

Monitoring the Status of Soil-Transmitted Helminthiases in Non-Endemic Implementation Units: A Case Study of Borgu in Northcentral Nigeria
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Statement and Considerations
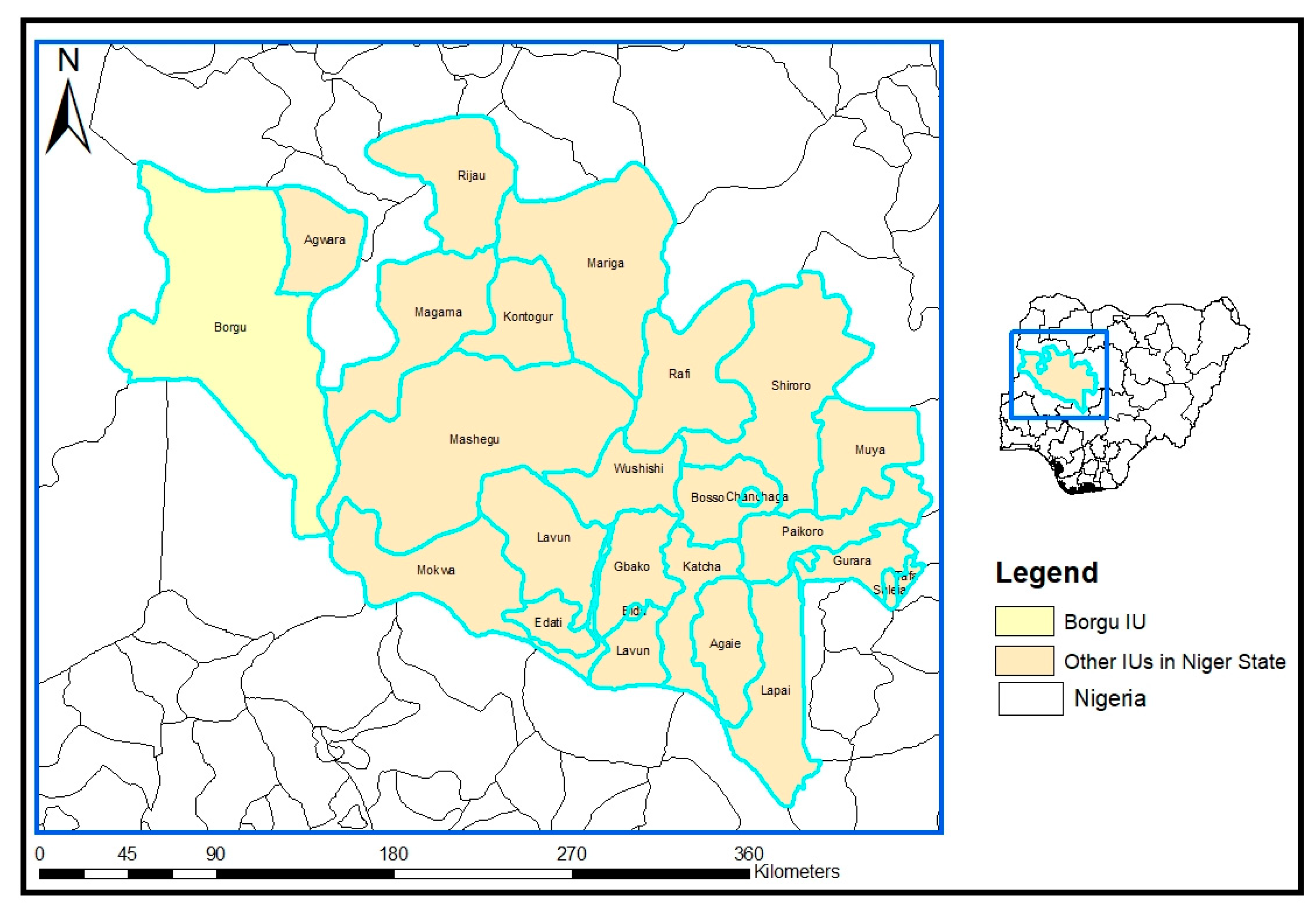
2.2. Study Area
2.3. Study Design
2.4. Selection of Communities
2.5. Sample Size Determination and Selection of Study Participants
2.6. Questionnaire Administration
2.7. Collection of Stool Samples
2.8. Parasitological Assessment of Stool Samples
2.9. Data Management and Analysis
3. Results
3.1. Demographic Characteristics of Study Participants
3.2. Prevalence and Intensity of Soil-Transmitted Helminths among the Study Participants
3.3. Association between Soil-Transmitted Helminths and Other Sociodemographic Variables
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Ascaris lumbricoides Model | Hookworm Model | |||||||
|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | p-Value | AOR (95% CI) | p-Value | OR (95% CI) | p-Value | AOR (95% CI) | p-Value | |
| Communities | ||||||||
| Monai | REF | - | REF | - | REF | - | REF | - |
| Tamanai | 2.59 (0.42–20) | 0.3 | 3.65 (0.34–43) | 0.28 | 3.14 (0.92–11) | 0.08 | 3.09 (0.64–16) | 0.16 |
| Koro | 6.38 (1.67–41.8) | 0.02 | 3.39 (0.6–27) | 0.19 | 1.93 (0.57–7.52) | 0.3 | 2.13 (0.49–9.9) | 0.31 |
| Musawa | - | - | - | - | 1.9 (0.26–11) | 0.47 | 5.03 (0.46–51) | 0.16 |
| Yuna | - | - | - | - | - | - | - | - |
| Gender | ||||||||
| Male | REF | - | REF | - | REF | - | REF | - |
| Female | 0.55 (0.03–0.1) | 0.25 | 0.54 (0.17–1.7) | 0.29 | 0.89 (0.36–2.25) | 0.79 | 0.92 (0.33–2.55) | 0.87 |
| Age group in years | ||||||||
| Age (6–8) | REF | - | REF | - | REF | - | REF | - |
| Age (9–11) | 1.75 (0.52–6.21) | 0.36 | 1.13 (0.28–4.8) | 0.87 | 2.99 (0.92–11) | 0.08 | 2.3 (0.62–9.6) | 0.22 |
| Age (12–14) | 1.25 (0.3–4.81) | 0.75 | 0.6 (0.12–2.8) | 0.53 | 3.25 (1.0–12) | 0.06 | 2.79 (0.74–12) | 0.14 |
| Age (15–17) | 3.3 (0.16–23.2) | 0.30 | 1.48 (0.06–14) | 0.75 | - | - | - | - |
| Parental occupation | ||||||||
| Farming | REF | - | REF | - | REF | - | REF | - |
| Fishing | - | - | - | - | 0.55 (0.03–3.54) | 0.59 | 0.7 (003–6.4) | 0.78 |
| Civil servant | 1.22 (0.28–5.3) | 0.78 | 1.45 (0.31–6.9) | 0.63 | 2.27 (0.76–7.57) | 0.15 | 2.51 (0.72–10) | 0.17 |
| Trading | 4.18 (0.52–2.0) | 0.07 | 3.22 (0.53–19) | 0.18 | 3.32 (0.65–14) | 0.11 | 2.51 (0.44–13) | 0.28 |
| Artisan | 4.53 (0.52–2.5) | 0.1 | 4.37 (0.49–32) | 0.15 | 1.69 (0.09–11) | 0.64 | 1.11 (0.05–8.98) | 0.93 |
| Miner | 4.18 (0.52–2.0) | 0.07 | 2.09 (0.34–12) | 0.4 | 1.03 (0.05–6.7) | 0.98 | 1.18 (0.05–10) | 0.89 |
| Driver | - | - | - | - | - | - | - | - |
| Access to latrine | ||||||||
| Yes | REF | - | REF | - | REF | - | REF | - |
| No | 1.97 (0.62–8.69) | 0.30 | 3.99 (0.94–22) | 0.08 | 1.04 (0.41–2.99) | 0.94 | 2.89 (0.85–11) | 0.1 |
| Walking barefoot | ||||||||
| Yes | REF | - | REF | - | REF | - | REF | - |
| No | 0.39 (0.12–1.08) | 0.08 | 0.35 (0.09–1.2) | 0.1 | 2.13 (0.83–6.11) | 0.13 | 2.17 (0.66–7.98) | 0.21 |
References
- Hotez, P.J.; Kamath, A. Neglected Tropical Diseases in Sub-Saharan Africa: Review of Their Prevalence, Distribution, and Disease Burden. PLoS Negl. Trop. Dis. 2009, 3, e412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Ending the Neglect to Attain the Sustainable Development Goals: A Road Map for Neglected Tropical Diseases 2021–2030; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- World Health Organization. Soil Transmitted Helminthiasis. Fact Sheet. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/soil-transmitted-helminth-infections (accessed on 3 February 2022).
- Grantham-McGregor, S.; Ani, C. A Review of Studies on the Effect of Iron Deficiency on Cognitive Development in Children. J. Nutr. 2001, 131, S649–S668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ezeamama, A.E.; Friedman, J.F.; Acosta, L.P.; Bellinger, D.C.; Langdon, G.C.; Manalo, D.L.; Olveda, R.M.; Kurtis, J.D.; McGarvey, S.T. Helminth infection and cognitive impairment among Filipino children. Am. J. Trop. Med. Hygiene 2005, 72, 540–548. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Helminth Control in School-Age Children: A Guide for Managers of Control Programmes. 2011. Available online: https://www.who.int/neglected_diseases/resources/9789241548267/en/ (accessed on 15 April 2021).
- Montresor, A.; Mupfasoni, D.; Mikhailov, A.; Mwinzi, P.; Lucianez, A.; Jamsheed, M.; Gasimov, E.; Warusavithana, S.; Yajima, A.; Bisoffi, Z.; et al. The global progress of soil-transmitted helminthiases control in 2020 and World Health Organization targets for 2023. PLoS Neglected Trop. Dis. 2020, 14, e0008505. [Google Scholar] [CrossRef]
- World Health Organization. Eliminating Soil-Transmitted Helminthiases as a Public Health Problem in Children. Progress Report 2001–2010 and Strategic Plan 2011-World Health Organization, Geneva. 2012. Available online: https://apps.who.int/iris/bitstream/handle/10665/44804/9789241503129_eng.pdf (accessed on 5 April 2022).
- Hotez, P.J.; Asojo, O.; Adesina, A.M. Nigeria: “Ground Zero” for the High Prevalence Neglected Tropical Diseases. PLoS Neglected Trop. Dis. 2012, 6, e1600. [Google Scholar] [CrossRef] [PubMed]
- Expanded Special Project for Elimination of Neglected Tropical Diseases (ESPEN). 2022. Available online: https://espen.afro.who.int/countries/nigeria (accessed on 15 January 2023).
- Federal Ministry of Health (FMOH), Neglected Tropical Diseasea Master Plan 2015. 2020. Available online: https://espen.afro.who.int/system/files/content/resources/NIGERIA_NTD_Master_Plan_2015_2020.pdf (accessed on 15 January 2023).
- Adewale, B.; Rahman, O.; Sulyman, M.; Uwalaka, C.; Ajayi, M. Status of Schistosoma haematobium Infection among Pupils around the Kainji Dam, Niger State: A Paradigm Shift in Infection Rate. Niger. J. Parasitol. 2020, 41. [Google Scholar] [CrossRef]
- Montresor, A.; Crompton, D.W.T.; Hall, A.; Bundy, D.A.P.; Savioli, L. Guidelines for the Evaluation of soil-Transmitted Hel-Minthiasis and Schistosomiasis at Community Level: A guide for Managers of Control Programmes. World Health Organization. 1998. Available online: https://apps.who.int/iris/handle/10665/63821 (accessed on 15 January 2023).
- Federal Ministry of Health (FMOH). National Protocol for Integrated Epidemiological Mapping and Baseline Survey for Schis-Tosomiasis and Soil Transmitted Helminthiasis. Available online: https://www.health.gov.ng/doc/PROTOCOL-FOR-SCHISTO-STH-MAPPING-1.pdf (accessed on 31 December 2022).
- Olamiju, F.; Nebe, O.J.; Mogaji, H.; Marcus, A.; Amodu–Agbi, P.; Urude, R.O.; Apake, E.; Olamiju, O.; Okoronkwo, C.; Achu, I.; et al. Schistosomiasis outbreak during COVID-19 pandemic in Takum, Northeast Nigeria: Analysis of infection status and associated risk factors. PLoS ONE 2022, 17, e0262524. [Google Scholar] [CrossRef]
- Mission to Save the Helpless (MITOSATH); Epidemiological Mapping Survey Report in Niger State, Nigeria. Unpublished Data.
- Nduka, F.; Nebe, O.; Njepuome, N.; Dakul, D.; Anagbogu, I.; Ngege, E.; Jacob, S.; Nwoye, I.; Nwankwo, U.; Urude, R.; et al. Epidemiological mapping of schistosomiasis and soil-transmitted helminthiasis for intervention strategies in Nigeria. Niger. J. Parasitol. 2019, 40, 218–225. [Google Scholar] [CrossRef]
- Avokpaho, E.F.G.A.; Houngbégnon, P.; Accrombessi, M.; Atindégla, E.; Yard, E.; Means, A.R.; Kennedy, D.S.; Littlewood, D.T.J.; Garcia, A.; Massougbodji, A.; et al. Factors associated with soil-transmitted helminths infection in Benin: Findings from the DeWorm3 study. PLoS Neglected Trop. Dis. 2021, 15, e0009646. [Google Scholar] [CrossRef]
- Agustina, K.K.; Wirawan, I.M.A.; Sudarmaja, I.M.; Subrata, M.; Dharmawan, N.S. The first report on the prevalence of soil-transmitted helminth infections and associated risk factors among traditional pig farmers in Bali Province, Indonesia. Veter.-World 2022, 15, 1154–1162. [Google Scholar] [CrossRef]
- Douglas, K.; Amadi, C. Soil transmitted helminth infection among farmers in ukwa west local government area, Abia state, South-East, Nigeria. Niger. J. Med. 2016, 25, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Campbell, S.J.; Savage, G.B.; Gray, D.J.; Atkinson, J.-A.M.; Magalhães, R.J.S.; Nery, S.V.; McCarthy, J.S.; Velleman, Y.; Wicken, J.H.; Traub, R.J.; et al. Water, Sanitation, and Hygiene (WASH): A Critical Component for Sustainable Soil-Transmitted Helminth and Schistosomiasis Control. PLoS Neglected Trop. Dis. 2014, 8, e2651. [Google Scholar] [CrossRef] [Green Version]
- Mogaji, H.; Dedeke, G.; Jaiyeola, O.; Adeniran, A.; Olabinke, D.; Oluwole, A.; Abe, E.; Adeaga, D.; Yusuff, Q.; Ekpo, U. A preliminary survey of school-based water, sanitation, hygiene (WASH) resources and soil-transmitted helminthiasis in eight public schools in Odeda LGA, Ogun State, Nigeria. Parasitol. Open 2017, 3, e16. [Google Scholar] [CrossRef] [Green Version]
- Anderson, R.; Truscott, J.; Hollingsworth, T.D. The coverage and frequency of mass drug administration required to eliminate persistent transmission of soil-transmitted helminths. Philos. Trans. R. Soc. B Biol. Sci. 2014, 369, 20130435. [Google Scholar] [CrossRef] [Green Version]
- Clarke, N.E.; Clements, A.C.A.; Doi, S.A.; Wang, D.; Campbell, S.J.; Gray, D.; Nery, S.V. Differential effect of mass deworming and targeted deworming for soil-transmitted helminth control in children: A systematic review and meta analysis. Lancet 2017, 389, 287–297. [Google Scholar] [CrossRef] [PubMed]
- Dunn, J.C.; Bettis, A.A.; Wyine, N.Y.; Lwin, A.M.M.; Lwin, S.T.; Su, K.K.; Sein, M.M.; Tun, A.; Maung, N.S.; Anderson, R.M. A cross-sectional survey of soil-transmitted helminthiases in two Myanmar villages receiving mass drug administration: Epidemiology of infection with a focus on adults. Parasites Vectors 2017, 10, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molyneux, D.H. The London Declaration on Neglected Tropical Diseases: 5 years on. Trans. R. Soc. Trop. Med. Hyg. 2017, 110, 623–625. [Google Scholar] [CrossRef] [Green Version]
- Mogaji, H.O.; Dedeke, G.A.; Bada, B.S.; Bankole, S.; Adeniji, A.; Fagbenro, M.T.; Omitola, O.O.; Oluwole, A.S.; Odoemene, N.S.; Abe, E.M.; et al. Distribution of ascariasis, trichuriasis and hookworm infections in Ogun State, Southwestern Nigeria. PLoS ONE 2020, 15, e0233423. [Google Scholar] [CrossRef]
- Shenoy, R.K.; Bockarie, M.J. Lymphatic filariasis in children: Clinical features, infection burdens and future prospects for elimination. Parasitology 2011, 138, 1559–1568. [Google Scholar] [CrossRef] [Green Version]
- Padmasiri, E.; Montresor, A.; Biswas, G.; De Silva, N. Controlling lymphatic filariasis and soil-transmitted helminthiasis together in South Asia: Opportunities and challenges. Trans. R. Soc. Trop. Med. Hyg. 2006, 100, 807–810. [Google Scholar] [CrossRef] [Green Version]
- Eneanya, O.A.; Gankpala, L.; Goss, C.W.; Bolay, F.K.; Weil, G.J.; Fischer, P.U. Impact of Annual versus Semiannual Mass Drug Administration with Ivermectin and Albendazole on Helminth Infections in Southeastern Liberia. Am. J. Trop. Med. Hyg. 2021, 106, 700–709. [Google Scholar] [CrossRef] [PubMed]
- Bassey, D.B.; Mogaji, H.O.; Dedeke, G.A.; Akeredolu-Ale, B.I.; Abe, E.M.; Oluwole, A.S.; Adeniran, A.A.; Agboola, O.A.; Mafiana, C.F.; Ekpo, U.F. The impact of Worms and Ladders, an innovative health educational board game on Soil-Transmitted Helminthiasis control in Abeokuta, Southwest Nigeria. PLoS Neglected Trop. Dis. 2020, 14, e0008486. [Google Scholar] [CrossRef] [PubMed]
- Bieri, F.A.; Gray, D.J.; Williams, G.M.; Raso, G.; Li, Y.-S.; Yuan, L.; He, Y.; Li, R.S.; Guo, F.-Y.; Li, S.-M.; et al. Health-Education Package to Prevent Worm Infections in Chinese Schoolchildren. N. Engl. J. Med. 2013, 368, 1603–1612. [Google Scholar] [CrossRef] [PubMed] [Green Version]

| Communities | |||||||
|---|---|---|---|---|---|---|---|
| Monai (n = 133) | Tamanai (n = 79) | Koro (n = 124) | Musawa (n = 36) | Yuna (n = 38) | Total (n = 410) | p-Value | |
| Sex | |||||||
| Female | 56 (42.1) | 41 (51.9) | 56 (45.2) | 16 (44.4) | 7 (10.5) | 173 (42.2) | 0.000 |
| Male | 77 (57.9) | 38 (48.1) | 68 (54.8) | 20 (55.6) | 34 (89.5) | 237 (57.8) | |
| Age group in years | |||||||
| 6–8 | 95 (71.4) | 5 (6.3) | 41 (33.1) | 22 (61.1) | 7 (18.4) | 170 (41.5) | 0.001 |
| 9–11 | 18 (13.5) | 43 (54.4) | 38 (30.6) | 14 (38.9) | 6 (15.8) | 119 (29.0) | |
| 12–14 | 20 (15.0) | 26 (32.9) | 39 (31.5) | 0 (0) | 25 (65.8) | 110 (26.8) | |
| 15–17 | 0 (0) | 5 (6.3) | 6 (4.8) | 0 (0) | 0 (0) | 11 (2.7) | |
| Parent’s occupation | |||||||
| Farming | 49 (36.8) | 20 (25.3) | 39 (31.5) | 20 (55.6) | 21 (55.3) | 149 (36.3) | 0.001 |
| Fishing | 18 (13.5) | 0 (0) | 2 (1.6) | 16 (44.4) | 17 (44.7) | 53 (12.9) | |
| Civil servant | 62 (46.6) | 29 (36.7) | 32 (25.8) | 0 (0) | 0 (0) | 123 (30.0) | |
| Trading | 1 (0.8) | 15 (19.0) | 13 (10.5) | 0 (0) | 0 (0) | 29 (7.1) | |
| Artisan | 0 (0) | 12 (15.2) | 6 (4.8) | 0 (0) | 0 (0) | 18 (4.4) | |
| Miner | 0 (0) | 0 (0) | 29 (23.4) | 0 (00 | 0 (00 | 29 (7.1) | |
| Driver | 3 (2.3) | 3 (3.8) | 3 (2.4) | 0 (0) | 0 (0) | 9 (2.2) | |
| Access to latrine | |||||||
| Yes | 29 (21.8) | 59 (74.7) | 38 (30.6) | 0 (0) | 0 (0) | 126 (30.7) | 0.001 |
| No | 104 (78.2) | 20 (25.3) | 86 (69.4) | 36 (100) | 38 (100) | 284 (69.3) | |
| Walking barefoot | |||||||
| Yes | 46 (34.6) | 11 (13.9) | 73 (58.9) | 34 (94.4) | 28 (73.7) | 192 (46.8) | 0.001 |
| No | 87 (65.4) | 68 (86.1) | 51 (41.1) | 2 (5.6) | 10 (26.3) | 218 (53.2) | |
| Overall STH | A. lumbricoides | Hookworm | ||||
|---|---|---|---|---|---|---|
| Communities | NE | NI (%) | NI (%) | Mean EPG ± SD (Min, Max) | NI (%) | Mean EPG ± SD (Min-Max) |
| Monai | 133 | 6 (4.5) | 2 (1.5) | 48 ± 33.94 (24, 72) | 4 (3.0) | 630 ± 421.37 (24, 960) |
| Tamanai | 79 | 10 (12.7) | 3 (3.8) | 40 ± 13.86 (24, 48) | 7 (8.9) | 572.57 ± 383.36 (240, 1344) |
| Koro | 124 | 18 (14.5) | 11 (8.9) | 39.27 ± 16.18 (24, 72) | 7 (5.6) | 250.29 ± 287.28 (24, 840) |
| Musawa | 36 | 2 (5.6) | - | - | 2 (5.6) | 48 ± 0.0 (0, 48) |
| Yuna | 38 | 0 (0) | - | - | 0 (0) | - |
| Total | 410 | 36 (8.8) | 16 (3.9) | 40 ± 17.0 (24, 72) | 20 (4.9) | 419 ± 379 (24, 1344) |
| Covariates | Frequency (%) | Positives (%) | Negatives (%) | p-Value | OR (95% CI) | p-Value | AOR (95% CI) | p-Value |
|---|---|---|---|---|---|---|---|---|
| n = 410 | n = 36 (8.8) | n = 374 (91.2) | ||||||
| Communities | ||||||||
| Monai | 133 (32.4) | 6 (4.5) | 127 (95.5) | 0.008 * | REF | - | REF | - |
| Tamanai | 79 (19.3) | 10 (12.7) | 69 (87.3) | 0.33 (0.11–0.92) | 0.04 * | 0.59 (0.16–2.03) | 0.41 | |
| Koro | 124 (30.2) | 18 (14.5) | 106 (85.5) | 0.28 (0.1–0.69) | 0.01 * | 0.39 (9.12–1.14) | 0.09 | |
| Musawa | 36 (8.8) | 2 (5.6) | 34 (94.4) | 0.8 (0.18–5.65) | 0.79 | 0.53 (0.09–4.26) | 0.5 | |
| Yuna | 38 (9.3) | 0 (0) | 38 (100) | - | - | - | - | |
| Gender | ||||||||
| Male | 173 (42.2) | 18 (7.6) | 155 (89.6) | 0.41 | REF | - | - | - |
| Female | 237 (57.8) | 18 (10.4) | 219 (92.4) | 1.41 (0.71–2.82) | 0.32 | - | - | |
| Age group in years | ||||||||
| Age (6–8) | 170 (41.5) | 9 (5.3) | 161 (94.7) | 0.21 | REF | - | REF | - |
| Age (9–11) | 119 (29.0) | 14 (11.8) | 105 (88.2) | 0.42 (0.17–0.99) | 0.05 * | 0.56 (0.21–1.5) | 0.25 | |
| Age (12–14) | 110 (26.8) | 12 (10.9) | 98 (89.1) | 0.46 (0.18–1.12) | 0.09 | 0.54 (0.19–1.45) | 0.22 | |
| Age (15–17) | 11 (2.7) | 1 (9.1) | 10 (90.9) | 0.56 (0.09–10.8) | 0.60 | 0.93 (0.13–19.1) | 0.95 | |
| Parental occupation | ||||||||
| Farming | 149 (36.3) | 9 (6.0) | 140 (94.0) | 0.038 * | REF | - | REF | - |
| Fishing | 53 (12.9) | 1 (1.9) | 52 (98.1) | 3.34 (0.61–62.4) | 0.26 | 2.13 (0.31–43.2) | 0.51 | |
| Civil servant | 123 (30.0) | 13 (10.6) | 110 (89.4) | 0.54 (0.22–1.31) | 0.18 | 0.61 (0.23–1.56) | 0.31 | |
| Trading | 29 (7.1) | 6 (20.7) | 23 (79.3) | 0.25 (0.08–0.79) | 0.01 * | 0.41 (0.12–1.41) | 0.14 | |
| Artisan | 18 (4.4) | 3 (16.7) | 15 (83.3) | 0.32 (0.08–1.56) | 0.11 | 0.54 (0.13–2.82) | 0.42 | |
| Miner | 29 (7.1) | 4 (13.8) | 25 (86.2) | 0.4 (0.12–1.57) | 0.15 | 0.74 (0.19–3.12) | 0.66 | |
| Driver | 9 (2.2) | 0 (0) | 9 (100) | - | - | - | - | |
| Access to latrine | ||||||||
| Yes | 126 (30.7) | 9 (7.1) | 117 (92.9) | 0.55 | REF | - | - | - |
| No | 284 (69.3) | 27 (9.5) | 257 (90.5) | 0.73 (0.32–1.55) | 0.44 | - | - | |
| Walking barefoot | ||||||||
| Yes | 192 (46.8) | 17 (8.9) | 175 (91.1) | 0.99 | REF | - | - | - |
| No | 218 (53.2) | 19 (8.7) | 199 (91.3) | 1.02 (0.51–2.02) | 0.96 | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adewale, B.; Mogaji, H.; Balogun, J.; Balogun, E.; Olamiju, F.; Herbert, D. Monitoring the Status of Soil-Transmitted Helminthiases in Non-Endemic Implementation Units: A Case Study of Borgu in Northcentral Nigeria. Pathogens 2023, 12, 491. https://doi.org/10.3390/pathogens12030491
Adewale B, Mogaji H, Balogun J, Balogun E, Olamiju F, Herbert D. Monitoring the Status of Soil-Transmitted Helminthiases in Non-Endemic Implementation Units: A Case Study of Borgu in Northcentral Nigeria. Pathogens. 2023; 12(3):491. https://doi.org/10.3390/pathogens12030491
Chicago/Turabian StyleAdewale, Babatunde, Hammed Mogaji, Joshua Balogun, Emmanuel Balogun, Francisca Olamiju, and De’Broski Herbert. 2023. "Monitoring the Status of Soil-Transmitted Helminthiases in Non-Endemic Implementation Units: A Case Study of Borgu in Northcentral Nigeria" Pathogens 12, no. 3: 491. https://doi.org/10.3390/pathogens12030491