
Bone Health in People Living with HIV/AIDS: An Update of Where We Are and Potential Future Strategies
Abstract
:1. Background
2. Methods
2.1. Inclusion Criteria
2.2. Exclusion Criteria
3. Prevalence of Fracture in Association with HIV
4. What Is the Impact of HIV on Bone Mineral Density?
4.1. The BMD before Encountering HIV Infection
4.2. Loss of BMD Is Likely to Occur at the Age of 50 Years
4.3. Direct Impact of HIV on BMD
4.4. Onset of ART Therapy and Bone Density
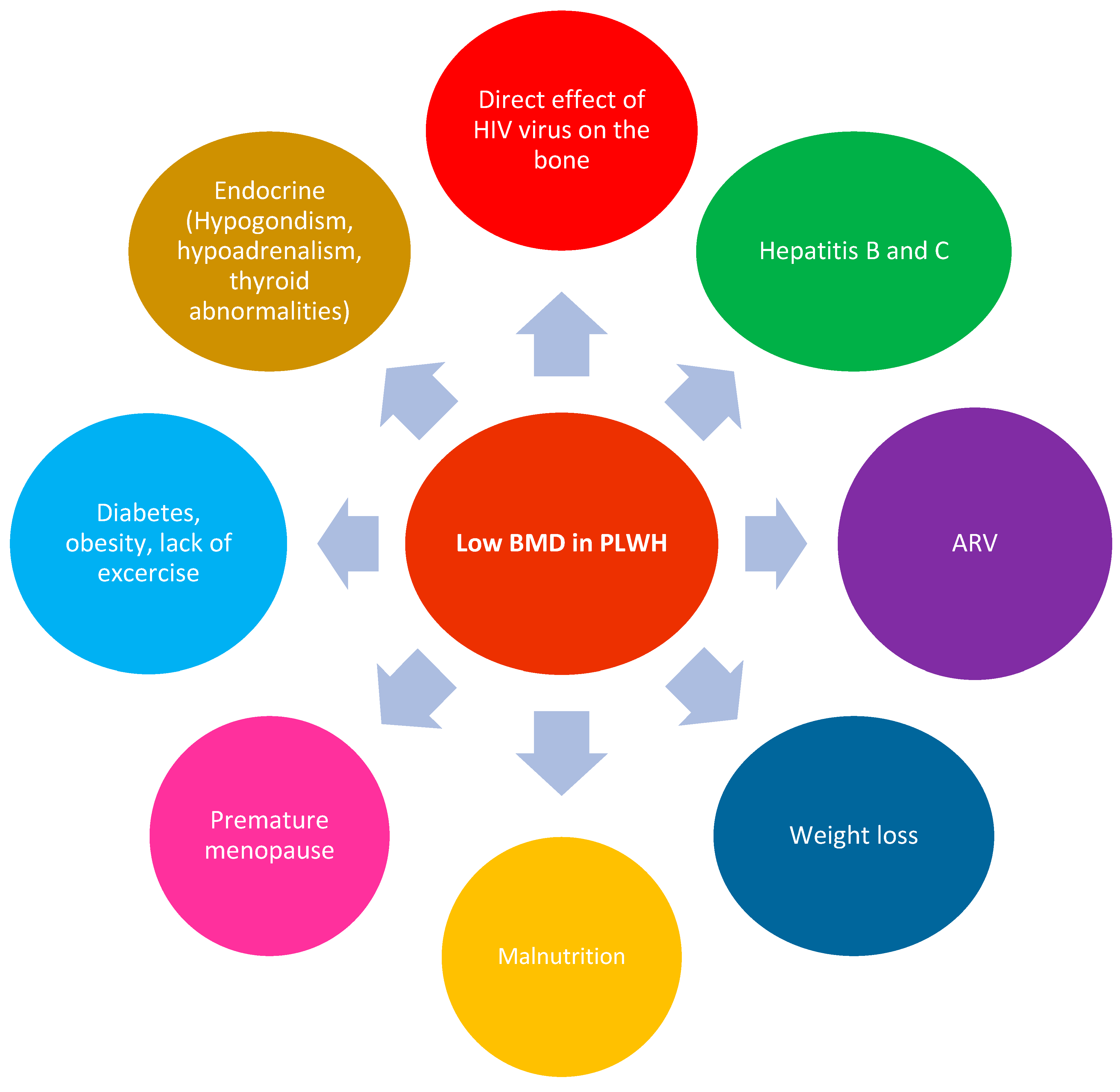
5. What Are the Physiological Changes That Lead to Increased Risk of Fracture in PLWHIV?
6. Impact of HIV on the Bones
7. Impact of Antiretroviral Treatments on the Bones
8. Impact of Hepatitis C on Bones
9. HIV and Endocrine/Metabolic Changes Relating to Impact on Bones
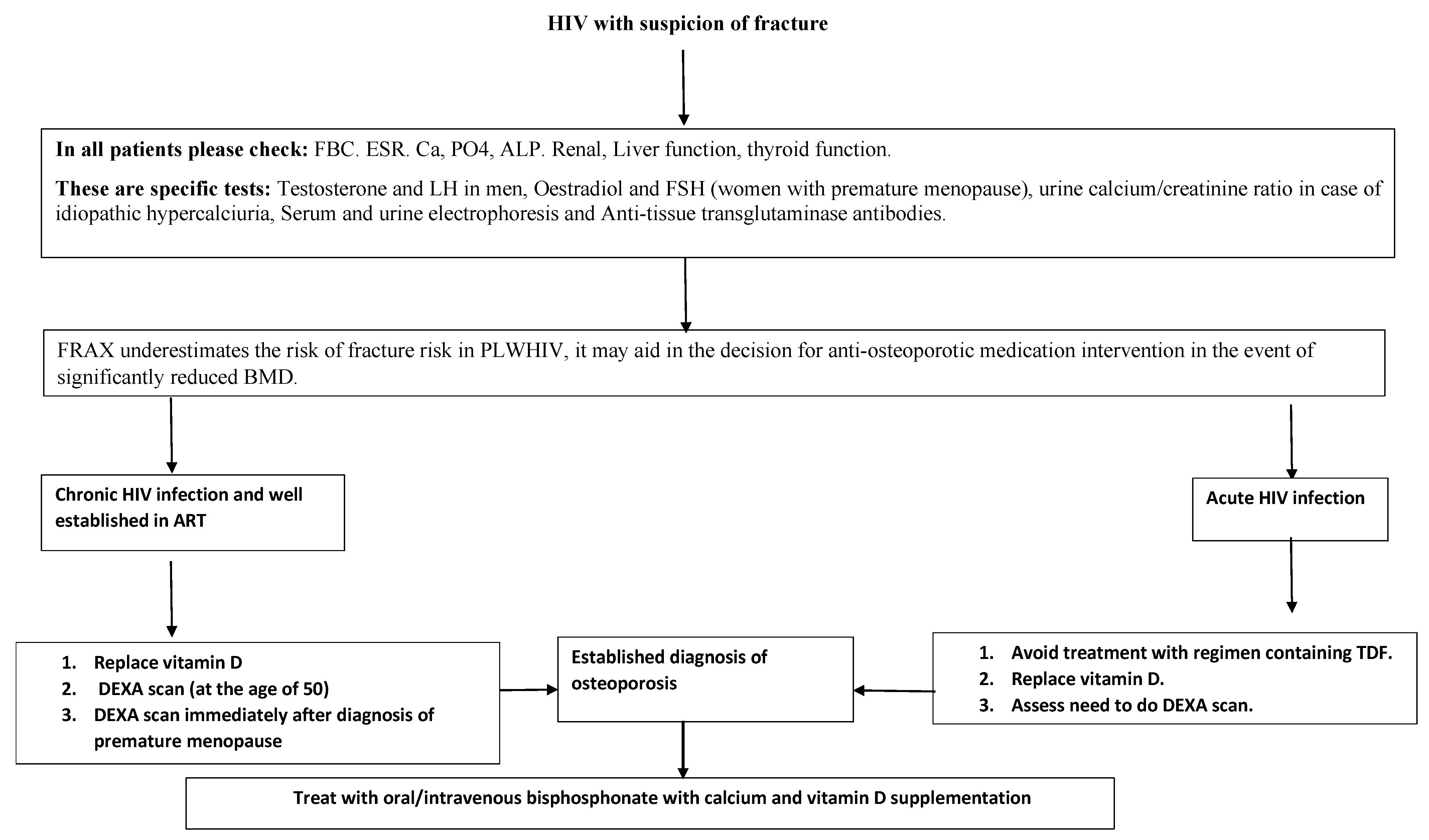
10. Prevention and Management of Osteoporosis in PLWHIV
General Recommendations
- Encouragement of physical exercise and a balanced diet, with the discontinuation of harmful behaviors where relevant (smoking, excess alcohol intake and obesity);
- Prevention of falls in the elderly population;
- Checking vitamin D levels at least once a year and taking supplements of calcium and vitamin D when needed;
- Education about bone health;
- Health education for women about the risk of premature menopause and impact on the bones;
- The need for regular bone screening through measurement of vitamin D and DEXA scans;
- A DEXA scan is indicated for all postmenopausal women, males older than 50 years, and patients with significant clinical risk factors for fragility fractures, because these patients are more likely to benefit from anti-osteoporotic medications in the case of low BMD [69];
- The FRAX® tool has been recommended for regular assessment of fracture risk in PLWHIV over the age of 40 in the guidelines [70];
- The addition of bisphosphonates to the cessation of TDF leads to greater increases in BMD than cessation of TDF alone [75];
- In the event of osteoporosis or a high risk of fracture, it may be important to consider anti-osteoporotic medication even if a bone-friendly ARV regimen has been adopted;
- PLWHIV receiving TAF or an integrase inhibitor-based regimen saw significantly greater increases in body weight than those receiving TDF [76]. The substitution of TDF with TAF is similarly related with an increase in body weight, obesity and an increase in blood lipid levels [77]. The degree to which changes in fat mass contribute to increased BMD or reduced bone loss reported with TAF or integrase inhibitors is still not yet elucidated.
11. Calcium and Vitamin D
12. Anti-Osteoporotic Drugs
12.1. Bisphosphonates
12.2. Denosumab, Teriparatide, Abaloparatide and Romosozumab
13. Limitations and Strength of the Study
14. Conclusions
Funding
Data Availability Statement
Conflicts of Interest
References
- Scherrer, A.U.; Traytel, A.; Braun, D.L.; Calmy, A.; Battegay, M.; Cavassini, M.; Furrer, H.; Schmid, P.; Bernasconi, E.; Stoeckle, M.; et al. Cohort Profile Update: The Swiss HIV Cohort Study (SHCS). Int. J. Epidemiol. 2022, 51, 33–34j. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, E.; Belloso, W.H.; Boyd, M.A.; Inkaya, A.C.; Hsieh, E.; Kambugu, A.; Kaminski, G.; Martinez, E.; Stellbrink, H.J.; Walmsley, S.; et al. Which HIV patients should be screened for osteoporosis: An international perspective. Curr. Opin. HIV AIDS 2016, 11, 268–276. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Noh, J.; Kim, W.; Seong, H.; Kim, J.H.; Lee, W.J.; Baek, Y.; Hyun, J.; Sohn, Y.; Cho, Y.; et al. Trends of age-related non-communicable diseases in people living with HIV and comparison with uninfected controls: A nationwide population-based study in South Korea. HIV Med. 2021, 22, 824–833. [Google Scholar] [CrossRef] [PubMed]
- Marcus, J.L.; Leyden, W.A.; Alexeeff, S.E.; Anderson, A.N.; Hechter, R.C.; Hu, H.; Lam, J.O.; Towner, W.J.; Yuan, Q.; Horberg, M.A.; et al. Comparison of Overall and Comorbidity-Free Life Expectancy between Insured Adults with and without HIV Infection, 2000–2016. JAMA Netw. Open 2020, 3, e207954. [Google Scholar] [CrossRef]
- Ahmed, M.H.; Bondje, S.; Jiwan, R.; Rawther, F.; Duku, A.; Husain, N.E.; Woodward, C.; Mital, D. Early menopause in acquired immunodeficiency syndrome. J. Res. Med. Sci. 2021, 26, 122. [Google Scholar] [CrossRef]
- Sharma, A.; Hoover, D.R.; Shi, Q.; Tien, P.C.; Weber, K.M.; Shah, J.G.; Yin, M.T. Human Immunodeficiency Virus (HIV) and Menopause Are Independently Associated with Lower Bone Mineral Density: Results From the Women’s Interagency HIV Study. Clin. Infect. Dis. 2022, 75, 65–72. [Google Scholar] [CrossRef]
- Youssef, J.; Sadera, R.; Mital, D.; Ahmed, M.H. HIV and the Pituitary Gland: Clinical and Biochemical Presentations. J. Lab. Physicians 2021, 13, 84–90. [Google Scholar] [CrossRef]
- Cahn, A.; Chairsky-Segal, I.; Olshtain-Pops, K.; Maayan, S.; Wolf, D.; Dresner-Pollak, R. Changes in thyroid function in Ethiopian and non-Ethiopian Israeli patients with human immunodeficiency virus infection or acquired immunodeficiency syndrome. Endocr. Pract. 2012, 18, 882–886. [Google Scholar] [CrossRef]
- Napoli, N.; Incalzi, R.A.; De Gennaro, G.; Marcocci, C.; Marfella, R.; Papalia, R.; Purrello, F.; Ruggiero, C.; Tarantino, U.; Tramontana, F.; et al. Bone fragility in patients with diabetes mellitus: A consensus statement from the working group of the Italian Diabetes Society (SID), Italian Society of Endocrinology (SIE), Italian Society of Gerontology and Geriatrics (SIGG), Italian Society of Orthopaedics and Traumatology (SIOT). Nutr. Metab. Cardiovasc. Dis. 2021, 31, 1375–1390. [Google Scholar]
- Husain, N.E.; Noor, S.K.; Elmadhoun, W.M.; Almobarak, A.O.; Awadalla, H.; Woodward, C.L.; Mital, D.; Ahmed, M.H. Diabetes, metabolic syndrome and dyslipidemia in people living with HIV in Africa: Re-emerging challenges not to be forgotten. HIV AIDS 2017, 9, 193–202. [Google Scholar] [CrossRef] [Green Version]
- Maffezzoni, F.; Porcelli, T.; Delbarba, A.; Pezzaioli, L.C.; Properzi, M.; Cappelli, C.; Castelli, F.; Quiros-Roldan, M.E.; Ferlin, A. Hypogonadism and bone health in men with HIV. Lancet HIV 2020, 7, e782–e790. [Google Scholar] [CrossRef]
- Foreman, S.C.; Wu, P.H.; Kuang, R.; John, M.D.; Tien, P.C.; Link, T.M.; Krug, R.; Kazakia, G.J. Factors associated with bone microstructural alterations assessed by HR-pQCT in long-term HIV-infected individuals. Bone 2020, 133, 115210. [Google Scholar] [CrossRef]
- Womack, J.A.; Murphy, T.E.; Ramsey, C.; Bathulapalli, H.; Leo-Summers, L.; Smith, A.C.; Bates, J.; Jarad, S.; Gill, T.M.; Hsieh, E.; et al. Brief Report: Are Serious Falls Associated with Subsequent Fragility Fractures Among Veterans Living with HIV? J. Acquir. Immune Defic. Syndr. 2021, 88, 192–196. [Google Scholar] [CrossRef]
- Ahmed, M.H.; Woodward, C.; Mital, D. Metabolic clinic for individuals with HIV/AIDS: A commitment and vision to the future of HIV services. Cardiovasc. Endocrinol. 2017, 6, 109–112. [Google Scholar] [CrossRef]
- Shiau, S.; Broun, E.C.; Arpadi, S.M.; Yin, M.T. Incident fractures in HIV-infected individuals: A systematic review and meta-analysis. AIDS 2013, 27, 1949–1957. [Google Scholar] [CrossRef] [Green Version]
- Dong, H.V.; Cortes, Y.I.; Shiau, S.; Yin, M.T. Osteoporosis and fractures in HIV/hepatitis C virus coinfection: A systematic review and meta-analysis. AIDS 2014, 28, 2119–2131. [Google Scholar] [CrossRef] [Green Version]
- O’Neill, T.J.; Rivera, L.; Struchkov, V.; Zaheen, A.; Thein, H.H. The effect of HIV-hepatitis C co-infection on bone mineral density and fracture: A meta-analysis. PLoS ONE 2014, 9, e101493. [Google Scholar] [CrossRef]
- Ilha, T.; Comim, F.V.; Copes, R.M.; Compston, J.E.; Premaor, M.O. HIV and Vertebral Fractures: A Systematic Review and Metanalysis. Sci. Rep. 2018, 8, 7838. [Google Scholar] [CrossRef] [Green Version]
- Starup-Linde, J.; Rosendahl, S.B.; Storgaard, M.; Langdahl, B. Management of Osteoporosis in Patients Living with HIV-A Systematic Review and Meta-analysis. J. Acquir. Immune Defic. Syndr. 2020, 83, 1–8. [Google Scholar] [CrossRef]
- Sharma, A.; Shi, Q.; Hoover, D.R.; Anastos, K.; Tien, P.C.; Young, M.A.; Cohen, M.H.; Golub, E.T.; Gustafson, D.; Yin, M.T. Increased Fracture Incidence in Middle-Aged HIV-Infected and HIV-Uninfected Women: Updated Results From the Women’s Interagency HIV Study. J. Acquir. Immune Defic. Syndr. 2015, 70, 54–61. [Google Scholar] [CrossRef] [Green Version]
- Gonciulea, A.; Wang, R.; Althoff, K.N.; Palella, F.J.; Lake, J.; Kingsley, L.A.; Brown, T.T. An increased rate of fracture occurs a decade earlier in HIV+ compared with HIV-men. AIDS 2017, 31, 1435–1443. [Google Scholar] [CrossRef]
- Jespersen, N.A.; Axelsen, F.; Dollerup, J.; Norgaard, M.; Larsen, C.S. The burden of non-communicable diseases and mortality in people living with HIV (PLHIV) in the pre-, early- and late-HAART era. HIV Med. 2021, 22, 478–490. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Wilson, I.B.; Zullo, A.R.; Meyers, D.J.; Lee, Y.; Daiello, L.A.; Kim, D.H.; Kiel, D.P.; Shireman, T.I.; Berry, S.D.; et al. Hip Fracture Rates in Nursing Home Residents with and without HIV. J. Am. Med. Dir. Assoc. 2022, 23, 517–518. [Google Scholar] [CrossRef] [PubMed]
- Thomsen, M.T.; Wiegandt, Y.L.; Gelpi, M.; Knudsen, A.D.; Fuchs, A.; Sigvardsen, P.E.; Kühl, J.T.; Nordestgaard, B.; Køber, L.; Lundgren, J.; et al. Prevalence of and Risk Factors for Low Bone Mineral Density Assessed by Quantitative Computed Tomography in People Living with HIV and Uninfected Controls. J. Acquir. Immune Defic. Syndr. 2020, 83, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Biver, E. Osteoporosis and HIV Infection. Calcif. Tissue Int. 2022, 110, 624–640. [Google Scholar] [CrossRef]
- Chang, C.J.; Chan, Y.L.; Pramukti, I.; Ko, N.Y.; Tai, T.W. People with HIV infection had lower bone mineral density and increased fracture risk: A meta-analysis. Arch. Osteoporos. 2021, 16, 47. [Google Scholar] [CrossRef]
- Macdonald, H.M.; Maan, E.J.; Berger, C.; Dunn, R.A.; Cote, H.C.F.; Murray, M.C.M.; Pick, N.; Prior, J.C. Deficits in bone strength, density and microarchitecture in women living with HIV: A cross-sectional HR-pQCT study. Bone 2020, 138, 115509. [Google Scholar] [CrossRef]
- Sellier, P.; Ostertag, A.; Collet, C.; Trout, H.; Champion, K.; Fernandez, S.; Lopes, A.; Morgand, M.; Clevenbergh, P.; Evans, J.; et al. Disrupted trabecular bone micro-architecture in middle-aged male HIV-infected treated patients. HIV Med. 2016, 17, 550–556. [Google Scholar] [CrossRef]
- Yin, M.T.; Lund, E.; Shah, J.; Zhang, C.A.; Foca, M.; Neu, N.; Nishiyama, K.K.; Zhou, B.; Guo, X.E.; Nelson, J.; et al. Lower peak bone mass and abnormal trabecular and cortical microarchitecture in young men infected with HIV early in life. AIDS 2014, 28, 345–353. [Google Scholar] [CrossRef] [Green Version]
- Ramalho, J.; Martins, C.S.W.; Galvao, J.; Furukawa, L.N.; Domingues, W.V.; Oliveira, I.B.; Dos Reis, L.M.; Pereira, R.M.; Nickolas, T.L.; Yin, M.T.; et al. Treatment of Human Immunodeficiency Virus Infection with Tenofovir Disoproxil Fumarate-Containing Antiretrovirals Maintains Low Bone Formation Rate, But Increases Osteoid Volume on Bone Histomorphometry. J. Bone Miner. Res. 2019, 34, 1574–1584. [Google Scholar] [CrossRef]
- Serrano, S.; Marinoso, M.L.; Soriano, J.C.; Rubies-Prat, J.; Aubia, J.; Coll, J.; Bosch, J.; Del Rio, L.; Vila, J.; Goday, A.; et al. Bone remodelling in human immunodeficiency virus-1-infected patients. A histomorphometric study. Bone 1995, 16, 185–191. [Google Scholar] [CrossRef]
- Rukuni, R.; Rehman, A.M.; Mukwasi-Kahari, C.; Madanhire, T.; Kowo-Nyakoko, F.; McHugh, G.; Filteau, S.; Chipanga, J.; Simms, V.; Mujuru, H.; et al. Effect of HIV infection on growth and bone density in peripubertal children in the era of antiretroviral therapy: A cross-sectional study in Zimbabwe. Lancet Child Adolesc. Health 2021, 5, 569–581. [Google Scholar] [CrossRef]
- Goh, S.S.L.; Lai, P.S.M.; Tan, A.T.B.; Ponnampalavanar, S. Reduced bone mineral density in human immunodeficiency virus-infected individuals: A meta-analysis of its prevalence and risk factors: Supplementary presentation. Osteoporos. Int. 2018, 29, 1683. [Google Scholar] [CrossRef] [Green Version]
- Gregson, C.L.; Madanhire, T.; Rehman, A.; Ferrand, R.A.; Cappola, A.R.; Tollman, S.; Mokoena, T.; ARK Consortium; Micklesfield, L.K.; Wade, A.N.; et al. Osteoporosis, Rather Than Sarcopenia, Is the Predominant Musculoskeletal Disease in a Rural South African Community Where Human Immunodeficiency Virus Prevalence Is High: A Cross-Sectional Study. J. Bone Miner. Res. 2022, 37, 244–255. [Google Scholar] [CrossRef]
- Bolland, M.J.; Grey, A.; Reid, I.R. Skeletal health in adults with HIV infection. Lancet Diabetes Endocrinol. 2015, 3, 63–74. [Google Scholar] [CrossRef]
- Hoy, J.F.; Grund, B.; Roediger, M.; Schwartz, A.V.; Shepherd, J.; Avihingsanon, A.; Badal-Faesen, S.; de Wit, S.; Jacoby, S.; La Rosa, A.; et al. Immediate Initiation of Antiretroviral Therapy for HIV Infection Accelerates Bone Loss Relative to Deferring Therapy: Findings from the START Bone Mineral Density Substudy, a Randomized Trial. J. Bone Miner. Res. 2017, 32, 1945–1955. [Google Scholar] [CrossRef] [Green Version]
- Guo, F.; Song, X.; Li, Y.; Guan, W.; Pan, W.; Yu, W.; Li, T.; Hsieh, E. Longitudinal change in bone mineral density among Chinese individuals with HIV after initiation of antiretroviral therapy. Osteoporos. Int. 2021, 32, 321–332. [Google Scholar] [CrossRef]
- Han, W.M.; Wattanachanya, L.; Apornpong, T.; Jantrapakde, J.; Avihingsanon, A.; Kerr, S.J.; Teeratakulpisarn, N.; Jadwattanakul, T.; Chaiwatanarat, T.; Buranasupkajorn, P.; et al. Bone mineral density changes among people living with HIV who have started with TDF-containing regimen: A five-year prospective study. PLoS ONE 2020, 15, e0230368. [Google Scholar] [CrossRef]
- Biver, E.; Calmy, A.; Delhumeau, C.; Durosier, C.; Zawadynski, S.; Rizzoli, R. Microstructural alterations of trabecular and cortical bone in long-term HIV-infected elderly men on successful antiretroviral therapy. AIDS 2014, 28, 2417–2427. [Google Scholar] [CrossRef] [Green Version]
- Vikulina, T.; Fan, X.; Yamaguchi, M.; Roser-Page, S.; Zayzafoon, M.; Guidot, D.M.; Ofotokun, I.; Weitzmann, M.N. Alterations in the immuno-skeletal interface drive bone destruction in HIV-1 transgenic rats. Proc. Natl. Acad. Sci. USA 2010, 107, 13848–13853. [Google Scholar] [CrossRef] [Green Version]
- Titanji, K.; Vunnava, A.; Sheth, A.N.; Delille, C.; Lennox, J.L.; Sanford, S.E.; Foster, A.; Knezevic, A.; Easley, K.A.; Weitzmann, M.N.; et al. Dysregulated B cell expression of RANKL and OPG correlates with loss of bone mineral density in HIV infection. PLoS Pathog. 2014, 10, e1004497. [Google Scholar] [CrossRef] [PubMed]
- Ofotokun, I.; Titanji, K.; Vunnava, A.; Roser-Page, S.; Vikulina, T.; Villinger, F.; Rogers, K.; Sheth, A.N.; Lahiri, C.D.; Lennox, J.L.; et al. Antiretroviral therapy induces a rapid increase in bone resorption that is positively associated with the magnitude of immune reconstitution in HIV infection. AIDS 2016, 30, 405–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ofotokun, I.; Titanji, K.; Vikulina, T.; Roser-Page, S.; Yamaguchi, M.; Zayzafoon, M.; Williams, I.R.; Weitzmann, M.N. Role of T-cell reconstitution in HIV-1 antiretroviral therapy-induced bone loss. Nat. Commun. 2015, 6, 8282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biver, E.; Calmy, A.; Rizzoli, R. Bone health in HIV and hepatitis B or C infections. Ther. Adv. Musculoskelet. Dis. 2017, 9, 22–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Titanji, K. Beyond Antibodies: B Cells and the OPG/RANK-RANKL Pathway in Health, Non-HIV Disease and HIV-Induced Bone Loss. Front. Immunol. 2017, 8, 1851. [Google Scholar] [CrossRef] [Green Version]
- Delpino, M.V.; Quarleri, J. Influence of HIV Infection and Antiretroviral Therapy on Bone Homeostasis. Front. Endocrinol. 2020, 11, 502. [Google Scholar] [CrossRef]
- Raynaud-Messina, B.; Bracq, L.; Dupont, M.; Souriant, S.; Usmani, S.M.; Proag, A.; Pingris, K.; Soldan, V.; Thibault, C.; Capilla, F.; et al. Bone degradation machinery of osteoclasts: An HIV-1 target that contributes to bone loss. Proc. Natl. Acad. Sci. USA 2018, 115, E2556–E2565. [Google Scholar] [CrossRef] [Green Version]
- Ofotokun, I. Deciphering how HIV-1 weakens and cracks the bone. Proc. Natl. Acad. Sci. USA 2018, 115, 2551–2553. [Google Scholar] [CrossRef] [Green Version]
- Moran, C.A.; Weitzmann, M.N.; Ofotokun, I. Bone Loss in HIV Infection. Curr. Treat. Options Infect. Dis. 2017, 9, 52–67. [Google Scholar] [CrossRef] [Green Version]
- Atencio, P.; Conesa-Buendia, F.M.; Cabello-Ubeda, A.; Llamas-Granda, P.; Perez-Tanoira, R.; Prieto-Perez, L.; Álvarez, B.Á.; Acosta, I.C.; Arboiro-Pinel, R.; Díaz-Curiel, M.; et al. Bone Deleterious Effects of Different NRTIs in Treatment-naive HIV Patients After 12 and 48 Weeks of Treatment. Curr. HIV Res. 2021, 19, 434–447. [Google Scholar] [CrossRef]
- Van Welzen, B.J.; Thielen, M.A.J.; Mudrikova, T.; Arends, J.E.; Hoepelman, A.I.M. Switching tenofovir disoproxil fumarate to tenofovir alafenamide results in a significant decline in parathyroid hormone levels: Uncovering the mechanism of tenofovir disoproxil fumarate-related bone loss? AIDS 2019, 33, 1531–1534. [Google Scholar] [CrossRef]
- Campbell, L.; Ibrahim, F.; Barbini, B.; Samarawickrama, A.; Orkin, C.; Fox, J.; Waters, L.; Gilleece, Y.; Tariq, S.; Post, F.A.; et al. Bone mineral density, kidney function and participant-reported outcome measures in women who switch from tenofovir disoproxil emtricitabine and a nonnucleoside reverse transcriptase inhibitor to abacavir, lamivudine and dolutegravir. HIV Med. 2022, 23, 362–370. [Google Scholar] [CrossRef]
- Nishijima, T.; Mutoh, Y.; Kawasaki, Y.; Tomonari, K.; Kikuchi, Y.; Gatanaga, H.; Oka, S.; ACC Study Team. Cumulative exposure of TDF is associated with kidney tubulopathy whether it is currently used or discontinued. AIDS 2018, 32, 179–188. [Google Scholar] [CrossRef]
- Gupta, S.K.; Post, F.A.; Arribas, J.R.; Eron, J.J., Jr.; Wohl, D.A.; Clarke, A.E.; Sax, P.E.; Stellbrink, H.J.; Esser, S.; Pozniak, A.L.; et al. Renal safety of tenofovir alafenamide vs. tenofovir disoproxil fumarate: A pooled analysis of 26 clinical trials. AIDS 2019, 33, 1455–1465. [Google Scholar] [CrossRef]
- Maggiolo, F.; Rizzardini, G.; Raffi, F.; Pulido, F.; Mateo-Garcia, M.G.; Molina, J.M.; Ong, E.; Shao, Y.; Piontkowsky, D.; Das, M.; et al. Bone mineral density in virologically suppressed people aged 60 years or older with HIV-1 switching from a regimen containing tenofovir disoproxil fumarate to an elvitegravir, cobicistat, emtricitabine, and tenofovir alafenamide single-tablet regimen: A multicentre, open-label, phase 3b, randomised trial. Lancet HIV 2019, 6, e655–e666. [Google Scholar]
- Baranek, B.; Wang, S.; Cheung, A.M.; Mishra, S.; Tan, D.H. The effect of tenofovir disoproxil fumarate on bone mineral density: A systematic review and meta-analysis. Antivir. Ther. 2020, 25, 21–32. [Google Scholar] [CrossRef]
- Yin, M.T.; RoyChoudhury, A.; Nishiyama, K.; Lang, T.; Shah, J.; Olender, S.; Ferris, D.C.; Zeana, C.; Sharma, A.; Zingman, B.; et al. Bone density and microarchitecture in hepatitis C and HIV-coinfected postmenopausal minority women. Osteoporos. Int. 2018, 29, 871–879. [Google Scholar] [CrossRef]
- Bedimo, R.; Maalouf, N.M.; Lo Re, V., 3rd. Hepatitis C virus coinfection as a risk factor for osteoporosis and fracture. Curr. Opin. HIV AIDS 2016, 11, 285–293. [Google Scholar] [CrossRef]
- Di Carlo, P.; Siracusa, L.; Mazzola, G.; Colletti, P.; Soresi, M.; Giannitrapani, L.; Li Vecchi, V.; Montalto, G. Vitamin D and Osteoporosis in HIV/HCV Coinfected Patients: A Literature Review. Int. J. Endocrinol. 2015, 2015, 969040. [Google Scholar] [CrossRef] [Green Version]
- Carrero, A.; Berenguer, J.; Hontanon, V.; Guardiola, J.M.; Navarro, J.; von Wichmann, M.A.; Téllez, M.J.; Quereda, C.; Santos, I.; Sanz, J.; et al. Effects of Hepatitis C Virus (HCV) Eradication on Bone Mineral Density in Human Immunodeficiency Virus/HCV-Coinfected Patients. Clin. Infect. Dis. 2021, 73, e2026–e2033. [Google Scholar] [CrossRef]
- Mirza, F.S.; Luthra, P.; Chirch, L. Endocrinological aspects of HIV infection. J. Endocrinol. Investig. 2018, 41, 881–899. [Google Scholar] [CrossRef] [PubMed]
- Emokpae, M.A.; Akinnuoye, I.M. Asymptomatic thyroid dysfunction in human immunodeficiency virus-1-infected subjects. J. Lab. Physicians 2018, 10, 130–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, M.; Ahmed, M.; Mital, D.; Ahmed, M.H. Management of hypercholesterolemia in individuals living with HIV/AIDS. In Cholesterol: From Chemistry and Biophysics to the Clinic; Academic Press: Cambridge, MA, USA, 2022; pp. 999–1020. [Google Scholar]
- Shieh, A.; Greendale, G.A.; Cauley, J.A.; Srikanthan, P.; Karlamangla, A.S. Longitudinal associations of insulin resistance with change in bone mineral density in midlife women. JCI Insight 2022, 7, e162085. [Google Scholar] [CrossRef]
- Ahn, S.H.; Seo, D.H.; Kim, S.H.; Nam, M.S.; Hong, S. The relationship between fatty liver index and bone mineral density in Koreans: KNHANES 2010–2011. Osteoporos. Int. 2018, 29, 181–190. [Google Scholar] [CrossRef] [PubMed]
- Choo, M.S.; Choi, S.R.; Han, J.H.; Lee, S.H.; Shim, Y.S. Association of insulin resistance with near peak bone mass in the femur and lumbar spine of Korean adults aged 25–35: The Korean National Health and Nutrition Examination Survey 2008–2010. PLoS ONE 2017, 12, e0177311. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Chen, F.; Liu, L.; Zhang, Q. Prevalence of osteoporosis in patients with diabetes mellitus: A systematic review and meta-analysis of observational studies. BMC Endocr. Disord. 2023, 23, 1. [Google Scholar] [CrossRef]
- Xu, Z.; He, P.; Xian, J.; Lu, W.; Shu, J.; Luo, W.; Gan, C.; Ke, R.; Xia, J.; Han, Z.; et al. Association between Nonalcoholic Fatty Liver Disease and Bone Mineral Density in HIV-Infected Patients Receiving Long-term TDF-Based Antiretroviral Therapy. Curr. HIV Res. 2021, 19, 40–46. [Google Scholar] [CrossRef]
- Biver, E.; Calmy, A.; Aubry-Rozier, B.; Birkhäuser, M.; Bischoff-Ferrari, H.A.; Ferrari, S.; Frey, D.; Kressig, R.W.; Lamy, O.; Lippuner, K.; et al. Diagnosis, prevention, and treatment of bone fragility in people living with HIV: A position statement from the Swiss Association against Osteoporosis. Osteoporos. Int. 2019, 30, 1125–1135. [Google Scholar] [CrossRef]
- Brown, T.T.; Hoy, J.; Borderi, M.; Guaraldi, G.; Renjifo, B.; Vescini, F.; Yin, M.T.; Powderly, W.G. Recommendations for evaluation and management of bone disease in HIV. Clin. Infect. Dis. 2015, 60, 1242–1251. [Google Scholar] [CrossRef] [Green Version]
- Yin, M.T.; Shiau, S.; Rimland, D.; Gibert, C.L.; Bedimo, R.J.; Rodriguez-Barradas, M.C.; Harwood, K.; Aschheim, J.; Justice, A.C.; Womack, J.A. Fracture Prediction with Modified-FRAX in Older HIV-Infected and Uninfected Men. J. Acquir. Immune Defic. Syndr. 2016, 72, 513–520. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.; Sharma, A.; Shi, Q.; Anastos, K.; Cohen, M.H.; Golub, E.T.; Gustafson, D.; Merenstein, D.; Mack, W.J.; Tien, P.C.; et al. Improved fracture prediction using different fracture risk assessment tool adjustments in HIV-infected women. AIDS 2018, 32, 1699–1706. [Google Scholar] [CrossRef]
- Hoy, J.F.; Richardson, R.; Ebeling, P.R.; Rojas, J.; Pocock, N.; Kerr, S.J.; Martinez, E.; Carr, A.; ZEST Study Investigators. Zoledronic acid is superior to tenofovir disoproxil fumarate-switching for low bone mineral density in adults with HIV. AIDS 2018, 32, 1967–1975. [Google Scholar] [CrossRef]
- Carr, A.; Kerr, S.J.; Richardson, R.; Ebeling, P.; Pocock, N.; Rojas, J.; Martinez, E.; Hoy, J.; ZEST study Investigators. Prolonged Effect of Zoledronic Acid on Bone Mineral Density and Turnover in HIV-Infected Adults on Tenofovir: A Randomized, Open-Label Study. J. Bone Miner. Res. 2019, 34, 2192–2197. [Google Scholar] [CrossRef]
- Lei, J.J.H.; Pereira, B.; Moyle, G.; Boffito, M.; Milinkovic, A. The benefits of tenofovir discontinuation with or without bisphosphonate therapy in osteoporotic people living with HIV. HIV Med. 2021, 22, 816–823. [Google Scholar] [CrossRef]
- Venter, W.D.F.; Sokhela, S.; Simmons, B.; Moorhouse, M.; Fairlie, L.; Mashabane, N.; Serenata, C.; Akpomiemie, G.; Masenya, M.; Qavi, A.; et al. Dolutegravir with emtricitabine and tenofovir alafenamide or tenofovir disoproxil fumarate versus efavirenz, emtricitabine, and tenofovir disoproxil fumarate for initial treatment of HIV-1 infection (ADVANCE): Week 96 results from a randomised, phase 3, non-inferiority trial. Lancet HIV 2020, 7, e666–e676. [Google Scholar]
- Surial, B.; Mugglin, C.; Calmy, A.; Cavassini, M.; Günthard, H.F.; Stöckle, M.; Bernasconi, E.; Schmid, P.; Tarr, P.E.; Furrer, H.; et al. Weight and Metabolic Changes After Switching From Tenofovir Disoproxil Fumarate to Tenofovir Alafenamide in People Living with HIV: A Cohort Study. Ann. Intern. Med. 2021, 174, 758–767. [Google Scholar] [CrossRef]
- King, E.M.; Swann, S.A.; Prior, J.C.; Berger, C.; Mayer, U.; Pick, N.; Campbell, A.R.; Côté, H.C.F.; Murray, M.C.M. CIHR team on Cellular Aging and HIV Comorbidities in Women and Children (CARMA). Vitamin D intakes among women living with and without HIV in Canada. HIV Med. 2023. Online ahead of print. [Google Scholar] [CrossRef]
- Kanwal, W.; Rehman, A. High prevalence of vitamin D deficiency in HIV-infected individuals in comparison with the general population across Punjab province, Pakistan. Saudi J. Biol. Sci. 2023, 30, 103484. [Google Scholar] [CrossRef]
- Mansueto, P.; Seidita, A.; Vitale, G.; Gangemi, S.; Iaria, C.; Cascio, A. Vitamin D Deficiency in HIV Infection: Not Only a Bone Disorder. BioMed Res. Int. 2015, 2015, 735615. [Google Scholar] [CrossRef]
- Ryom, L.; De Miguel, R.; Cotter, A.G.; Podlekareva, D.; Beguelin, C.; Waalewijn, H.; Arribas, J.R.; Mallon, P.W.G.; Marzolini, C.; Kirk, O.; et al. Major revision version 11.0 of the European AIDS Clinical Society Guidelines 2021. HIV Med. 2022, 23, 849–858. [Google Scholar] [CrossRef]
- Wang, Y.; Huang, X.; Wu, Y.; Li, A.; Tian, Y.; Ren, M.; Li, Z.; Zhang, T.; Wu, H.; Wang, W. Increased Risk of Vitamin D Deficiency Among HIV-Infected Individuals: A Systematic Review and Meta-Analysis. Front. Nutr. 2021, 8, 722032. [Google Scholar] [CrossRef] [PubMed]
- Qurban, R.; Saeed, S.; Kanwal, W.; Junaid, K.; Rehman, A. Potential immune modulatory effect of vitamin D in HIV infection: A review. Clin. Nutr. ESPEN 2022, 47, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, N.; Aguilar-Jimenez, W.; Rugeles, M.T. The Potential Protective Role of Vitamin D Supplementation on HIV-1 Infection. Front. Immunol. 2019, 10, 2291. [Google Scholar] [CrossRef] [PubMed]
- Netto, E.C.; Silva, A.C.; Pedroso, C.; Brites, C. Hypovitaminosis D Is Associated with Higher Levels of Inflammatory Cytokines and with HAM/TSP in HTLV-Infected Patients. Viruses 2021, 13, 2223, Erratum in Viruses 2022, 14, 1633. [Google Scholar] [CrossRef] [PubMed]
- Havens, P.L.; Stephensen, C.B.; Hazra, R.; Flynn, P.M.; Wilson, C.M.; Rutledge, B.; Bethel, J.; Pan, C.G.; Woodhouse, L.R.; Van Loan, M.D.; et al. Vitamin D3 decreases parathyroid hormone in HIV-infected youth being treated with tenofovir: A randomized, placebo-controlled trial. Clin. Infect. Dis. 2012, 54, 1013–1025. [Google Scholar] [CrossRef] [Green Version]
- Giacomet, V.; Vigano, A.; Manfredini, V.; Cerini, C.; Bedogni, G.; Mora, S.; Borelli, M.; Trabattoni, D.; Zuccotti GVGiacomet, V.; Vigano, A. Cholecalciferol supplementation in HIV-infected youth with vitamin D insufficiency: Effects on vitamin D status and T-cell phenotype: A randomized controlled trial. HIV Clin. Trials 2013, 14, 51–60. [Google Scholar] [CrossRef] [Green Version]
- Havens, P.L.; Stephensen, C.B.; Van Loan, M.D.; Schuster, G.U.; Woodhouse, L.R.; Flynn, P.M.; Gordon, C.M.; Pan, C.G.; Rutledge, B.; Harris, D.R.; et al. Vitamin D3 Supplementation Increases Spine Bone Mineral Density in Adolescents and Young Adults with Human Immunodeficiency Virus Infection Being Treated with Tenofovir Disoproxil Fumarate: A Randomized, Placebo-Controlled Trial. Clin. Infect. Dis. 2018, 66, 220–228. [Google Scholar] [CrossRef] [Green Version]
- Sudjaritruk, T.; Bunupuradah, T.; Aurpibul, L.; Kanjanavanit, S.; Chotecharoentanan, T.; Sricharoen, N.; Ounchanum, P.; Suntarattiwong, P.; Pornpaisalsakul, K.; Puthanakit, T.; et al. Impact of Vitamin D and Calcium Supplementation on Bone Mineral Density and Bone Metabolism among Thai Adolescents with Perinatally Acquired Human Immunodeficiency Virus (HIV) Infection: A Randomized Clinical Trial. Clin. Infect. Dis. 2021, 73, 1555–1564. [Google Scholar] [CrossRef]
- Overton, E.T.; Chan, E.S.; Brown, T.T.; Tebas, P.; McComsey, G.A.; Melbourne, K.M.; Napoli, A.; Hardin, W.R.; Ribaudo, H.J.; Yin, M.T. Vitamin D and Calcium Attenuate Bone Loss with Antiretroviral Therapy Initiation: A Randomized Trial. Ann. Intern. Med. 2015, 162, 815–824. [Google Scholar] [CrossRef] [Green Version]
- Havers, F.P.; Detrick, B.; Cardoso, S.W.; Berendes, S.; Lama, J.R.; Sugandhavesa, P.; Mwelase, N.H.; Campbell, T.B.; Gupta, A.; ACTG A5175 PEARLS and NWCS319 Study Teams. Change in vitamin d levels occurs early after antiretroviral therapy initiation and depends on treatment regimen in resource-limited settings. PLoS ONE 2014, 9, e95164. [Google Scholar] [CrossRef]
- Wohl, D.A.; Orkin, C.; Doroana, M.; Pilotto, J.H.; Sungkanuparph, S.; Yeni, P.; Vanveggel, S.; Deckx, H.; Boven, K.W. Change in vitamin D levels and risk of severe vitamin D deficiency over 48 weeks among HIV-1-infected, treatment-naive adults receiving rilpivirine or efavirenz in a Phase III trial (ECHO). Antivir. Ther. 2014, 19, 191–200. [Google Scholar] [CrossRef] [Green Version]
- Cusato, J.; Tempestilli, M.; Calcagno, A.; Vergori, A.; Piselli, P.; Antonucci, M.; Avataneo, V.; Palermiti, A.; Notari, S.; Antinori, A.; et al. Vitamin D as Modulator of Drug Concentrations: A Study on Two Italian Cohorts of People Living with HIV Administered with Efavirenz. Nutrients 2021, 13, 3571. [Google Scholar] [CrossRef]
- Bi, X.; Liu, F.; Zhang, X.; Wang, H.; Ye, Z.; Yun, K.; Huang, X.; Ding, H.; Geng, W.; Xu, J. Vitamin D and Calcium Supplementation Reverses Tenofovir-Caused Bone Mineral Density Loss in People Taking ART or PrEP: A Systematic Review and Meta-Analysis. Front. Nutr. 2022, 9, 749948. [Google Scholar] [CrossRef]
- Pinzone, M.R.; Moreno, S.; Cacopardo, B.; Nunnari, G. Is there enough evidence to use bisphosphonates in HIV-infected patients? A systematic review and meta-analysis. AIDS Rev. 2014, 16, 213–222. [Google Scholar] [PubMed]
- Bolland, M.J.; Grey, A.; Horne, A.M.; Briggs, S.E.; Thomas, M.G.; Ellis-Pegler, R.B.; Gamble, G.D.; Reid, I.R. Effects of intravenous zoledronate on bone turnover and bone density persist for at least five years in HIV-infected men. J. Clin. Endocrinol. Metab. 2012, 97, 1922–1928. [Google Scholar] [CrossRef]
- Negredo, E.; Bonjoch, A.; Pérez-Álvarez, N.; Ornelas, A.; Puig, J.; Herrero, C.; Estany, C.; del Río, L.; di Gregorio, S.; Echeverría, P.; et al. Comparison of two different strategies of treatment with zoledronate in HIV-infected patients with low bone mineral density: Single dose versus two doses in 2 years. HIV Med. 2015, 16, 441–448. [Google Scholar] [CrossRef]
- Ofotokun, I.; Collins, L.F.; Titanji, K.; Foster, A.; Moran, C.A.; Sheth, A.N.; Lahiri, C.D.; Lennox, J.L.; Ward, L.; Easley, K.A.; et al. Antiretroviral Therapy-Induced Bone Loss Is Durably Suppressed by a Single Dose of Zoledronic Acid in Treatment-Naive Persons with Human Immunodeficiency Virus Infection: A Phase IIB Trial. Clin. Infect. Dis. 2020, 71, 1655–1663. [Google Scholar] [CrossRef]
- Ofotokun, I.; Titanji, K.; Lahiri, C.D.; Vunnava, A.; Foster, A.; Sanford, S.E.; Sheth, A.N.; Lennox, J.L.; Knezevic, A.; Ward, L.; et al. A Single-dose Zoledronic Acid Infusion Prevents Antiretroviral Therapy-induced Bone Loss in Treatment-naive HIV-infected Patients: A Phase IIb Trial. Clin. Infect. Dis. 2016, 63, 663–671. [Google Scholar] [CrossRef] [Green Version]
- Bolland, M.J.; Horne, A.M.; Briggs, S.E.; Thomas, M.G.; Reid, I.; Gamble, G.D.; Grey, A.B. Effects of Intravenous Zoledronate on Bone Turnover and Bone Density Persist for at Least 11 Years in HIV-Infected Men. J. Bone Miner. Res. 2019, 34, 1248–1253. [Google Scholar] [CrossRef]
- Huang, J.; Meixner, L.; Fernandez, S.; McCutchan, J.A. A double-blinded, randomized controlled trial of zoledronate therapy for HIV-associated osteopenia and osteoporosis. AIDS 2009, 23, 51–57. [Google Scholar] [CrossRef] [Green Version]
- Bolland, M.J.; Grey, A.B.; Horne, A.M.; Briggs, S.E.; Thomas, M.G.; Ellis-Pegler, R.B.; Woodhouse, A.F.; Gamble, G.D.; Reid, I.R. Annual zoledronate increases bone density in highly active antiretroviral therapy-treated human immunodeficiency virus-infected men: A randomized controlled trial. J. Clin. Endocrinol. Metab. 2007, 92, 1283–1288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, W.; Li, X.F.; Ren, D.C.; Song, M.; Duan, L.; Liu, J.Z.; Zhan, Z.R. Administration of zoledronic acid alleviates osteoporosis in HIV patients by suppressing osteoclastogenesis via regulating RANKL expression. Mol. Med. 2021, 27, 19. [Google Scholar] [CrossRef] [PubMed]
- McComsey, G.A.; Kendall, M.A.; Tebas, P.; Swindells, S.; Hogg, E.; Alston-Smith, B.; Suckow, C.; Gopalakrishnan, G.; Benson, C.; Wohl, D.A. Alendronate with calcium and vitamin D supplementation is safe and effective for the treatment of decreased bone mineral density in HIV. AIDS 2007, 21, 2473–2482. [Google Scholar] [CrossRef] [Green Version]
- Rozenberg, S.; Lanoy, E.; Bentata, M.; Viard, J.P.; Valantin, M.A.; Missy, P.; Darasteanu, I.; Roux, C.; Kolta, S.; Costagliola, D.; et al. Effect of alendronate on HIV-associated osteoporosis: A randomized, double-blind, placebo-controlled, 96-week trial (ANRS 120). AIDS Res. Hum. Retrovir. 2012, 28, 972–980. [Google Scholar] [CrossRef]
- Jacobson, D.L.; Lindsey, J.C.; Gordon, C.; Hazra, R.; Spiegel, H.; Ferreira, F.; Amaral, F.R.; Pagano-Therrien, J.; Gaur, A.; George, K.; et al. Alendronate Improves Bone Mineral Density in Children and Adolescents Perinatally Infected with Human Immunodeficiency Virus with Low Bone Mineral Density for Age. Clin. Infect. Dis. 2020, 71, 1281–1288. [Google Scholar] [CrossRef]
- Lindsey, J.C.; Jacobson, D.L.; Spiegel, H.M.; Gordon, C.M.; Hazra, R.; Siberry, G.K. Safety and Efficacy of 48 and 96 Weeks of Alendronate in Children and Adolescents with Perinatal Human Immunodeficiency Virus Infection and Low Bone Mineral Density for Age. Clin. Infect. Dis. 2021, 72, 1059–1063. [Google Scholar] [CrossRef]
- Guaraldi, G.; Orlando, G.; Madeddu, G.; Vescini, F.; Ventura, P.; Campostrini, S.; Mura, M.S.; Parise, N.; Caudarella, R.; Esposito, R. Alendronate reduces bone resorption in HIV-associated osteopenia/osteoporosis. HIV Clin. Trials 2004, 5, 269–277. [Google Scholar] [CrossRef]
- Negredo, E.; Martinez-Lopez, E.; Paredes, R.; Rosales, J.; Perez-Alvarez, N.; Holgado, S.; Gel, S.; del Rio, L.; Tena, X.; Rey-Joly, C.; et al. Reversal of HIV-1-associated osteoporosis with once-weekly alendronate. AIDS 2005, 19, 343–345. [Google Scholar]
- Mondy, K.; Powderly, W.G.; Claxton, S.A.; Yarasheski, K.H.; Royal, M.; Stoneman, J.S.; Hoffmann, M.E.; Tebas, P. Alendronate, vitamin D, and calcium for the treatment of osteopenia/osteoporosis associated with HIV infection. J. Acquir. Immune Defic. Syndr. 2005, 38, 426–431. [Google Scholar] [CrossRef]
- Rocha, V.M.D.; Faria, M.B.B.; Junior, F.; Lima, C.; Fiorelli, R.K.A.; Cassiano, K.M. Use of Bisphosphonates, Calcium and Vitamin D for Bone Demineralization in Patients with Human Immunodeficiency Virus/Acquired Immune Deficiency Syndrome: A Systematic Review and Meta-Analysis of Clinical Trials. J. Bone Metab. 2020, 27, 175–186. [Google Scholar] [CrossRef]
- Makras, P.; Petrikkos, P.; Anastasilakis, A.D.; Kolynou, A.; Katsarou, A.; Tsachouridou, O.; Metallidis, S.; Yavropoulou, M.P. Denosumab versus zoledronate for the treatment of low bone mineral density in male HIV-infected patients. Bone Rep. 2021, 15, 101128. [Google Scholar] [CrossRef] [PubMed]
- Marasco, E.; Mussa, M.; Motta, F.; Bobbio-Pallavicini, F.; Maserati, R.; Montecucco, C.; Bogliolo, L. Denosumab for the treatment of HIV-associated osteoporosis with fractures in a premenopausal woman. Reumatismo 2021, 73, 54–58. [Google Scholar] [CrossRef]
- Wheeler, A.L.; Tien, P.C.; Grunfeld, C.; Schafer, A.L. Teriparatide treatment of osteoporosis in an HIV-infected man: A case report and literature review. AIDS 2015, 29, 245–246. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Theme | Main Outcome of Systematic Review or Meta-Analysis | References |
|---|---|---|
| Prevalence of fracture in PLWHIV | Fragility fracture in HIV was found in meta-analyses to be around 35 to 68% in comparison with the non-HIV-infected population. | [15,16,17,18] |
| Frequency and prevalence of vertebral fracture | The estimated frequency of vertebral fracture in PLWHIV was 22%, while the prevalence was 4.1 to 47%. | [19] |
| HIV and BMD | PLWHIV had lower bone mineral density and increased fracture risk. | [26] |
| HIV, ARV and BMD | The prevalence of osteopenia/osteoporosis in HIV-infected and antiretroviral therapy (ARV)-treated individuals was increased by two times compared to controls. | [33] |
| HIV, osteoporosis and viral hepatitis | Hepatitis C and B were associated with osteoporosis in PLWHIV | [16,17] |
| HIV, TDF and BMD | The impact of TDF in BMD in treatment of HIV, pre-exposure prophylaxis (PrEP) and HBV was assessed. The meta-analysis showed that TDF caused greater decreases in BMD when used for all three indications, and the magnitude of this decrease was greater for HIV treatment compared with PrEP. The risk of fracture did not increase in the PrEP group. | [55] |
| Diabetes and osteoporosis | A high prevalence of osteoporosis was observed among individuals with type 2 diabetes around the globe. | [65] |
| HIV and Vitamin D | PLWHIV were prone to having low Vitamin D compared with the general population, and risk factors were ART, older age, lower BMI, lower latitude and male sex. | [94] |
| Impact of Vitamin D supplements on BMD in PLWHIV | Vitamin D (4000 IU/D) and calcium supplementation was related to a significant increase in BMD in the spine and hip of participants taking TDF-based drugs. | [106] |
| Bisphosphonates and osteoporosis in PLWHIV | Oral and intravenous bisphosphonates were associated with increased bone mineral density at the lumbar spine and total hip over two years in HIV-positive patients. | [107] |
| The combination of bisphosphonate, Vitamin D and calcium | Better improvement in BMD was achieved in PLWHIV when bisphosphonates were combined with calcium and vitamin D | [111] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmed, M.; Mital, D.; Abubaker, N.E.; Panourgia, M.; Owles, H.; Papadaki, I.; Ahmed, M.H. Bone Health in People Living with HIV/AIDS: An Update of Where We Are and Potential Future Strategies. Microorganisms 2023, 11, 789. https://doi.org/10.3390/microorganisms11030789
Ahmed M, Mital D, Abubaker NE, Panourgia M, Owles H, Papadaki I, Ahmed MH. Bone Health in People Living with HIV/AIDS: An Update of Where We Are and Potential Future Strategies. Microorganisms. 2023; 11(3):789. https://doi.org/10.3390/microorganisms11030789
Chicago/Turabian StyleAhmed, Musaab, Dushyant Mital, Nuha Eljaili Abubaker, Maria Panourgia, Henry Owles, Ioanna Papadaki, and Mohamed H. Ahmed. 2023. "Bone Health in People Living with HIV/AIDS: An Update of Where We Are and Potential Future Strategies" Microorganisms 11, no. 3: 789. https://doi.org/10.3390/microorganisms11030789