
A Retrospective Assessment of Sputum Samples and Antimicrobial Resistance in COVID-19 Patients

 , , , ,
, , , ,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Considerations
2.2. Inclusion Criteria and Study Variables
2.3. Study Terminology and Sputum Sampling
- Infections diagnosed within 48 h of hospital admission were classified as co-infections. Infections identified after 48 h of admission were classified as superinfections [4,22,23,24]. Biological samples for the diagnosis of co-infection/superinfection in COVID-19 patients were collected after evaluating the following clinical criteria: purulent sputum, persistent fever (>38 °C), deterioration of ventilatory parameters, or hemodynamic instability.
- Laboratory criteria: worsening of leukocytosis or leucopenia, increased procalcitonin, or C-reactive protein.
- Radiological criteria: progression/worsening of the chest radiological pattern, or onset of a pattern characteristic for bacterial pneumonia such as basal consolidation, nodules, cavitation, or pleural effusion.
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Study Cohort
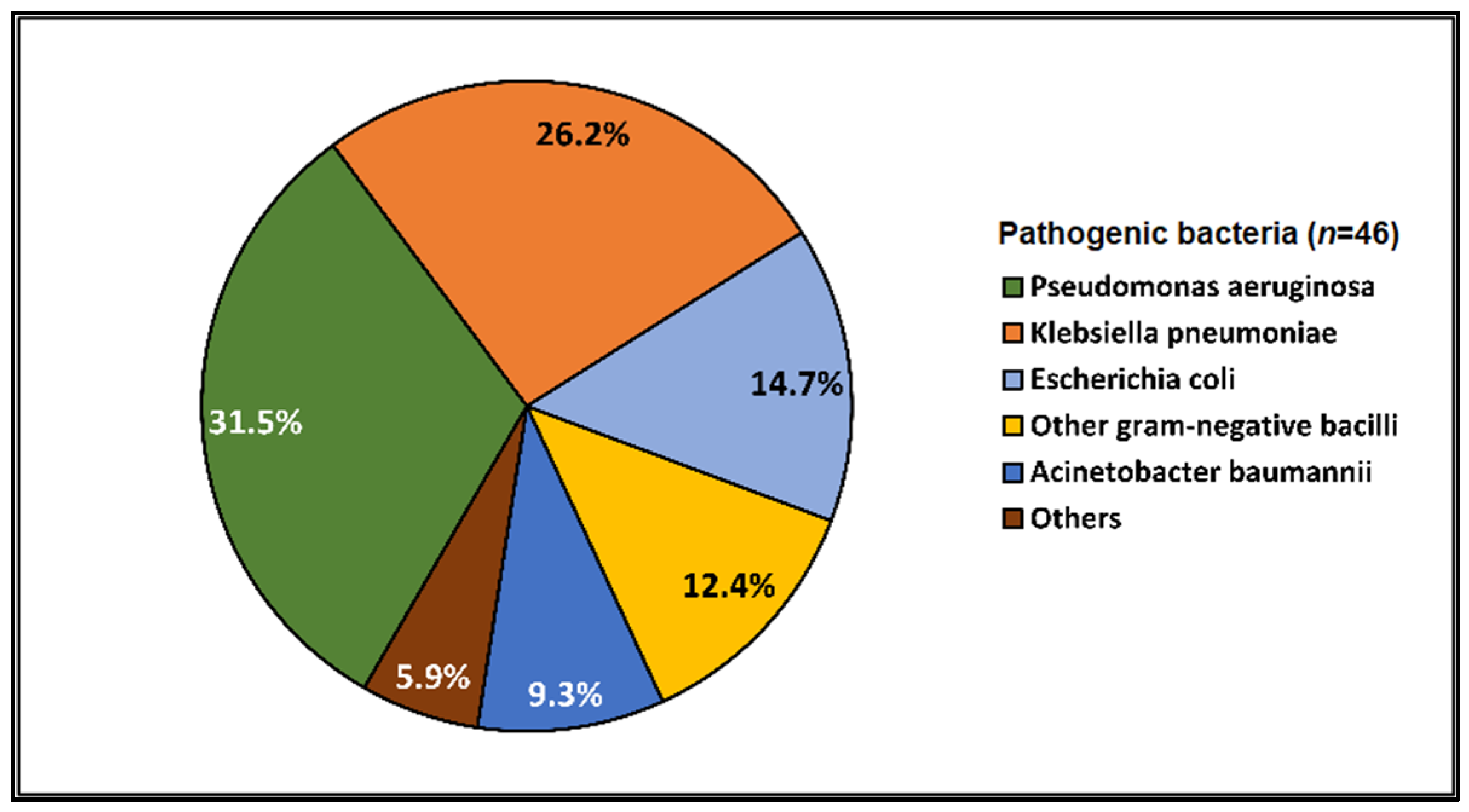
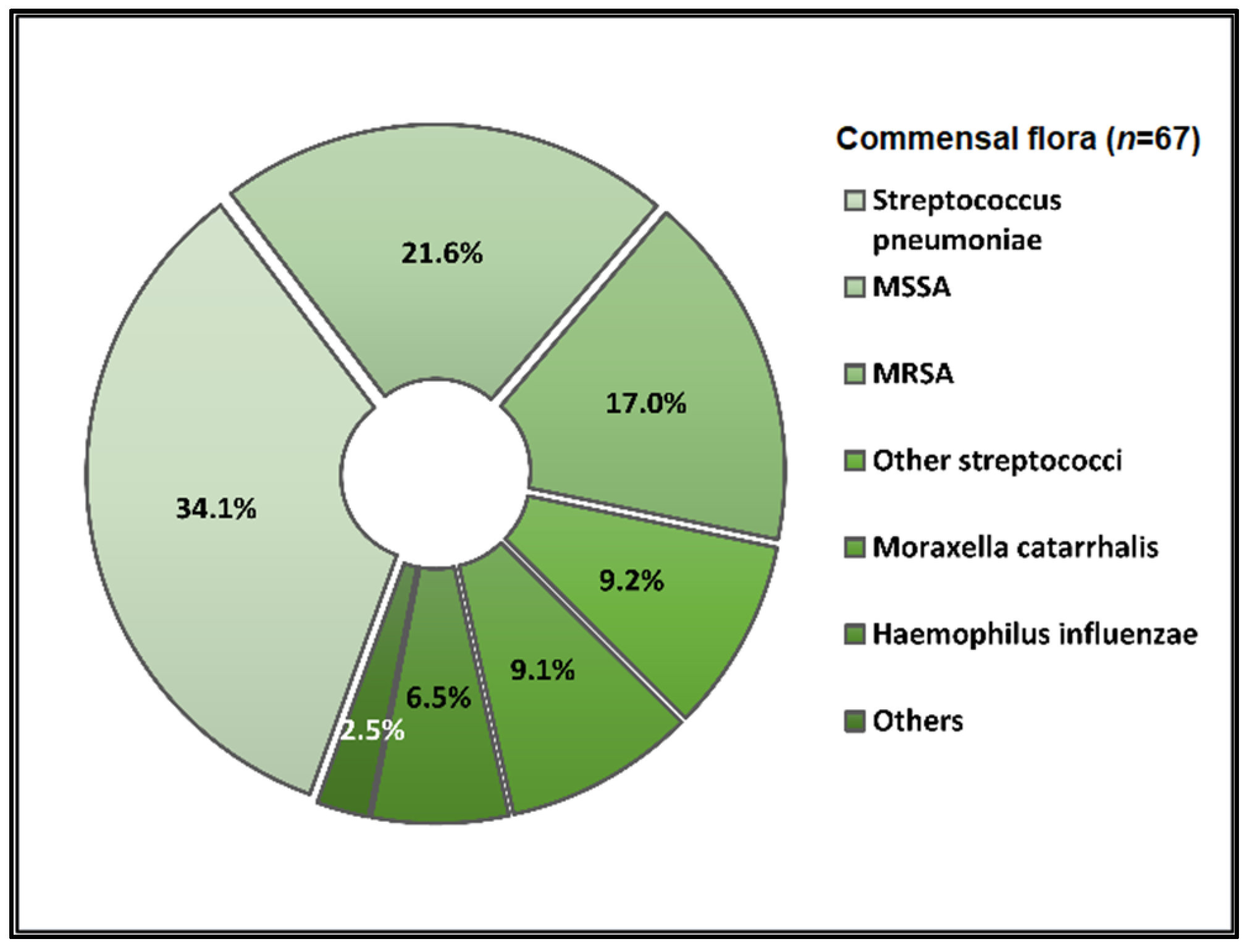
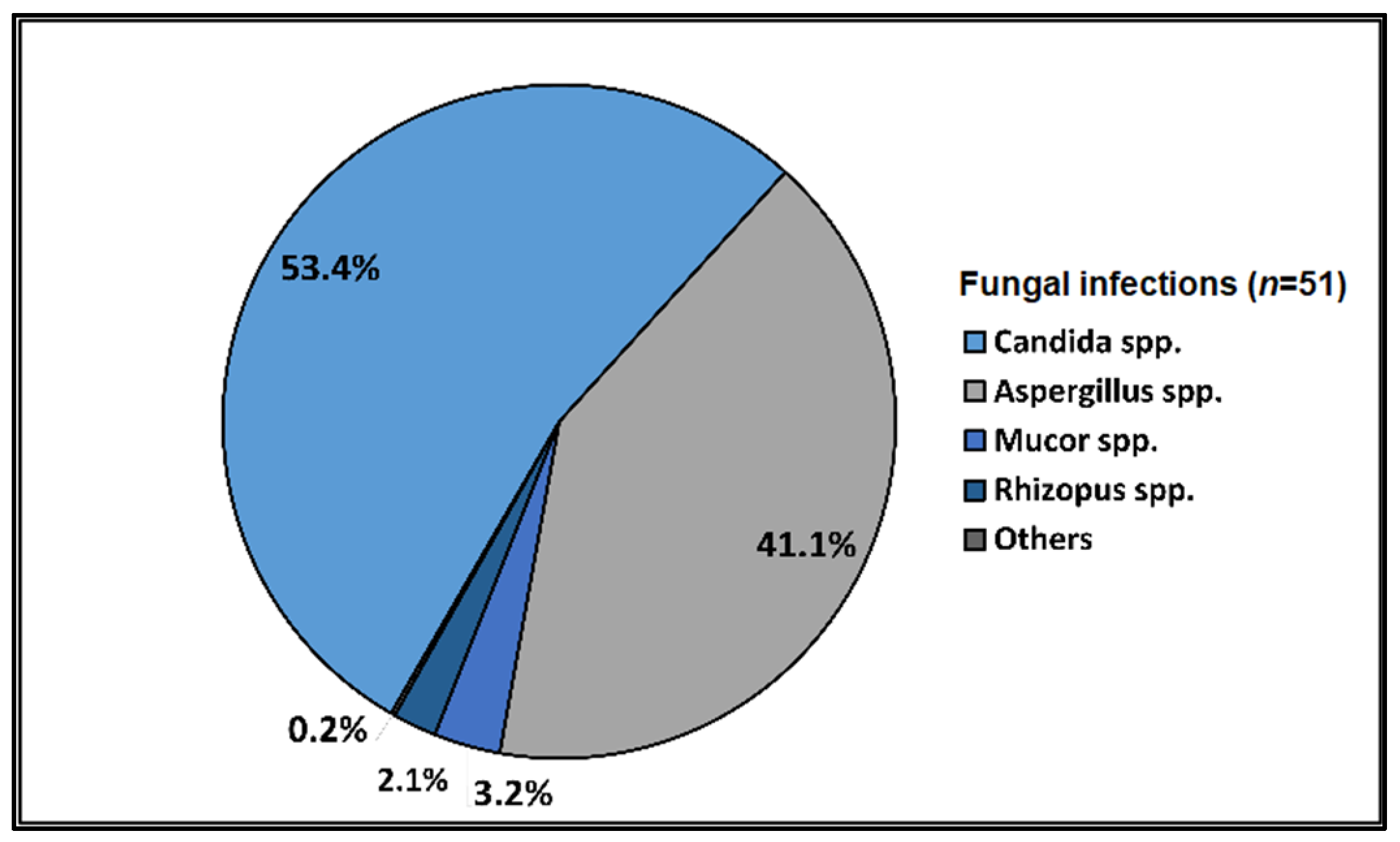
3.2. Microbial Identification
3.3. Biological Findings
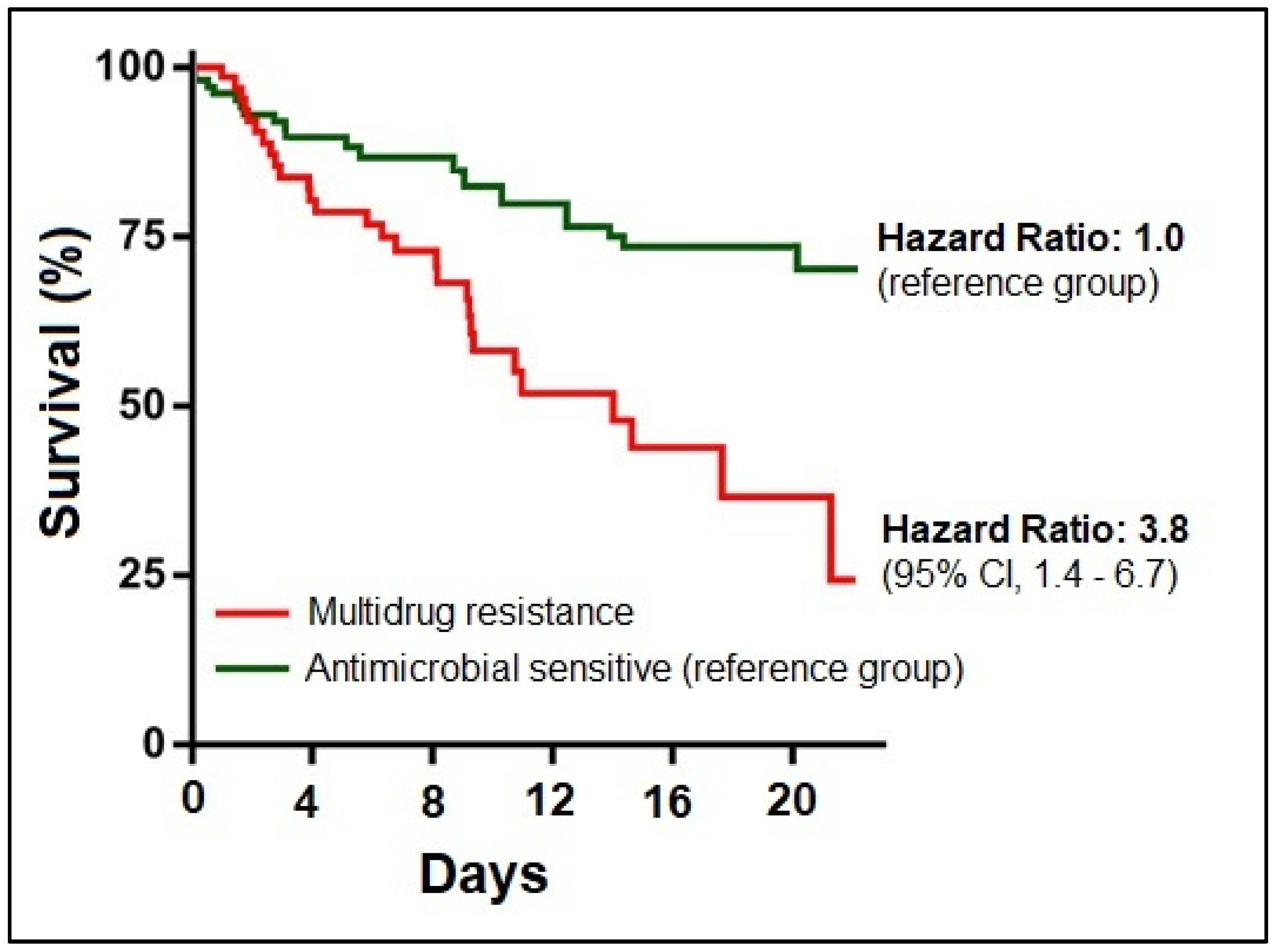
3.4. Outcomes and Predictions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liang, S.T.; Liang, L.T.; Rosen, J.M. COVID-19: A Comparison to the 1918 Influenza and How We Can Defeat It. Postgrad. Med. J. 2021, 97, 273–274. [Google Scholar] [CrossRef]
- Antimicrobial Resistance in the Age of COVID-19. Nat. Microbiol. 2020, 5, 779. [CrossRef] [PubMed]
- Kariyawasam, R.M.; Julien, D.A.; Jelinski, D.C.; Larose, S.L.; Rennert-May, E.; Conly, J.M.; Dingle, T.C.; Chen, J.Z.; Tyrrell, G.J.; Ronksley, P.E.; et al. Antimicrobial Resistance (AMR) in COVID-19 Patients: A Systematic Review and Meta-Analysis (November 2019–June 2021). Antimicrob. Resist. Infect. Control. 2022, 11, 45. [Google Scholar] [CrossRef] [PubMed]
- Rotondo, J.C.; Martini, F.; Maritati, M.; Caselli, E.; Gallenga, C.E.; Guarino, M.; De Giorgio, R.; Mazziotta, C.; Tramarin, M.L.; Badiale, G.; et al. Advanced Molecular and Immunological Diagnostic Methods to Detect SARS-CoV-2 Infection. Microorganisms 2022, 10, 1193. [Google Scholar] [CrossRef] [PubMed]
- Biancolella, M.; Colona, V.L.; Mehrian-Shai, R.; Watt, J.L.; Luzzatto, L.; Novelli, G.; Reichardt, J.K.V. COVID-19 2022 Update: Transition of the Pandemic to the Endemic Phase. Hum. Genom. 2022, 16, 19. [Google Scholar] [CrossRef]
- Grinbaum, R.S.; Kiffer, C.R.V. Bacterial Infections in COVID-19 Patients: A Review. Rev. Assoc. Med. Bras. 2021, 67, 1863–1868. [Google Scholar] [CrossRef]
- Langford, B.J.; So, M.; Simeonova, M.; Leung, V.; Lo, J.; Kan, T.; Raybardhan, S.; Sapin, M.E.; Mponponsuo, K.; Farrell, A.; et al. Antimicrobial Resistance in Patients with COVID-19: A Systematic Review and Meta-Analysis. Lancet Microbe 2023, 4, e179–e191. [Google Scholar] [CrossRef] [PubMed]
- Marinescu, A.R.; Laza, R.; Musta, V.F.; Cut, T.G.; Dumache, R.; Tudor, A.; Porosnicu, M.; Lazureanu, V.E.; Licker, M. Clostridium Difficile and COVID-19: General Data, Ribotype, Clinical Form, Treatment-Our Experience from the Largest Infectious Diseases Hospital in Western Romania. Medicina 2021, 57, 1099. [Google Scholar] [CrossRef] [PubMed]
- Dima, A.; Balaban, D.V.; Jurcut, C.; Berza, I.; Jurcut, R.; Jinga, M. Perceptions of Romanian Physicians on Lockdowns for COVID-19 Prevention. Healthcare 2021, 9, 95. [Google Scholar] [CrossRef]
- Gyselinck, I.; Janssens, W.; Verhamme, P.; Vos, R. Rationale for Azithromycin in COVID-19: An Overview of Existing Evidence. BMJ Open. Respir. Res. 2021, 8, e000806. [Google Scholar] [CrossRef]
- Laza, R.; Dragomir, C.; Musta, V.F.; Lazureanu, V.E.; Nicolescu, N.D.; Marinescu, A.R.; Paczeyka, R.; Porosnicu, T.M.; Bica-Porfir, V.; Laitin, S.M.D.; et al. Analysis of Deaths and Favorable Developments of Patients with SARS-CoV-2 Hospitalized in the Largest Hospital for Infectious Diseases and Pneumo-Phthisiology in the West of the Country. Int. J. Gen. Med. 2022, 15, 3417–3431. [Google Scholar] [CrossRef]
- Ditz, B.; Christenson, S.; Rossen, J.; Brightling, C.; Kerstjens, H.A.M.; van den Berge, M.; Faiz, A. Sputum Microbiome Profiling in COPD: Beyond Singular Pathogen Detection. Thorax 2020, 75, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Joseph, C.; Togawa, Y.; Shindo, N. Bacterial and Viral Infections Associated with Influenza. Influenza Respir. Viruses 2013, 7, 105–113. [Google Scholar] [CrossRef]
- Guarnera, A.; Podda, P.; Santini, E.; Paolantonio, P.; Laghi, A. Differential Diagnoses of COVID-19 Pneumonia: The Current Challenge for the Radiologist—A Pictorial Essay. Insights Imaging 2021, 12, 34. [Google Scholar] [CrossRef]
- Lansbury, L.; Lim, B.; Baskaran, V.; Lim, W.S. Co-Infections in People with COVID-19: A Systematic Review and Meta-Analysis. J. Infect. 2020, 81, 266–275. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239. [Google Scholar] [CrossRef] [PubMed]
- Tudoran, M.; Tudoran, C.; Lazureanu, V.; Marinescu, A.; Pop, G.; Pescariu, A.; Enache, A.; Cut, T. Alterations of Left Ventricular Function Persisting during Post-Acute COVID-19 in Subjects without Previously Diagnosed Cardiovascular Pathology. J. Pers. Med. 2021, 11, 225. [Google Scholar] [CrossRef] [PubMed]
- Santos, A.P.; Gonçalves, L.C.; Oliveira, A.C.C.; Queiroz, P.H.P.; Ito, C.R.M.; Santos, M.O.; Carneiro, L.C. Bacterial Co-Infection in Patients with COVID-19 Hospitalized (ICU and Not ICU): Review and Meta-Analysis. Antibiotics 2022, 11, 894. [Google Scholar] [CrossRef]
- Cut, T.G.; Ciocan, V.; Novacescu, D.; Voicu, A.; Marinescu, A.R.; Lazureanu, V.E.; Muresan, C.O.; Enache, A.; Dumache, R. Autopsy Findings and Inflammatory Markers in SARS-CoV-2: A Single-Center Experience. Int. J. Gen. Med. 2022, 15, 8743–8753. [Google Scholar] [CrossRef]
- Dumache, R.; Enache, A.; Cut, T.; Paul, C.; Mihailescu, A.; Ionescu, A.; Novacescu, D.; Marinescu, A.; Ciocan, V.; Muresan, C.; et al. Deficiency of Vitamin D, a Major Risk Factor for SARS-CoV-2 Severity. Clin. Lab. 2022, 68. [Google Scholar] [CrossRef]
- Ceccarelli, M.; Marino, A.; Pulvirenti, S.; Coco, V.; Busà, B.; Nunnari, G.; Cacopardo, B.S. Bacterial and Fungal Co-Infections and Superinfections in a Cohort of COVID-19 Patients: Real-Life Data from an Italian Third Level Hospital. Infect. Dis. Rep. 2022, 14, 372–382. [Google Scholar] [CrossRef] [PubMed]
- Feldman, C.; Anderson, R. The Role of Co-Infections and Secondary Infections in Patients with COVID-19. Pneumonia 2021, 13, 5. [Google Scholar] [CrossRef] [PubMed]
- Paparoupa, M.; Aldemyati, R.; Roggenkamp, H.; Berinson, B.; Nörz, D.; Olearo, F.; Kluge, S.; Roedl, K.; de Heer, G.; Wichmann, D. The Prevalence of Early- and Late-onset Bacterial, Viral, and Fungal Respiratory Superinfections in Invasively Ventilated COVID-19 Patients. J. Med. Virol. 2022, 94, 1920–1925. [Google Scholar] [CrossRef] [PubMed]
- Metlay, J.P.; Waterer, G.W.; Long, A.C.; Anzueto, A.; Brozek, J.; Crothers, K.; Cooley, L.A.; Dean, N.C.; Fine, M.J.; Flanders, S.A.; et al. Diagnosis and Treatment of Adults with Community-Acquired Pneumonia. An Official Clinical Practice Guideline of the American Thoracic Society and Infectious Diseases Society of America. Am. J. Respir. Crit. Care Med. 2019, 200, e45–e67. [Google Scholar] [CrossRef] [PubMed]
- Mocanu, A.; Lazureanu, V.E.; Laza, R.; Marinescu, A.R.; Cut, T.G.; Sincaru, S.-V.; Marza, A.M.; Popescu, I.-M.; Herlo, L.-F.; Nelson-Twakor, A.; et al. Laboratory Findings and Clinical Outcomes of ICU-Admitted COVID-19 Patients: A Retrospective Assessment of Particularities Identified among Romanian Minorities. J. Pers. Med. 2023, 13, 195. [Google Scholar] [CrossRef] [PubMed]
- Bakaletz, L.O. Viral–Bacterial Co-Infections in the Respiratory Tract. Curr. Opin. Microbiol. 2017, 35, 30–35. [Google Scholar] [CrossRef]
- Mirzaei, R.; Goodarzi, P.; Asadi, M.; Soltani, A.; Ali Abraham, H.A.; Jeda, A.S.; Dashtbin, S.; Jalalifar, S.; Mohammadzadeh, R.; Teimoori, A.; et al. Bacterial Co-infections with SARS-CoV-2. IUBMB Life 2020, 72, 2097–2111. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.; Pavia, A.T. Editorial Commentary: The Modern Quest for the “Holy Grail” of Pneumonia Etiology. Clin. Infect. Dis. 2016, 62, 826–828. [Google Scholar] [CrossRef]
- Ewig, S.; Schlochtermeier, M.; Goïke, N.; Niederman, M.S. Applying Sputum as a Diagnostic Tool in Pneumonia. Chest 2002, 121, 1486–1492. [Google Scholar] [CrossRef]
- Mandell, L.A.; Wunderink, R.G.; Anzueto, A.; Bartlett, J.G.; Campbell, G.D.; Dean, N.C.; Dowell, S.F.; File, T.M.; Musher, D.M.; Niederman, M.S.; et al. Infectious Diseases Society of America/American Thoracic Society Consensus Guidelines on the Management of Community-Acquired Pneumonia in Adults. Clin. Infect. Dis. 2007, 44, S27–S72. [Google Scholar] [CrossRef]
- Asti, L.; Bartsch, S.M.; Umscheid, C.A.; Hamilton, K.; Nachamkin, I.; Lee, B.Y. The Potential Economic Value of Sputum Culture Use in Patients with Community-Acquired Pneumonia and Healthcare-Associated Pneumonia. Clin. Microbiol. Infect. 2019, 25, 1038.e1–1038.e9. [Google Scholar] [CrossRef] [PubMed]
- Messika, J.; Stoclin, A.; Bouvard, E.; Fulgencio, J.-P.; Ridel, C.; Muresan, I.-P.; Boffa, J.-J.; Bachmeyer, C.; Denis, M.; Gounant, V.; et al. The Challenging Diagnosis of Non-Community-Acquired Pneumonia in Non-Mechanically Ventilated Subjects: Value of Microbiological Investigation. Respir. Care 2016, 61, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Cataño-Correa, J.C.; Cardona-Arias, J.A.; Porras Mancilla, J.P.; García, M.T. Bacterial Superinfection in Adults with COVID-19 Hospitalized in Two Clinics in Medellín-Colombia, 2020. PLoS ONE 2021, 16, e0254671. [Google Scholar] [CrossRef] [PubMed]
- Timpau, A.-S.; Miftode, R.-S.; Costache, I.-I.; Petris, A.O.; Miftode, I.-L.; Gheorghe, L.; Timpau, R.; Miftode, I.D.; Prepeliuc, C.S.; Coman, I.; et al. An Overview of the Impact of Bacterial Infections and the Associated Mortality Predictors in Patients with COVID-19 Admitted to a Tertiary Center from Eastern Europe. Antibiotics 2023, 12, 144. [Google Scholar] [CrossRef] [PubMed]
- Langford, B.J.; So, M.; Raybardhan, S.; Leung, V.; Soucy, J.-P.R.; Westwood, D.; Daneman, N.; MacFadden, D.R. Antibiotic Prescribing in Patients with COVID-19: Rapid Review and Meta-Analysis. Clin. Microbiol. Infect. 2021, 27, 520–531. [Google Scholar] [CrossRef] [PubMed]
- Novacescu, A.N.; Buzzi, B.; Bedreag, O.; Papurica, M.; Rogobete, A.F.; Sandesc, D.; Sorescu, T.; Baditoiu, L.; Musuroi, C.; Vlad, D.; et al. Bacterial and Fungal Superinfections in COVID-19 Patients Hospitalized in an Intensive Care Unit from Timișoara, Romania. Infect. Drug Resist. 2022, 15, 7001–7014. [Google Scholar] [CrossRef]
- Contou, D.; Claudinon, A.; Pajot, O.; Micaëlo, M.; Longuet Flandre, P.; Dubert, M.; Cally, R.; Logre, E.; Fraissé, M.; Mentec, H.; et al. Bacterial and Viral Co-Infections in Patients with Severe SARS-CoV-2 Pneumonia Admitted to a French ICU. Ann. Intensive Care 2020, 10, 119. [Google Scholar] [CrossRef] [PubMed]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA 2020, 323, 1574. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Torres, V.; de Mendoza, C.; de la Fuente, S.; Sánchez, E.; Martínez-Urbistondo, M.; Herráiz, J.; Gutiérrez, A.; Gutiérrez, Á.; Hernández, C.; Callejas, A.; et al. Bacterial Infections in Patients Hospitalized with COVID-19. Intern. Emerg. Med. 2022, 17, 431–438. [Google Scholar] [CrossRef] [PubMed]
- Scott, H.; Zahra, A.; Fernandes, R.; Fries, B.C.; Thode, H.C.; Singer, A.J. Bacterial Infections and Death among Patients with Covid-19 versus Non COVID-19 Patients with Pneumonia. Am. J. Emerg. Med. 2022, 51, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Dubourg, G.; Abat, C.; Rolain, J.-M.; Raoult, D. Correlation between Sputum and Bronchoalveolar Lavage Fluid Cultures. J. Clin. Microbiol. 2015, 53, 994–996. [Google Scholar] [CrossRef] [PubMed]
- Mazloomirad, F.; Hasanzadeh, S.; Sharifi, A.; Nikbakht, G.; Roustaei, N.; Khoramrooz, S.S. Identification and Detection of Pathogenic Bacteria from Patients with Hospital-Acquired Pneumonia in Southwestern Iran; Evaluation of Biofilm Production and Molecular Typing of Bacterial Isolates. BMC Pulm. Med. 2021, 21, 408. [Google Scholar] [CrossRef] [PubMed]
- Musuuza, J.S.; Watson, L.; Parmasad, V.; Putman-Buehler, N.; Christensen, L.; Safdar, N. Prevalence and Outcomes of Co-Infection and Superinfection with SARS-CoV-2 and Other Pathogens: A Systematic Review and Meta-Analysis. PLoS ONE 2021, 16, e0251170. [Google Scholar] [CrossRef] [PubMed]
- Ripa, M.; Galli, L.; Poli, A.; Oltolini, C.; Spagnuolo, V.; Mastrangelo, A.; Muccini, C.; Monti, G.; De Luca, G.; Landoni, G.; et al. Secondary Infections in Patients Hospitalized with COVID-19: Incidence and Predictive Factors. Clin. Microbiol. Infect. 2021, 27, 451–457. [Google Scholar] [CrossRef] [PubMed]
- Lv, Z.; Cheng, S.; Le, J.; Huang, J.; Feng, L.; Zhang, B.; Li, Y. Clinical Characteristics and Co-Infections of 354 Hospitalized Patients with COVID-19 in Wuhan, China: A Retrospective Cohort Study. Microbes Infect. 2020, 22, 195–199. [Google Scholar] [CrossRef]
- Patel, A.; Emerick, M.; Cabunoc, M.K.; Williams, M.H.; Preas, M.A.; Schrank, G.; Rabinowitz, R.; Luethy, P.; Johnson, J.K.; Leekha, S. Rapid Spread and Control of Multidrug-Resistant Gram-Negative Bacteria in COVID-19 Patient Care Units. Emerg. Infect. Dis. 2021, 27, 1234–1237. [Google Scholar] [CrossRef] [PubMed]
- Clancy, C.J.; Schwartz, I.S.; Kula, B.; Nguyen, M.H. Bacterial Superinfections Among Persons With Coronavirus Disease 2019: A Comprehensive Review of Data From Postmortem Studies. Open Forum Infect. Dis. 2021, 8, ofab065. [Google Scholar] [CrossRef]
- Despotović, A.; Barać, A.; Cucanić, T.; Cucanić, K.; Stevanović, G. Antibiotic (Mis)Use in COVID-19 Patients before and after Admission to a Tertiary Hospital in Serbia. Antibiotics 2022, 11, 847. [Google Scholar] [CrossRef] [PubMed]
- Nag, V.L.; Kaur, N. Superinfections in COVID-19 Patients: Role of Antimicrobials. Dubai Med. J. 2021, 4, 117–126. [Google Scholar] [CrossRef]
- Wongsurakiat, P.; Tulatamakit, S. Clinical Pulmonary Infection Score and a Spot Serum Procalcitonin Level to Guide Discontinuation of Antibiotics in Ventilator-Associated Pneumonia: A Study in a Single Institution with High Prevalence of Nonfermentative Gram-Negative Bacilli Infection. Adv. Respir. Dis. 2018, 12, 175346661876013. [Google Scholar] [CrossRef]
- Lăzureanu, V.; Poroșnicu, M.; Gândac, C.; Moisil, T.; Bădițoiu, L.; Laza, R.; Musta, V.; Crișan, A.; Marinescu, A.-R. Infection with Acinetobacter Baumannii in an Intensive Care Unit in the Western Part of Romania. BMC Infect. Dis. 2016, 16, 95. [Google Scholar] [CrossRef] [PubMed]
- Rayeesa Faheem, S.; Srinivas, T.; Sadhana, Y. A Comparative Study of Acinetobacter Infections in COVID and Non-COVID Patients. J. Infect. Dis. Epidemiol. 2022, 8, E19–E26. [Google Scholar] [CrossRef]
- Soltani, S.; Zakeri, A.; Zandi, M.; Kesheh, M.M.; Tabibzadeh, A.; Dastranj, M.; Faramarzi, S.; Didehdar, M.; Hafezi, H.; Hosseini, P.; et al. The Role of Bacterial and Fungal Human Respiratory Microbiota in COVID-19 Patients. BioMed Res. Int. 2021, 2021, 6670798. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, S.; Saito, M.; Tamura, A.; Prawisuda, D.; Mizutani, T.; Yotsuyanagi, H. The Human Microbiome and COVID-19: A Systematic Review. PLoS ONE 2021, 16, e0253293. [Google Scholar] [CrossRef] [PubMed]
- Sharov, K.S. SARS-CoV-2-Related Pneumonia Cases in Pneumonia Picture in Russia in March-May 2020: Secondary Bacterial Pneumonia and Viral Co-Infections. J. Glob. Health 2020, 10, 020504. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, C.G.K.; Allon, S.J.; Nyquist, S.K.; Mbano, I.M.; Miao, V.N.; Tzouanas, C.N.; Cao, Y.; Yousif, A.S.; Bals, J.; Hauser, B.M.; et al. SARS-CoV-2 Receptor ACE2 Is an Interferon-Stimulated Gene in Human Airway Epithelial Cells and Is Detected in Specific Cell Subsets across Tissues. Cell 2020, 181, 1016–1035.e19. [Google Scholar] [CrossRef]
- Merenstein, C.; Liang, G.; Whiteside, S.A.; Cobián-Güemes, A.G.; Merlino, M.S.; Taylor, L.J.; Glascock, A.; Bittinger, K.; Tanes, C.; Graham-Wooten, J.; et al. Signatures of COVID-19 Severity and Immune Response in the Respiratory Tract Microbiome. mBio 2021, 12, e01777-21. [Google Scholar] [CrossRef] [PubMed]
- Rothberg, M.B.; Haessler, S.D. Complications of Seasonal and Pandemic Influenza. Crit. Care Med. 2010, 38, e91–e97. [Google Scholar] [CrossRef] [PubMed]
- Monecke, S.; Müller, E.; Dorneanu, O.S.; Vremeră, T.; Ehricht, R. Molecular Typing of MRSA and of Clinical Staphylococcus Aureus Isolates from Iaşi, Romania. PLoS ONE 2014, 9, e97833. [Google Scholar] [CrossRef]
- Bouchiat, C.; Curtis, S.; Spiliopoulou, I.; Bes, M.; Cocuzza, C.; Codita, I.; Dupieux, C.; Giormezis, N.; Kearns, A.; Laurent, F.; et al. MRSA Infections among Patients in the Emergency Department: A European Multicentre Study. J. Antimicrob. Chemother. 2017, 72, 372–375. [Google Scholar] [CrossRef] [PubMed]
- Hassoun, A.; Linden, P.K.; Friedman, B. Incidence, Prevalence, and Management of MRSA Bacteremia across Patient Populations—a Review of Recent Developments in MRSA Management and Treatment. Crit Care 2017, 21, 211. [Google Scholar] [CrossRef] [PubMed]
- Basile, K.; Halliday, C.; Kok, J.; Chen, S.C.-A. Fungal Infections Other Than Invasive Aspergillosis in COVID-19 Patients. J. Fungi 2022, 8, 58. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, I.S.; Friedman, D.Z.P.; Zapernick, L.; Dingle, T.C.; Lee, N.; Sligl, W.; Zelyas, N.; Smith, S.W. High Rates of Influenza-Associated Invasive Pulmonary Aspergillosis May Not Be Universal: A Retrospective Cohort Study from Alberta, Canada. Clin. Infect. Dis. 2020, 71, 1760–1763. [Google Scholar] [CrossRef] [PubMed]
- Mouren, D.; Goyard, C.; Catherinot, E.; Givel, C.; Chabrol, A.; Tcherakian, C.; Longchampt, E.; Vargaftig, J.; Farfour, E.; Legal, A.; et al. COVID-19 and Pneumocystis Jirovecii Pneumonia: Back to the Basics. Respir. Med. Res. 2021, 79, 100814. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.K.; Singh, R.; Joshi, S.R.; Misra, A. Mucormycosis in COVID-19: A Systematic Review of Cases Reported Worldwide and in India. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 102146. [Google Scholar] [CrossRef] [PubMed]
- Kurt, A.F.; Mete, B.; Urkmez, S.; Demirkiran, O.; Dumanli, G.Y.; Bozbay, S.; Dilken, O.; Karaali, R.; Balkan, I.I.; Saltoğlu, N.; et al. Incidence, Risk Factors, and Prognosis of Bloodstream Infections in COVID-19 Patients in Intensive Care: A Single-Center Observational Study. J. Intensive Care Med. 2022, 37, 1353–1362. [Google Scholar] [CrossRef] [PubMed]
- Koltsida, G.; Zaoutis, T. Fungal Lung Disease. Paediatr. Respir. Rev. 2021, 37, 99–104. [Google Scholar] [CrossRef]
- Arastehfar, A.; Carvalho, A.; Nguyen, M.H.; Hedayati, M.T.; Netea, M.G.; Perlin, D.S.; Hoenigl, M. COVID-19-Associated Candidiasis (CAC): An Underestimated Complication in the Absence of Immunological Predispositions? J. Fungi 2020, 6, 211. [Google Scholar] [CrossRef]
- Sharifipour, E.; Shams, S.; Esmkhani, M.; Khodadadi, J.; Fotouhi-Ardakani, R.; Koohpaei, A.; Doosti, Z.; EJ Golzari, S. Evaluation of Bacterial Co-Infections of the Respiratory Tract in COVID-19 Patients Admitted to ICU. BMC Infect Dis. 2020, 20, 646. [Google Scholar] [CrossRef]
- Muzurovic, S.; Babajic, E.; Masic, T.; Smajic, R.; Selmanagic, A. The Relationship between Oral Hygiene and Oral Colonisation with Candida Species. Med. Arch. 2012, 66, 415. [Google Scholar] [CrossRef] [PubMed]
- Pisano, M.; Romano, A.; Di Palo, M.P.; Baroni, A.; Serpico, R.; Contaldo, M. Oral Candidiasis in Adult and Pediatric Patients with COVID-19. Biomedicines 2023, 11, 846. [Google Scholar] [CrossRef] [PubMed]
- Oancea, R.; Amariei, C.; Eaton, K.A.; Widström, E. The Healthcare System and the Provision of Oral Healthcare in European Union Member States: Part 5: Romania. Br. Dent. J. 2016, 220, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Babamahmoodi, F.; Rezai, M.S.; Ahangarkani, F.; Mohammadi Kali, A.; Alizadeh-Navaei, R.; Alishahi, A.; Najafi, N.; Haddadi, A.; Davoudi, A.; Azargon, L.; et al. Multiple Candida Strains Causing Oral Infection in COVID-19 Patients under Corticosteroids and Antibiotic Therapy: An Observational Study. Front. Cell. Infect. Microbiol. 2022, 12, 1103226. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, J. Enhanced Antibiotic Resistance as a Collateral COVID-19 Pandemic Effect? J. Hosp. Infect. 2021, 107, 114–115. [Google Scholar] [CrossRef] [PubMed]
- Szabó, S.; Feier, B.; Capatina, D.; Tertis, M.; Cristea, C.; Popa, A. An Overview of Healthcare Associated Infections and Their Detection Methods Caused by Pathogen Bacteria in Romania and Europe. J. Clin. Med. 2022, 11, 3204. [Google Scholar] [CrossRef] [PubMed]
- Pérez de la Lastra, J.M.; Anand, U.; González-Acosta, S.; López, M.R.; Dey, A.; Bontempi, E.; Morales delaNuez, A. Antimicrobial Resistance in the COVID-19 Landscape: Is There an Opportunity for Anti-Infective Antibodies and Antimicrobial Peptides? Front. Immunol. 2022, 13, 921483. [Google Scholar] [CrossRef] [PubMed]
- Rawson, T.M.; Moore, L.S.P.; Zhu, N.; Ranganathan, N.; Skolimowska, K.; Gilchrist, M.; Satta, G.; Cooke, G.; Holmes, A. Bacterial and Fungal Coinfection in Individuals with Coronavirus: A Rapid Review To Support COVID-19 Antimicrobial Prescribing. Clin. Infect. Dis. 2020, 71, 2459–2468. [Google Scholar] [CrossRef] [PubMed]
- Khoshbakht, R.; Kabiri, M.; Neshani, A.; Khaksari, M.N.; Sadrzadeh, S.M.; Mousavi, S.M.; Ghazvini, K.; Ghavidel, M. Assessment of Antibiotic Resistance Changes during the COVID-19 Pandemic in Northeast of Iran during 2020–2022: An Epidemiological Study. Antimicrob. Resist. Infect. Control 2022, 11, 121. [Google Scholar] [CrossRef] [PubMed]
- Sulayyim, H.J.A.; Ismail, R.; Hamid, A.A.; Ghafar, N.A. Antibiotic Resistance during COVID-19: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 11931. [Google Scholar] [CrossRef]
- Protocol-tratament-covid19-ms. Available online: https://www.cnscbt.ro/index.php/legislatie_cov/1617-protocolul-de-tratament-covid-19/file (accessed on 17 December 2022).
- Malik, P.; Patel, U.; Mehta, D.; Patel, N.; Kelkar, R.; Akrmah, M.; Gabrilove, J.L.; Sacks, H. Biomarkers and Outcomes of COVID-19 Hospitalisations: Systematic Review and Meta-Analysis. BMJ Evid.-Based Med. 2021, 26, 107–108. [Google Scholar] [CrossRef]
- Dumache, R.; Daescu, E.; Ciocan, V.; Mureşan, C.; Talida, C.; Gavrilita, D.; Enache, A. Molecular Testing of SARS-CoV-2 Infection from Blood Samples in Disseminated Intravascular Coagulation (DIC) and Elevated D-Dimer Levels. Clin. Lab. 2021, 67. [Google Scholar] [CrossRef] [PubMed]
- Mocanu, A.; Lazureanu, V.E.; Marinescu, A.R.; Cut, T.G.; Laza, R.; Rusu, L.-C.; Marza, A.M.; Nelson-Twakor, A.; Negrean, R.A.; Popescu, I.-M.; et al. A Retrospective Assessment of Laboratory Findings and Cytokine Markers in Severe SARS-CoV-2 Infection among Patients of Roma Population. J. Clin. Med. 2022, 11, 6777. [Google Scholar] [CrossRef] [PubMed]
- Cheng, K.; He, M.; Shu, Q.; Wu, M.; Chen, C.; Xue, Y. Analysis of the Risk Factors for Nosocomial Bacterial Infection in Patients with COVID-19 in a Tertiary Hospital. Risk Manag. Healthc. Policy 2020, 13, 2593–2599. [Google Scholar] [CrossRef]
- Fehér, Á.; Szarvas, Z.; Lehoczki, A.; Fekete, M.; Fazekas-Pongor, V. Co-Infections in COVID-19 Patients and Correlation with Mortality Rate. Minireview. Physiol. Int. 2022, 109, 1–8. [Google Scholar] [CrossRef]
- Shafran, N.; Shafran, I.; Ben-Zvi, H.; Sofer, S.; Sheena, L.; Krause, I.; Shlomai, A.; Goldberg, E.; Sklan, E.H. Secondary Bacterial Infection in COVID-19 Patients Is a Stronger Predictor for Death Compared to Influenza Patients. Sci. Rep. 2021, 11, 12703. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Quinn, J.; Pinsky, B.; Shah, N.H.; Brown, I. Rates of Co-Infection between SARS-CoV-2 and Other Respiratory Pathogens. JAMA 2020, 323, 2085. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Positive Sputum | Negative Sputum (n = 243) | p-Value | ||
|---|---|---|---|---|---|
| Pathogenic bacteria (n = 46) | Commensal Pathogens (n = 67) | Fungi (n = 51) | |||
| Age | 0.369 | ||||
| 18–40 years | 2 (4.3%) | 4 (6.0%) | 1 (2.0%) | 14 (5.8%) | |
| 40–65 years | 19 (41.3%) | 22 (32.8%) | 25 (49.0%) | 79 (32.5%) | |
| >65 years | 25 (54.3%) | 41 (61.2%) | 25 (49.0%) | 150 (61.7%) | |
| Age (mean ± SD) | 62.1 ± 12.0 | 66.8 ± 13.7 | 64.4 ± 11.3 | 67.5 ± 14.8 | 0.073 |
| Sex | 0.900 | ||||
| Men | 27 (58.7%) | 35 (52.2%) | 28 (54.9%) | 129 (53.1%) | |
| Women | 19 (41.3%) | 32 (47.8%) | 23 (45.1%) | 114 (46.9%) | |
| Area of residence | 0.649 | ||||
| Urban | 24 (52.5%) | 32 (56.9%) | 29 (56.9%) | 136 (56.0%) | |
| Rural | 22 (47.8%) | 35 (43.1%) | 22 (43.1%) | 107 (44.0%) | |
| BMI | 0.539 | ||||
| Underweight (<18.5 kg/m2) | 4 (8.7%) | 4 (6.0%) | 6 (11.8%) | 14 (5.8%) | |
| Normal weight (18.5–25.0 kg/m2) | 25 (54.3%) | 40 (59.7%) | 22 (43.1%) | 130 (53.5%) | |
| Overweight (>25.0 kg/m2) | 17 (37.0%) | 23 (34.3%) | 23 (45.1%) | 99 (40.7%) | |
| Smoking status | 0.195 | ||||
| No | 12 (26.1%) | 10 (14.9%) | 9 (17.6%) | 63 (25.9%) | |
| Yes | 34 (73.9%) | 57 (85.1%) | 42 (82.4%) | 180 (74.1%) | |
| Pre-existing lung disease | 0.532 | ||||
| No | 5 (10.9%) | 6 (9.0%) | 9 (17.6%) | 33 (13.6%) | |
| Yes | 41 (89.1%) | 61 (91.0%) | 42 (82.4%) | 210 (86.4%) | |
| Comorbidities | 0.166 | ||||
| 0 | 3 (6.5%) | 1 (1.5%) | 2 (3.9%) | 12 (4.9%) | |
| 1–2 | 23 (50.0%) | 35 (52.2%) | 27 (52.9%) | 155 (63.8%) | |
| ≥3 | 20 (46.3%) | 31 (46.3%) | 22 (43.1%) | 76 (31.3%) | |
| Variables | Positive Sputum | Negative Sputum (n = 243) | p-Value | ||
|---|---|---|---|---|---|
| Pathogenic bacteria (n = 46) | Commensal Pathogens (n = 67) | Fungi (n = 51) | |||
| Days from symptom onset until hospitalization (mean ± SD) | 6.1 ± 1.4 | 5.9 ± 1.0 | 4.7 ± 1.5 | 6.8 ± 1.8 | <0.001 |
| Days from positive COVID-19 PCR test until hospitalization (mean ± SD) | 4.2 ± 1.5 | 4.0 ± 1.4 | 4.2 ± 1.5 | 4.0 ± 1.4 | 0.359 |
| Prior hospitalization | 0.279 | ||||
| No | 40 (87.0%) | 59 (88.1%) | 40 (78.4%) | 215 (88.5%) | |
| Yes | 6 (13.0%) | 8 (11.9%) | 11 (21.6%) | 28 (11.5%) | |
| Time of sampling | 0.520 | ||||
| Within 48 h from admission | 28 (60.9%) | 36 (53.7%) | 31 (60.8%) | 126 (51.9%) | |
| After 48 h from admission | 18 (39.1%) | 31 (46.3%) | 20 (39.2%) | 117 (48.1%) | |
| Multidrug resistance | 0.283 | ||||
| Yes | 42 (91.3%) | 55 (82.1%) | 41 (80.4%) | - | |
| No | 4 (8.7%) | 12 (17.9%) | 10 (19.6%) | - | |
| Variables | Positive Sputum | p-Value | ||
|---|---|---|---|---|
| Pathogenic bacteria (n = 46) | Commensal Pathogens (n = 67) | Fungi (n = 51) | ||
| Distribution of antimicrobial resistance | ||||
| 0 drug resistance | 4 (8.7%) | 12 (17.9%) | 10 (19.6%) | 0.283 |
| 1 drug resistance | 7 (15.2%) | 15 (22.4%) | 11 (21.6%) | 0.616 |
| 2 drug resistance | 10 (21.7%) | 18 (26.9%) | 13 (25.5%) | 0.822 |
| 3 drug resistance | 11 (23.9%) | 10 (14.9%) | 14 (27.5%) | 0.227 |
| 4 drug resistance | 7 (15.2%) | 6 (9.0%) | 3 (5.8%) | 0.289 |
| 5 drug resistance | 4 (8.7%) | 3 (4.5%) | 0 (0.0%) | 0.106 |
| >5 drug resistance | 3 (6.5%) | 3 (4.5%) | 0 (0.0%) | 0.208 |
| Variables | Positive Sputum | Negative Sputum (n = 243) | p-Value | |||
|---|---|---|---|---|---|---|
| Normal Range | Pathogenic bacteria (n = 46) | Commensal Pathogens (n = 67) | Fungi (n = 51) | |||
| RBC (millions/mm3) | 4.35–5.65 | 6 (13.0%) | 12 (17.9%) | 11 (21.6%) | 28 (11.5%) | 0.207 |
| PLT (thousands/mm3) | 150–450 | 2 (4.3%) | 4 (6.0%) | 1 (2.0%) | 14 (5.8%) | 0.705 |
| WBC (thousands/mm3) | 4.5–11.0 | 34 (73.9%) | 57 (85.1%) | 29 (56.9%) | 114 (46.9%) | <0.001 |
| Lymphocytes (thousands/mm3) | 1.0–4.8 | 11 (23.9%) | 18 (26.9%) | 27 (52.9%) | 107 (44.0%) | 0.002 |
| Hb (g/dL) | 13.0–17.0 | 7 (15.2%) | 6 (9.0%) | 10 (19.6%) | 33 (13.6%) | 0.413 |
| Hematocrit (%) | 36–48 | 10 (21.7%) | 12 (17.9%) | 8 (15.7%) | 35 (14.4%) | 0.620 |
| Creatinine (µmol/L) | 0.74–1.35 | 17 (37.0%) | 23 (34.3%) | 25 (49.0%) | 97 (39.9%) | 0.422 |
| BUN (mmol/L) | 2.1–8.5 | 12 (26.1%) | 10 (14.9%) | 9 (17.6%) | 50 (20.6%) | 0.497 |
| GFR | >60 | 6 (13.0%) | 10 (14.9%) | 3 (5.8%) | 12 (4.9%) | 0.021 |
| Fasting glucose (mg/dL) | 72–125 | 23 (50.0%) | 35 (52.2%) | 27 (52.9%) | 92 (37.9%) | 0.048 |
| ALT (U/L) | 7–35 | 6 (13.0%) | 8 (11.9%) | 13 (25.5%) | 26 (10.7%) | 0.041 |
| AST (U/L) | 10–40 | 4 (8.7%) | 9 (13.4%) | 10 (19.6%) | 22 (9.1%) | 0.142 |
| INR | 1.1 | 5 (10.9%) | 7 (10.4%) | 7 (13.7%) | 13 (5.3%) | 0.125 |
| Ferritin (ng/mL) | 15–300 | 13 (28.3%) | 44 (23.9%) | 19 (37.3%) | 62 (25.5%) | 0.339 |
| LDH (U/L) | 100–300 | 16 (34.8%) | 23 (34.3%) | 20 (39.2%) | 56 (23.0%) | 0.037 |
| Procalcitonin (ng/mL) | <0.5 | 28 (60.9%) | 41 (61.2%) | 12 (23.5%) | 29 (11.9%) | <0.001 |
| Lactate (mmol/L) | <1 | 18 (39.1%) | 30 (44.8%) | 35 (68.6%) | 58 (23.9%) | <0.001 |
| CRP (mg/L) | 0–10 | 40 (87.0%) | 59 (88.1%) | 39 (76.5%) | 124 (51.0%) | <0.001 |
| IL-6 (pg/mL) | 0–16 | 32 (69.6%) | 37 (55.2%) | 39 (76.5%) | 133 (54.7%) | 0.012 |
| ESR (mm/h) | 0–22 | 28 (60.9%) | 32 (47.8%) | 34 (66.7%) | 95 (39.1%) | 0.001 |
| Fibrinogen (g/L) | 2–4 | 31 (67.4%) | 39 (58.2%) | 30 (58.8%) | 91 (37.4%) | <0.001 |
| D-dimer (ng/mL) | <250 | 25 (54.3%) | 46 (68.7%) | 31 (60.8%) | 94 (38.7%) | <0.001 |
| Variables | Positive Sputum | Negative Sputum (n = 243) | p-Value | ||
|---|---|---|---|---|---|
| Pathogenic bacteria (n = 46) | Commensal Pathogens (n = 67) | Fungi (n = 51) | |||
| Severe complications | 0.028 | ||||
| Yes | 16 (34.8%) | 23 (34.3%) | 20 (39.2%) | 55 (22.6%) | |
| No | 30 (65.2%) | 44 (65.7%) | 31 (60.8%) | 187 (77.4%) | |
| COVID-19 severity | 0.122 | ||||
| Mild | 5 (10.9%) | 7 (10.4%) | 4 (7.8%) | 28 (11.5%) | |
| Moderate | 18 (39.1%) | 31 (46.3%) | 15 (29.4%) | 119 (49.0%) | |
| Severe | 23 (50.0%) | 29 (43.3%) | 32 (62.7%) | 96 (39.5%) | |
| Oxygen saturation at admission | 0.040 | ||||
| ≤98% | 7 (15.2%) | 9 (13.4%) | 5 (9.8%) | 38 (15.6%) | |
| 92–97% | 16 (34.8%) | 27 (40.3%) | 13 (25.5%) | 112 (46.1%) | |
| <92% | 23 (50.0%) | 31 (46.3%) | 33 (64.7%) | 93 (38.3%) | |
| Oxygen supplementation at admission | <0.001 | ||||
| Yes | 34 (73.9%) | 46 (68.7%) | 41 (80.4%) | 117 (48.1%) | |
| No | 12 (26.1%) | 21 (31.3%) | 10 (19.6%) | 126 (51.9%) | |
| Oxygen flow rate (L/min) | 12.8 ± 4.6 | 12.0 ± 5.1 | 12.8 ± 4.6 | 12.0 ± 5.1 | 0.120 |
| Outcomes | 0.118 | ||||
| ICU admission | 15 (32.6%) | 21 (31.3%) | 18 (35.3%) | 42 (17.3%) | 0.003 |
| Days in the ICU (mean ± SD) | 7.9 ± 2.2 | 7.3 ± 1.8 | 9.5 ± 2.4 | 6.6 ± 1.3 | <0.001 |
| Mortality | 13 (28.2%) | 15 (22.4%) | 14 (27.5%) | 34 (14.0%) | 0.023 |
| Days from admission until death (mean ± SD) | 8.8 ± 2.0 | 8.5 ± 1.5 | 10.2 ± 2.4 | 8.3 ± 1.1 | <0.001 |
| Days of hospitalization among survivors (mean ± SD) | 14.6 ± 5.2 | 13.8 ± 4.5 | 17.2 ± 6.0 | 12.0 ± 4.3 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cut, T.G.; Mavrea, A.; Cumpanas, A.A.; Novacescu, D.; Oancea, C.I.; Bratosin, F.; Marinescu, A.R.; Laza, R.; Mocanu, A.; Pescariu, A.S.; et al. A Retrospective Assessment of Sputum Samples and Antimicrobial Resistance in COVID-19 Patients. Pathogens 2023, 12, 620. https://doi.org/10.3390/pathogens12040620
Cut TG, Mavrea A, Cumpanas AA, Novacescu D, Oancea CI, Bratosin F, Marinescu AR, Laza R, Mocanu A, Pescariu AS, et al. A Retrospective Assessment of Sputum Samples and Antimicrobial Resistance in COVID-19 Patients. Pathogens. 2023; 12(4):620. https://doi.org/10.3390/pathogens12040620
Chicago/Turabian StyleCut, Talida Georgiana, Adelina Mavrea, Alin Adrian Cumpanas, Dorin Novacescu, Cristian Iulian Oancea, Felix Bratosin, Adelina Raluca Marinescu, Ruxandra Laza, Alexandra Mocanu, Alexandru Silvius Pescariu, and et al. 2023. "A Retrospective Assessment of Sputum Samples and Antimicrobial Resistance in COVID-19 Patients" Pathogens 12, no. 4: 620. https://doi.org/10.3390/pathogens12040620