
High Procalcitonin, C-Reactive Protein, and α-1 Acid Glycoprotein Levels in Whole Blood Samples Could Help Rapid Discrimination of Active Tuberculosis from Latent Tuberculosis Infection and Healthy Individuals

Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Samples
2.2. Whole Blood Collection and Serum Preparation
2.3. Analysis of Serum Acute Phase Protein Markers
2.4. Statistical Analysis
3. Results
3.1. Quantitative APP Marker Analysis Results for the Active TB, LTBI, and Healthy Individuals
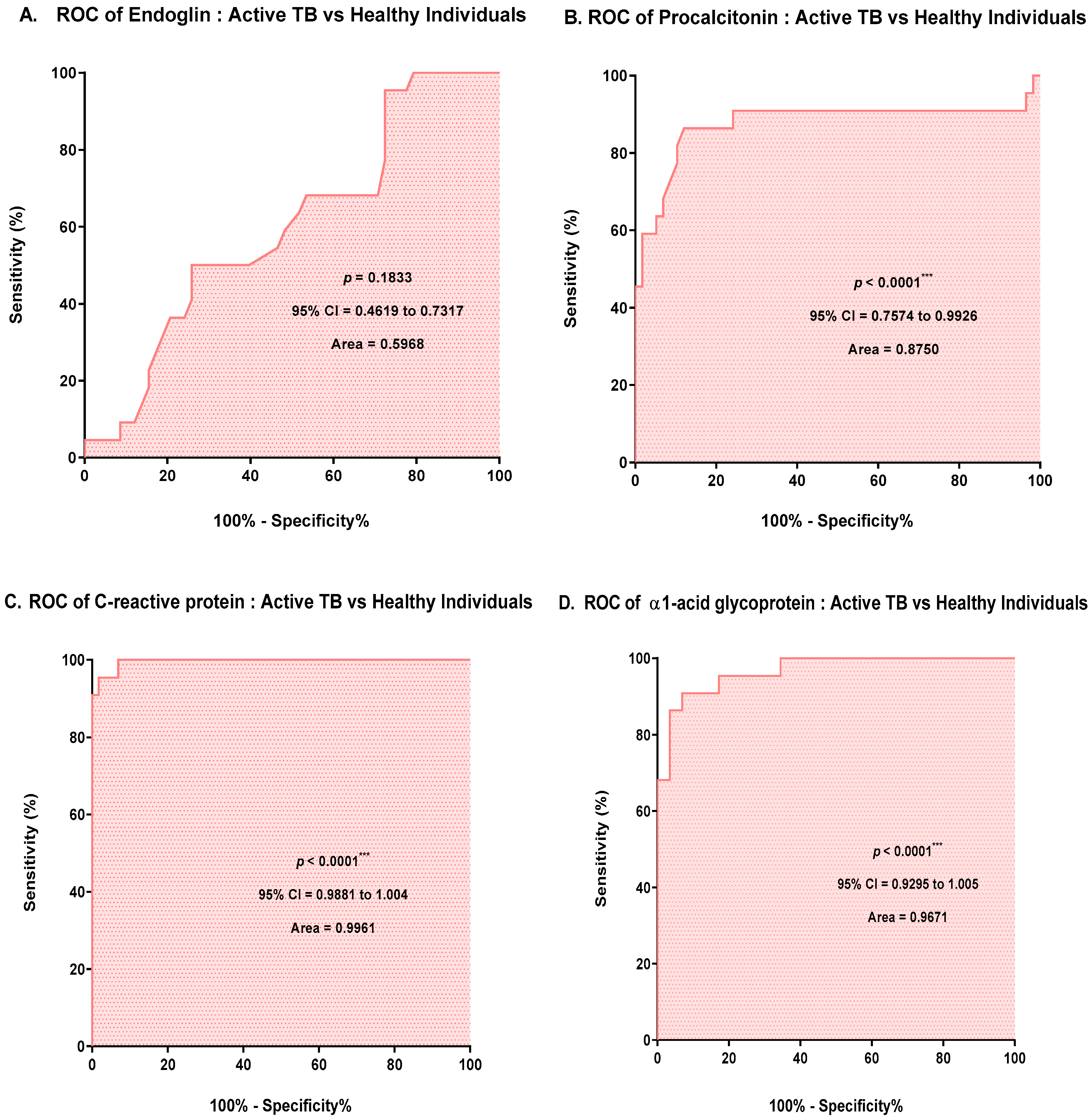
3.2. ROC Curve Analysis Based on the Results for APPs
3.3. Diagnostic Performance of the Quantitative APP Markers
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Zambuzi, F.A.; Cardoso-Silva, P.M.; Espindola, M.S.; Soares, L.S.; Galvao-Lima, L.J.; Brauer, V.S.; Gomes, M.S.; Amaral, L.R.; Schaller, M.; Bollela, V.R.; et al. Identification of promising plasma immune biomarkers to differentiate active pulmonary tuberculosis. Cytokine 2016, 88, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Ren, N.; JinLi, J.; Chen, Y.; Zhou, X.; Wang, J.; Ge, P.; Khan, F.A.; Zhang, L.; Hu, C.; Robertson, I.D.; et al. Identification of new diagnostic biomarkers for Mycobacterium tuberculosis and the potential application in the serodiagnosis of human tuberculosis. Microb. Biotechnol. 2018, 11, 893–904. [Google Scholar] [CrossRef] [PubMed]
- Cho, K.S. Tuberculosis control in the Republic of Korea. Epidemiol. Health 2018, 40, e2018036. [Google Scholar] [CrossRef] [PubMed]
- Cao, S.H.; Chen, Y.Q.; Sun, Y.; Liu, Y.; Zheng, S.H.; Zhang, Z.G.; Li, C.Y. Screening of Serum Biomarkers for Distinguishing between Latent and Active Tuberculosis Using Proteome Microarray. Biomed. Environ. Sci. 2018, 31, 515–526. [Google Scholar] [CrossRef]
- Salgame, P.; Geadas, C.; Collins, L.; Jones-Lopez, E.; Ellner, J.J. Latent tuberculosis infection—Revisiting and revising concepts. Tuberculosis 2015, 95, 373–384. [Google Scholar] [CrossRef]
- Campbell, J.R.; Krot, J.; Elwood, K.; Cook, V.; Marra, F. A systematic review on TST and IGRA tests used for diagnosis of LTBI in immigrants. Mol. Diagn. Ther. 2015, 19, 9–24. [Google Scholar] [CrossRef]
- Mamishi, S.; Mahmoudi, S.; Banar, M.; Hosseinpour Sadeghi, R.; Marjani, M.; Pourakbari, B. Diagnostic accuracy of interferon (IFN)-gamma inducible protein 10 (IP-10) as a biomarker for the discrimination of active and latent tuberculosis. Mol. Biol. Rep. 2019, 46, 6263–6269. [Google Scholar] [CrossRef]
- Lee, S.W.; Wu, L.S.; Huang, G.M.; Huang, K.Y.; Lee, T.Y.; Weng, J.T. Gene expression profiling identifies candidate biomarkers for active and latent tuberculosis. BMC Bioinform. 2016, 17 (Suppl. 1), 3. [Google Scholar] [CrossRef]
- Won, E.J.; Choi, J.H.; Cho, Y.N.; Jin, H.M.; Kee, H.J.; Park, Y.W.; Kwon, Y.S.; Kee, S.J. Biomarkers for discrimination between latent tuberculosis infection and active tuberculosis disease. J. Infect. 2017, 74, 281–293. [Google Scholar] [CrossRef]
- Sun, T.; Wu, B.; Wang, J.; Yuan, T.; Huang, H.; Xu, D.; Deng, S. Evaluation of the Diagnostic Efficacy of Monocyte Parameters and MCP-1 to Distinguishing Active Tuberculosis from Latent Tuberculosis. Clin. Lab. 2019, 65. [Google Scholar] [CrossRef]
- Liu, J.; Jiang, T.; Jiang, F.; Xu, D.; Wei, L.; Wang, C.; Chen, Z.; Zhang, X.; Li, J. Comparative proteomic analysis of serum diagnosis patterns of sputum smear-positive pulmonary tuberculosis based on magnetic bead separation and mass spectrometry analysis. Int. J. Clin. Exp. Med. 2015, 8, 2077–2085. [Google Scholar] [PubMed]
- Xu, D.; Li, Y.; Li, X.; Wei, L.L.; Pan, Z.; Jiang, T.T.; Chen, Z.L.; Wang, C.; Cao, W.M.; Zhang, X.; et al. Serum protein S100A9, SOD3, and MMP9 as new diagnostic biomarkers for pulmonary tuberculosis by iTRAQ-coupled two-dimensional LC-MS/MS. Proteomics 2015, 15, 58–67. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; Pan, L.; Jia, H.; Zhang, Z.; Gao, M.; Huang, M.; Wang, J.; Sun, Q.; Wei, R.; Du, B.; et al. Label-Free Quantitative Proteomics Identifies Novel Plasma Biomarkers for Distinguishing Pulmonary Tuberculosis and Latent Infection. Front. Microbiol. 2018, 9, 1267. [Google Scholar] [CrossRef]
- Santos, V.S.; Goletti, D.; Kontogianni, K.; Adams, E.R.; Molina-Moya, B.; Dominguez, J.; Crudu, V.; Martins-Filho, P.R.S.; Ruhwald, M.; Lawson, L.; et al. Acute phase proteins and IP-10 as triage tests for the diagnosis of tuberculosis: Systematic review and meta-analysis. Clin. Microbiol. Infect. 2019, 25, 169–177. [Google Scholar] [CrossRef]
- Stavrum, R.; PrayGod, G.; Range, N.; Faurholt-Jepsen, D.; Jeremiah, K.; Faurholt-Jepsen, M.; Krarup, H.; Aabye, M.G.; Changalucha, J.; Friis, H.; et al. Increased level of acute phase reactants in patients infected with modern Mycobacterium tuberculosis genotypes in Mwanza, Tanzania. BMC Infect. Dis. 2014, 14, 309. [Google Scholar] [CrossRef] [PubMed]
- Jayakumar, A.; Vittinghoff, E.; Segal, M.R.; MacKenzie, W.R.; Johnson, J.L.; Gitta, P.; Saukkonen, J.; Anderson, J.; Weiner, M.; Engle, M.; et al. Serum biomarkers of treatment response within a randomized clinical trial for pulmonary tuberculosis. Tuberculosis 2015, 95, 415–420. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Remolina, L.; Ollauri-Ibanez, C.; Perez-Roque, L.; Nunez-Gomez, E.; Perez-Barriocanal, F.; Lopez-Novoa, J.M.; Pericacho, M.; Rodriguez-Barbero, A. Circulating soluble endoglin modifies the inflammatory response in mice. PLoS ONE 2017, 12, e0188204. [Google Scholar] [CrossRef]
- Chen, C.; Yan, T.; Liu, L.; Wang, J.; Jin, Q. Identification of a Novel Serum Biomarker for Tuberculosis Infection in Chinese HIV Patients by iTRAQ-Based Quantitative Proteomics. Front. Microbiol. 2018, 9, 330. [Google Scholar] [CrossRef]
- Yoon, C.; Chaisson, L.H.; Patel, S.M.; Allen, I.E.; Drain, P.K.; Wilson, D.; Cattamanchi, A. Diagnostic accuracy of C-reactive protein for active pulmonary tuberculosis: A meta-analysis. Int. J. Tuberc. Lung Dis. 2017, 21, 1013–1019. [Google Scholar] [CrossRef]
- Martinez Cordero, E.; Gonzalez, M.M.; Aguilar, L.D.; Orozco, E.H.; Hernandez Pando, R. Alpha-1-acid glycoprotein, its local production and immunopathological participation in experimental pulmonary tuberculosis. Tuberculosis 2008, 88, 203–211. [Google Scholar] [CrossRef]
- Ding, R.D.; Zhang, H.J. Effect of linezolid on serum PCT, ESR, and CRP in patients with pulmonary tuberculosis and pneumonia. Medicine 2018, 97, e12177. [Google Scholar] [CrossRef] [PubMed]
- Shim, T.S. Diagnosis and Treatment of Latent Tuberculosis Infection. Korean J. Med. 2012, 82, 284–290. [Google Scholar] [CrossRef]
- Lim, H.-J.; Lee, J.H. New Diagnostic Methods for Tuberculosis. Korean J. Med. 2012, 82, 263–268. [Google Scholar] [CrossRef]
- Marais, B.J.; Brittle, W.; Painczyk, K.; Hesseling, A.C.; Beyers, N.; Wasserman, E.; van Soolingen, D.; Warren, R.M. Use of light-emitting diode fluorescence microscopy to detect acid-fast bacilli in sputum. Clin. Infect. Dis. 2008, 47, 203–207. [Google Scholar] [CrossRef] [PubMed]
- Shi, T.; Huang, L.; Zhou, Y.; Tian, J. Role of GBP1 in innate immunity and potential as a tuberculosis biomarker. Sci. Rep. 2022, 12, 11097. [Google Scholar] [CrossRef]
- WHO. Global Tuberculosis Report 2021; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Sharma, S.K.; Vashishtha, R.; Chauhan, L.S.; Sreenivas, V.; Seth, D. Comparison of TST and IGRA in Diagnosis of Latent Tuberculosis Infection in a High TB-Burden Setting. PLoS ONE 2017, 12, e0169539. [Google Scholar] [CrossRef]
- Schoonderwoerd, M.J.A.; Goumans, M.T.H.; Hawinkels, L. Endoglin: Beyond the Endothelium. Biomolecules 2020, 10, 289. [Google Scholar] [CrossRef]
- Kerbel, R.S. Tumor angiogenesis. N. Engl. J. Med. 2008, 358, 2039–2049. [Google Scholar] [CrossRef]
- Mossenta, M.; Busato, D.; Baboci, L.; Cintio, F.D.; Toffoli, G.; Bo, M.D. New Insight into Therapies Targeting Angiogenesis in Hepatocellular Carcinoma. Cancers 2019, 11, 1086. [Google Scholar] [CrossRef]
- Jeng, K.S.; Sheen, I.S.; Lin, S.S.; Leu, C.M.; Chang, C.F. The Role of Endoglin in Hepatocellular Carcinoma. Int. J. Mol. Sci. 2021, 22, 3208. [Google Scholar] [CrossRef]
- Paauwe, M.; Schoonderwoerd, M.J.A.; Helderman, R.; Harryvan, T.J.; Groenewoud, A.; van Pelt, G.W.; Bor, R.; Hemmer, D.M.; Versteeg, H.H.; Snaar-Jagalska, B.E.; et al. Endoglin Expression on Cancer-Associated Fibroblasts Regulates Invasion and Stimulates Colorectal Cancer Metastasis. Clin. Cancer Res. 2018, 24, 6331–6344. [Google Scholar] [CrossRef] [PubMed]
- Zsila, F.; Bosze, S.; Beke-Somfai, T. Interaction of antitubercular drug candidates with alpha1-acid glycoprotein produced in pulmonary granulomas. Int. J. Biol. Macromol. 2020, 147, 1318–1327. [Google Scholar] [CrossRef] [PubMed]
- Baumann, H.; Gauldie, J. The acute phase response. Immunol. Today 1994, 15, 74–80. [Google Scholar] [CrossRef]
- Talks, B.J.; Bradwell, S.B.; Delamere, J.; Rayner, W.; Clarke, A.; Lewis, C.T.; Thomas, O.D.; Bradwell, A.R. Urinary Alpha-1-Acid Glycoprotein Is a Sensitive Marker of Glomerular Protein Leakage at Altitude. High Alt. Med. Biol. 2018, 19, 295–298. [Google Scholar] [CrossRef]
- Davies, J. Procalcitonin. J. Clin. Pathol. 2015, 68, 675–679. [Google Scholar] [CrossRef]
- Li, B.; Zhao, X.; Li, S. Serum Procalcitonin Level and Mortality Risk in Critically ill Patients with Ventilator-Associated Pneumonia. Cell Physiol. Biochem. 2015, 37, 1967–1972. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Demographic and Clinical Characteristics | Active TB | LTBI | Healthy Individuals |
|---|---|---|---|
| Total number (n = 129) | 22 | 29 | 58 |
| Median age (range), years | 55.2 (23–89) | 44.6 (21–70) | 33.2 (22–61) |
| Gender, male/female | 15/7 | 6/23 | 12/46 |
| AFB stain results | |||
| + positive, n (%) | 2 (9.1) | NA | NA |
| ++ positive, n (%) | 4 (18.2) | NA | NA |
| +++ positive, n (%) | 4 (18.2) | NA | NA |
| ++++ positive, n (%) | 4 (18.2) | NA | NA |
| Negative | 8 (36.4) | NA | NA |
| AFB culture results | |||
| Positive, n (%) | 19 (86.4) | NA | NA |
| Negative, n (%) | 3 (13.6) | NA | NA |
| MTB-PCR results | |||
| Positive, n (%) | 21 (95.5) | NA | NA |
| Negative, n (%) | 1 (4.5) | NA | NA |
| CXR | |||
| Positive, n (%) | 22 (100.0) | 4 (13.8) | 0 (0.0) |
| Negative, n (%) | 0 (0.0) | 25 (86.2) | 58 (100.0) |
| IGRA test results | |||
| Positive, n (%) | NA | 29 (100.0) | 0 (0.0) |
| Negative, n (%) | NA | 0 (0.0) | 58 (100.0) |
| Acute-Phase Protein Markers | Active TB, Mean Level ± SD | LTBI, Mean Level ± SD | Healthy Individuals, Mean Level ± SD |
|---|---|---|---|
| Endoglin (pg/mL) | 1267.88 ± 214.47 | 1209 ± 252.60 | 1371.81 ± 303.69 |
| Procalcitonin (pg/mL) | 44.11 ± 29.21 | 22.68 ± 11.67 | 18.15 ± 4.58 |
| C-reactive protein (ng/mL) | 343,491.91 ± 362,153.63 | 2358.38 ± 1213.21 | 3375.52 ± 1833.75 |
| α1-acid glycoprotein (µg/mL) | 6886.68 ± 2438.14 | 3749.57 ± 1369.43 | 2969.90 ± 795.71 |
| Acute-Phase Protein Markers | Active TB vs. LTBI | LTBI vs. Healthy Control | Active TB vs. Healthy Individuals | Active TB vs. LTBI vs. Healthy Individuals |
|---|---|---|---|---|
| Endoglin | 0.3848 | 0.0149 * | 0.1457 | 0.0287 * |
| Procalcitonin | 0.0007 *** | 0.0112 * | <0.0001 *** | <0.0001 *** |
| C-reactive protein | <0.0001 *** | 0.0083 ** | <0.0001 *** | <0.0001 *** |
| α1-acid glycoprotein | < 0.0001 *** | 0.0012 ** | <0.0001 *** | <0.0001 *** |
| Acute-Phase Protein Markers | AUC (95% CI) | Cut-Off Value | Sensitivity (%) (95% CI) | Specificity (%) (95% CI) | p Value |
|---|---|---|---|---|---|
| Endoglin | 0.60 (0.46–0.73) | >1330 ng/mL | 54.55 (32.21–75.61) | 53.45 (39.87–66.66) | 0.1833 |
| Procalcitonin | 0.87 (0.76–0.99) | >23 ng/mL | 86.36 (65.09–97.09) | 87.93 (76.70–95.01) | <0.0001 |
| C-reactive protein | 0.99 (0.99–1.00) | >8853 ng/mL | 95.45 (77.16–99.88) | 98.28 (90.76–99.96) | <0.0001 |
| α-1-acid glycoprotein | 0.98 (0.93–1.00) | >4548 ng/mL | 90.91 (70.84–98.99) | 93.10 (83.27–98.09) | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, Y.-J.; Park, H.; Park, S.-B.; Lee, J.; Hyun, H.; Jung, M.; Lee, E.J.; Je, M.-A.; Kim, J.; Lee, Y.S.; et al. High Procalcitonin, C-Reactive Protein, and α-1 Acid Glycoprotein Levels in Whole Blood Samples Could Help Rapid Discrimination of Active Tuberculosis from Latent Tuberculosis Infection and Healthy Individuals. Microorganisms 2022, 10, 1928. https://doi.org/10.3390/microorganisms10101928
Kang Y-J, Park H, Park S-B, Lee J, Hyun H, Jung M, Lee EJ, Je M-A, Kim J, Lee YS, et al. High Procalcitonin, C-Reactive Protein, and α-1 Acid Glycoprotein Levels in Whole Blood Samples Could Help Rapid Discrimination of Active Tuberculosis from Latent Tuberculosis Infection and Healthy Individuals. Microorganisms. 2022; 10(10):1928. https://doi.org/10.3390/microorganisms10101928
Chicago/Turabian StyleKang, Yun-Jeong, Heechul Park, Sung-Bae Park, Jiyoung Lee, Hyanglan Hyun, Minju Jung, Eun Ju Lee, Min-A Je, Jungho Kim, Yong Sung Lee, and et al. 2022. "High Procalcitonin, C-Reactive Protein, and α-1 Acid Glycoprotein Levels in Whole Blood Samples Could Help Rapid Discrimination of Active Tuberculosis from Latent Tuberculosis Infection and Healthy Individuals" Microorganisms 10, no. 10: 1928. https://doi.org/10.3390/microorganisms10101928