
The Impact of Early Life Experiences and Gut Microbiota on Neurobehavioral Development in Preterm Infants: A Longitudinal Cohort Study
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Inclusion and Exclusion Criteria
2.3. Measurements
2.3.1. Demographic and Clinical Data Collection
2.3.2. Assessment of Daily Painful/Stressful Experiences
2.3.3. Fecal Sample and Gut Microbiota
2.3.4. Neurobehavioral Development Assessment
2.4. Data Analysis
3. Results
3.1. Demographic and Clinical Characteristics
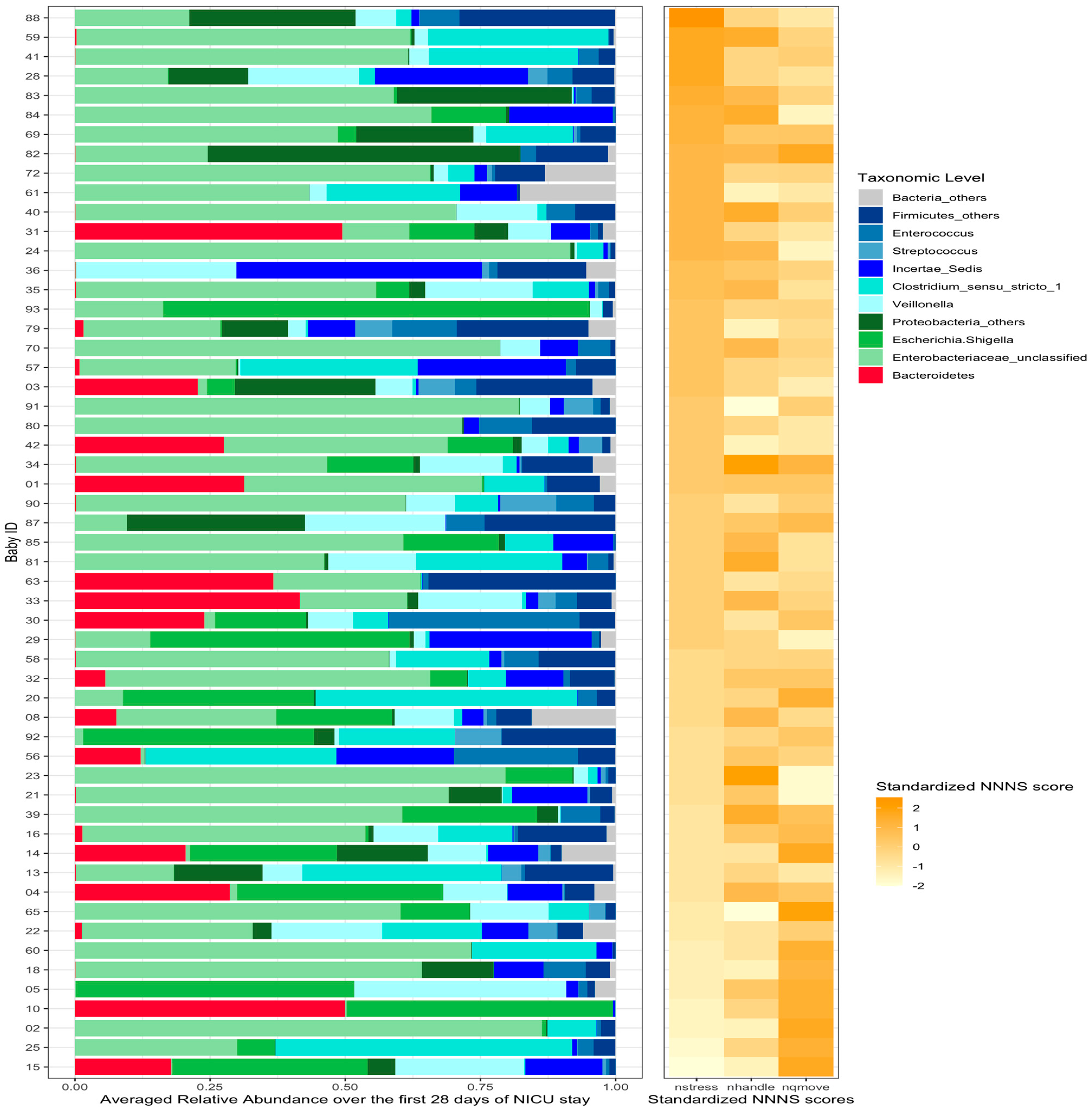
3.2. The Gut Microbiota Compositions
3.3. Neurobehavioral Development
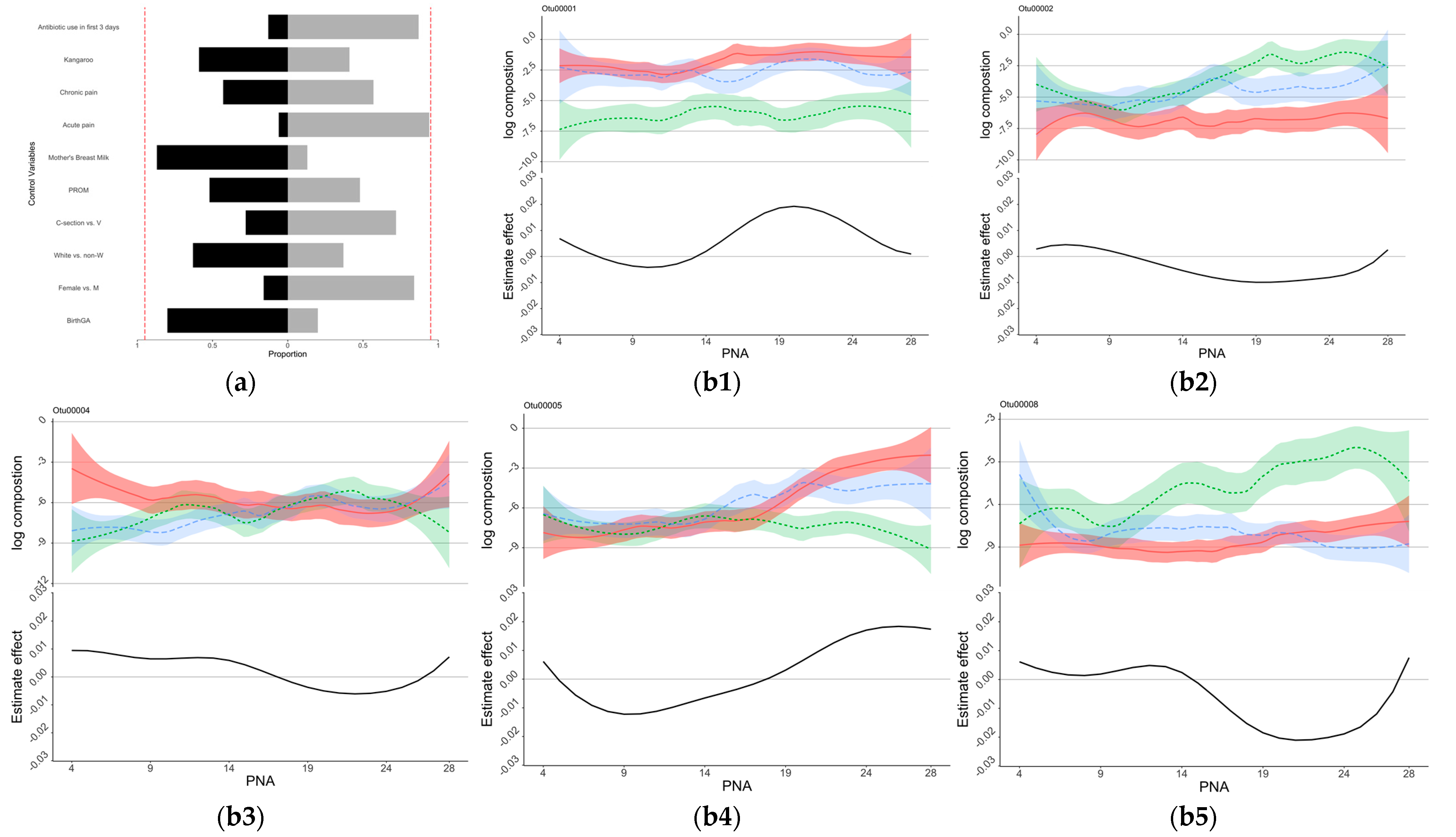
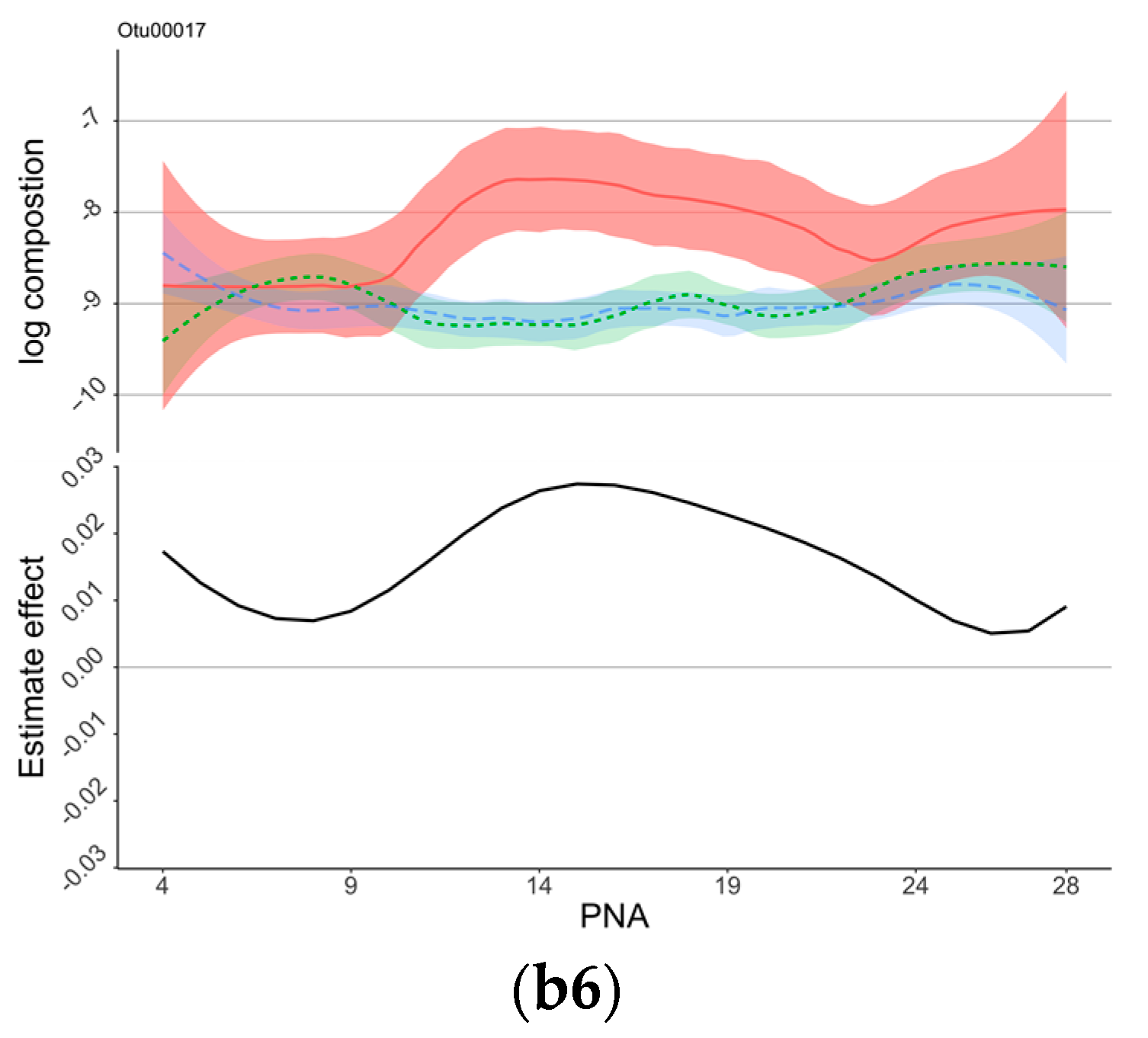
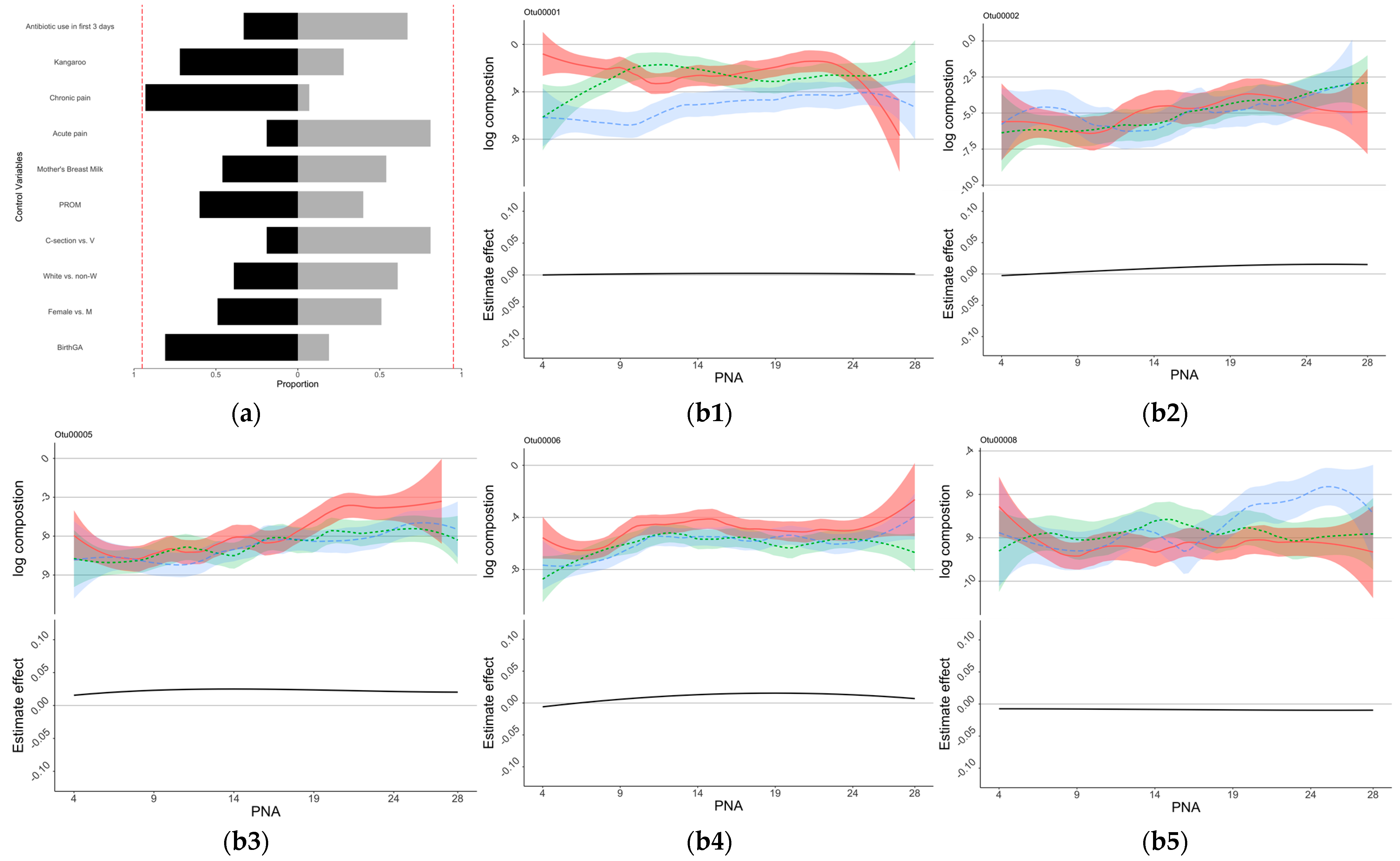
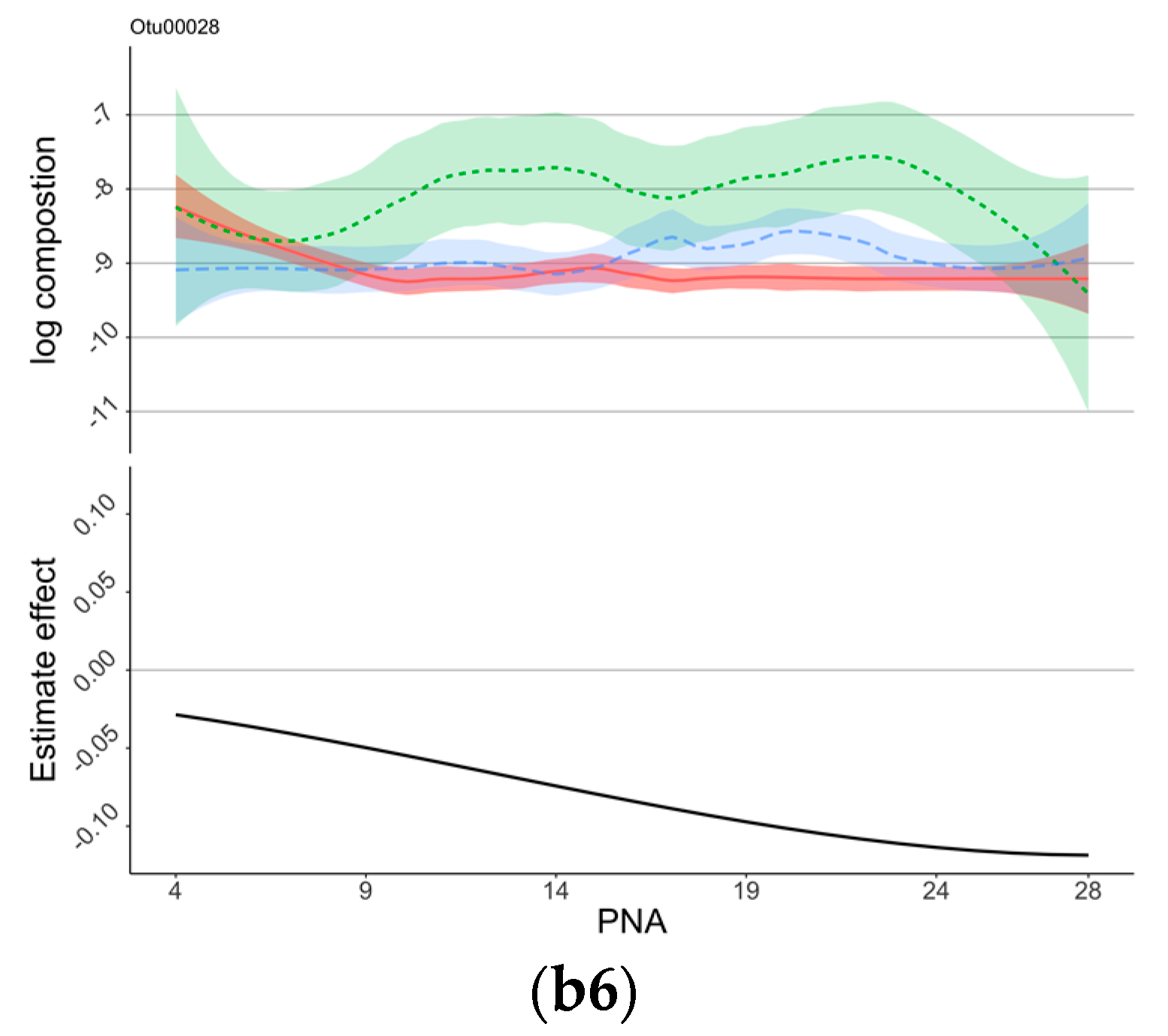
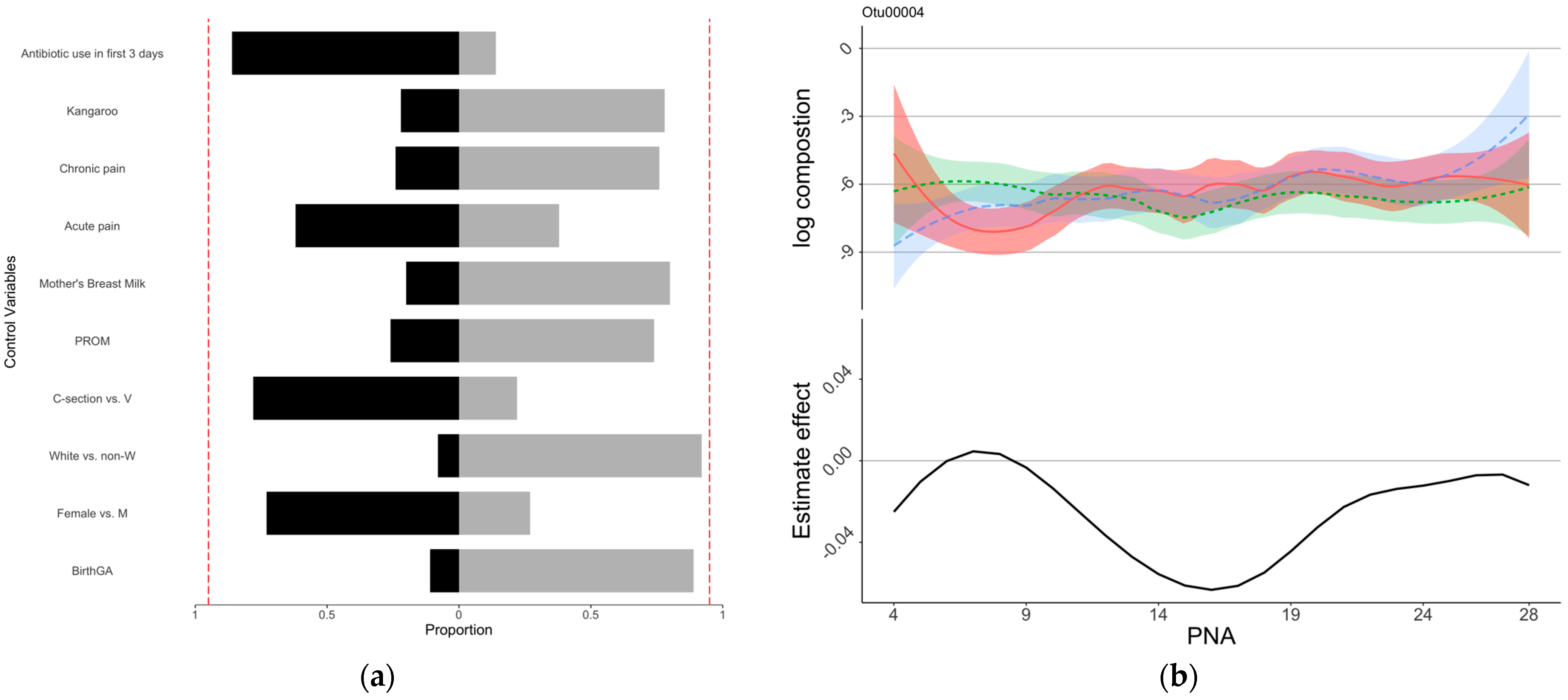
3.4. Associations of Pain/Stress Experience and Gut Microbiota with Neurobehaviors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bell, E.F.; Hintz, S.R.; Hansen, N.I.; Bann, C.M.; Wyckoff, M.H.; DeMauro, S.B.; Walsh, M.C.; Vohr, B.R.; Stoll, B.J.; Carlo, W.A.; et al. Mortality, In-Hospital Morbidity, Care Practices, and 2-Year Outcomes for Extremely Preterm Infants in the US, 2013–2018. JAMA 2022, 327, 248–263. [Google Scholar] [CrossRef]
- Glass, H.C.; Costarino, A.T.; Stayer, S.A.; Brett, C.M.; Cladis, F.; Davis, P.J. Outcomes for extremely premature infants. Anesth. Analg. 2015, 120, 1337–1351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swamy, G.K.; Ostbye, T.; Skjaerven, R. Association of preterm birth with long-term survival, reproduction, and next-generation preterm birth. JAMA 2008, 299, 1429–1436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, T.; Griffith, T.; Zhang, Y.; Li, H.; Hussain, N.; Lester, B.; Cong, X. Early-life factors associated with neurobehavioral outcomes in preterm infants during NICU hospitalization. Pediatr. Res. 2022, 92, 1695–1704. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.M. Short- and Long-Term Outcomes for Extremely Preterm Infants. Am. J. Perinatol. 2016, 33, 318–328. [Google Scholar] [CrossRef] [Green Version]
- Vohr, B. Long-term outcomes of moderately preterm, late preterm, and early term infants. Clin. Perinatol. 2013, 40, 739–751. [Google Scholar] [CrossRef]
- Srinivas Jois, R. Neurodevelopmental outcome of late-preterm infants: A pragmatic review. Aust. J. Gen. Pract. 2018, 47, 776–781. [Google Scholar] [CrossRef] [PubMed]
- Aatsinki, A.-K.; Lahti, L.; Uusitupa, H.-M.; Munukka, E.; Keskitalo, A.; Nolvi, S.; O’Mahony, S.; Pietilä, S.; Elo, L.L.; Eerola, E.; et al. Gut microbiota composition is associated with temperament traits in infants. Brain Behav. Immun. 2019, 80, 849–858. [Google Scholar] [CrossRef] [PubMed]
- Seki, D.; Mayer, M.; Hausmann, B.; Pjevac, P.; Giordano, V.; Goeral, K.; Unterasinger, L.; Klebermaß-Schrehof, K.; De Paepe, K.; Van de Wiele, T.; et al. Aberrant gut-microbiota-immune-brain axis development in premature neonates with brain damage. Cell Host Microbe 2021, 29, 1558–1572.e6. [Google Scholar] [CrossRef]
- Oliphant, K.; Ali, M.; D’Souza, M.; Hughes, P.D.; Sulakhe, D.; Wang, A.Z.; Xie, B.; Yeasin, R.; Msall, M.E.; Andrews, B.; et al. Bacteroidota and Lachnospiraceae integration into the gut microbiome at key time points in early life are linked to infant neurodevelopment. Gut Microbes 2021, 13, 1997560. [Google Scholar] [CrossRef]
- Olson, C.A.; Iñiguez, A.J.; Yang, G.E.; Fang, P.; Pronovost, G.N.; Jameson, K.G.; Rendon, T.K.; Paramo, J.; Barlow, J.T.; Ismagilov, R.F.; et al. Alterations in the gut microbiota contribute to cognitive impairment induced by the ketogenic diet and hypoxia. Cell Host Microbe 2021, 29, 1378–1392.e6. [Google Scholar] [CrossRef]
- Stewart, C.J.; Marrs, E.C.L.; Nelson, A.; Lanyon, C.; Perry, J.D.; Embleton, N.D.; Cummings, S.P.; Berrington, J. Development of the preterm gut microbiome in twins at risk of necrotising enterocolitis and sepsis. PLoS ONE 2013, 8, e73465. [Google Scholar] [CrossRef]
- Beghetti, I.; Barone, M.; Turroni, S.; Biagi, E.; Sansavini, A.; Brigidi, P.; Corvaglia, L.; Aceti, A. Early-life gut microbiota neurodevelopment in preterm infants: Any role for Bifidobacterium? Eur. J. Pediatr. 2022, 181, 1773–1777. [Google Scholar] [CrossRef] [PubMed]
- Rozé, J.C.; Ancel, P.Y.; Marchand-Martin, L.; Rousseau, C.; Montassier, E.; Monot, C.; Le Roux, K.; Butin, M.; Resche-Rigon, M.; Aires, J.; et al. Assessment of Neonatal Intensive Care Unit Practices and Preterm Newborn Gut Microbiota and 2-Year Neurodevelopmental Outcomes. JAMA Netw. Open 2020, 3, e2018119. [Google Scholar] [CrossRef] [PubMed]
- Sordillo, J.E.; Korrick, S.; Laranjo, N.; Carey, V.; Weinstock, G.M.; Gold, D.R.; O’Connor, G.; Sandel, M.; Bacharier, L.B.; Beigelman, A.; et al. Association of the Infant Gut Microbiome with Early Childhood Neurodevelopmental Outcomes: An Ancillary Study to the VDAART Randomized Clinical Trial. JAMA Netw. Open 2019, 2, e190905. [Google Scholar] [CrossRef] [Green Version]
- Richardson, D.K.; Corcoran, J.D.; Escobar, G.J.; Lee, S.K. SNAP-II and SNAPPE-II: Simplified newborn illness severity mortality risk scores. J. Pediatr. 2001, 138, 92–100. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Cong, X.; Xu, W.; Janton, S.; Henderson, W.A.; Matson, A.; McGrath, J.M.; Maas, K.; Graf, J. Gut Microbiome Developmental Patterns in Early Life of Preterm Infants: Impacts of Feeding and Gender. PLoS ONE 2016, 11, e0152751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.; Li, H.; Hird, S.M.; Chen, M.-H.; Xu, W.; Maas, K.; Cong, X. Sex Differences in Gut Microbial Development of Preterm Infant Twins in Early Life: A Longitudinal Analysis. Front. Cell. Infect. Microbiol. 2021, 11, 671074. [Google Scholar] [CrossRef] [PubMed]
- Schloss, P.D.; Westcott, S.L.; Ryabin, T.; Hall, J.R.; Hartmann, M.; Hollister, E.B.; Lesniewski, R.A.; Oakley, B.B.; Parks, D.H.; Robinson, C.J.; et al. Introducing mothur: Open-source, platform-independent, community-supported software for describing and comparing microbial communities. Appl. Environ. Microbiol. 2009, 75, 7537–7541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edgar, R.C. Updating the 97% identity threshold for 16S ribosomal RNA OTUs. Bioinformatics 2018, 34, 2371–2375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yilmaz, P.; Parfrey, L.W.; Yarza, P.; Gerken, J.; Pruesse, E.; Quast, C.; Schweer, T.; Peplies, J.; Ludwig, W.; Glöckner, F.O. The SILVA and “All-species Living Tree Project (LTP)” taxonomic frameworks. Nucleic Acids Res. 2014, 42, D643–D648. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quast, C.; Pruesse, E.; Yilmaz, P.; Gerken, J.; Schweer, T.; Yarza, P.; Peplies, J.; Glöckner, F.O. The SILVA ribosomal RNA gene database project: Improved data processing and web-based tools. Nucleic Acids Res. 2013, 41, D590–D596. [Google Scholar] [CrossRef] [PubMed]
- Lester, B.M.; Tronick, E.Z.; Brazelton, T.B. The Neonatal Intensive Care Unit Network Neurobehavioral Scale procedures. Pediatrics 2004, 113, 641–667. [Google Scholar] [CrossRef]
- Wickham, H. Package ‘ggplot2’: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016; Volume 10, pp. 970–978. [Google Scholar]
- Sun, Z.; Xu, W.; Cong, X.; Li, G.; Chen, K. Log-Contrast Regression with Functional Compositional Predictors: Linking Preterm Infant’s Gut Microbiome Trajectories to Neurobehavioral Outcome. Ann. Appl. Stat. 2020, 14, 1535–1556. [Google Scholar] [CrossRef]
- Yuan, M.; Lin, Y. Model selection and estimation in regression with grouped variables. J. R. Stat. Soc. Ser. B (Stat. Methodol.) 2006, 68, 49–67. [Google Scholar] [CrossRef]
- Provenzi, L.; Olson, K.; Giusti, L.; Montirosso, R.; DeSantis, A.; Tronick, E. NICU Network Neurobehavioral Scale: 1-month normative data and variation from birth to 1 month. Pediatr. Res. 2018, 83, 1104–1109. [Google Scholar] [CrossRef]
- McGowan, E.C.; Hofheimer, J.A.; O’Shea, T.M.; Kilbride, H.; Carter, B.S.; Check, J.; Helderman, J.; Neal, C.R.; Pastyrnak, S.; Smith, L.M.; et al. Analysis of Neonatal Neurobehavior and Developmental Outcomes Among Preterm Infants. JAMA Netw. Open 2022, 5, e2222249. [Google Scholar] [CrossRef]
- Kiblawi, Z.N.; Smith, L.M.; Diaz, S.D.; LaGasse, L.L.; Derauf, C.; Newman, E.; Shah, R.; Arria, A.; Huestis, M.; Haning, W.; et al. Prenatal methamphetamine exposure and neonatal and infant neurobehavioral outcome: Results from the IDEAL study. Subst. Abus. 2014, 35, 68–73. [Google Scholar] [CrossRef] [Green Version]
- Lavanga, M.; Bollen, B.; Caicedo, A.; Dereymaeker, A.; Jansen, K.; Ortibus, E.; Van Huffel, S.; Naulaers, G. The effect of early procedural pain in preterm infants on the maturation of electroencephalogram and heart rate variability. Pain 2021, 162, 1556–1566. [Google Scholar] [CrossRef]
- Russell, J.T.; Lauren Ruoss, J.; de la Cruz, D.; Li, N.; Bazacliu, C.; Patton, L.; McKinley, K.L.; Garrett, T.J.; Polin, R.A.; Triplett, E.W.; et al. Antibiotics and the developing intestinal microbiome, metabolome and inflammatory environment in a randomized trial of preterm infants. Sci. Rep. 2021, 11, 1943. [Google Scholar] [CrossRef] [PubMed]
- Currie, A.J.; Curtis, S.; Strunk, T.; Riley, K.; Liyanage, K.; Prescott, S.; Doherty, D.; Simmer, K.; Richmond, P.; Burgner, D. Preterm Infants Have Deficient Monocyte and Lymphocyte Cytokine Responses to Group B Streptococcus. Infect. Immun. 2011, 79, 1588–1596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lyte, M. Microbial endocrinology and the microbiota-gut-brain axis. Adv. Exp. Med. Biol. 2014, 817, 3–24. [Google Scholar] [CrossRef] [PubMed]
- Cong, X.; Henderson, W.A.; Graf, J.; McGrath, J.M. Early Life Experience and Gut Microbiome. Adv. Neonatal Care 2015, 15, 314–323. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.-G.; Sakamoto, K.; Seo, S.-U.; Pickard, J.M.; Gillilland, M.G.; Pudlo, N.A.; Hoostal, M.; Li, X.; Wang, T.D.; Feehley, T.; et al. Neonatal acquisition of Clostridia species protects against colonization by bacterial pathogens. Science 2017, 356, 315–319. [Google Scholar] [CrossRef] [Green Version]
- Streit, F.; Prandovszky, E.; Send, T.; Zillich, L.; Frank, J.; Sabunciyan, S.; Foo, J.; Sirignano, L.; Lange, B.; Bardtke, S.; et al. Microbiome profiles are associated with cognitive functioning in 45-month-old children. Brain Behav. Immun. 2021, 98, 151–160. [Google Scholar] [CrossRef]
- Wasser, C.I.; Mercieca, E.-C.; Kong, G.; Hannan, A.J.; McKeown, S.J.; Glikmann-Johnston, Y.; Stout, J.C. Gut dysbiosis in Huntington’s disease: Associations among gut microbiota, cognitive performance and clinical outcomes. Brain Commun. 2020, 2, fcaa110. [Google Scholar] [CrossRef]
- Wang, L.; de Ángel Solá, D.; Acevedo Flores, M.; Schriefer, A.; Wang, L.; Gerónimo López, K.; Chang, A.; Warner, B.; Shan, L.; Holtz, L.R.; et al. Prenatal food insecurity post Hurricane Maria is associated with decreased Veillonella in the infant gut. Pediatr. Res. 2020, 88, 917–924. [Google Scholar] [CrossRef]
- Guo, H.; Chou, W.-C.; Lai, Y.; Liang, K.; Tam, J.W.; Brickey, W.J.; Chen, L.; Montgomery, N.D.; Li, X.; Bohannon, L.M.; et al. Multi-omics analyses of radiation survivors identify radioprotective microbes and metabolites. Science 2020, 370, eaay9097. [Google Scholar] [CrossRef]
- Hu, Y.; Yang, Q.; Liu, B.; Dong, J.; Sun, L.; Zhu, Y.; Su, H.; Yang, J.; Yang, F.; Chen, X.; et al. Gut microbiota associated with pulmonary tuberculosis dysbiosis caused by anti-tuberculosis drugs. J. Infect. 2019, 78, 317–322. [Google Scholar] [CrossRef]
- Rabe, H.; Lundell, A.C.; Sjöberg, F.; Ljung, A.; Strömbeck, A.; Gio-Batta, M.; Maglio, C.; Nordström, I.; Andersson, K.; Nookaew, I.; et al. Neonatal gut colonization by Bifidobacterium is associated with higher childhood cytokine responses. Gut Microbes 2020, 12, 1847628. [Google Scholar] [CrossRef] [PubMed]
- Schönherr-Hellec, S.; Klein, G.L.; Delannoy, J.; Ferraris, L.; Rozé, J.C.; Butel, M.J.; Aires, J. Clostridial Strain-Specific Characteristics Associated with Necrotizing Enterocolitis. Appl. Environ. Microbiol. 2018, 84, e02428-17. [Google Scholar] [CrossRef] [Green Version]
- Park, Y.M.; Lee, S.-Y.; Kang, M.-J.; Kim, B.-S.; Lee, M.-J.; Jung, S.S.; Yoon, J.S.; Cho, H.-J.; Lee, E.; Yang, S.-I.; et al. Imbalance of Gut Streptococcus, Clostridium, and Akkermansia Determines the Natural Course of Atopic Dermatitis in Infant. Allergy Asthma Immunol. Res. 2020, 12, 322. [Google Scholar] [CrossRef] [PubMed]
- Geetha, O.; Cherie, C.; Natalie, T.W.H.; Merchant, K.; Chien, C.M.; Chandran, S. Streptococcus gallolyticus subspecies pasteurianus causing early onset neonatal sepsis complicated by solitary liver abscess in a preterm infant. Access Microbiol. 2021, 3, 000200. [Google Scholar] [CrossRef]
- Nieto-Moro, M.; Ecclesia, F.G.; Tomé-Masa, I.; De Lama Caro-Patón, G.; Leoz-Gordillo, I.; Cabrero-Hernández, M.; García-Salido, A. SARS-CoV-2 and Streptococcus pneumoniae coinfection as a cause of severe pneumonia in an infant. Pediatr. Pulmonol. 2020, 55, 2198–2200. [Google Scholar] [CrossRef] [PubMed]
- Turner, P.; Melchiorre, S.; Moschioni, M.; Barocchi, M.A.; Turner, C.; Watthanaworawit, W.; Kaewcharernnet, N.; Nosten, F.; Goldblatt, D. Assessment of Streptococcus pneumoniae pilus islet-1 prevalence in carried and transmitted isolates from mother–infant pairs on the Thailand–Burma border. Clin. Microbiol. Infect. 2012, 18, 970–975. [Google Scholar] [CrossRef] [Green Version]
- Pannaraj, P.S.; Li, F.; Cerini, C.; Bender, J.M.; Yang, S.; Rollie, A.; Adisetiyo, H.; Zabih, S.; Lincez, P.J.; Bittinger, K.; et al. Association Between Breast Milk Bacterial Communities and Establishment and Development of the Infant Gut Microbiome. JAMA Pediatr. 2017, 171, 647. [Google Scholar] [CrossRef] [Green Version]
- Aguilar-Lopez, M.; Wetzel, C.; MacDonald, A.; Ho, T.T.B.; Donovan, S.M. Human Milk-Based or Bovine Milk-Based Fortifiers Differentially Impact the Development of the Gut Microbiota of Preterm Infants. Front. Pediatr. 2021, 9, 719096. [Google Scholar] [CrossRef]
- Béghin, L.; Tims, S.; Roelofs, M.; Rougé, C.; Oozeer, R.; Rakza, T.; Chirico, G.; Roeselers, G.; Knol, J.; Rozé, J.C.; et al. Fermented infant formula (with Bifidobacterium breve C50 and Streptococcus thermophilus O65) with prebiotic oligosaccharides is safe and modulates the gut microbiota towards a microbiota closer to that of breastfed infants. Clin. Nutr. 2021, 40, 778–787. [Google Scholar] [CrossRef]
- Jiang, H.; Xu, L.; Zhang, X.; Zhang, Z.; Ruan, B. The microbiome in bipolar depression: A longitudinal study of one pair of monozygotic twins. Bipolar Disord. 2019, 21, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Laue, H.E.; Karagas, M.R.; Coker, M.O.; Bellinger, D.C.; Baker, E.R.; Korrick, S.A.; Madan, J.C. Sex-specific relationships of the infant microbiome and early-childhood behavioral outcomes. Pediatr. Res. 2022, 92, 580–591. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Li, H.; Maas, K.; Starkweather, A.; Chen, M.; Cong, X. Sex-specific gut microbiome profiles among preterm infants during the neonatal intensive care hospitalization. Interdiscip. Nurs. Res. 2022, 1, 6–13. [Google Scholar] [CrossRef]
- Stearns, J.C.; Alliance, N.; Zulyniak, M.A.; de Souza, R.J.; Campbell, N.C.; Fontes, M.; Shaikh, M.; Sears, M.R.; Becker, A.B.; Mandhane, P.J.; et al. Ethnic and diet-related differences in the healthy infant microbiome. Genome Med. 2017, 9, 32. [Google Scholar] [CrossRef] [Green Version]
- Cheng, Y.; Selma-Royo, M.; Cao, X.; Calatayud, M.; Qi, Q.; Zhou, J.; Zeng, L.; Garcia-Mantrana, I.; Collado, M.C.; Han, B. Influence of Geographical Location on Maternal-Infant Microbiota: Study in Two Populations From Asia and Europe. Front. Cell. Infect. Microbiol. 2022, 11, 663513. [Google Scholar] [CrossRef] [PubMed]
- Vogel, S.C.; Brito, N.H.; Callaghan, B.L. Early Life Stress and the Development of the Infant Gut Microbiota: Implications for Mental Health and Neurocognitive Development. Curr. Psychiatry Rep. 2020, 22, 61. [Google Scholar] [CrossRef] [PubMed]
- Cryan, J.F.; Dinan, T.G. Mind-altering microorganisms: The impact of the gut microbiota on brain and behaviour. Nat. Rev. Neurosci. 2012, 13, 701–712. [Google Scholar] [CrossRef] [PubMed]
- Sarkar, A.; Harty, S.; Lehto, S.M.; Moeller, A.H.; Dinan, T.G.; Dunbar, R.I.M.; Cryan, J.F.; Burnet, P.W. The Microbiome in Psychology and Cognitive Neuroscience. Trends Cogn. Sci. 2018, 22, 611–636. [Google Scholar] [CrossRef]
- Samara, J.; Moossavi, S.; Alshaikh, B.; Ortega, V.A.; Pettersen, V.K.; Ferdous, T.; Hoops, S.L.; Soraisham, A.; Vayalumkal, J.; Dersch-Mills, D.; et al. Supplementation with a probiotic mixture accelerates gut microbiome maturation and reduces intestinal inflammation in extremely preterm infants. Cell Host Microbe 2022, 30, 696–711.e5. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 55) | Female (n = 30) | Male (n = 25) | |
|---|---|---|---|
| Birth gestational age (weeks) | 30.72 (1.71) | 30.53 (1.72) | 30.96 (1.71) |
| Birth body length (cm) | 39.94 (3.25) | 39.56 (3.34) | 40.38 (3.17) |
| Birth body weight (g) | 1444.53 (406.61) | 1362.87 (413.29) | 1542.52 (383.76) |
| Birth head circumference (cm) | 27.86 (1.88) | 27.50 (2.05) | 28.31 (1.59) |
| SNAPE II [media, IQR] a | 9.31 (9.66) | 11.07 (10.57) | 7.2 (8.15) |
| C-section (n, %) | 34 (61.82%) | 21 (70.00%) | 13 (52.00%) |
| Premature rupture of membranes (n, %) | 22 (40%) | 11 (36.67%) | 11 (44%) |
| Race (n, %) | |||
| White | 41 (74.54%) | 23 (76.67%) | 18 (72.00%) |
| American African | 11 (20.00%) | 4 (13.33%) | 7 (28.00%) |
| Asian | 2 (3.64%) | 2 (6.67%) | 0 (0.00%) |
| Unknown | 1 (1.82%) | 1 (3.33%) | 0 (0.00%) |
| Averaged MBM percentage b | 61.46% (32.07) | 63.09% (33.02) | 59.51% (31.46) |
| Averaged acute pain c | 62.66 (9.94) | 62.01 (9.65) | 63.43 (10.42) |
| Averaged chronic pain c | 89.84 (36.72) | 93.44 (37.76) | 85.82 (35.68) |
| NNNS a | Total (n = 55) | Female (n = 30) | Male (n = 25) |
|---|---|---|---|
| Stress/abstinence (NSTRESS) | 0.18 (0.09) | 0.19 (0.09) | 0.17 (0.09) |
| Handling (NHANDLING) | 0.56 (0.21) | 0.57 (0.21) | 0.56 (0.22) |
| Quality of movement (NQMOVE) | 3.97 (0.62) | 3.90 (0.65) | 4.05 (0.60) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, J.; Li, H.; Zhao, T.; Chen, K.; Chen, M.-H.; Sun, Z.; Xu, W.; Maas, K.; Lester, B.M.; Cong, X.S. The Impact of Early Life Experiences and Gut Microbiota on Neurobehavioral Development in Preterm Infants: A Longitudinal Cohort Study. Microorganisms 2023, 11, 814. https://doi.org/10.3390/microorganisms11030814
Chen J, Li H, Zhao T, Chen K, Chen M-H, Sun Z, Xu W, Maas K, Lester BM, Cong XS. The Impact of Early Life Experiences and Gut Microbiota on Neurobehavioral Development in Preterm Infants: A Longitudinal Cohort Study. Microorganisms. 2023; 11(3):814. https://doi.org/10.3390/microorganisms11030814
Chicago/Turabian StyleChen, Jie, Hongfei Li, Tingting Zhao, Kun Chen, Ming-Hui Chen, Zhe Sun, Wanli Xu, Kendra Maas, Barry M. Lester, and Xiaomei S. Cong. 2023. "The Impact of Early Life Experiences and Gut Microbiota on Neurobehavioral Development in Preterm Infants: A Longitudinal Cohort Study" Microorganisms 11, no. 3: 814. https://doi.org/10.3390/microorganisms11030814