
Genetic Determinants of Macrolide and Fluoroquinolone Resistance in Mycoplasma genitalium and Their Prevalence in Moscow, Russia
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
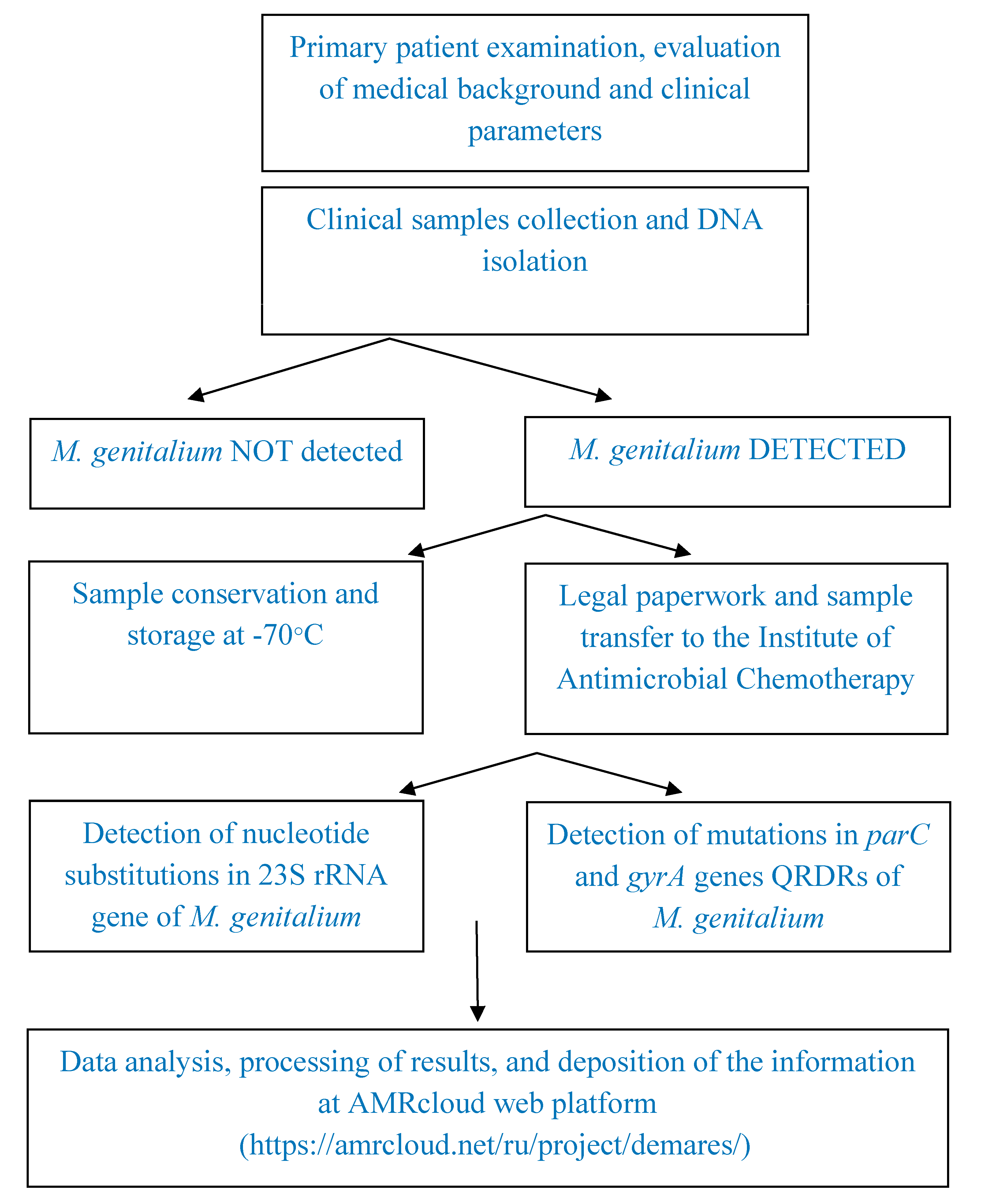
2.1. Experimental Design
2.2. Validation Criteria
2.3. Detection of M. genitalium and Macrolide and Quinolone Resistance
2.4. Statistical Analysis
3. Results
3.1. Specimens Involved in the Investigation
3.2. Main Results of the Investigation
3.3. Additional Results of the Investigation
4. Discussions
5. Limitations of the Investigation
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Health Sector Strategies on, Respectively, HIV, Viral Hepatitis and Sexually Transmitted Infections for the Period 2022–2030. Available online: https://www.who.int/publications/m/item/global-health-sector-strategies-on-respectively--hiv-viral-hepatitis-and-stis-for-2022-2030 (accessed on 9 September 2022).
- Chernova, O.A.; Chernov, V.M.; Mouzykantov, A.A.; Baranova, N.B.; Edelstein, I.A.; Aminov, R.I. Antimicrobial Drug Resistance Mechanisms among Mollicutes. Int. J. Antimicrob. Agents 2021, 57, 106253. [Google Scholar] [CrossRef] [PubMed]
- van der Schalk, T.E.; Braam, J.F.; Kusters, J.G. Molecular Basis of Antimicrobial Resistance in Mycoplasma genitalium. Int. J. Antimicrob. Agents 2020, 55, 105911. [Google Scholar] [CrossRef] [PubMed]
- Shipitsyna, E.; Savicheva, A.; Sokolovskiy, E.; Ballard, R.C.; Domeika, M.; Unemo, M.; Jensen, J.S.; Babayan, K.; Manukyan, E.; Ismailov, R.; et al. Guidelines for the Laboratory Diagnosis of Mycoplasma genitalium Infections in East European Countries. Acta Derm. Venereol. 2010, 90, 461–467. [Google Scholar] [CrossRef] [Green Version]
- Savelieva, G.M.; Sukhikh, G.T.; Serov, V.N. Obstetrics: National Guidelines; GEOTAR-Media: Moscow, Russia, 2022; ISBN 978-5-9704-3365-2. [Google Scholar]
- Savelieva, G.M.; Serov, V.N.; Radzinsky, V.E. Gynecology: National Guidelines; GEOTAR-Media: Moscow, Russia, 2022; ISBN 9785970441527. [Google Scholar]
- Urogenital Diseases Caused by Mycoplasma genitalium. Clinical Guidelines. Available online: https://cr.minzdrav.gov.ru/schema/216_1 (accessed on 9 September 2022).
- Federal Clinical Guidelines. Dermatovenereology 2015; Business Express: Moscow, Russia, 2015; ISBN 978-5-89644-123-6. [Google Scholar]
- Hokynar, K.; Hiltunen-Back, E.; Mannonen, L.; Puolakkainen, M. Prevalence of Mycoplasma Genitalium and Mutations Associated with Macrolide and Fluoroquinolone Resistance in Finland. Int. J. STD AIDS 2018, 29, 904–907. [Google Scholar] [CrossRef]
- Hilmarsdóttir, I.; Arnardóttir, E.M.; Jóhannesdóttir, E.R.; Valsdóttir, F.; Golparian, D.; Hadad, R.; Vigfússon, H.B.; Unemo, M. Prevalence of Mycoplasma Genitalium and Antibiotic Resistance-Associated Mutations in Patients at a Sexually Transmitted Infection Clinic in Iceland, and Comparison of the s-Diamgtv and Aptima Mycoplasma genitalium Assays for Diagnosis. J. Clin. Microbiol. 2020, 58, e01084-20. [Google Scholar] [CrossRef]
- Guschin, A.; Ryzhikh, P.; Rumyantseva, T.; Gomberg, M.; Unemo, M. Treatment Efficacy, Treatment Failures and Selection of Macrolide Resistance in Patients with High Load of Mycoplasma genitalium during Treatment of Male Urethritis with Josamycin. BMC Infect. Dis. 2015, 15, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández-Huerta, M.; Fernández-Huerta, M.; Barberá, M.J.; Barberá, M.J.; Esperalba, J.; Esperalba, J.; Fernandez-Naval, C.; Fernandez-Naval, C.; Vall-Mayans, M.; Vall-Mayans, M.; et al. Prevalence of Mycoplasma genitalium and Macrolide Resistance among Asymptomatic People Visiting a Point of Care Service for Rapid STI Screening: A Cross-Sectional Study. Sex. Transm. Infect. 2020, 96, 300–305. [Google Scholar] [CrossRef]
- Fernández-Huerta, M.; Barberá, M.J.; Serra-Pladevall, J.; Esperalba, J.; Martínez-Gómez, X.; Centeno, C.; Pich, O.Q.; Pumarola, T.; Espasa, M. Mycoplasma genitalium and Antimicrobial Resistance in Europe: A Comprehensive Review. Int. J. STD AIDS 2020, 31, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Hamasuna, R.; Le, P.T.; Kutsuna, S.; Furubayashi, K.; Matsumoto, M.; Ohmagari, N.; Fujimoto, N.; Matsumoto, T.; Jensen, J.S. Mutations in Parc and Gyra of Moxifloxacin-Resistant and Susceptible Mycoplasma genitalium Strains. PLoS ONE 2018, 13, e0198355. [Google Scholar] [CrossRef] [Green Version]
- Hadad, R.; Golparian, D.; Lagos, A.C.; Ljungberg, J.; Nilsson, P.; Jensen, J.S.; Fredlund, H.; Unemo, M. Macrolide and Fluoroquinolone Resistance in Mycoplasma genitalium in Two Swedish Counties, 2011–2015. APMIS 2018, 126, 123–127. [Google Scholar] [CrossRef]
- Gnanadurai, R.; Fifer, H. Mycoplasma genitalium: A Review. Microbiology 2020, 166, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Huerta, M.; Bodiyabadu, K.; Esperalba, J.; Bradshaw, C.S.; Serra-Pladevall, J.; Garland, S.M.; Fernández-Naval, C.; Jensen, J.S.; Pumarola, T.; Ebeyan, S.; et al. Multicenter Clinical Evaluation of a Novel Multiplex Real-Time PCR (QPCR) Assay for Detection of Fluoroquinolone Resistance in Mycoplasma genitalium. J. Clin. Microbiol. 2019, 57, e00886-19. [Google Scholar] [CrossRef] [Green Version]
- Lau, A.; Bradshaw, C.S.; Lewis, D.; Fairley, C.K.; Chen, M.Y.; Kong, F.Y.S.; Hocking, J.S. The Efficacy of Azithromycin for the Treatment of Genital Mycoplasma genitalium: A Systematic Review and Meta-Analysis. Clin. Infect. Dis. 2015, 61, 1389–1399. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Le, W.J.; Li, S.; Cao, Y.P.; Su, X.H. Meta-Analysis of the Efficacy of Moxifloxacin in Treating Mycoplasma genitalium Infection. Int. J. STD AIDS 2017, 28, 1106–1114. [Google Scholar] [CrossRef] [PubMed]
- Kuzmenkov, A.Y.; Vinogradova, A.G.; Trushin, I.V.; Avramenko, A.A.; Edelstein, M.V.; Dekhnich, A.V.; Kozlov, R.S. AMRcloud: A New Paradigm in Monitoring of Antibiotic Resistance. Clin. Microbiol. Antimicrob. Chemother. 2019, 21, 119–124. [Google Scholar] [CrossRef] [Green Version]
- Federal Clinical Recommendations for Patients with Urogenital Diseases Caused by Mycoplasma genitalium. Obstet. Gynecol. 2016, 4, 64–69.
- Sethi, S.; Zaman, K.; Jain, N. Mycoplasma genitalium Infections: Current Treatment Options and Resistance Issues. Infect. Drug Resist. 2017, 10, 283–292. [Google Scholar] [CrossRef] [Green Version]
- Nijhuis, R.H.T.; Severs, T.T.; van der Vegt, D.S.J.M.; Van Zwet, A.A.; Kusters, J.G. High Levels of Macrolide Resistance-Associated Mutations in Mycoplasma genitalium Warrant Antibiotic Susceptibility-Guided Treatment. J. Antimicrob. Chemother. 2015, 70, 2515–2518. [Google Scholar] [CrossRef] [Green Version]
- Kisina, V.I.; Romanova, I.V.; Zhukova, O.V.; Yakovtev, S.V. Comparative Analysis of Modern Approaches to the Treatment of m. Genitalium Infection in Clinical Practice. Antibiot. I Khimioterapiya 2019, 64, 31–37. [Google Scholar] [CrossRef]
- Machalek, D.A.; Tao, Y.; Shilling, H.; Jensen, J.S.; Unemo, M.; Murray, G.; Chow, E.P.F.; Low, N.; Garland, S.M.; Vodstrcil, L.A.; et al. Prevalence of mutations associated with resistance to macrolides and fluoroquinolones in Mycoplasma genitalium: A systematic review and meta-analysis. Lancet Infect. Dis. 2020, 20, 1302–1314. [Google Scholar] [CrossRef]
- Murray, G.L.; Bradshaw, C.S.; Bissessor, M.; Danielewski, J.; Garland, S.M.; Jensen, J.S.; Fairley, C.K.; Tabrizi, S.N. Increasing Macrolide and Fluoroquinolone Resistance in Mycoplasma genitalium. Emerg. Infect. Dis. 2017, 23, 809–812. [Google Scholar] [CrossRef]
- Bodiyabadu, K.; Danielewski, J.; Garland, S.M.; Machalek, D.A.; Bradshaw, C.S.; Birnie, J.; Ebeyan, S.; Lundgren, M.; Murray, G. Detection of ParC Gene Mutations Associated with Quinolone Resistance in Mycoplasma genitalium: Evaluation of a Multiplex Real-Time PCR Assay. J. Med. Microbiol. 2021, 70, 001257. [Google Scholar] [CrossRef]
- Le Roy, C.; Hénin, N.; Pereyre, S.; Bébéar, C. Fluoroquinolone-Resistant Mycoplasma Genitalium, Southwestern France. Emerg. Infect. Dis. 2016, 22, 1677–1679. [Google Scholar] [CrossRef] [Green Version]
- Shimada, Y.; Deguchi, T.; Nakane, K.; Masue, T.; Yasuda, M.; Yokoi, S.; Ito, S.; Nakano, M.; Ito, S.; Ishiko, H. Emergence of Clinical Strains of Mycoplasma genitalium Harbouring Alterations in ParC Associated with Fluoroquinolone Resistance. Int. J. Antimicrob. Agents 2010, 36, 255–258. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, M.; Maeda, S.; Deguchi, T. In Vitro Activity of Fluoroquinolones against Mycoplasma genitalium and Their Bacteriological Efficacy for Treatment of m. Genitalium-Positive Nongonococcal Urethritis in Men. Clin. Infect. Dis. 2005, 41, 1357–1359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maeda, S.I.; Tamaki, M.; Kojima, K.; Yoshida, T.; Ishiko, H.; Yasuda, M.; Deguchi, T. Association of Mycoplasma genitalium Persistence in the Urethra with Recurrence of Nongonococcal Urethritis. Sex. Transm. Dis. 2001, 28, 472–476. [Google Scholar] [CrossRef]
- Jernberg, E.; Moghaddam, A.; Moi, H. Azithromycin and Moxifloxacin for Microbiological Cure of Mycoplasma genitalium Infection: An Open Study. Int. J. STD AIDS 2008, 19, 676–679. [Google Scholar] [CrossRef]
- Potekaev, N.N.; Dolja, O.V.; Zukova, O.V.; Kisina, V.I.; Guschin, A.E.; Gomberg, M.A.; Frigo, N.V.; Zabirov, K.I.; Kovalyk, V.P.; Romanova, I.V.; et al. Department of Health of the Moscow City. Urogenital Diseases, caused by Mycoplasma genitalium. 4–20. Clinical Guidelines. 2021. Available online: https://mosgorzdrav.ru (accessed on 9 September 2022).
- Hooper, D.C.; Jacoby, G.A. Mechanisms of Drug Resistance: Quinolone Resistance. Ann. N. Y. Acad. Sci. 2015, 1354, 12–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Redgrave, L.S.; Sutton, S.B.; Webber, M.A.; Piddock, L.J.V. Fluoroquinolone Resistance: Mechanisms, Impact on Bacteria, and Role in Evolutionary Success. Trends Microbiol. 2014, 22, 438–445. [Google Scholar] [CrossRef]
- Shipitsyna, E.; Rumyantseva, T.; Golparian, D.; Khayrullina, G.; Lagos, A.C.; Edelstein, I.; Joers, K.; Jensen, J.S.; Savicheva, A.; Rudneva, N.; et al. Prevalence of Macrolide and Fluoroquinolone Resistance-Mediating Mutations in Mycoplasma genitalium in Five Cities in Russia and Estonia. PLoS ONE 2017, 12, e0175763. [Google Scholar] [CrossRef] [Green Version]
- Shedko, E.D.; Khayrullina, G.A.; Goloveshkina, E.N.; Akimkin, V.G. Clinical Evaluation of Commercial PCR Assays for Antimicrobal Resistance in Mycoplasma genitalium and Estimation of Resistance-Mediated Mutation Prevalence in Moscow and Moscow Region. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 1413–1418. [Google Scholar] [CrossRef] [PubMed]
- Rachina, S.A.; Kozlov, R.S.; Kurkova, A.A.; Portnyagina, U.S.; Palyutin, S.C.; Khokhlov, A.L.; Reshetko, O.V.; Zhuravleva, M.V.; Palagin, I.S. On Behalf Of Russian Working Group Of The Project. Antimicrobial Dispensing Practice in Community Pharmacies in Russia during the COVID-19 Pandemic. Antibiotics 2022, 11, 586. [Google Scholar] [CrossRef] [PubMed]
- Fookes, M.C.; Hadfield, J.; Harris, S.R.; Parmar, S.; Unemo, M.; Jensen, J.S.; Thomson, N.R. Mycoplasma genitalium: Whole genome sequence analysis, recombination and population structure. BMC Genom. 2017, 18, 993. [Google Scholar] [CrossRef] [PubMed]
- Tyulenev, Y.A.; Guschin, A.E.; Kisina, V.I. Localization Features of Sexually Transmitted Infections in Subjectively Asymptomatic Men Who Have Sex with Men. Klin. Dermatol. I Venerol. 2021, 20, 55–61. [Google Scholar] [CrossRef]
- Tyulenev, Y.A.; Guschin, A.E. Sexually Transmitted Infections in Asymptomatic Men Who Have Sex with Men. Klin. Dermatol. I Venerol. 2020, 19, 802–808. [Google Scholar] [CrossRef]


{kind=link}
| Primer Name | Primer Sequence, 5′-3′ |
|---|---|
| Mpg gyrA SeqF | CCTGATGCTAGAGATGGACTTAAACC |
| Mpg gyrA SeqR | TAATCTTGCTTCTGTATAACGTTGTGC |
| Mpg parC SeqF Mpg parC SeqR | GTCTTTGCAGTTAGCTTTAGTAAGTATGC CTCGCACCATTGATAAAGAGGTTAGG |
| Mpg 23s SeqF Mpg 23s SeqR | CGTCCCGCTTGAATGGTGTAAC GCGCTACAACTGGAGCATAAG |
| 23S rRNA Gene of M. genitalium | N = 213 | % | 95% CI |
|---|---|---|---|
| Wild-type (S) | 158 | 74.2 | 67.9–79.6% |
| Mutations (R) | 55 | 25.8 | 20.4–32.1% |
| A2059G | 36 | 65.5 | 52.3–77% |
| A2058G | 19 | 34,6 | 23.4–47.8% |
| parC gene | N = 213 | % | 95% CI |
| Wild-type (S) | 176 | 82.6 | 77–87.1% |
| Mutations (R) | 37 | 17.4 | 12.9–23.1% |
| D84N (Asp87Asn) a | 20 | 54.1 | 38.4–69% |
| S80I (Ser83Ile) | 12 | 32.4 | 19.6–49% |
| S80N (Ser83Asn) | 3 | 8.1 | 2.8–21.3% |
| D84G (Asp87Gly) | 1 | 2.7 | 0.5–14% |
| D84Y (Asp87Tyr) | 1 | 2.7 | 0.5–14% |
| parC+23S rRNA gene | 15 | 7.1 | 4.3–11.3% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Edelstein, I.A.; Guschin, A.E.; Romanov, A.V.; Negasheva, E.S.; Kozlov, R.S. Genetic Determinants of Macrolide and Fluoroquinolone Resistance in Mycoplasma genitalium and Their Prevalence in Moscow, Russia. Pathogens 2023, 12, 496. https://doi.org/10.3390/pathogens12030496
Edelstein IA, Guschin AE, Romanov AV, Negasheva ES, Kozlov RS. Genetic Determinants of Macrolide and Fluoroquinolone Resistance in Mycoplasma genitalium and Their Prevalence in Moscow, Russia. Pathogens. 2023; 12(3):496. https://doi.org/10.3390/pathogens12030496
Chicago/Turabian StyleEdelstein, Inna Alexandrovna, Alexandr Evgenjevich Guschin, Andrew Vyacheslavovich Romanov, Ekaterina Sergeevna Negasheva, and Roman Sergeevich Kozlov. 2023. "Genetic Determinants of Macrolide and Fluoroquinolone Resistance in Mycoplasma genitalium and Their Prevalence in Moscow, Russia" Pathogens 12, no. 3: 496. https://doi.org/10.3390/pathogens12030496