
Paraprobiotics in Non-Surgical Periodontal Therapy: Clinical and Microbiological Aspects in a 6-Month Follow-Up Domiciliary Protocol for Oral Hygiene

 ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Trial Design
2.2.1. Participants
2.2.2. Interventions and Outcomes
2.2.3. Sample Size
2.2.4. Randomization and Blinding
2.2.5. Statistical Methods
3. Results
3.1. Participant Flow and Baseline Data
3.2. Periodontal Parameters
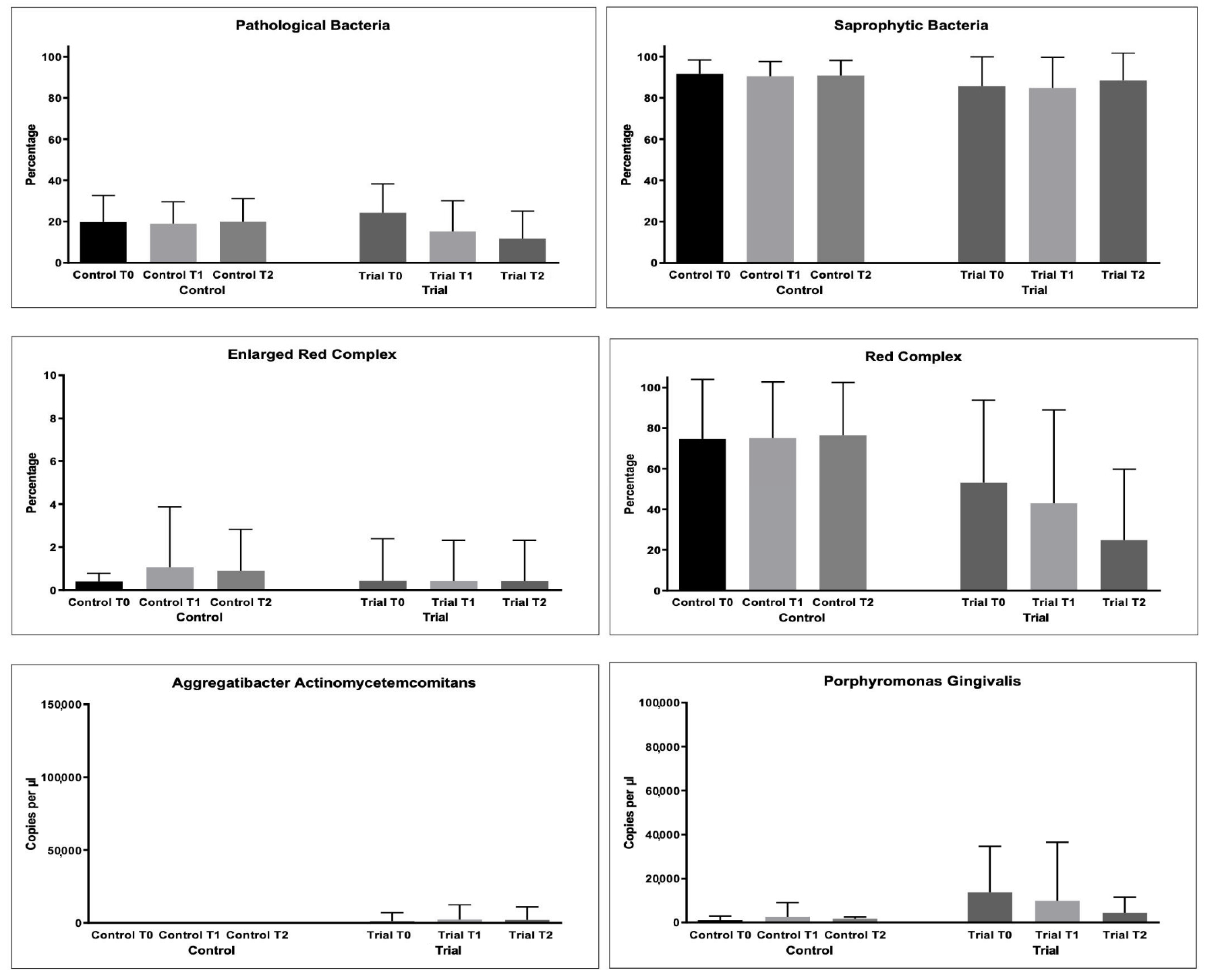
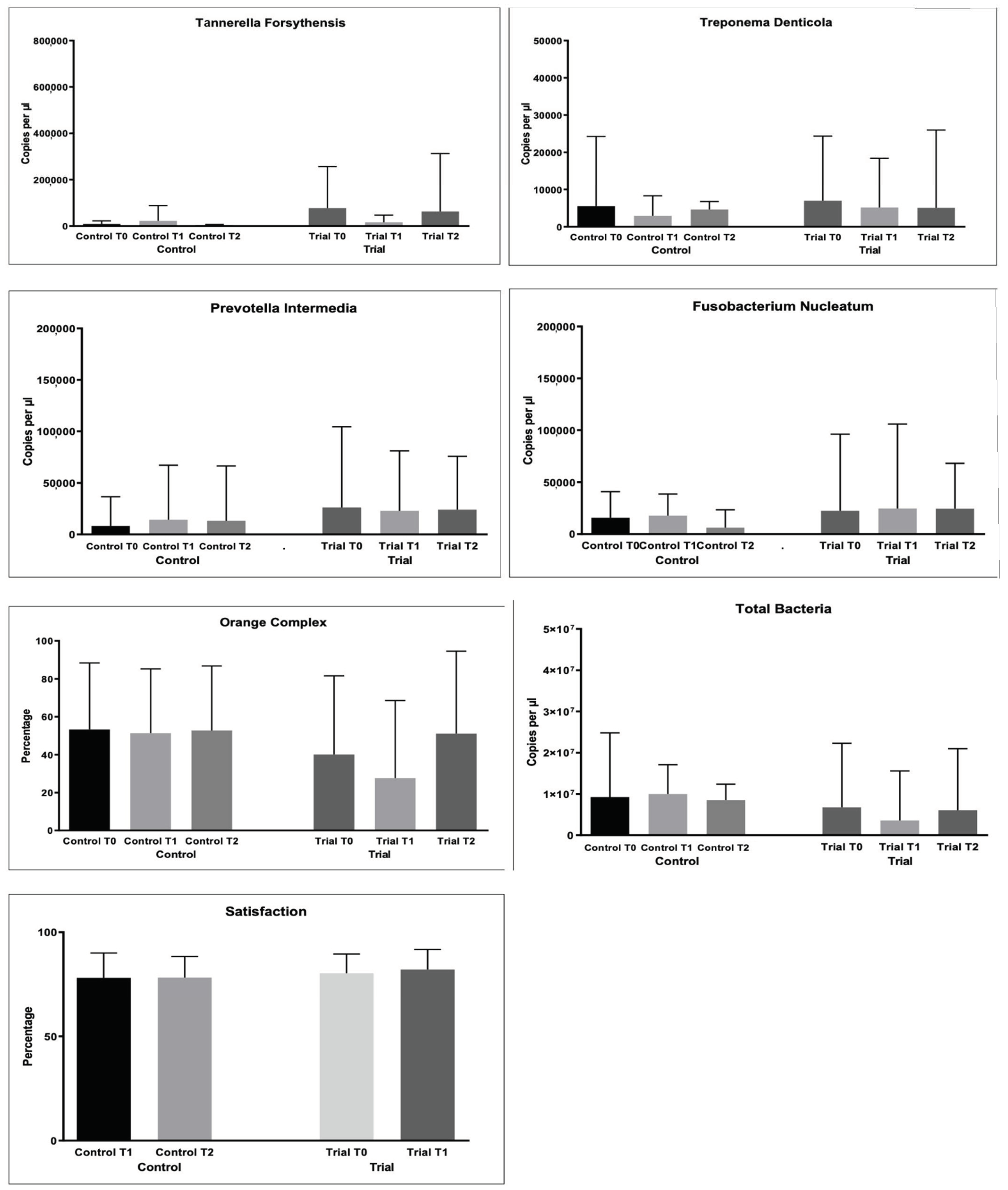
3.3. Microbiological Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baelum, V.; Lopez, R. Periodontal disease epidemiology—Learned and unlearned? Periodontol. 2000 2013, 62, 37–58. [Google Scholar] [CrossRef]
- Preshaw, P.M.; Alba, A.L.; Herrera, D.; Jepsen, S.; Konstantinidis, A.; Makrilakis, K.; Taylor, R. Periodontitis and diabetes: A two-way relationship. Diabetologia 2012, 55, 21–31. [Google Scholar] [CrossRef] [Green Version]
- Kinane, D.F.; Chestnutt, I.G. Smoking and periodontal disease. Crit. Rev. Oral. Biol. Med. 2000, 11, 356–365. [Google Scholar] [CrossRef] [Green Version]
- Wilton, J.M.; Griffiths, G.S.; Curtis, M.A.; Maiden, M.F.; Gillett, I.R.; Wilson, D.T.; Sterne, J.A.; Johnson, N.W. Detection of high-risk groups and individuals for periodontal diseases. Systemic predisposition and markers of general health. J. Clin. Periodontol. 1988, 15, 339–346. [Google Scholar] [CrossRef]
- Barr, C.; Lopez, M.R.; Rua-Dobles, A. Periodontal changes by HIV serostatus in a cohort of homosexual and bisexual men. J. Clin. Periodontol. 1992, 19, 794–801. [Google Scholar] [CrossRef]
- Shapira, L.; Wilensky, A.; Kinane, D.F. Effect of genetic variability on the inflammatory response to periodontal infection. J. Clin. Periodontol. 2005, 32, 72–86. [Google Scholar] [CrossRef]
- Marsh, P.D. Dental plaque: Biological significance of a biofilm and community life-style. J. Clin. Periodontol. 2005, 32, 7–15. [Google Scholar] [CrossRef]
- Berezow, A.B.; Darveau, R.P. Microbial shift and periodontitis. Periodontol. 2000 2011, 55, 36–47. [Google Scholar] [CrossRef]
- Mombelli, A. Microbial colonization of the periodontal pocket and its significance for periodontal therapy. Periodontol. 2000 2018, 76, 85–96. [Google Scholar] [CrossRef]
- de Sousa, E.T.; de Araújo, J.S.M.; Pires, A.C.; Lira Dos Santos, E.J. Local delivery natural products to treat periodontitis: A systematic review and meta-analysis. Clin. Oral Investig. 2021, 25, 4599–4619. [Google Scholar] [CrossRef]
- Anton, D.M.; Martu, M.A.; Maris, M.; Maftei, G.A.; Sufaru, I.G.; Tatarciuc, D.; Luchian, I.; Ioanid, N.; Martu, S. Study on the effects of melatonin on glycemic control and periodontal parameters in patients with type II diabetes mellitus and periodontal disease. Medicina 2021, 57, 140. [Google Scholar] [CrossRef]
- Invernici, M.M.; Salvador, S.L.; Silva, P.; Soares, M.; Casarin, R.; Palioto, D.B.; Souza, S.; Taba, M., Jr.; Novaes, A.B., Jr.; Furlaneto, F.; et al. Effects of bifidobacterium probiotic on the treatment of chronic periodontitis: A randomized clinical trial. J. Clin. Periodontol. 2018, 45, 1198–1210. [Google Scholar] [CrossRef] [Green Version]
- Francino, M. Antibiotics and the human gut microbiome: Dysbioses and accumulation of resistances. Front. Microbiol. 2016, 6, 1543–1545. [Google Scholar] [CrossRef] [Green Version]
- Joint FAO/WHO Working Group. Working Group Report on Drafting Guidelines for the Evaluation of Probiotics in Food; Food and Agriculture Organization of the United Nations; World Health Organization: London, ON, Canada, 2002. [Google Scholar]
- İnce, G.; Gürsoy, H.; İpçi, Ş.D.; Cakar, G.; Emekli-Alturfan, E.; Yılmaz, S. Clinical and biochemical evaluation of lozenges containing lactobacillus reuteri as an adjunct to non-surgical periodontal therapy in chronic periodontitis. J. Periodontol. 2015, 86, 746–754. [Google Scholar] [CrossRef]
- Siciliano, R.A.; Reale, A.; Mazzeo, M.F.; Morandi, S.; Silvetti, T.; Brasca, M. Paraprobiotics: A new perspective for functional foods and nutraceuticals. Nutrients 2021, 13, 1225. [Google Scholar] [CrossRef]
- Piqué, N.; Berlanga, M.; Miñana-Galbis, D. Health benefits of heat-killed (Tyndallized) probiotics: An overview. Int. J. Mol. Sci. 2019, 20, 2534. [Google Scholar] [CrossRef] [Green Version]
- Żółkiewicz, J.; Marzec, A.; Ruszczyński, M.; Feleszko, W. Postbiotics—A step beyond pre- and probiotics. Nutrients 2020, 12, 2189. [Google Scholar] [CrossRef]
- Butera, A.; Gallo, S.; Pascadopoli, M.; Taccardi, D.; Scribante, A. Home oral care of periodontal patients using antimicrobial gel with postbiotics, lactoferrin, and aloe barbadensis leaf juice powder vs. conventional chlorhexidine gel: A split-mouth randomized clinical trial. Antibiotics 2022, 11, 118. [Google Scholar] [CrossRef]
- Michels, M.; Jesus, G.; Voytena, A.; Rossetto, M.; Ramlov, F.; Córneo, E.; Feuser, P.; Gelain, D.; Dal-Pizzol, F. Immunomodulatory effect of bifidobacterium, lactobacillus, and streptococcus strains of paraprobiotics in lipopolysaccharide-stimulated inflammatory responses in RAW-264.7 macrophages. Curr. Microbiol. 2021, 79, 9. [Google Scholar] [CrossRef]
- Shenderov, B.A. Metabiotics: Novel idea or natural development of probiotic conception. Microb. Ecol. Health Dis. 2013, 24, 20399. [Google Scholar] [CrossRef]
- Oleskin, A.V.; Shenderov, B.A. Probiotics and psychobiotics: The role of microbial neurochemicals. Probiotics Antimicrob. Proteins 2019, 11, 1071–1085. [Google Scholar] [CrossRef]
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45, S286–S291. [Google Scholar] [CrossRef] [Green Version]
- Butera, A.; Gallo, S.; Maiorani, C.; Molino, D.; Chiesa, A.; Preda, C.; Esposito, F.; Scribante, A. Probiotic alternative to chlorhexidine in periodontal therapy: Evaluation of clinical and microbiological parameters. Microorganisms 2021, 9, 69. [Google Scholar] [CrossRef]
- Ainamo, J.; Bay, I. Problems and proposals for recording gingivitis and plaque. Int. Dent. J. 1975, 25, 229–235. [Google Scholar]
- Mühlemann, H.R.; Son, S. Gingival sulcus bleeding—A leading symptom in initial gingivitis. Helv. Odontol. Acta 1971, 15, 107–113. [Google Scholar]
- Lange, D.E.; Plagmann, H.C.; Eenboom, A.; Promesberger, A. Klinische Bewertungsverahren zur Objektivierung der Mundhygiene. Dtsch. Zahnarztl. Z. 1977, 32, 44–47. (In German) [Google Scholar]
- Silness, J.; Loe, H. Periodontal disease in pregnancy. II. Correlation between oral hygiene and periodontal condtion. Acta Odontol Scand. 1964, 22, 121–135. [Google Scholar] [CrossRef]
- Martelli, F.S.; Fanti, E.; Rosati, C.; Martelli, M.; Bacci, G.; Martelli, M.L.; Medico, E. Long-term efficacy of microbiology-driven periodontal laser-assisted therapy. Eur. J. Clin. Microbiol. Infect. Dis. 2016, 35, 423–431. [Google Scholar] [CrossRef]
- Cheng, L.; Liu, W.; Zhang, T.; Xu, T.; Shu, Y.X.; Yuan, B.; Yang, Y.M.; Hu, T. Evaluation of the effect of a toothpaste containing Pudilan extract on inhibiting plaques and reducing chronic gingivitis: A randomized, double-blinded, parallel controlled clinical trial. J. Ethnopharmacol. 2019, 240, 111870. [Google Scholar] [CrossRef]
- Piepho, H.P. An algorithm for a letter-based representation of all-pairwise comparisons. J. Comput. Graph. Stat. 2004, 13, 456–466. [Google Scholar] [CrossRef]
- Dubar, M.; Clerc-Urmès, I.; Baumann, C.; Clément, C.; Alauzet, C.; Bisson, C. Relations of psychosocial factors and cortisol with periodontal and bacterial parameters: A prospective clinical study in 30 patients with periodontitis before and after non-surgical treatment. Int. J. Environ. Res. Public Health 2020, 17, 7651. [Google Scholar] [CrossRef]
- Goehler, L.E.; Gaykema, R.P.A.; Opitz, N.; Reddaway, R.; Badr, N.; Lyte, M. Activation in vagal afferents and central autonomic pathways: Early responses to intestinal infection with Campylobacter Jejuni. Brain Behav. Immun. 2005, 19, 334–344. [Google Scholar] [CrossRef]
- Butera, A.; Gallo, S.; Maiorani, C.; Preda, C.; Chiesa, A.; Esposito, F.; Pascadopoli, M.; Scribante, A. Management of gingival bleeding in periodontal patients with domiciliary use of toothpastes containing hyaluronic acid, lactoferrin, or paraprobiotics: A randomized controlled clinical trial. Appl. Sci. 2021, 11, 8586. [Google Scholar] [CrossRef]
- Ikram, S.; Hassan, N.; Baig, S.; Borges, K.J.J.; Raffat, M.A.; Akram, Z. Effect of local probiotic (Lactobacillus reuteri) vs. systemic antibiotic therapy as an adjunct to non-surgical periodontal treatment in chronic periodontitis. J. Investig. Clin. Dent. 2019, 10, e12393. [Google Scholar] [CrossRef]
- Teughels, W.; Durukan, A.; Ozcelik, O.; Pauwels, M.; Quirynen, M.; Haytac, M.C. Clinical and microbiological effects of lactobacillus reuteri probiotics in the treatment of chronic periodontitis: A randomized placebo- controlled study. J. Clin. Periodontol. 2013, 40, 1025–1035. [Google Scholar] [CrossRef] [Green Version]
- Vivekananda, M.R.; Vandana, K.L.; Bhat, K.G. Effect of the probiotic Lactobacilli reuteri (Prodentis) in the management of periodontal disease: A preliminary randomized clinical trial. J. Oral Microbiol. 2010, 2, 5344. [Google Scholar] [CrossRef]
- Szkaradkiewicz, A.K.; Stopa, J.; Karpiński, T.M. Effect of oral administration involving a probiotic strain of lactobacillus reuteri on pro- inflammatory cytokine response in patients with chronic periodontitis. Arch. Immunol. Ther. Exp. 2014, 62, 495–500. [Google Scholar] [CrossRef] [Green Version]
- Mocanu, R.C.; Martu, M.A.; Luchian, I.; Sufaru, I.G.; Maftei, G.A.; Ioanid, N.; Martu, S.; Tatarciuc, M. Microbiologic profiles of patients with dental prosthetic treatment and periodontitis before and after photoactivation therapy-randomized clinical trial. Microorganisms 2021, 9, 713. [Google Scholar] [CrossRef]
- Hammami, C.; Nasri, W. Antibiotics in the treatment of periodontitis: A systematic review of the literature. Int. J. Dent. 2021, 2021, 6846074. [Google Scholar] [CrossRef]
- Yang, B.; Pang, X.; Li, Z.; Chen, Z.; Wang, Y. Immunomodulation in the treatment of periodontitis: Progress and perspectives. Front. Immunol. 2021, 12, 781378. [Google Scholar] [CrossRef]
- Butera, A.; Gallo, S.; Pascadopoli, M.; Luraghi, G.; Scribante, A. Ozonized water administration in peri-implant mucositis sites: A randomized clinical trial. Appl. Sci. 2021, 11, 7812. [Google Scholar] [CrossRef]
- Dompe, C.; Moncrieff, L.; Matys, J.; Grzech-Leśniak, K.; Kocherova, I.; Bryja, A.; Bruska, M.; Dominiak, M.; Mozdziak, P.; Skiba, T.H.I.; et al. Photobiomodulation—Underlying mechanism and clinical applications. J. Clin. Med. 2020, 9, 1724. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Product | Manufacturer | Composition |
|---|---|---|
| Biorepair Peribioma toothpaste | Coswell S.p.A., Funo di Argelato, BO, Italy | Aqua, Sorbitol, Zinc Hydroxyapatite *, Glycerin, Hydrated Silica, Silica, Cocamidopropyl Betaine, Cellulose Gum, Aroma, Sodium Hyaluronate, Hamamelis Virginiana Leaf Extract, Spirulina Platensis Extract, Calendula Officinalis Flower Extract, Bifidobacterium *, Lactobacillus *, Zinc PCA, Benzyl Alcohol, Sodium Benzoate, Phenoxyethanol, Sodium Saccharin, Maltodextrin, Citric Acid, Potassium Sorbate, Sodium Myristoyl Sarcosinate, Sodium Methyl Cocoyl Taurate, Limonene, Eugenol, CI 77891, CI 16255. |
| Biorepair Peribioma Mousse mouthwash | Coswell S.p.A., Funo di Argelato, BO, Italy | Aqua, Sorbitol, Xylitol, Zinc Hydroxyapatite *, Aroma, Pistacia Lentiscus (Mastic) Gum Oil, Lactobacillus *, Bifidobacterium*,Sodium Hyaluronate, Ascorbic Acid, Hamamelis Virginiana Leaf Extract, Spirulina Platensis Extract, Calendula Officinalis Flower Extract, Tocopheryl Acetate, Retinyl Palmitate, Eucalyptus Globulus Leaf Oil, PEG-40 Hydrogenated Castor Oil, Phenoxyethanol, Sodium Benzoate, Cocamidopropyl Betaine, Glycerin, Maltodextrin, Sodium Saccharin, Helianthus Annuus Seed Oil, Potassium Sorbate, BHT, Limonene, CI 16255. |
| Curasept Intensive Treatment (0.2% chlorhexidine) toothpaste | Curasept S.p.A., Saronno, VA, Italy | Purified Water, Sorbitol, Hydrated Silica, PEG-32, Cocamidopropyl Betaine, Xylitol, Cellulose Gum, Aroma, Sodium Hyaluronate, Ascorbic Acid, Chlorhexidine, Digluconate, Sodium Metabisulfite, Sodium Citrate, Titanium Dioxide (C.I. 77891), Sodium Benzoate, Sodium Saccharin, Citric Acid, C.I. 17200, C.I. 42090. |
| Appointment | Procedures |
|---|---|
| |
| |
| |
| Baseline (T0) |
|
| |
| |
| After 3 months (T3) After 6 months (T6) |
|
| Group | Time | BOP | PPD | CAL | BS | SBI | API | PI | AG | GR | PS |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Mean | Mean | Mean | Mean | Mean | Mean | Mean | Mean | Mean | ||
| (SD) | (SD) | (SD) | (SD) | (SD) | (SD) | (SD) | (SD) | (SD) | (SD) | ||
| Control | T0 | 81.25 (17.23) a | 6.88 (1.26) a,d | 6.83 (1.87) a | 1.78 (0.80) a | 1.96 (0.80) a | 79.75 (21.61) a | 70.00 (26.56) a,b,c | 2.85 (0.67) a,b | 3.48 (1.28) a | 94.00 (10.46) a |
| T1 | 69.25 (18.16) b | 5.55 (1.27) b,e | 6.05 (2.07) b,c | 1.68 (0.75) a | 1.82 (0.73) a | 78.00 (20.03) a | 51.75 (23.13) b | 2.55 (0.61) b | 3.40 (1.18) a | 67.50 (13.33) b | |
| T2 | 74.00 (14.01) b | 6.40 (1.08) c,f | 6.53 (1.82) a | 1.70 (0.57) a | 2.00 (0.44) a | 81.00 (20.17) a | 72.00 (22.33) a,c | 2.75 (0.62) a,b | 3.44 (1.19) a | 76.25 (8.41) c | |
| Trial | T0 | 66.75 (33.41) a,b | 6.69 (1.15) b,c,d | 6.23 (0.62) a,b | 1.46 (0.80) a | 2.15 (0.83) a | 93.50 (15.65) a | 83.00 (18.95) c | 3.21 (0.72) a | 3.23 (0.78) a | 62.35 (39.55) b,c |
| T1 | 29.25 (20.82) c | 5.92 (0.64) a,e,f | 5.73 (0.94) a,b | 0.90 (0.36) b | 1.74 (0.84) a,b | 71.00 (31.48) a,b | 54.50 (23.50) a,b,d | 3.18 (0.70) a | 3.20 (0.73) a | 24.55 (21.98) d | |
| T2 | 26.00 (14.85) c | 4.91 (1.18) e | 4.64 (1.78) c | 0.54 (0.42) c | 1.15 (0.41) b | 67.00 (28.95) b | 46.75 (21.66) b,d | 3.09 (0.80) a,b | 3.08 (0.69) a | 12.46 (17.62) d |
| Group | Time | Total Bacteria Count | AAE | PG | TF | TD | PI | FN |
|---|---|---|---|---|---|---|---|---|
| Mean | Mean | Mean | Mean | Mean | Mean | Mean | ||
| (SD) | (SD) | (SD) | (SD) | (SD) | (SD) | (SD) | ||
| Control | T0 | 9,225,901.65 (15,558,308.5) a | 0.83 (2.20) a | 1053.05 (1842.44) a | 8416.22 (13584.71) a | 5505.00 (18730.81) a | 8295.00 (28278.05) a | 15,792.48 (25232.49) a |
| T1 | 9,986,050.23 (7,074,899.18) a | 0.64 (2.61) a | 2567.22 (6425.14) a | 21,956.85 (65,796.72) a | 2959.11 (5366.56) a | 14,227.38 (52,965.73) a | 17,811.83 (20,803.62) a | |
| T2 | 8,502,000.00 (3,858,474.75) a | 1.05 (2.14) a | 1695.80 (794.89) a | 4099.00 (1993.82) a | 4651.00 (2158.87) a | 13,304.81 (53,130.25) a | 6275.86 (17,221.46) a | |
| Trial | T0 | 6,732,956.50 (15,565,648.5) a | 1315.00 (5669.24) a | 13,634.51 (21,032.74) a | 77,338.46 (179,432.46) a | 7023.45 (17,331.05) a | 26,163.01 (78,205.03) a | 22,547.43 (73,550.18) a |
| T1 | 3,577,611.70 (12,004,436.6) a | 2300.00 (10,074.20) a | 9933.55 (26,547.19) a | 14,984.63 (31,781.70) a | 5189.00 (13,216.46) a | 22,916.50 (58,000.75) a | 24,758.25 (81,217.50) a | |
| T2 | 6,038,339.10 (14,922,620.2) a | 2045.00 (8933.82) a | 4362.55 (7230.12) a | 62,514.97 (250,286.56) a | 5095.50 (20,882.84) a | 24,086.56 (51,657.98) a | 24,483.45 (43,599.34) a |
| Group | Time | Pathogen Bacteria | Enlarged Red Complex | Red Complex | Orange Complex |
|---|---|---|---|---|---|
| Mean | Mean | Mean | Mean | ||
| (SD) | (SD) | (SD) | (SD) | ||
| Control | T0 | 19.71 (12.93) a | 0.4 | 74.58 | 53.27 |
| (0.39) a | (29.41) a | (35.14) a | |||
| T1 | 18.92 (10.64) a | 1.08 | 75.19 | 51.38 | |
| (2.79) a | (27.52) a | (33.83) a | |||
| T2 | 19.90 (11.20) a | 0.91 | 76.38 | 52.69 | |
| (1.91) a | (26.10) a | (34.08) a | |||
| Trial | T0 | 24.20 (14.09) a | 0.44 | 52.95 | 40.09 |
| (1.95) a | (40.85) a | (41.49) a | |||
| T1 | 15.24 (14.87) a,b | 0.42 | 42.86 | 27.66 | |
| (1.89) a | (46.10) a,b | (40.87) a | |||
| T2 | 11.70 (13.40) b | 0.42 | 24.69 | 51.09 | |
| (1.89) a | (35.02) b | (43.52) a |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Butera, A.; Gallo, S.; Pascadopoli, M.; Maiorani, C.; Milone, A.; Alovisi, M.; Scribante, A. Paraprobiotics in Non-Surgical Periodontal Therapy: Clinical and Microbiological Aspects in a 6-Month Follow-Up Domiciliary Protocol for Oral Hygiene. Microorganisms 2022, 10, 337. https://doi.org/10.3390/microorganisms10020337
Butera A, Gallo S, Pascadopoli M, Maiorani C, Milone A, Alovisi M, Scribante A. Paraprobiotics in Non-Surgical Periodontal Therapy: Clinical and Microbiological Aspects in a 6-Month Follow-Up Domiciliary Protocol for Oral Hygiene. Microorganisms. 2022; 10(2):337. https://doi.org/10.3390/microorganisms10020337
Chicago/Turabian StyleButera, Andrea, Simone Gallo, Maurizio Pascadopoli, Carolina Maiorani, Antonella Milone, Mario Alovisi, and Andrea Scribante. 2022. "Paraprobiotics in Non-Surgical Periodontal Therapy: Clinical and Microbiological Aspects in a 6-Month Follow-Up Domiciliary Protocol for Oral Hygiene" Microorganisms 10, no. 2: 337. https://doi.org/10.3390/microorganisms10020337