
Clinical Evidence for the Use of Octenidine Dihydrochloride to Prevent Healthcare-Associated Infections and Decrease Staphylococcus aureus Carriage or Transmission—A Review
 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
- What is the impact of using OCT-containing solutions for the decolonization of known carriers of S. aureus including methicillin-resistant S. aureus (MRSA) and methicillin-susceptible S. aureus (MSSA) on transmission or infection?
- What is the impact of using OCT-containing solutions directly before surgical interventions (pre-incisional antisepsis or skin preparation) or universally and multiple times before and after surgical interventions (pre-operative bathing/washing) on the occurrence of SSIs?
- What is the impact of using OCT-containing solutions directly before catheter insertion (pre-insertional antisepsis) or universally and multiple times among patients at risk on the occurrence of ICU- or catheter-related bloodstream infections and infections at catheter insertion sites?
2. Materials and Methods
3. Results
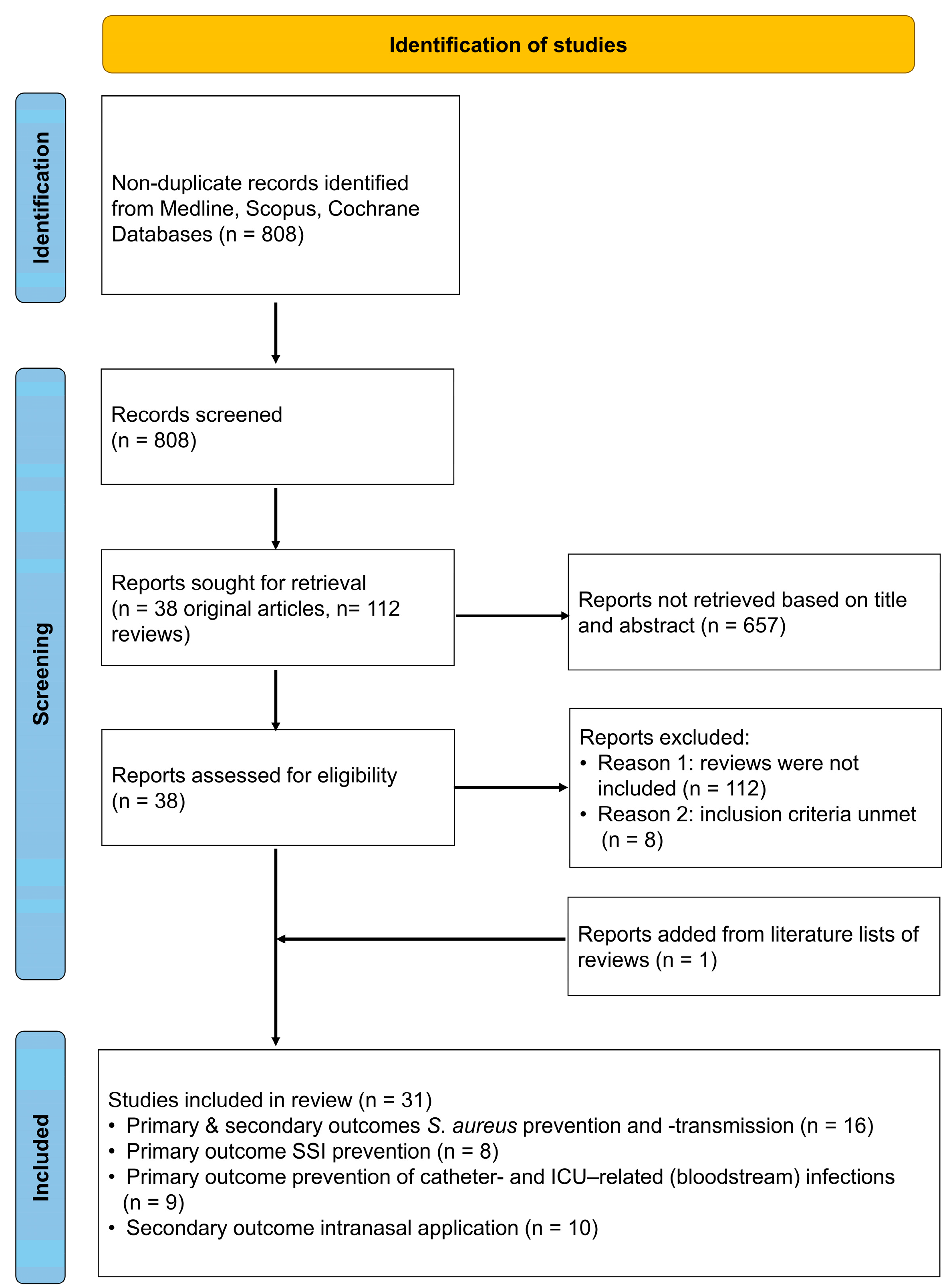
3.1. Literature Search Results
3.2. S. aureus Decolonization, Infection Prevention, and Nosocomial Transmission
3.3. Incidence of Surgical Site Infections
3.4. Incidence of ICU- or Catheter-Related Bloodstream Infections and Insertion Site Infections
3.5. Secondary Outcome—Nasal Application of OCT
4. Discussion
4.1. Outcomes of S. aureus Decolonization and Prevention of S. aureus Infection and Transmission
4.2. Outcome Prevention of Surgical Site Infections
4.3. Outcome Prevention of ICU-/Catheter-Related Bloodstream Infections and Insertion Site Infections
4.4. Secondary Outcome Intranasal OCT Use
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Malanovic, N.; Ön, A.; Pabst, G.; Zellner, A.; Lohner, K. Octenidine: Novel Insights into the Detailed Killing Mechanism of Gram-Negative Bacteria at a Cellular and Molecular Level. Int. J. Antimicrob. Agents 2020, 56, 106146. [Google Scholar] [CrossRef]
- Malanovic, N.; Buttress, J.A.; Vejzovic, D.; Ön, A.; Piller, P.; Kolb, D.; Lohner, K.; Strahl, H. Disruption of the Cytoplasmic Membrane Structure and Barrier Function Underlies the Potent Antiseptic Activity of Octenidine in Gram-Positive Bacteria. Appl. Environ. Microbiol. 2022, 88, e0018022. [Google Scholar] [CrossRef]
- Babalska, Z.Ł.; Korbecka-Paczkowska, M.; Karpiński, T.M. Wound Antiseptics and European Guidelines for Antiseptic Application in Wound Treatment. Pharmaceuticals 2021, 14, 1253. [Google Scholar] [CrossRef]
- Kramer, A.; Dissemond, J.; Kim, S.; Willy, C.; Mayer, D.; Papke, R.; Tuchmann, F.; Assadian, O. Consensus on Wound Antisepsis: Update 2018. Skin Pharmacol. Physiol. 2018, 31, 28–58. [Google Scholar] [CrossRef]
- Hübner, N.-O.; Siebert, J.; Kramer, A. Octenidine Dihydrochloride, a Modern Antiseptic for Skin, Mucous Membranes and Wounds. Skin Pharmacol. Physiol. 2010, 23, 244–258. [Google Scholar] [CrossRef]
- Denkel, L.A.; Kramer, T.S.; Schwab, F.; Golembus, J.; Wolke, S.; Gastmeier, P.; Geffers, C. Chlorhexidine and Octenidine Susceptibility of Bacterial Isolates from Clinical Samples in a Three-Armed Cluster Randomised Decolonisation Trial. PLoS ONE 2022, 17, e0278569. [Google Scholar] [CrossRef]
- Hardy, K.; Sunnucks, K.; Gil, H.; Shabir, S.; Trampari, E.; Hawkey, P.; Webber, M. Increased Usage of Antiseptics Is Associated with Reduced Susceptibility in Clinical Isolates of Staphylococcus aureus. mBio 2018, 9, e00894-18. [Google Scholar] [CrossRef]
- Franz, T.; Vögelin, E. Aseptic Tissue Necrosis and Chronic Inflammation after Irrigation of Penetrating Hand Wounds Using Octenisept®. J. Hand Surg. Eur. Vol. 2012, 37, 61–64. [Google Scholar] [CrossRef]
- Schupp, C.J.; Holland-Cunz, S. Persistent Subcutaneous Oedema and Aseptic Fatty Tissue Necrosis after Using Octenisept. Eur. J. Pediatr. Surg. 2009, 19, 179–183. [Google Scholar] [CrossRef]
- Zhao, T.; Wu, X.; Zhang, Q.; Li, C.; Worthington, H.V.; Hua, F. Oral Hygiene Care for Critically Ill Patients to Prevent Ventilator-Associated Pneumonia. Cochrane Database Syst. Rev. 2020, 12, CD008367. [Google Scholar] [CrossRef]
- Hadiati, D.R.; Hakimi, M.; Nurdiati, D.S.; Masuzawa, Y.; da Silva Lopes, K.; Ota, E. Skin Preparation for Preventing Infection Following Caesarean Section. Cochrane Database Syst. Rev. 2020, 6, CD007462. [Google Scholar] [CrossRef]
- Frost, S.A.; Alogso, M.-C.; Metcalfe, L.; Lynch, J.M.; Hunt, L.; Sanghavi, R.; Alexandrou, E.; Hillman, K.M. Chlorhexidine Bathing and Health Care-Associated Infections among Adult Intensive Care Patients: A Systematic Review and Meta-Analysis. Crit. Care 2016, 20, 379. [Google Scholar] [CrossRef] [PubMed]
- Afonso, E.; Blot, K.; Blot, S. Prevention of Hospital-Acquired Bloodstream Infections through Chlorhexidine Gluconate-Impregnated Washcloth Bathing in Intensive Care Units: A Systematic Review and Meta-Analysis of Randomised Crossover Trials. Eurosurveillance 2016, 21, 30400. [Google Scholar] [CrossRef] [PubMed]
- Lewis, S.R.; Schofield-Robinson, O.J.; Rhodes, S.; Smith, A.F. Chlorhexidine Bathing of the Critically Ill for the Prevention of Hospital-Acquired Infection. Cochrane Database Syst. Rev. 2019, 8, CD012248. [Google Scholar] [CrossRef] [PubMed]
- Lai, N.M.; Lai, N.A.; O’Riordan, E.; Chaiyakunapruk, N.; Taylor, J.E.; Tan, K. Skin Antisepsis for Reducing Central Venous Catheter-Related Infections. Cochrane Database Syst. Rev. 2016, 7, CD010140. [Google Scholar] [CrossRef]
- Liu, Z.; Norman, G.; Iheozor-Ejiofor, Z.; Wong, J.K.; Crosbie, E.J.; Wilson, P. Nasal Decontamination for the Prevention of Surgical Site Infection in Staphylococcus aureus Carriers. Cochrane Database Syst. Rev. 2017, 5, CD012462. [Google Scholar] [CrossRef]
- Webster, J.; Osborne, S. Preoperative Bathing or Showering with Skin Antiseptics to Prevent Surgical Site Infection. Cochrane Database Syst. Rev. 2015, 20, CD004985. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef]
- Allport, J.; Choudhury, R.; Bruce-Wootton, P.; Reed, M.; Tate, D.; Malviya, A. Efficacy of Mupirocin, Neomycin and Octenidine for Nasal Staphylococcus aureus Decolonisation: A Retrospective Cohort Study. Antimicrob. Resist. Infect. Control 2022, 11, 5. [Google Scholar] [CrossRef]
- Aung, A.-H.; Kyaw, W.M.; Heng, Y.K.; Tey, H.L.; Ang, B.; Chow, A. Intranasal Octenidine for Methicillin-Resistant Staphylococcus aureus (MRSA) Carriers and Universal Octenidine Bathing Reduced MRSA Acquisition in an Acute-Care General Ward. Infect. Control Hosp. Epidemiol. 2021, 43, 1701–1704. [Google Scholar] [CrossRef]
- Buehlmann, M.; Frei, R.; Fenner, L.; Dangel, M.; Fluckiger, U.; Widmer, A.F. Highly Effective Regimen for Decolonization of Methicillin-Resistant Staphylococcus aureus Carriers. Infect. Control Hosp. Epidemiol. 2008, 29, 510–516. [Google Scholar] [CrossRef] [PubMed]
- Chow, A.; Wong, J.; Zhang, W.; Poh, B.-F.; Ang, B. Intranasal Octenidine and Universal Chlorhexidine Bathing Can Reduce Meticillin-Resistant Staphylococcus aureus Acquisition in an Extended Care Facility in Singapore. J. Hosp. Infect. 2020, 105, 628–631. [Google Scholar] [CrossRef] [PubMed]
- Chow, A.; Hon, P.Y.; Tin, G.; Zhang, W.; Poh, B.F.; Ang, B. Intranasal Octenidine and Universal Antiseptic Bathing Reduce Methicillin-Resistant Staphylococcus aureus (MRSA) Prevalence in Extended Care Facilities. Epidemiol. Infect. 2018, 146, 2036–2041. [Google Scholar] [CrossRef] [PubMed]
- Danilevicius, M.; Juzéniené, A.; Juzénaité-Karneckiené, I.; Veršinina, A. MRSA Decontamination Using Octenidine-Based Products. Br. J. Nurs. 2015, 24, S36, S38–S40. [Google Scholar] [CrossRef] [PubMed]
- Hansen, D.; Patzke, P.-I.; Werfel, U.; Benner, D.; Brauksiepe, A.; Popp, W. Success of MRSA Eradication in Hospital Routine: Depends on Compliance. Infection 2007, 35, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.N.A.; Le, B.D.; Tambyah, P.; Hsu, L.Y.; Pada, S.; Archuleta, S.; Salmon, S.; Mukhopadhyay, A.; Dillon, J.; Ware, R.; et al. Antiseptic Body Washes for Reducing the Transmission of Methicillin-Resistant Staphylococcus aureus: A Cluster Crossover Study. Open Forum Infect. Dis. 2015, 2, ofv051. [Google Scholar] [CrossRef]
- Kaminski, A.; Kammler, J.; Wick, M.; Muhr, G.; Kutscha-Lissberg, F. Transmission of Methicillin-Resistant Staphylococcus aureus among Hospital Staff in a German Trauma Centre: A Problem without a Current Solution? J. Bone Jt. Surg. Br. 2007, 89, 642–645. [Google Scholar] [CrossRef]
- Pichler, G.; Pux, C.; Babeluk, R.; Hermann, B.; Stoiser, E.; De Campo, A.; Grisold, A.; Zollner-Schwetz, I.; Krause, R.; Schippinger, W. MRSA Prevalence Rates Detected in a Tertiary Care Hospital in Austria and Successful Treatment of MRSA Positive Patients Applying a Decontamination Regime with Octenidine. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 21–27. [Google Scholar] [CrossRef]
- Rengelshausen, J.; Nürnberger, J.; Philipp, T.; Kribben, A. Decolonization of Methicillin-Resistant Staphylococcus aureus by Disinfection of the Skin. Am. J. Med. 2000, 108, 685–686. [Google Scholar] [CrossRef]
- Richter, A.; Eder, I.; König, B.; Lutze, B.; Rodloff, A.C.; Thome, U.H.; Weiss, M.; Chaberny, I.F. Decolonization of Health Care Workers In a Neonatal Intensive Care Unit Carrying a Methicillin-Susceptible Staphylococcus aureus Isolate. Gesundheitswesen 2018, 80, 54–58. [Google Scholar] [CrossRef]
- Rohr, U.; Mueller, C.; Wilhelm, M.; Muhr, G.; Gatermann, S. Methicillin-Resistant Staphylococcus aureus Whole-Body Decolonization among Hospitalized Patients with Variable Site Colonization by Using Mupirocin in Combination with Octenidine Dihydrochloride. J. Hosp. Infect. 2003, 54, 305–309. [Google Scholar] [CrossRef] [PubMed]
- Sloot, N.; Siebert, J.; Höffler, U. Eradication of MRSA from Carriers by Means of Whole-Body Washing with an Antiseptic in Combination with Mupirocin Nasal Ointment. Zentralbl. Hyg. Umweltmed. 1999, 202, 513–523. [Google Scholar] [CrossRef] [PubMed]
- Spencer, C.; Orr, D.; Hallam, S.; Tillmanns, E. Daily Bathing with Octenidine on an Intensive Care Unit Is Associated with a Lower Carriage Rate of Meticillin-Resistant Staphylococcus aureus. J. Hosp. Infect. 2013, 83, 156–159. [Google Scholar] [CrossRef] [PubMed]
- Wisgrill, L.; Zizka, J.; Unterasinger, L.; Rittenschober-Böhm, J.; Waldhör, T.; Makristathis, A.; Berger, A. Active Surveillance Cultures and Targeted Decolonization Are Associated with Reduced Methicillin-Susceptible Staphylococcus aureus Infections in VLBW Infants. Neonatology 2017, 112, 267–273. [Google Scholar] [CrossRef]
- Hachenberg, J.; Acis, E.; Auer-Schmidt, M.M.; Warm, M.; Malter, W.; Thangarajah, F.; Eichler, C. Preoperative Octenidine Application in Breast Reconstruction Surgery. In Vivo 2021, 35, 549–554. [Google Scholar] [CrossRef]
- Jeans, E.; Holleyman, R.; Tate, D.; Reed, M.; Malviya, A. Methicillin Sensitive Staphylococcus aureus Screening and Decolonisation in Elective Hip and Knee Arthroplasty. J. Infect. 2018, 77, 405–409. [Google Scholar] [CrossRef]
- Karl, T.; Reuss, I.; Schwab, F.; Martin, M. Reduction of Inguinal Surgical Site Infections after Interventions on the Lower Extremities in Vascular Surgery. Gefässchirurgie 2017, 22, 533–541. [Google Scholar] [CrossRef]
- Kohler, P.; Sommerstein, R.; Schönrath, F.; Ajdler-Schäffler, E.; Anagnostopoulos, A.; Tschirky, S.; Falk, V.; Kuster, S.P.; Sax, H. Effect of Perioperative Mupirocin and Antiseptic Body Wash on Infection Rate and Causative Pathogens in Patients Undergoing Cardiac Surgery. Am. J. Infect. Control 2015, 43, E33–E38. [Google Scholar] [CrossRef]
- Matiasek, J.; Kienzl, P.; Otti, G.R.; Turk, B.R.; Djedovic, G.; Rieger, U.M. Aseptic Surgical Preparation for Upper Eyelid Blepharoplasty via Full-Face Octenidine Antiseptic without Antibiotic Medication Shows Effective Prophylaxis against Post-Surgical Wound Infection. Int. Wound J. 2018, 15, 84–89. [Google Scholar] [CrossRef]
- Reiser, M.; Scherag, A.; Forstner, C.; Brunkhorst, F.M.; Harbarth, S.; Doenst, T.; Pletz, M.W.; Hagel, S. Effect of Pre-Operative Octenidine Nasal Ointment and Showering on Surgical Site Infections in Patients Undergoing Cardiac Surgery. J. Hosp. Infect. 2017, 95, 137–143. [Google Scholar] [CrossRef]
- Baier, C.; Ipaktchi, R.; Schwab, F.; Smith, A.; Liu, X.; Ebadi, E.; Limbourg, A.; Mett, T.R.; Bange, F.-C.; Vogt, P.M. Universal Decolonization with Octenidine: First Experiences in a Tertiary Burn Intensive Care Unit. Burns Open 2019, 3, 8–11. [Google Scholar] [CrossRef]
- Bilir, A.; Yelken, B.; Erkan, A. Cholorhexidine, Octenidine or Povidone Iodine for Catheter Related Infections: A Randomized Controlled Trial. J. Res. Med. Sci. 2013, 18, 510–512. [Google Scholar] [CrossRef]
- Denkel, L.A.; Maechler, F.; Schwab, F.; Kola, A.; Weber, A.; Gastmeier, P.; Pfäfflin, F.; Weber, S.; Werner, G.; Pfeifer, Y.; et al. Infections Caused by Extended-Spectrum β-Lactamase-Producing Enterobacterales after Rectal Colonization with ESBL-Producing Escherichia coli or Klebsiella pneumoniae. Clin. Microbiol. Infect. 2020, 26, 1046–1051. [Google Scholar] [CrossRef] [PubMed]
- Dettenkofer, M.; Wilson, C.; Gratwohl, A.; Schmoor, C.; Bertz, H.; Frei, R.; Heim, D.; Luft, D.; Schulz, S.; Widmer, A.F. Skin Disinfection with Octenidine Dihydrochloride for Central Venous Catheter Site Care: A Double-Blind, Randomized, Controlled Trial. Clin. Microbiol. Infect. 2010, 16, 600–606. [Google Scholar] [CrossRef]
- Furtwängler, R.; Laux, C.; Graf, N.; Simon, A. Impact of a Modified Broviac Maintenance Care Bundle on Bloodstream Infections in Paediatric Cancer Patients. GMS Hyg. Infect. Control 2015, 10, Doc15. [Google Scholar] [CrossRef] [PubMed]
- Gastmeier, P.; Kämpf, K.-P.; Behnke, M.; Geffers, C.; Schwab, F. An Observational Study of the Universal Use of Octenidine to Decrease Nosocomial Bloodstream Infections and MDR Organisms. J. Antimicrob. Chemother. 2016, 71, 2569–2576. [Google Scholar] [CrossRef] [PubMed]
- Messler, S.; Klare, I.; Wappler, F.; Werner, G.; Ligges, U.; Sakka, S.G.; Mattner, F. Reduction of Nosocomial Bloodstream Infections and Nosocomial Vancomycin-Resistant Enterococcus faecium on an Intensive Care Unit after Introduction of Antiseptic Octenidine-Based Bathing. J. Hosp. Infect. 2019, 101, 264–271. [Google Scholar] [CrossRef]
- Tietz, A.; Frei, R.; Dangel, M.; Bolliger, D.; Passweg, J.R.; Gratwohl, A.; Widmer, A.E. Octenidine Hydrochloride for the Care of Central Venous Catheter Insertion Sites in Severely Immunocompromised Patients. Infect. Control Hosp. Epidemiol. 2005, 26, 703–707. [Google Scholar] [CrossRef]
- Vogelsang, H.; Lang, A.; Cevik, B.; Botteck, N.M.; Weber, T.P.; Herzog-Niescery, J. Incidence of Infection in Non-Tunnelled Thoracic Epidural Catheters after Major Abdominal Surgery. Acta Anaesthesiol. Scand. 2020, 64, 1312–1318. [Google Scholar] [CrossRef]
- Masuyama, T.; Yasuda, H.; Sanui, M.; Lefor, A.K. Effect of Skin Antiseptic Solutions on the Incidence of Catheter-Related Bloodstream Infection: A Systematic Review and Network Meta-Analysis. J. Hosp. Infect. 2021, 110, 156–164. [Google Scholar] [CrossRef]
- Köck, R.; Becker, K.; Cookson, B.; van Gemert-Pijnen, J.E.; Harbarth, S.; Kluytmans, J.; Mielke, M.; Peters, G.; Skov, R.L.; Struelens, M.J.; et al. Systematic Literature Analysis and Review of Targeted Preventive Measures to Limit Healthcare-Associated Infections by Meticillin-Resistant Staphylococcus aureus. Eurosurveillance 2014, 19, 20860. [Google Scholar] [CrossRef] [PubMed]
- Dittmann, K.; Schmidt, T.; Müller, G.; Cuny, C.; Holtfreter, S.; Troitzsch, D.; Pfaff, P.; Hübner, N.-O. Susceptibility of Livestock-Associated Methicillin-Resistant Staphylococcus aureus (LA-MRSA) to Chlorhexidine Digluconate, Octenidine Dihydrochloride, Polyhexanide, PVP-Iodine and Triclosan in Comparison to Hospital-Acquired MRSA (HA-MRSA) and Community-Aquired MRSA (CA-MRSA): A Standardized Comparison. Antimicrob. Resist. Infect. Control 2019, 8, 122. [Google Scholar] [CrossRef] [PubMed]
- Denkel, L.A.; Schwab, F.; Clausmeyer, J.; Behnke, M.; Golembus, J.; Wolke, S.; Gastmeier, P.; Geffers, C. Central-Line Associated Bloodstream Infections in Intensive Care Units before and after Implementation of Daily Antiseptic Bathing with Chlorhexidine or Octenidine—A Post-Hoc Analysis of a Cluster-Randomised Controlled Trial. Res. Square, 2022; preprint. [Google Scholar] [CrossRef]
- Meißner, A.; Hasenclever, D.; Brosteanu, O.; Chaberny, I.F. EFFECT of Daily Antiseptic Body Wash with Octenidine on Nosocomial Primary Bacteraemia and Nosocomial Multidrug-Resistant Organisms in Intensive Care Units: Design of a Multicentre, Cluster-Randomised, Double-Blind, Cross-over Study. BMJ Open 2017, 7, e016251. [Google Scholar] [CrossRef] [PubMed]
- Schaumburg, T.; Chaberny, I.F.; Kolbe-Busch, S.; Hasenclever, D.; Köhler, N.; Breitenstein, Y. Effect of Daily Antiseptic Body Wash with Octenidine on ICU-Acquired Bacteremia and ICU Acquired Multidrug Resistant Organisms (MDRO) in Intensive Care Units (ICU)—A Multicentre, Cluster-Randomised, Double-Blind, Cross-over Study. In Proceedings of the 74th Annual Meeting of the German Society for Hygiene and Microbiology e.V. (DGHM), Berlin, Germany, 5–7 September 2022. [Google Scholar]
- National Healthcare Safety Network Bloodstream Infection Event (Central Line-Associated Bloodstream Infection and Non-Central Line Associated Bloodstream Infection). Available online: https://www.cdc.gov/nhsn/pdfs/pscmanual/4psc_clabscurrent.pdf (accessed on 26 November 2022).
- Lutz, J.T.; Diener, I.V.; Freiberg, K.; Zillmann, R.; Shah-Hosseini, K.; Seifert, H.; Berger-Schreck, B.; Wisplinghoff, H. Efficacy of Two Antiseptic Regimens on Skin Colonization of Insertion Sites for Two Different Catheter Types: A Randomized, Clinical Trial. Infection 2016, 44, 707–712. [Google Scholar] [CrossRef]
- Ammerlaan, H.S.M.; Kluytmans, J.A.J.W.; Wertheim, H.F.L.; Nouwen, J.L.; Bonten, M.J.M. Eradication of Methicillin-Resistant Staphylococcus aureus Carriage: A Systematic Review. Clin. Infect. Dis. 2009, 48, 922–930. [Google Scholar] [CrossRef] [PubMed]
- Dadashi, M.; Hajikhani, B.; Darban-Sarokhalil, D.; van Belkum, A.; Goudarzi, M. Mupirocin Resistance in Staphylococcus aureus: A Systematic Review and Meta-Analysis. J. Glob. Antimicrob. Resist. 2020, 20, 238–247. [Google Scholar] [CrossRef]


{kind=link}
| Study (Ref.) | Year | Country | Design 1 | Setting 2 | Commercial Support 3 |
|---|---|---|---|---|---|
| Studies using OCT in bundles to prevent S. aureus or MRSA spread and infection among patients with confirmed carriage | |||||
| Allport [19] | 2010–2018 | UK | Retrospective cohort | 1 hospital, orthopedics | ND |
| Aung [20] | 2016–1018 | Singapore | Controlled B/A | 1 hospital, dermatology | ND |
| Buehlmann [21] | 2002–2007 | Switzerland | Noncomparative | 1 UH | ND |
| Chow [22] | 2013–2019 | Singapore | Interrupted time-series | 1 RH | Schülke/Mayr |
| Chow [23] | 2014–2016 | Singapore | Controlled B/A | 1 RH, 2 CH | Schülke/Mayr |
| Danilevicius [24] | 2011–2012 | Lithuania | Noncomparative | 1 UH | Schülke/Mayr |
| Hansen [25] | 1999–2004 | Germany | Noncomparative | 1 TH, medical wards | ND |
| Harris [26] | 2011–2013 | Singapore | Cluster crossover | 1 TH | Schülke/Mayr |
| Kaminski [27] | 2001–2002 | Germany | Noncomparative | 1 TH | ND |
| Pichler [28] | 2016 | Austria | Noncomparative | 1 TH | ND |
| Rengelshausen [29] | unknown | Germany | Noncomparative | 1 hospital, hemodialysis | ND |
| Richter [30] | 2016 | Germany | Noncomparative | 1 UH, 1 neonatal ICU | ND |
| Rohr [31] | 1998–2002 | Germany | Noncomparative | 2 hospitals | Schülke/Mayr |
| Sloot [32] | 1997–1998 | Germany | Noncomparative | 1 hospital | Schülke/Mayr 4 |
| Spencer [33] | 2009–2011 | UK | Retrospective cohort | 1 hospital, 1 ICU | ND |
| Wisgrill [34] | 2011–2016 | Austria | Retrospective cohort | 1 UH, neonatal wards | ND |
| Studies using OCT for pre-incisional antisepsis or universally among patients and assessing the effects on surgical site infections | |||||
| Hachenberg [35] | 2016–2019 | Germany | Retrospective cohort | 1 municipal hospital | ND |
| Jeans [36] | 2007–2014 | UK | Retrospective cohort | 3 hospitals, orthopedics | ND |
| Karl [37] | 2015–2017 | Germany | Prospective cohort | 1 TH, vascular surgery | ND |
| Kohler [38] | 2009–2010 | Switzerland | Controlled B/A | 1 TH | ND |
| Matiasek [39] | 2010–2016 | Austria | Noncomparative | 1 UH, plastic surgery | ND |
| Reiser [40] | 2013–2014 | Germany | Controlled B/A | 1 UH | Schülke/Mayr |
| Studies using OCT universally among defined patients and assessing the effects on ICU-/catheter-related bloodstream and insertion site infections | |||||
| Baier [41] | 2012–2017 | Germany | Retrospective cohort | 1 UH, 1 ICU | ND |
| Bilir [42] | unknown | Turkey | Randomized trial | 1 UH, 1 ICU | ND |
| Denkel [43] | 2017–2018 | Germany | Cluster-randomized controlled trial | 68 hospitals, 72 ICUs | Sage/Stryker, Schülke/Mayr |
| Dettenkofer [44] | 2002–2005 | Switzerland/Germany | Double-blind randomized controlled trial | 2 UH, haematology/surgical unit | Schülke/Mayr |
| Furtwängler [45] | 2009–2013 | Germany | Observational study | 1 UH, paediatric cancer centre | Becton Dickinson |
| Gastmeier [46] | 2013–2015 | Germany | Interrupted time-series | 1 UH, 17 adult ICUs | ND |
| Messler [47] | 2012–2014 | Germany | Before-and-after | 1 UH, 1 surgical ICU | Schülke/Mayr |
| Tietz [48] | 2000–2001 | Switzerland | Noncomparative | 1 UC, bone marrow transplant unit | Schülke/Mayr |
| Vogelsang [49] | 2010–2018 | Germany | Retrospective cohort | 1 UC, anaesthesiology | ND |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Köck, R.; Denkel, L.; Feßler, A.T.; Eicker, R.; Mellmann, A.; Schwarz, S.; Geffers, C.; Hübner, N.-O.; Leistner, R. Clinical Evidence for the Use of Octenidine Dihydrochloride to Prevent Healthcare-Associated Infections and Decrease Staphylococcus aureus Carriage or Transmission—A Review. Pathogens 2023, 12, 612. https://doi.org/10.3390/pathogens12040612
Köck R, Denkel L, Feßler AT, Eicker R, Mellmann A, Schwarz S, Geffers C, Hübner N-O, Leistner R. Clinical Evidence for the Use of Octenidine Dihydrochloride to Prevent Healthcare-Associated Infections and Decrease Staphylococcus aureus Carriage or Transmission—A Review. Pathogens. 2023; 12(4):612. https://doi.org/10.3390/pathogens12040612
Chicago/Turabian StyleKöck, Robin, Luisa Denkel, Andrea T. Feßler, Rudolf Eicker, Alexander Mellmann, Stefan Schwarz, Christine Geffers, Nils-Olaf Hübner, and Rasmus Leistner. 2023. "Clinical Evidence for the Use of Octenidine Dihydrochloride to Prevent Healthcare-Associated Infections and Decrease Staphylococcus aureus Carriage or Transmission—A Review" Pathogens 12, no. 4: 612. https://doi.org/10.3390/pathogens12040612