

Diagnostic Performance of Different Laboratory Methods for the Detection of Extrapulmonary Tuberculosis
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Settings and Participants
2.2. Specimen Processing, Microscopy and Culture
2.3. Xpert MTB/RIF Assay
2.4. GenoType MTBDRplus Assay
2.5. Statistical Analysis
3. Results
3.1. Type of EPTB Specimens and Bacteriologically Positive Cases
3.2. Overall Performance of Four Laboratory Methods in Detecting EPTB Cases
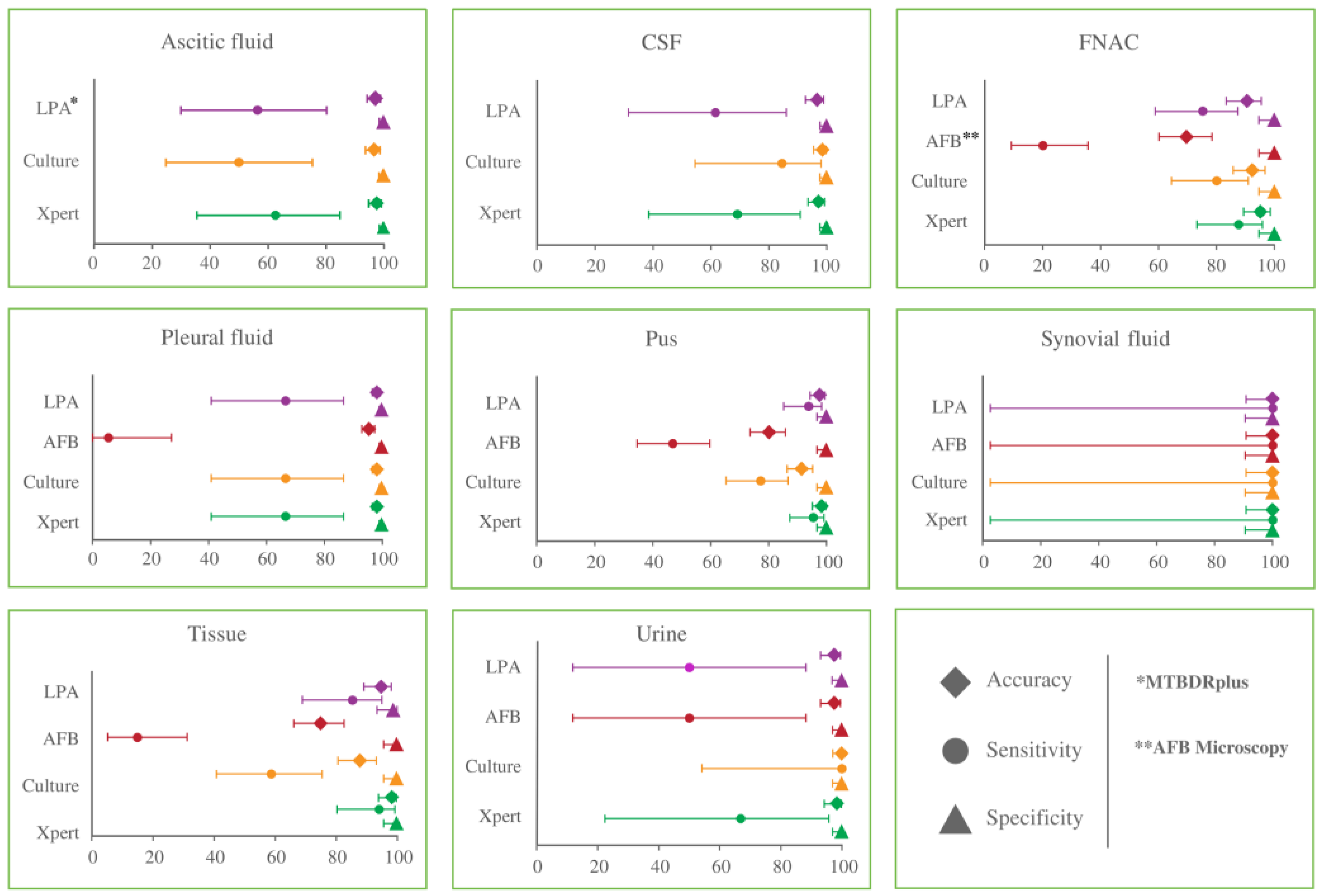
3.3. Diagnostic Performance of Four Diagnostic Methods for the Detection of EPTB Cases in Various Specimen Types
3.4. Semi-Quantitative Distribution and Detection by AFB Microscopy and Xpert MTB/RIF Assay
3.5. Comparison of Two Rapid Molecular Methods for Detection of EPTB and Rifampicin Susceptibility
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Global Tuberculosis Report 2022; WHO: Geneva, Switzerland, 2022. [Google Scholar]
- Metaferia, Y.; Seid, A.; Fenta, G.M.; Gebretsadik, D. Assessment of Extrapulmonary Tuberculosis Using Gene Xpert MTB/RIF Assay and Fluorescent Microscopy and Its Risk Factors at Dessie Referral Hospital, Northeast Ethiopia. BioMed Res. Int. 2018, 2018, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Yoon, H.J.; Song, Y.G.; Park, W.I.; Choi, J.-P.; Chang, K.H.; Kim, J.M. Clinical Manifestations and Diagnosis of Extrapulmonary Tuberculosis. Yonsei Med J. 2004, 45, 453–461. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J.; Kang, J.Y.; Kim, S.I.; Chang, M.S.; Kim, Y.R.; Park, Y.J. Predictors for false-negative QuantiFERON-TB Gold assay results in patients with extrapulmonary tuberculosis. BMC Infect. Dis. 2018, 18, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Zürcher, K.; Ballif, M.; Kiertiburanakul, S.; Chenal, H.; Yotebieng, M.; Grinsztejn, B.; Michael, D.; Sterling, T.R.; Ngonyani, K.M.; Mandalakas, A.M.; et al. Diagnosis and clinical outcomes of extrapulmonary tuberculosis in antiretroviral therapy programmes in low- and middle-income countries: A multicohort study. J. Int. AIDS Soc. 2019, 22, e25392. [Google Scholar] [CrossRef]
- Chakravorty, S.; Sen, M.K.; Tyagi, J.S. Diagnosis of Extrapulmonary Tuberculosis by Smear, Culture, and PCR Using Universal Sample Processing Technology. J. Clin. Microbiol. 2005, 43, 4357–4362. [Google Scholar] [CrossRef]
- Kabir, S.; Uddin, M.K.M.; Chisti, M.J.; Fannana, T.; Haque, M.E.; Uddin, M.R.; Banu, S.; Ahmed, T. Role of PCR method using IS6110 primer in detecting Mycobacterium tuberculosis among the clinically diagnosed childhood tuberculosis patients at an urban hospital in Dhaka, Bangladesh. Int. J. Infect. Dis. 2018, 68, 108–114. [Google Scholar] [CrossRef]
- Sankar, S.; Ramamurthy, M.; Nandagopal, B.; Sridharan, G. An Appraisal of PCR-Based Technology in the Detection of Mycobacterium tuberculosis. Mol. Diagn. Ther. 2011, 15, 1–11. [Google Scholar] [CrossRef]
- Prasad, S.; Singhal, M.; Negi, S.S.; Gupta, S.; Singh, S.; Rawat, D.S.; Rai, A. Targeted detection of 65kDa heat shock protein gene in endometrial biopsies for reliable diagnosis of genital tuberculosis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2012, 160, 215–218. [Google Scholar] [CrossRef]
- Gill, M.K.; Kukreja, S.; Chhabra, N. Evaluation of nested polymerase chain reaction for rapid diagnosis of clinically suspected tuberculous pleurisy. J. Clin. Diagn. Res. JCDR 2013, 7, 2456. [Google Scholar] [CrossRef]
- Katoch, V.M. Advances in Molecular Diagnosis of Tuberculosis. Med J. Armed Forces India 2003, 59, 182–186. [Google Scholar] [CrossRef]
- Gaur, M.; Singh, A.; Sharma, V.; Tandon, G.; Bothra, A.; Vasudeva, A.; Kedia, S.; Khanna, A.; Khanna, V.; Lohiya, S.; et al. Diagnostic performance of non-invasive, stool-based molecular assays in patients with paucibacillary tuberculosis. Sci. Rep. 2020, 10, 1–8. [Google Scholar] [CrossRef]
- CCarnevale, G.G.; Vargas, F.S.; Caiaffa-Filho, H.H.; Acencio, M.M.P.; Marçal, L.J.; Sales, R.K.B.; Teixeira, L.R.; Antonangelo, L. Preanalytical conditions can interfere with M. tuberculosis detection by PCR in respiratory samples. Clinics 2018, 73, e410. [Google Scholar] [CrossRef]
- Boehme, C.C.; Nabeta, P.; Hillemann, D.; Nicol, M.P.; Shenai, S.; Krapp, F.; Allen, J.; Tahirli, R.; Blakemore, R.; Rustomjee, R.; et al. Rapid Molecular Detection of Tuberculosis and Rifampin Resistance. N. Engl. J. Med. 2010, 363, 1005–1015. [Google Scholar] [CrossRef]
- Aurilio, R.B.; Marsili, V.V.; Malaquias, T.D.S.S.; Kritski, A.L.; Sant’Anna, C.C. The use of Gene-Xpert MTB RIF in the diagnosis of extrapulmonary tuberculosis in childhood and adolescence. Rev. Soc. Bras. Med. Trop. 2020, 53. [Google Scholar] [CrossRef]
- Singh, B.K.; Sharma, R.; Chaubey, J.; Gupta, N.; Soneja, M.; Jorwal, P.; Nischal, N.; Biswas, A.; Wig, N.; Sarin, S.; et al. Evaluation of genotype MTBDRplus V2 and genotype MTBDRsl V2 for the diagnosis of extrapulmonary tuberculosis in India. Tuberculosis 2020, 125, 102014. [Google Scholar] [CrossRef]
- Munshi, S.K.; Rahman, F.; Kamal, S.M.; Noor, R. Comparisons among the diagnostic methods used for the detection of extra-pulmonary tuberculosis in Bangladesh. Int. J. Mycobacteriol. 2012, 1, 190–195. [Google Scholar] [CrossRef]
- Petroff, S. A new and rapid method for the isolation and cultivation of tubercle bacilli directly from the sputum and feces. J. Exp. Med. 1915, 21, 38. [Google Scholar] [CrossRef]
- World Health Organization. Automated Real-Time Nucleic Acid Amplification Technology for Rapid and Simultaneous Detection of Tuberculosis and Rifampicin Resistance: Xpert MTB; Report No.: 9241506334; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Lifescience, H. Genotype MTBDRplus VER 2.0: Molecular Genetic Assay for Identification of the M. tuberculosis Complex and Its Resistance to Rifampicin and Isoniazid from Clinical Specimens and Cultivated Sample; Hain Lifescience GmbH: Nehren, Germany, 2012. [Google Scholar]
- Uddin, M.K.M.; Ather, F.; Akter, S.; Nasrin, R.; Rahman, T.; Kabir, S.N.; Rahman, S.M.M.; Pouzol, S.; Hoffmann, J.; Banu, S. Diagnostic Yield of Xpert MTB/RIF Assay Using Bronchoalveolar Lavage Fluid in Detecting Mycobacterium tuberculosis among the Sputum-Scarce Suspected Pulmonary TB Patients. Diagnostics 2022, 12, 1676. [Google Scholar] [CrossRef]
- Deng, Y.; Duan, Y.-f.; Gao, S.-p.; Wang, J.-m. Comparison of LAMP, GeneXpert, mycobacterial culture, smear microscopy, TSPOT. TB, TBAg/PHA ratio for diagnosis of pulmonary tuberculosis. Curr. Med. Sci. 2021, 41, 1023–1028. [Google Scholar] [CrossRef]
- Norbis, L.; Alagna, R.; Tortoli, E.; Codecasa, L.R.; Migliori, G.B.; Cirillo, D.M. Challenges and perspectives in the diagnosis of extrapulmonary tuberculosis. Expert Rev. Anti-infective Ther. 2014, 12, 633–647. [Google Scholar] [CrossRef]
- Singh, U.B.; Pandey, P.; Mehta, G.; Bhatnagar, A.K.; Mohan, A.; Goyal, V.; Ahuja, V.; Ramachandran, R.; Sachdeva, K.S.; Samantaray, J.C. Genotypic, Phenotypic and Clinical Validation of GeneXpert in Extra-Pulmonary and Pulmonary Tuberculosis in India. PLoS ONE 2016, 11, e0149258. [Google Scholar] [CrossRef] [PubMed]
- Denkinger, C.M.; Schumacher, S.G.; Boehme, C.C.; Dendukuri, N.; Pai, M.; Steingart, K.R. Xpert MTB/RIF assay for the diagnosis of extrapulmonary tuberculosis: A systematic review and meta-analysis. Eur. Respir. J. 2014, 44, 435–446. [Google Scholar] [CrossRef] [PubMed]
- Maynard-Smith, L.; Larke, N.; A Peters, J.; Lawn, S.D. Diagnostic accuracy of the Xpert MTB/RIF assay for extrapulmonary and pulmonary tuberculosis when testing non-respiratory samples: A systematic review. BMC Infect. Dis. 2014, 14, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Vadwai, V.; Boehme, C.; Nabeta, P.; Shetty, A.; Alland, D.; Rodrigues, C. Xpert MTB/RIF: A new pillar in diagnosis of extrapulmonary tuberculosis? J. Clin. Microbiol. 2011, 49, 2540–2545. [Google Scholar] [CrossRef]
- Raghuvanshi, S.; Kotwal, A.; Maheshwari, R.; Sindhwani, G. Evaluation of line-probe assay for molecular analysis and drug susceptibility of extra-pulmonary tuberculosis. Int. J. Tuberc. Lung Dis. 2018, 22, 1077–1081. [Google Scholar] [CrossRef]
- Sharma, S.K.; Chaubey, J.; Singh, B.K.; Sharma, R.; Mittal, A.; Sharma, A. Drug resistance patterns among extra-pulmonary tuberculosis cases in a tertiary care centre in North India. Int. J. Tuberc. Lung Dis. 2017, 21, 1112–1117. [Google Scholar] [CrossRef]
- Tadesse, M.; Abebe, G.; Bekele, A.; Bezabih, M.; Yilma, D.; Apers, L.; de Jong, B.; Rigouts, L. Xpert MTB/RIF assay for the diagnosis of extrapulmonary tuberculosis: A diagnostic evaluation study. Clin. Microbiol. Infect. 2019, 25, 1000–1005. [Google Scholar] [CrossRef]
- Tortoli, E.; Russo, C.; Piersimoni, C.; Mazzola, E.; Monte, P.D.; Pascarella, M.; Borroni, E.; Mondo, A.; Piana, F.; Scarparo, C.; et al. Clinical validation of Xpert MTB/RIF for the diagnosis of extrapulmonary tuberculosis. Eur. Respir. J. 2012, 40, 442–447. [Google Scholar] [CrossRef]
- Bahr, N.C.; Tugume, L.; Rajasingham, R.; Kiggundu, R.; Williams, D.A.; Morawski, B.; Alland, D.; Meya, D.B.; Rhein, J.; Boulware, D.R. Improved diagnostic sensitivity for tuberculous meningitis with Xpert® MTB/RIF of centrifuged CSF. Int. J. Tuberc. Lung Dis. 2015, 19, 1209–1215. [Google Scholar] [CrossRef]
- World Health Organization. WHO Meeting Report of a Technical Expert Consultation: Non-Inferiority Analysis of Xpert MTB/RIF Ultra Compared to Xpert MTB/RIF; HTM/TB; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Chakravorty, S.; Simmons, A.M.; Rowneki, M.; Parmar, H.; Cao, Y.; Ryan, J.; Banada, P.P.; Deshpande, S.; Shenai, S.; Gall, A.; et al. The New Xpert MTB/RIF Ultra: Improving Detection of Mycobacterium tuberculosis and Resistance to Rifampin in an Assay Suitable for Point-of-Care Testing. Mbio 2017, 8, e00812-17. [Google Scholar] [CrossRef]
- Rahman, A.; Sahrin, M.; Afrin, S.; Earley, K.; Ahmed, S.; Rahman, S.M.; Banu, S. Comparison of Xpert MTB/RIF assay and GenoType MTBDR plus DNA probes for detection of mutations associated with rifampicin resistance in Mycobacterium tuberculosis. PLoS ONE 2016, 11, e0152694. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Tests | Results | Culture | Sensitivity (95% CI) | Specificity (95% CI) | PPV (%) | NPV (%) | Accuracy (%) | Kappa Coefficient | p-Value | AUC | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Positive n = 141 (10.52) | Negative n = 1199 (89.48%) | ||||||||||
| AFB Microscopy | Positive n = 49 (3.66%) | 38 | 11 | 27.0 (19.8–35.1) | 99.1 (98.4–99.5) | 77.6 | 92 | 91.4 | 0.3656 | <0.001 | 0.630 |
| Negative n = 1291 (96.34%) | 103 | 1188 | |||||||||
| Xpert MTB/RIF assay | Positive n = 166 (12.39%) | 118 | 48 | 83.7 (76.5–89.4) | 96.0 (94.7–97.0) | 71.1 | 98 | 94.7 | 0.739 | <0.001 | 0.898 |
| Negative n = 1174 (87.61%) | 23 | 1151 | |||||||||
| MTBDRplus assay | Positive n = 154 (11.49%) | 112 | 42 | 79.4 (71.8–85.8) | 96.5 (95.3–97.5) | 72.7 | 97.6 | 94.7 | 0.7296 | <0.001 | 0.880 |
| Negative n = 1186 (88.51%) | 29 | 1157 | |||||||||
| Tests | Results | CRS | Sensitivity (95% CI) | Specificity (95% CI) | PPV (%) | NPV (%) | Accuracy (%) | Kappa Coefficient | p-Value | AUC | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Positive n = 194 | Negative n = 1146 | ||||||||||
| Culture | Positive n = 141 (10.52%) | 141 | 0 | 72.7 (65.8–78.8) | 100 (99.7–100) | 100 | 95.6 | 96 | 0.8198 | <0.001 | 0.863 |
| Negative n = 1199 (89.48%) | 53 | 1146 | |||||||||
| AFB Microscopy | Positive n = 49 (3.66%) | 49 | 0 | 25.3 (19.3–32.0) | 100 (99.7–100) | 100 | 88.8 | 89.2 | 0.3663 | <0.001 | 0.626 |
| Negative n = 1291 (96.34%) | 145 | 1146 | |||||||||
| Xpert MTB/RIF assay | Positive n = 166 (12.39%) | 166 | 0 | 85.6 (79.8–90.2) | 100 (99.7–100) | 100 | 97.6 | 97.9 | 0.9102 | <0.001 | 0.928 |
| Negative n = 1174 (87.61%) | 28 | 1146 | |||||||||
| MTBDRplus assay | Positive n = 154 (11.49%) | 154 | 0 | 79.4 (73.0–84.8) | 100 (99.7–100) | 100 | 96.6 | 97 | 0.8682 | <0.001 | 0.870 |
| Negative n = 1186 (88.51%) | 40 | 1146 | |||||||||
| Tests | Gradings | Positive Cases n (%) | Specimen Types | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Pleural Fluid | Ascitic Fluid | Pus | CSF | Tissue | Urine | FNAC | Synovial Fluid | |||
| AFB Microscopy Positive (n = 49) | Scanty | 21 (42.9) | 1 | 0 | 10 | 0 | 4 | 1 | 4 | 1 |
| 1+ | 18 (36.7) | 0 | 0 | 14 | 0 | 0 | 2 | 2 | 0 | |
| 2+ | 5 (10.2) | 0 | 0 | 3 | 0 | 0 | 0 | 2 | 0 | |
| 3+ | 5 (10.2) | 0 | 0 | 4 | 0 | 1 | 0 | 0 | 0 | |
| Xpert MTB/RIF Positive (n = 166) | Very low | 54 (32.5) | 4 | 10 | 8 | 5 | 15 | 1 | 11 | 0 |
| Low | 76 (45.8) | 7 | 0 | 31 | 4 | 15 | 1 | 18 | 0 | |
| Medium | 28 (16.9) | 1 | 0 | 19 | 0 | 1 | 2 | 4 | 1 | |
| High | 8 (4.8) | 0 | 0 | 5 | 0 | 1 | 0 | 2 | 0 | |
| Tests | Results | Xpert MTB/RIF Assay | Sensitivity (95% CI) | Specificity (95% CI) | PPV (%) | NPV (%) | Accuracy (%) | p-Value | |
|---|---|---|---|---|---|---|---|---|---|
| Positive (n = 166) | Negative (n = 1174) | ||||||||
| MTBDRplus assay | Positive (n = 154) | 145 | 9 | 87.3 (81.3–92.0) | 99.2 (98.5–99.6) | 94.2 | 98.2 | 97.8 | <0.001 |
| Negative (n = 1199) | 21 | 1165 | |||||||
| Sensitive (n = 143) | Resistant (n = 2) | ||||||||
| RIF-Sensitive (n = 143) | 143 | 0 | 100 (97.5–100) | 100 (15.8–100) | 100 | 100 | 100 | - | |
| RIF-Resistant (n = 2) | 0 | 2 | |||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Uddin, M.K.M.; Ather, M.F.; Kabir, S.; Rahman, A.; Choudhury, S.; Nasrin, R.; Rahman, T.; Rahman, S.M.M.; Ahmed, S.; Banu, S. Diagnostic Performance of Different Laboratory Methods for the Detection of Extrapulmonary Tuberculosis. Microorganisms 2023, 11, 1066. https://doi.org/10.3390/microorganisms11041066
Uddin MKM, Ather MF, Kabir S, Rahman A, Choudhury S, Nasrin R, Rahman T, Rahman SMM, Ahmed S, Banu S. Diagnostic Performance of Different Laboratory Methods for the Detection of Extrapulmonary Tuberculosis. Microorganisms. 2023; 11(4):1066. https://doi.org/10.3390/microorganisms11041066
Chicago/Turabian StyleUddin, Mohammad Khaja Mafij, Md. Fahim Ather, Senjuti Kabir, Arfatur Rahman, Sabrina Choudhury, Rumana Nasrin, Tanjina Rahman, S. M. Mazidur Rahman, Shahriar Ahmed, and Sayera Banu. 2023. "Diagnostic Performance of Different Laboratory Methods for the Detection of Extrapulmonary Tuberculosis" Microorganisms 11, no. 4: 1066. https://doi.org/10.3390/microorganisms11041066