
Detection of Helicobacter pylori from Extracted Teeth of a Patient with Idiopathic Thrombocytopenic Purpura
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. DNA Extraction
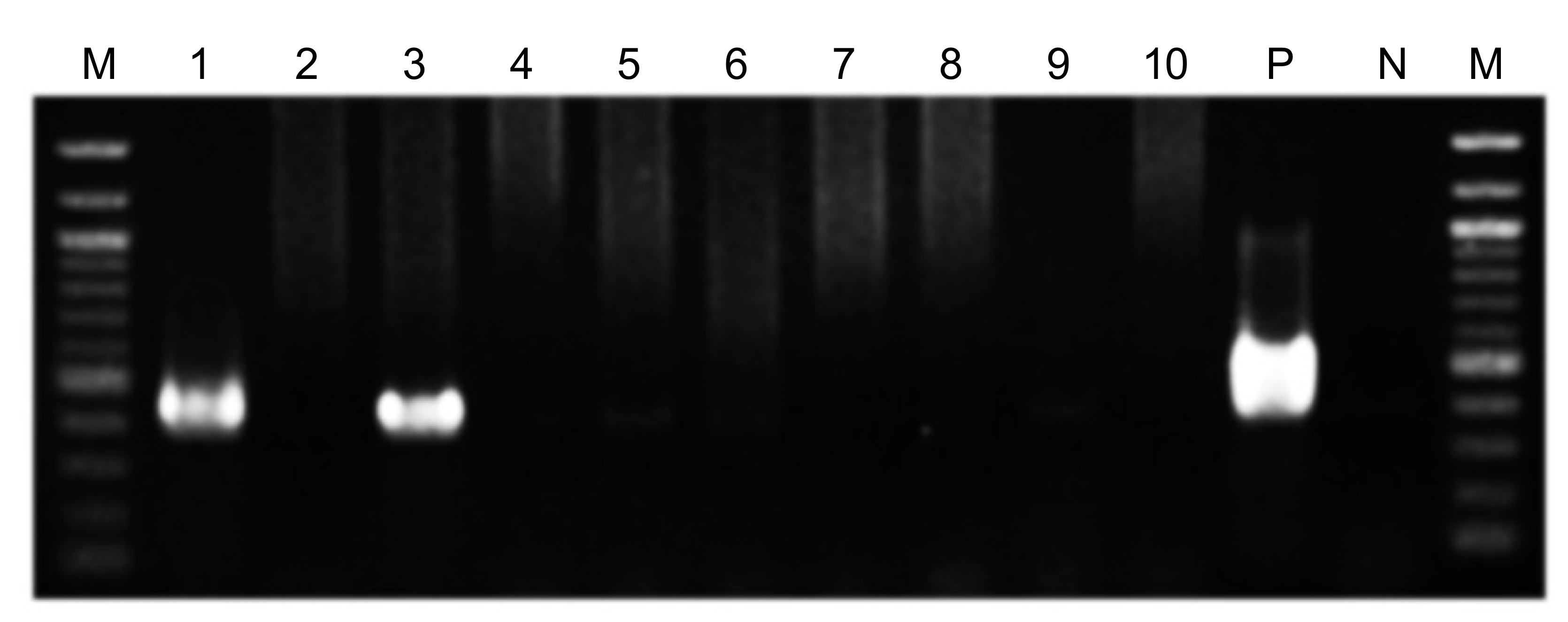
2.3. PCR Detection of Bacteria
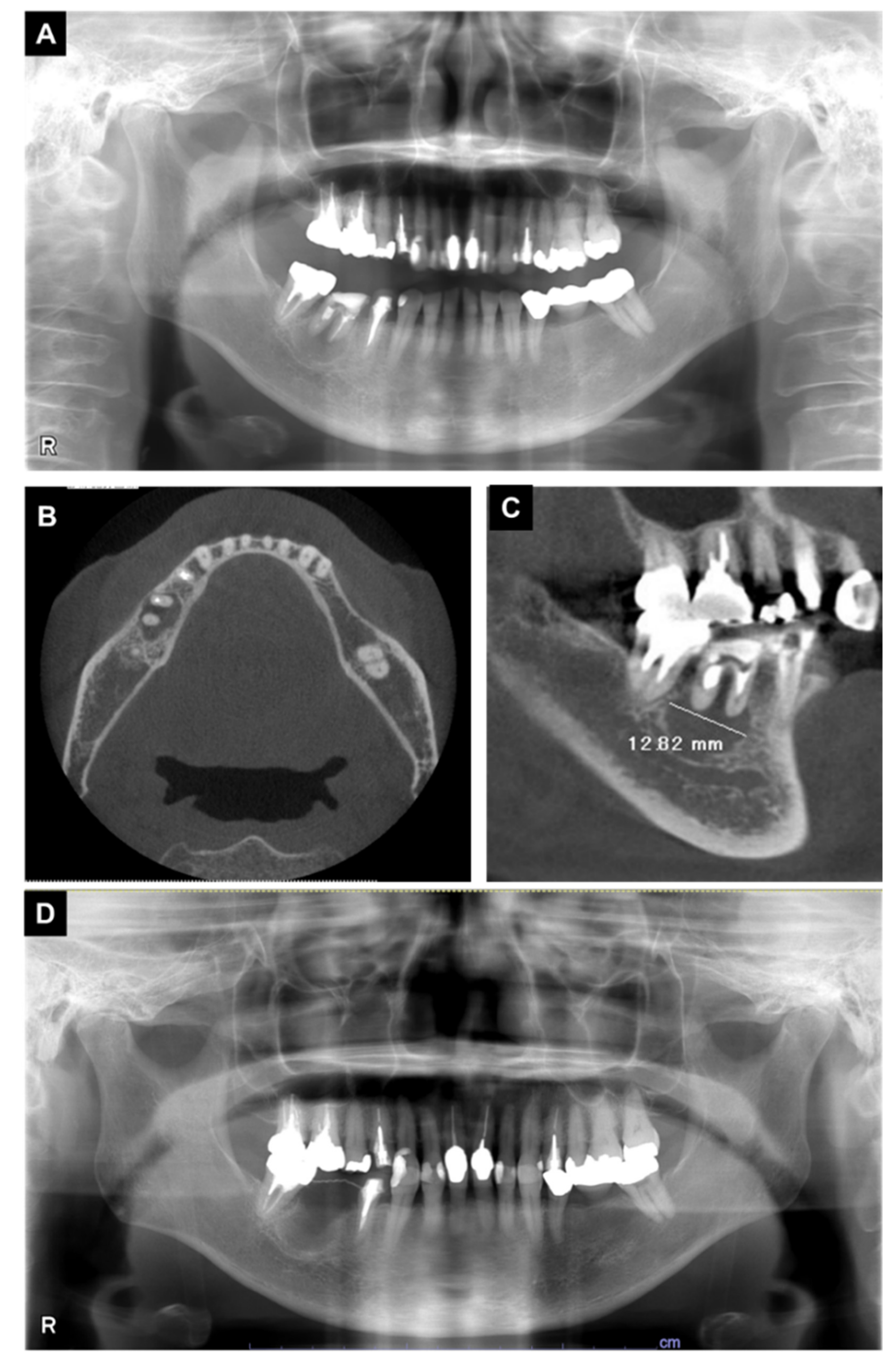
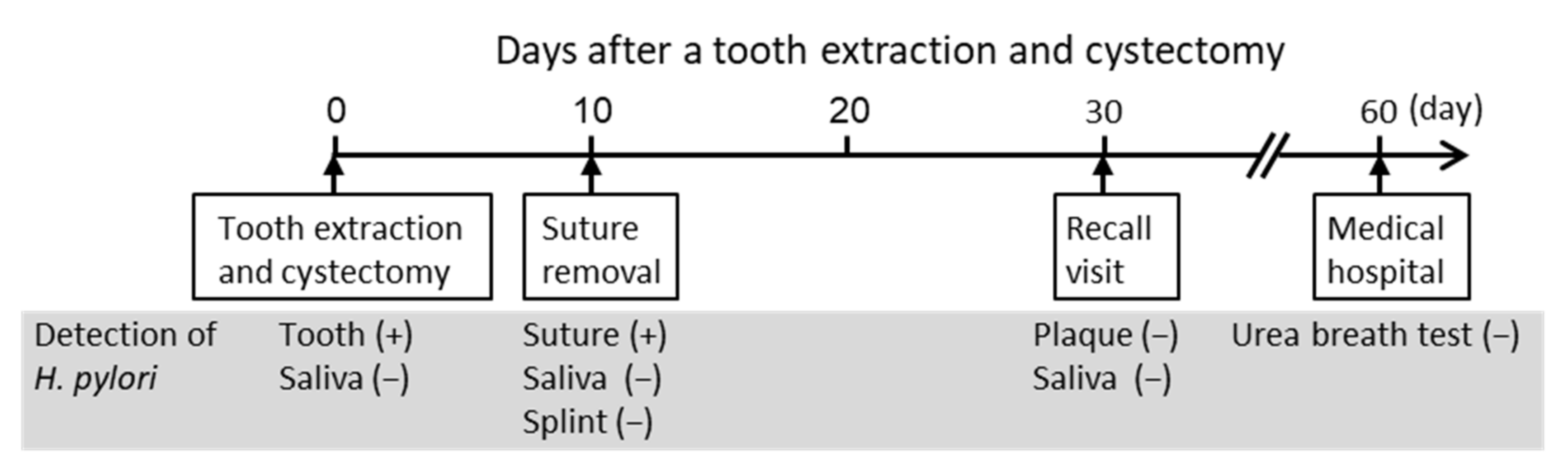
3. Case Report
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rodeghiero, F.; Stasi, R.; Gernsheimer, T.; Michel, M.; Provan, D.; Arnold, D.M.; Bussel, J.B.; Cines, D.B.; Chong, B.H.; Cooper, N.; et al. Standardization of terminology, definitions and outcome criteria in immune thrombocytopenic purpura of adults and children: Report from an international working group. Blood 2009, 113, 2386–2393. [Google Scholar] [CrossRef] [PubMed]
- Swinkels, M.; Rijkers, M.; Voorberg, J.; Vidarsson, G.; Leebeek, F.W.G.; Jansen, A.J.G. Emerging concepts in immune thrombocytopenia. Front. Immunol. 2018, 9, 880. [Google Scholar] [CrossRef] [PubMed]
- Kayal, L.; Jayachandran, S.; Singh, K. Idiopathic thrombocytopenic purpura. Contemp. Clin. Dent. 2014, 5, 410–414. [Google Scholar] [CrossRef] [PubMed]
- Lilleyman, J.S. Intracranial haemorrhage in idiopathic thrombocytopenic purpura. Paediatric Haematology Forum of the British Society for Haematology. Arch. Dis. Child. 1994, 71, 251–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butros, L.J.; Bussel, J.B. Intracranial hemorrhage in immune thrombocytopenic purpura: A retrospective analysis. J. Pediatr. Hematol. Oncol. 2003, 25, 660–664. [Google Scholar] [CrossRef]
- Psaila, B.; Petrovic, A.; Page, L.K.; Menell, J.; Schonholz, M.; Bussel, J.B. Intracranial hemorrhage (ICH) in children with immune thrombocytopenia (ITP): Study of 40 cases. Blood 2009, 114, 4777–4783. [Google Scholar] [CrossRef] [Green Version]
- Bal, M.V.; Koyuncuoglu, C.Z.; Saygun, I. Immune thrombocytopenic purpura presenting as unprovoked gingival hemorrhage: A case report. Open Dent. J. 2014, 8, 164–167. [Google Scholar] [CrossRef]
- Bussel, J.B. The use of intravenous gamma-globulin in idiopathic thrombocytopenic purpura. Clin. Immunol. Immunopathol. 1989, 53, S147–S155. [Google Scholar] [CrossRef]
- Fennerty, M.B. Helicobacter pylori. Arch. Intern. Med. 1994, 154, 721–727. [Google Scholar] [CrossRef]
- Wang, Y.K.; Kuo, F.C.; Liu, C.J.; Wu, M.C.; Shih, H.Y.; Wang, S.S.; Wu, J.Y.; Kuo, C.H.; Huang, Y.K.; Wu, D.C. Diagnosis of Helicobacter pylori infection: Current options and developments. World J. Gastroenterol. 2015, 21, 11221–11235. [Google Scholar] [CrossRef]
- De Korwin, J.D.; Ianiro, G.; Gibiino, G.; Gasbarrini, A. Helicobacter pylori infection and extragastric diseases in 2017. Helicobacter 2017, 22 (Suppl. 1), e12411. [Google Scholar] [CrossRef]
- Goni, E.; Franceschi, F. Helicobacter pylori and extragastric diseases. Helicobacter 2016, 21 (Suppl 1), 45–48. [Google Scholar] [CrossRef]
- Gasbarrini, A.; Franceschi, F.; Tartaglione, R.; Landolfi, R.; Pola, P.; Gasbarrini, G. Regression of autoimmune thrombocytopenia after eradication of Helicobacter pylori. Lancet 1998, 352, 878. [Google Scholar] [CrossRef]
- Hwang, J.J.; Lee, D.H.; Yoon, H.; Shin, C.M.; Park, Y.S.; Kim, N. The effects of Helicobacter pylori eradication therapy for chronic idiopathic thrombocytopenic purpura. Gut. Liver 2016, 10, 356–361. [Google Scholar] [CrossRef] [PubMed]
- Amiri, M. Impact of Helicobacter pylori eradication therapy on platelet counts in patients with chronic idiopathic thrombocytopenic purpura. Glob. J. Health Sci. 2015, 8, 35–40. [Google Scholar] [CrossRef] [Green Version]
- Stasi, R.; Provan, D. Helicobacter pylori and chronic ITP. Hematol. Am. Soc. Hematol. Educ. Program 2008, 2008, 206–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krasteva, A.; Panov, V.; Krasteva, A.; Kisselova, A. Oral cavity and systemic diseases—Helicobacter pylori and dentistry. Biotechnol. Biotechnol. Equip. 2011, 25, 2447–2451. [Google Scholar] [CrossRef] [Green Version]
- Westblom, T.U.; Bhatt, B.D. Diagnosis of Helicobacter pylori infection. Curr. Top. Microbiol. Immunol. 1999, 241, 215–235. [Google Scholar] [CrossRef]
- Silva, D.G.; Tinoco, E.M.; Rocha, G.A.; Rocha, A.M.; Guerra, J.B.; Saraiva, I.E.; Queiroz, D.M. Helicobacter pylori transiently in the mouth may participate in the transmission of infection. Mem. Inst. Oswaldo. Cruz. 2010, 105, 657–660. [Google Scholar] [CrossRef] [Green Version]
- Ogaya, Y.; Nomura, R.; Watanabe, Y.; Nakano, K. Detection of Helicobacter pylori DNA in inflamed dental pulp specimens from Japanese children and adolescents. J. Med. Microbiol. 2015, 64, 117–123. [Google Scholar] [CrossRef]
- Nomura, R.; Ogaya, Y.; Matayoshi, S.; Morita, Y.; Nakano, K. Molecular and clinical analyses of Helicobacter pylori colonization in inflamed dental pulp. BMC Oral Health 2018, 18, 64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mapstone, N.P.; Lynch, D.A.; Lewis, F.A.; Axon, A.T.; Tompkins, D.S.; Dixon, M.F.; Quirke, P. Identification of Helicobacter pylori DNA in the mouths and stomachs of patients with gastritis using PCR. J. Clin. Pathol. 1993, 46, 540–543. [Google Scholar] [CrossRef] [PubMed]
- Miyabayashi, H.; Furihata, K.; Shimizu, T.; Ueno, I.; Akamatsu, T. Influence of oral Helicobacter pylori on the success of eradication therapy against gastric Helicobacter pylori. Helicobacter 2000, 5, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Chi, D.S.; Laffan, J.J.; Li, C.; Ferguson, D.A., Jr.; Litchfield, P.; Thomas, E. Comparison of cytotoxin genotypes of Helicobacter pylori in stomach and saliva. Dig. Dis. Sci. 2002, 47, 1850–1856. [Google Scholar] [CrossRef]
- Park, C.Y.; Kwak, M.; Gutierrez, O.; Graham, D.Y.; Yamaoka, Y. Comparison of genotyping Helicobacter pylori directly from biopsy specimens and genotyping from bacterial cultures. J. Clin. Microbiol. 2003, 41, 3336–3338. [Google Scholar] [CrossRef] [Green Version]
- Smith, S.I.; Oyedeji, K.S.; Arigbabu, A.O.; Cantet, F.; Megraud, F.; Ojo, O.O.; Uwaifo, A.O.; Otegbayo, J.A.; Ola, S.O.; Coker, A.O. Comparison of three PCR methods for detection of Helicobacter pylori DNA and detection of cagA gene in gastric biopsy specimens. World J. Gastroenterol. 2004, 10, 1958–1960. [Google Scholar] [CrossRef]
- Nakano, K.; Inaba, H.; Nomura, R.; Nemoto, H.; Takeda, M.; Yoshioka, H.; Matsue, H.; Takahashi, T.; Taniguchi, K.; Amano, A.; et al. Detection of cariogenic Streptococcus mutans in extirpated heart valve and atheromatous plaque specimens. J. Clin. Microbiol. 2006, 44, 3313–3317. [Google Scholar] [CrossRef] [Green Version]
- Goodwin, C.S.; Mendall, M.M.; Northfield, T.C. Helicobacter pylori infection. Lancet 1997, 349, 265–269. [Google Scholar] [CrossRef]
- Hamada, M.; Nomura, R.; Ogaya, Y.; Matayoshi, S.; Kadota, T.; Morita, Y.; Uzawa, N.; Nakano, K. Potential involvement of Helicobacter pylori from oral specimens in overweight body-mass index. Sci. Rep. 2019, 9, 4845. [Google Scholar] [CrossRef] [Green Version]
- Kadota, T.; Ogaya, Y.; Hatakeyama, R.; Nomura, R.; Nakano, K. Comparison of oral flora before and after triple therapy for Helicobacter pylori eradication in patient with gastric disease. Odontology 2019, 107, 261–267. [Google Scholar] [CrossRef]
- Iwai, K.; Watanabe, I.; Yamamoto, T.; Kuriyama, N.; Matsui, D.; Nomura, R.; Ogaya, Y.; Oseko, F.; Adachi, K.; Takizawa, S.; et al. Association between Helicobacter pylori infection and dental pulp reservoirs in Japanese adults. BMC Oral. Health 2019, 19, 267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitsuhata, C.; Kado, N.; Hamada, M.; Nomura, R.; Kozai, K. Characterization of the unique oral microbiome of children with Down syndrome. Sci. Rep. 2022, 12, 14150. [Google Scholar] [CrossRef] [PubMed]
- Asao, Y.; Iwamoto, Y.; Mitsuhata, C.; Naito, M.; Kozai, K. Three-year survey of oral hygiene conditions of Cambodian public primary school children. J. Oral Sci. 2022, 64, 208–211. [Google Scholar] [CrossRef] [PubMed]
- Asao, Y.; Iwamoto, Y.; Chea, C.; Chher, T.; Mitsuhata, C.; Naito, M.; Kozai, K. The effect of improving oral health literacy among teachers on the oral health condition of primary schoolchildren in Cambodia. Eur. J. Paediatr. Dent. 2022, in press. [Google Scholar]
- Lauritano, D.; Cura, F.; Candotto, V.; Gaudio, R.M.; Mucchi, D.; Carinci, F. Periodontal pockets as a reservoir of Helicobacter pylori causing relapse of gastric ulcer: A review of the literature. J. Biol. Regul. Homeost. Agents 2015, 29, 123–126. [Google Scholar]
- Tongtawee, T.; Wattanawongdon, W.; Simawaranon, T. Effects of periodontal therapy on eradication and recurrence of Helicobacter pylori infection after successful treatment. J. Int. Med. Res. 2019, 47, 875–883. [Google Scholar] [CrossRef] [Green Version]
- Kadota, T.; Hamada, M.; Nomura, R.; Ogaya, Y.; Okawa, R.; Uzawa, N.; Nakano, K. Distribution of Helicobacter pylori and periodontopathic bacterial species in the oral cavity. Biomedicines 2020, 8, 161. [Google Scholar] [CrossRef]
- Payão, S.L.; Rasmussen, L.T. Helicobacter pylori and its reservoirs: A correlation with the gastric infection. World. J. Gastrointest. Pharmacol. Ther. 2016, 7, 126–132. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Primer | Sequence (5′–3′) | Size (bp) | References |
|---|---|---|---|
| First step PCR | |||
| ureA-aF | ATG AAA CTC ACC CCA AAA GA | 488 | [21] |
| ureA-bR | CCG AAA GTT TTT TCT CTG TCA AAG TCT A | ||
| Second step PCR | |||
| ureA-bF | AAA CGC AAA GAA AAA GGC ATT AA | 383 | [21] |
| ureA-aR | TTC ACT TCA AAG AAA TGG AAG TGT GA |
| Item | Abbreviation | Value | Standard Value |
|---|---|---|---|
| Red blood cell count | RBC | 4.5 × 106/μL | 3.8–4.8 × 106/μL |
| White blood cell count | WBC | 4.1 × 103/μL | 4.0–9.0 × 103/μL |
| Platelet count | Plt | 36 × 103/μL | 130–400 × 103/μL |
| Hemoglobin | Hb | 13.1 g/dL | 12.0–16.0 g/dL |
| Activated partial thromboplastin time | APTT | 28.6 s | 22.0–39.0 s |
| Prothrombin time | PT (s) | 12.7 s | 10.0–13.0 s |
| Prothrombin time activity | PT (%) | 89.10% | 80.0–120.0% |
| Prothrombin time-international normalized ratio | PT-INR | 1.1 | 1.0 ± 0.15 |
| Study No. | Oral Specimen | Number of Subjects (Age) | History of Gastrointestinal Disease | Detection Rates of H. pylori | References |
|---|---|---|---|---|---|
| 1 | Inflamed dental pulp | n = 131 (1–19 years) | Unknown | 38.90% | [21] |
| 2 | Dental plaque (Extracted tooth) | n = 87 | Digestive diseases | 9.20% | [29] |
| Saliva | (20–83 years; | (n = 16) | 14.90% | ||
| mean 45.6 years) | |||||
| 3 | Dental pulp | n = 192 | Urine antibody test positive (n = 25) | 12.00% | [31] |
| Dental plaque | (mean 58.6 years) | 1.00% | |||
| Saliva | 0% | ||||
| 4 | Dental plaque | n = 1 (29 years) | Stomachache and Urine antibody test positive | 100% | [30] |
| Saliva | 100% | ||||
| 5 | Dental pulp | n = 39 (16–70 years; | Previous H. pylori infection in gastric tissue (n = 4) | 2.60% | [37] |
| Dental plaque (Extracted tooth) | mean 35.3 years) | 17.90% | |||
| Saliva | 5.10% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hamada, M.; Nomura, R.; Matayoshi, S.; Ogaya, Y.; Kameyama, H.; Uzawa, N.; Nakano, K. Detection of Helicobacter pylori from Extracted Teeth of a Patient with Idiopathic Thrombocytopenic Purpura. Microorganisms 2022, 10, 2285. https://doi.org/10.3390/microorganisms10112285
Hamada M, Nomura R, Matayoshi S, Ogaya Y, Kameyama H, Uzawa N, Nakano K. Detection of Helicobacter pylori from Extracted Teeth of a Patient with Idiopathic Thrombocytopenic Purpura. Microorganisms. 2022; 10(11):2285. https://doi.org/10.3390/microorganisms10112285
Chicago/Turabian StyleHamada, Masakazu, Ryota Nomura, Saaya Matayoshi, Yuko Ogaya, Hiroyasu Kameyama, Narikazu Uzawa, and Kazuhiko Nakano. 2022. "Detection of Helicobacter pylori from Extracted Teeth of a Patient with Idiopathic Thrombocytopenic Purpura" Microorganisms 10, no. 11: 2285. https://doi.org/10.3390/microorganisms10112285