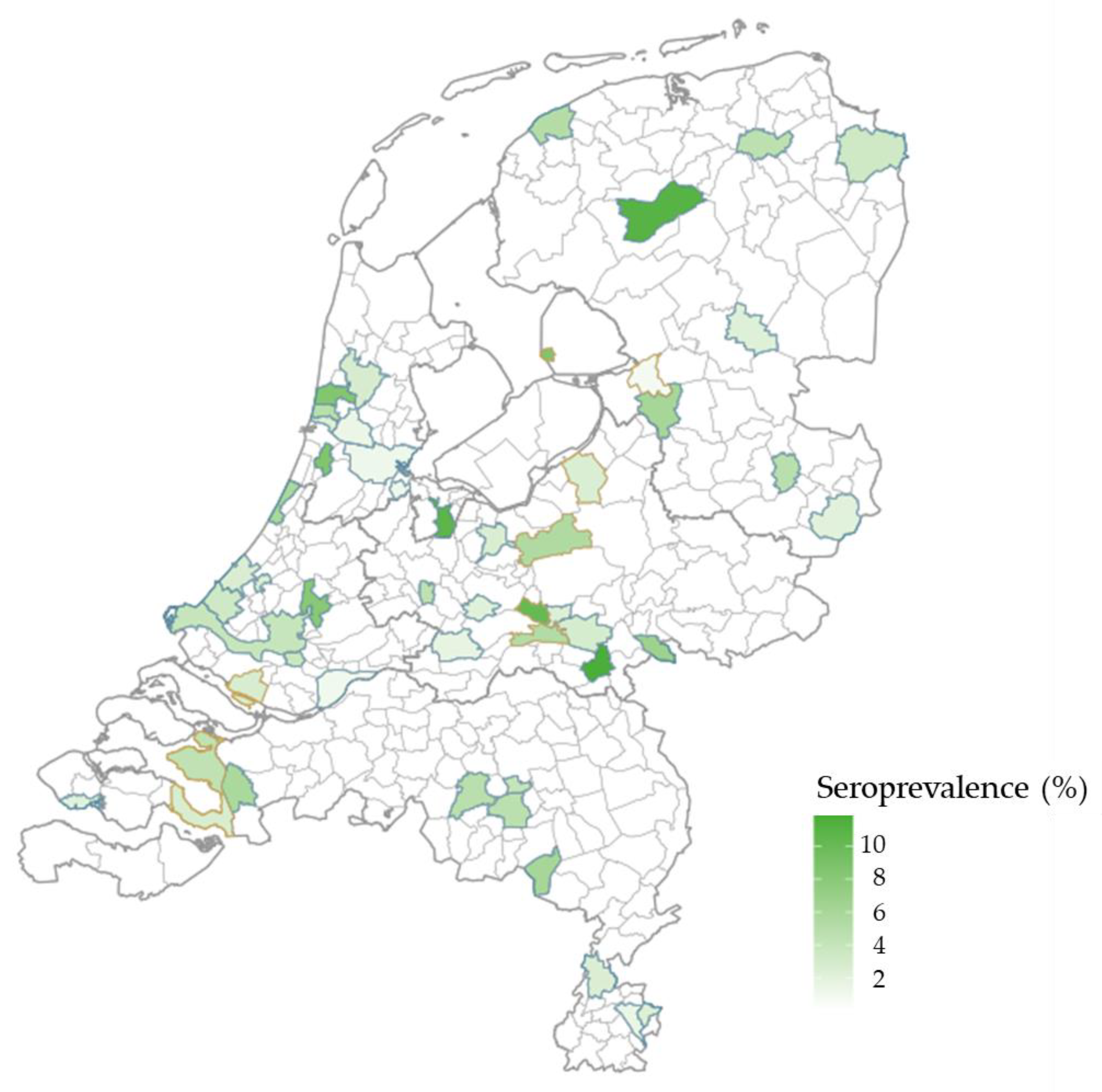
3.3. Seroprevalence Estimates
3.4. Risk Factor Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Branda, J.A.; Steere, A.C. Laboratory Diagnosis of Lyme Borreliosis. Clin. Microbiol. Rev. 2021, 34, e00018–e00019. [Google Scholar] [CrossRef] [PubMed]
- van den Wijngaard, C.C.; Hofhuis, A.; Harms, M.G.; Haagsma, J.A.; Wong, A.; de Wit, G.A.; Havelaar, A.H.; Lugner, A.K.; Suijkerbuijk, A.W.; van Pelt, W. The burden of Lyme borreliosis expressed in disability-adjusted life years. Eur. J. Public Health 2015, 25, 1071–1078. [Google Scholar] [CrossRef] [PubMed]
- van den Wijngaard, C.C.; Hofhuis, A.; Simoes, M.; Rood, E.; van Pelt, W.; Zeller, H.; Van Bortel, W. Surveillance perspective on Lyme borreliosis across the European Union and European Economic Area. Euro Surveill. 2017, 22, 30569. [Google Scholar] [CrossRef]
- ECDC. ECDC Comment: European Commission Updates Communicable Disease Surveillance List—Lyme Neuroborreliosis Now under EU/EEA Surveillance. Available online: https://www.ecdc.europa.eu/en/news-events/ecdc-comment-european-commission-updates-communicable-disease-surveillance-list-lyme (accessed on 11 January 2023).
- Hofhuis, A.; Harms, M.; Bennema, S.; van den Wijngaard, C.C.; van Pelt, W. Physician reported incidence of early and late Lyme borreliosis. Parasit. Vectors 2015, 8, 161. [Google Scholar] [CrossRef] [PubMed]
- Lernout, T.; Kabamba-Mukadi, B.; Saegeman, V.; Tre-Hardy, M.; de Laveleye, M.; Asikainen, T.; Dessau, R.B.; Quoilin, S.; Litzroth, A. The value of seroprevalence data as surveillance tool for Lyme borreliosis in the general population: The experience of Belgium. BMC Public Health 2019, 19, 597. [Google Scholar] [CrossRef]
- De Melker, H.E.; Conyn-van Spaendonck, M.A. Immunosurveillance and the evaluation of national immunization programmes: A population-based approach. Epidemiol. Infect. 1998, 121, 637–643. [Google Scholar] [CrossRef] [PubMed]
- van der Klis, F.R.; Mollema, L.; Berbers, G.A.; de Melker, H.E.; Coutinho, R.A. Second national serum bank for population-based seroprevalence studies in The Netherlands. Neth. J. Med. 2009, 67, 301–308. [Google Scholar]
- Verberk, J.D.M.; Vos, R.A.; Mollema, L.; van Vliet, J.; van Weert, J.W.M.; de Melker, H.E.; van der Klis, F.R.M. Third national biobank for population-based seroprevalence studies in The Netherlands, including the Caribbean Netherlands. BMC Infect. Dis. 2019, 19, 470. [Google Scholar] [CrossRef]
- Schimmer, B.; Notermans, D.W.; Harms, M.G.; Reimerink, J.H.; Bakker, J.; Schneeberger, P.; Mollema, L.; Teunis, P.; van Pelt, W.; van Duynhoven, Y. Low seroprevalence of Q fever in The Netherlands prior to a series of large outbreaks. Epidemiol. Infect. 2012, 140, 27–35. [Google Scholar] [CrossRef]
- Korndewal, M.J.; Mollema, L.; Tcherniaeva, I.; van der Klis, F.; Kroes, A.C.; Oudesluys-Murphy, A.M.; Vossen, A.C.; de Melker, H.E. Cytomegalovirus infection in The Netherlands: Seroprevalence, risk factors, and implications. J. Clin. Virol. 2015, 63, 53–58. [Google Scholar] [CrossRef]
- Liang, F.T.; Steere, A.C.; Marques, A.R.; Johnson, B.J.; Miller, J.N.; Philipp, M.T. Sensitive and specific serodiagnosis of Lyme disease by enzyme-linked immunosorbent assay with a peptide based on an immunodominant conserved region of Borrelia burgdorferi vlsE. J. Clin. Microbiol. 1999, 37, 3990–3996. [Google Scholar] [CrossRef] [PubMed]
- Team, R.C. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022. [Google Scholar]
- Lumley, T. Analysis of Complex Survey Samples. J. Stat. Softw. 2004, 9, 1–19. [Google Scholar] [CrossRef]
- Bates, D.; Mächler, M.; Bolker, B.; Walker, S. Fitting Linear Mixed-Effects Models Using lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- Johansson, M.; Manfredsson, L.; Wistedt, A.; Serrander, L.; Tjernberg, I. Significant variations in the seroprevalence of C6 ELISA antibodies in a highly endemic area for Lyme borreliosis: Evaluation of age, sex and seasonal differences. APMIS 2017, 125, 476–481. [Google Scholar] [CrossRef] [PubMed]
- Strnad, M.; Honig, V.; Ruzek, D.; Grubhoffer, L.; Rego, R.O.M. Europe-Wide Meta-Analysis of Borrelia burgdorferi Sensu Lato Prevalence in Questing Ixodes ricinus Ticks. Appl. Environ. Microbiol. 2017, 83, e00609-17. [Google Scholar] [CrossRef] [PubMed]
- Cuellar, J.; Dub, T.; Sane, J.; Hytonen, J. Seroprevalence of Lyme borreliosis in Finland 50 years ago. Clin. Microbiol. Infect. 2020, 26, 632–636. [Google Scholar] [CrossRef] [PubMed]
- van den Wijngaard, C.C.; Brown, V.; Harms, M.; van Pelt, W.; Hofhuis, A. Increase in the Incidence and Burden of Lyme borreliosis in The Netherlands between 2014 and 2017. Available online: https://www.rivm.nl/documenten/increase-in-incidence-and-burden-of-lyme-borreliosis-in-netherlands-between-2014-and (accessed on 10 January 2023).
- Dessau, R.B.; van Dam, A.P.; Fingerle, V.; Gray, J.; Hovius, J.W.; Hunfeld, K.P.; Jaulhac, B.; Kahl, O.; Kristoferitsch, W.; Lindgren, P.E.; et al. To test or not to test? Laboratory support for the diagnosis of Lyme borreliosis: A position paper of ESGBOR, the ESCMID study group for Lyme borreliosis. Clin. Microbiol. Infect. 2018, 24, 118–124. [Google Scholar] [CrossRef]
- Lipsett, S.C.; Branda, J.A.; McAdam, A.J.; Vernacchio, L.; Gordon, C.D.; Gordon, C.R.; Nigrovic, L.E. Evaluation of the C6 Lyme Enzyme Immunoassay for the Diagnosis of Lyme Disease in Children and Adolescents. Clin. Infect. Dis. 2016, 63, 922–928. [Google Scholar] [CrossRef]
- Baarsma, M.E.; Vrijlandt, A.; Ursinus, J.; Zaaijer, H.L.; Jurriaans, S.; van Dam, A.P.; Hovius, J.W. Diagnostic performance of the ZEUS Borrelia VlsE1/pepC10 assay in European LB patients: A case-control study. Eur. J. Clin. Microbiol. Infect. Dis. 2022, 41, 387–393. [Google Scholar] [CrossRef]
- van Gorkom, T.; Kremer, K.; Voet, W.; Notermans, D.W.; Vlaminckx, B.J.M.; Sankatsing, S.U.C.; Thijsen, S.F.T. Disagreement between the results from three commercial tests for the detection of Borrelia-specific serum antibodies in The Netherlands associated with antibiotic treatment for Lyme borreliosis: A retrospective study. Eur. J. Clin. Microbiol. Infect. Dis. 2017, 36, 2137–2146. [Google Scholar] [CrossRef]
- Woudenberg, T.; Böhm, S.; Böhmer, M.; Katz, K.; Willrich, N.; Stark, K.; Kuhnert, R.; Fingerle, V.; Wilking, H. Dynamics of Borrelia burgdorferi-Specific Antibodies: Seroconversion and Seroreversion between Two Population-Based, Cross-Sectional Surveys among Adults in Germany. Microorganisms 2020, 8, 1859. [Google Scholar] [CrossRef]
- Dehnert, M.; Fingerle, V.; Klier, C.; Talaska, T.; Schlaud, M.; Krause, G.; Wilking, H.; Poggensee, G. Seropositivity of Lyme borreliosis and associated risk factors: A population-based study in Children and Adolescents in Germany (KiGGS). PLoS ONE 2012, 7, e41321. [Google Scholar] [CrossRef] [PubMed]
- Pachner, A.R.; Amemiya, K.; Bartlett, M.; Schaefer, H.; Reddy, K.; Zhang, W.F. Lyme borreliosis in rhesus macaques: Effects of corticosteroids on spirochetal load and isotype switching of anti-Borrelia burgdorferi antibody. Clin. Diagn. Lab. Immunol. 2001, 8, 225–232. [Google Scholar] [CrossRef]
- Aguero-Rosenfeld, M.E.; Nowakowski, J.; Bittker, S.; Cooper, D.; Nadelman, R.B.; Wormser, G.P. Evolution of the serologic response to Borrelia burgdorferi in treated patients with culture-confirmed erythema migrans. J. Clin. Microbiol. 1996, 34, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Markowicz, M.; Reiter, M.; Gamper, J.; Stanek, G.; Stockinger, H. Persistent Anti-Borrelia IgM Antibodies without Lyme Borreliosis in the Clinical and Immunological Context. Microbiol. Spectr. 2021, 9, e0102021. [Google Scholar] [CrossRef]
- Hoeve-Bakker, B.J.A.; Jonker, M.; Brandenburg, A.H.; den Reijer, P.M.; Stelma, F.F.; van Dam, A.P.; van Gorkom, T.; Kerkhof, K.; Thijsen, S.F.T.; Kremer, K. The Performance of Nine Commercial Serological Screening Assays for the Diagnosis of Lyme Borreliosis: A Multicenter Modified Two-Gate Design Study. Microbiol. Spectr. 2022, 10, e0051022. [Google Scholar] [CrossRef]
- Kerkhof, K.; Sluydts, V.; Willen, L.; Kim, S.; Canier, L.; Heng, S.; Tsuboi, T.; Sochantha, T.; Sovannaroth, S.; Menard, D.; et al. Serological markers to measure recent changes in malaria at population level in Cambodia. Malar. J. 2016, 15, 529. [Google Scholar] [CrossRef]
- Hofhuis, A.; van de Kassteele, J.; Sprong, H.; van den Wijngaard, C.C.; Harms, M.G.; Fonville, M.; Docters van Leeuwen, A.; Simoes, M.; van Pelt, W. Predicting the risk of Lyme borreliosis after a tick bite, using a structural equation model. PLoS ONE 2017, 12, e0181807. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| National Sample | Low NIP Vaccination Coverage Sample | |||||
|---|---|---|---|---|---|---|
| Total | Weighted Anti-Borrelia Antibodies Seroprevalence | Total | ||||
| n | % | % | 95% CI | n | % | |
| Overall | 4567 | 100 | 4.4 | 3.5–5.2 | 1025 | 100 |
| Gender | ||||||
| Female | 2511 | 55.0 | 3.1 | 2.3–4.0 | 610 | 59.5 |
| Male | 2056 | 45.0 | 5.7 | 4.4–7.2 | 415 | 40.5 |
| Age (years) | ||||||
| 0–19 | 840 | 18.4 | 2.6 | 1.4–4.4 | 205 | 20.0 |
| 20–39 | 1392 | 30.5 | 3.6 | 2.2–5.5 | 359 | 35.0 |
| 40–59 | 1188 | 26.0 | 3.6 | 2.5–5.1 | 265 | 25.9 |
| 60–88 | 1147 | 25.1 | 7.7 | 5.9–9.7 | 196 | 19.1 |
| Region 1 | ||||||
| Northeast | 916 | 20.1 | 5.2 | 2.6–9.0 | NA | NA |
| Southeast | 1135 | 24.9 | 4.2 | 3.0–5.6 | NA | NA |
| Central | 847 | 18.5 | 4.2 | 1.8–8.2 | NA | NA |
| Southwest | 870 | 19.0 | 3.7 | 2.1–5.9 | NA | NA |
| Northwest | 799 | 17.5 | 4.8 | 2.2–8.9 | NA | NA |
| LVC municipalities | NA | NA | NA | NA | 1025 | 100 |
| Degree of urbanization (addresses per km2) | ||||||
| Very high (>2500) | 988 | 21.6 | 4.3 | 2.5–6.8 | 0 | 0 |
| High (1500–2500) | 1480 | 32.4 | 4.1 | 2.6–6.0 | 0 | 0 |
| Medium (1000–1500) | 884 | 19.4 | 4.0 | 1.9–7.2 | 128 | 12.5 |
| Low (500–1000) | 829 | 18.2 | 4.0 | 2.4–6.2 | 560 | 54.6 |
| Very low (0–500) | 386 | 8.5 | 8.0 | 0.0–57.5 | 337 | 32.9 |
| Ethnicity | ||||||
| Dutch | 3604 | 78.9 | 4.7 | 3.7–5.8 | 981 | 95.7 |
| Other Western | 317 | 6.9 | 4.8 | 2.6–7.9 | 29 | 2.8 |
| Moroccan and Turkish | 112 | 2.5 | 3.2 | 0.1–15.1 | 3 | 0.3 |
| Surinamese, Aruban, The Netherlands Antillean | 223 | 4.9 | 1.2 | 0.3–3.6 | 4 | 0.4 |
| Other non-Western | 311 | 6.8 | 2.5 | 1.0–5.0 | 8 | 0.8 |
| Level of education 2 | ||||||
| Low | 1262 | 27.6 | 4.1 | 2.7–6.0 | 615 | 60.0 |
| Middle | 1480 | 32.4 | 3.1 | 2.2–4.1 | 143 | 14.0 |
| High | 1559 | 34.1 | 5.7 | 4.3–7.5 | 211 | 20.6 |
| Number of tick bites in the last 5 years | ||||||
| Never | 3364 | 73.7 | 3.4 | 2.6–4.3 | 765 | 74.6 |
| 1–4 times | 565 | 12.4 | 8.2 | 5.5–11.8 | 131 | 12.8 |
| 5–9 times | 42 | 0.9 | 8.8 | 2.3–21.7 | 9 | 0.9 |
| ≥10 times | 28 | 0.6 | 23.5 | 9.9–42.7 | 7 | 0.7 |
| Unknown | 292 | 6.4 | 4.6 | 2.6–7.4 | 67 | 6.5 |
| n | npos | % | aOR [95% CI] | ||
|---|---|---|---|---|---|
| Gender | |||||
| Female | 3121 | 99 | 3.2 | Reference | |
| Male | 2471 | 135 | 5.5 | 1.78 [1.35–2.35] | |
| Age (years) | |||||
| 0–19 | 1045 | 28 | 2.7 | Reference | |
| 20–39 | 1751 | 51 | 2.9 | 1.19 [0.73–1.92] | |
| 40–59 | 1453 | 51 | 3.5 | 1.52 [0.94–2.46] | |
| 60–88 | 1343 | 104 | 7.7 | 3.97 [2.55–6.20] | |
| Number of tick bites in the last 5 years | |||||
| Never | 4129 | 129 | 3.1 | Reference | |
| 1–4 tick bites | 696 | 54 | 7.8 | 2.52 [1.79–3.55] | |
| 5–9 tick bites | 51 | 5 | 9.8 | 2.92 [1.10–7.76] | |
| ≥10 tick bites | 35 | 9 | 25.7 | 10.01 [4.41–22.73] | |
| Unknown | 359 | 21 | 5.8 | 1.84 [1.13–2.99] | |
| Country of birth | |||||
| The Netherlands | 4928 | 219 | 4.4 | Reference | |
| Turkey and Morocco | 69 | 1 | 1.4 | 0.22 [0.03–1.65] | |
| SAN | 177 | 4 | 2.3 | 0.41 [0.15–1.17] | |
| Other | 418 | 10 | 2.4 | 0.45 [0.23–0.89] | |
| Level of education 1 | |||||
| Low | 1623 | 62 | 3.8 | Reference | |
| Middle | 1877 | 61 | 3.2 | 0.96 [0.66–1.41] | |
| High | 1770 | 95 | 5.4 | 1.40 [0.98–2.01] | |
| Use of antibiotics in the last 3 months | |||||
| Never | 4284 | 182 | 4.2 | Reference | |
| 1 time | 422 | 17 | 4.0 | 0.92 [0.54–1.54] | |
| 2 times or more | 120 | 1 | 0.8 | 0.16 [0.02–1.14] | |
| Eating pork meat | |||||
| Never | 538 | 25 | 4.6 | Reference | |
| <1 day/month | 463 | 25 | 5.4 | 1.07 [0.59–1.94] | |
| 1–3 days/month | 1220 | 53 | 4.3 | 0.78 [0.47–1.30] | |
| 1–3 days/week | 2636 | 103 | 3.9 | 0.69 [0.43–1.11] | |
| >3 days/week | 302 | 6 | 2.0 | 0.32 [0.13–0.80] | |
| Eating unwashed vegetables | |||||
| Never | 2051 | 85 | 4.1 | Reference | |
| <1 day/month | 635 | 39 | 6.1 | 1.66 [1.10–2.49] | |
| 1–3 days/month | 946 | 30 | 3.2 | 0.87 [0.56–1.35] | |
| 1–3 days/week | 1137 | 41 | 3.6 | 1.03 [0.69–1.53] | |
| >3 days/week | 474 | 24 | 5.1 | 1.76 [1.08–2.86] | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hoeve-Bakker, B.J.A.; van den Berg, O.E.; Doppenberg, H.S.; van der Klis, F.R.M.; van den Wijngaard, C.C.; Kluytmans, J.A.J.W.; Thijsen, S.F.T.; Kerkhof, K. Seroprevalence and Risk Factors of Lyme Borreliosis in The Netherlands: A Population-Based Cross-Sectional Study. Microorganisms 2023, 11, 1081. https://doi.org/10.3390/microorganisms11041081
Hoeve-Bakker BJA, van den Berg OE, Doppenberg HS, van der Klis FRM, van den Wijngaard CC, Kluytmans JAJW, Thijsen SFT, Kerkhof K. Seroprevalence and Risk Factors of Lyme Borreliosis in The Netherlands: A Population-Based Cross-Sectional Study. Microorganisms. 2023; 11(4):1081. https://doi.org/10.3390/microorganisms11041081
Chicago/Turabian StyleHoeve-Bakker, B. J. A., Oda E. van den Berg, H. S. Doppenberg, Fiona R. M. van der Klis, Cees C. van den Wijngaard, Jan A. J. W. Kluytmans, Steven F. T. Thijsen, and Karen Kerkhof. 2023. "Seroprevalence and Risk Factors of Lyme Borreliosis in The Netherlands: A Population-Based Cross-Sectional Study" Microorganisms 11, no. 4: 1081. https://doi.org/10.3390/microorganisms11041081