
Prescription of Rifampicin for Staphylococcus aureus Infections Increased the Incidence of Corynebacterium striatum with Decreased Susceptibility to Rifampicin in a Hungarian Clinical Center

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Calculating Antibiotic Resistance Index
2.3. Strain Typing with IR Biotyper® (IRBT)
2.4. Data Analysis
3. Results
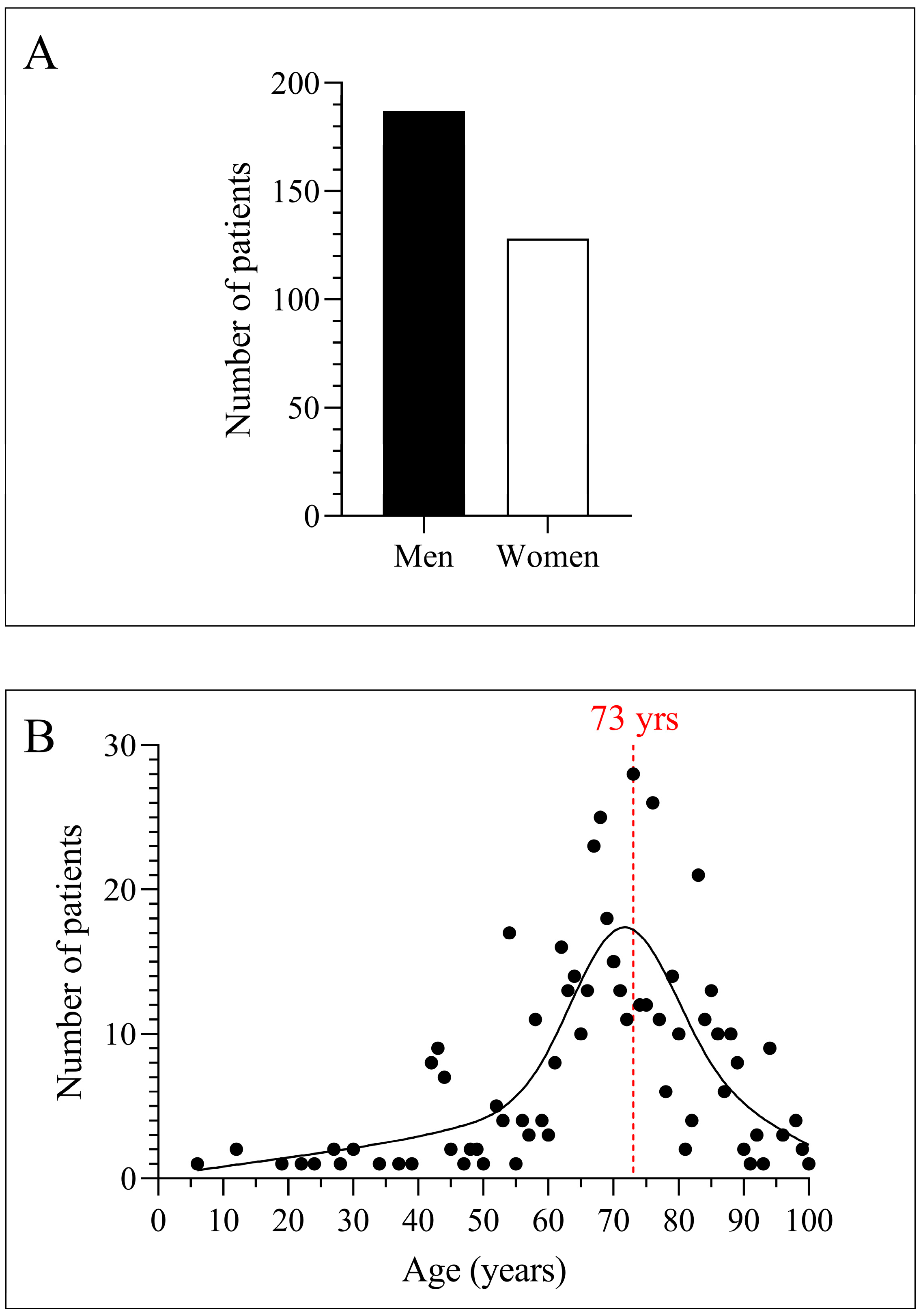
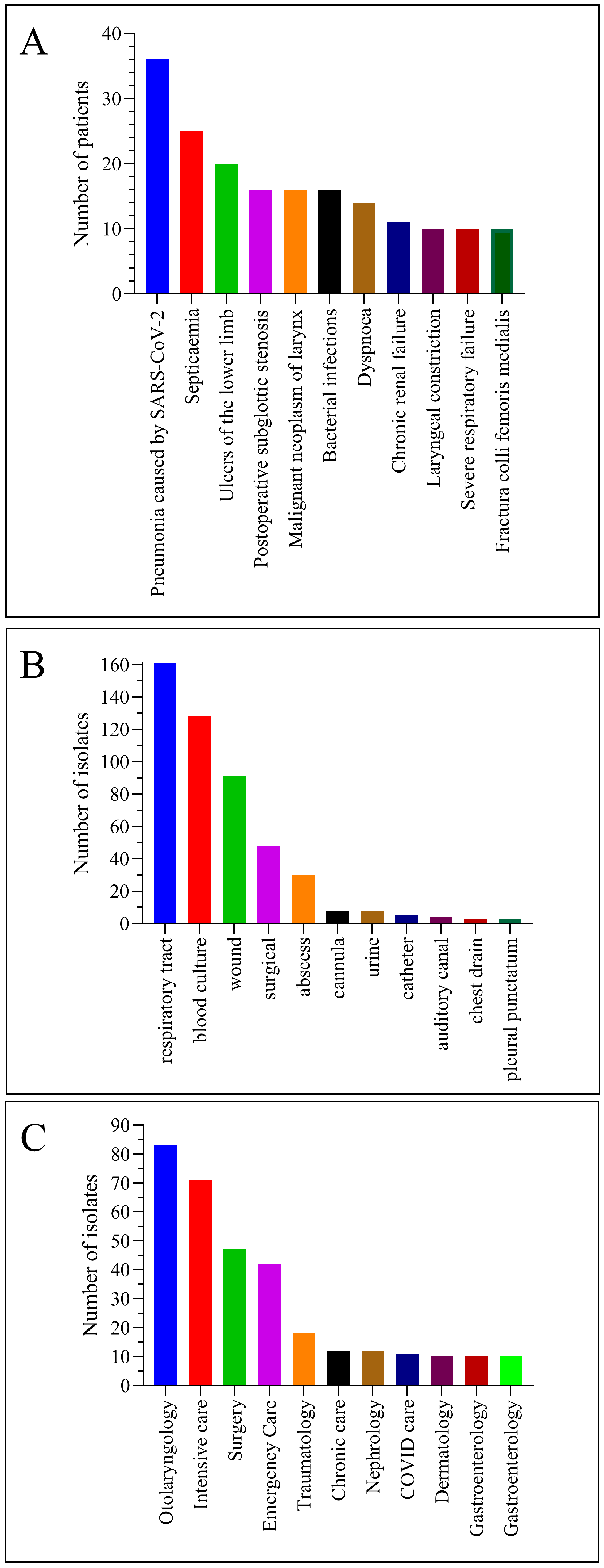
3.1. The C. striatum Was Isolated Mainly from the Respiratory Tract of Elderly Male Patients with COVID-19
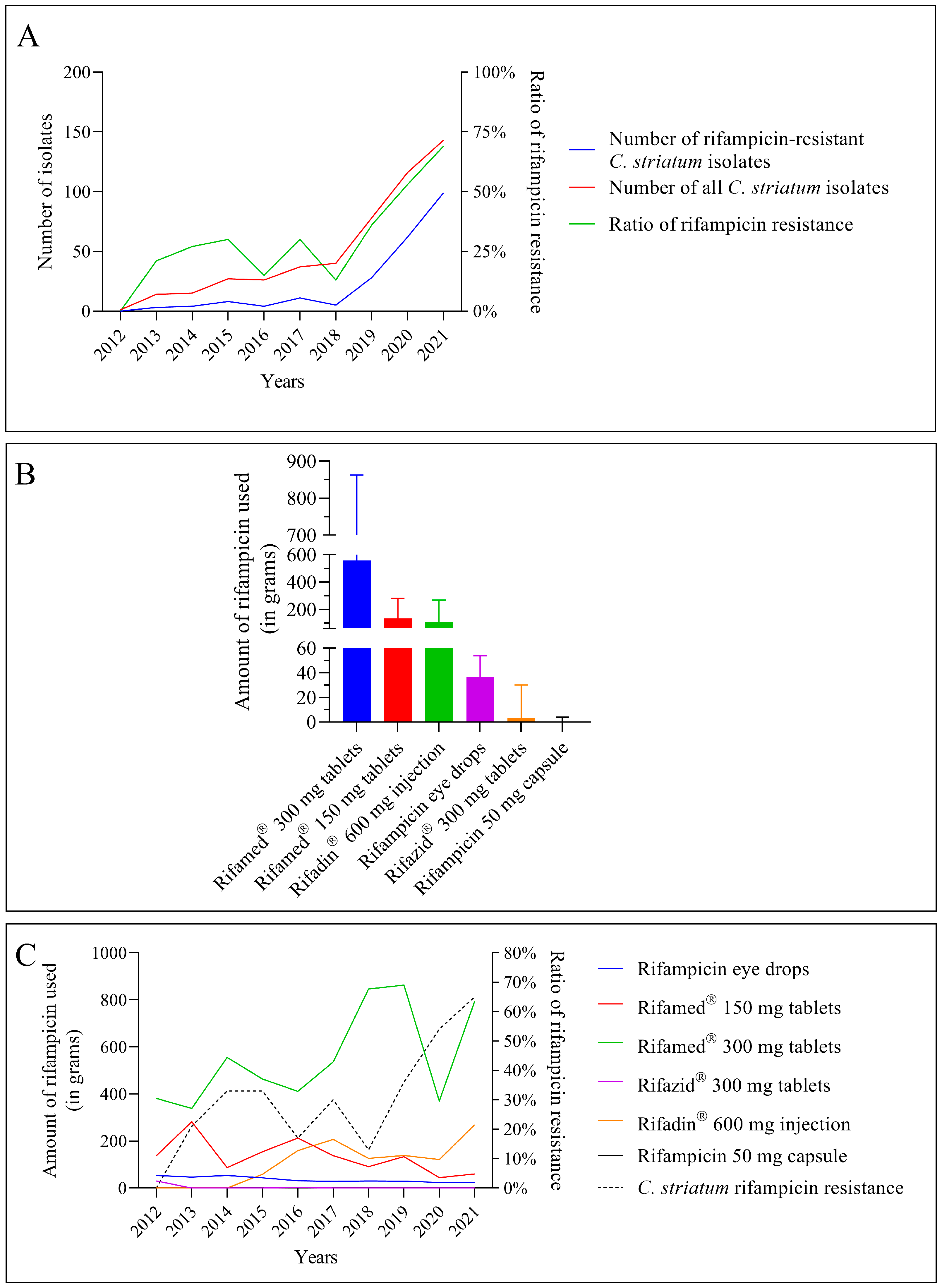
3.2. The Number of C. striatum Isolates, Their Resistance to Rifampicin, and the Use of Certain Antibiotics Containing Rifampicin Increased Concomitantly during the Study
3.3. Not All Rifampicin-Containing Medications Experienced a Rise in Usage as the Resistance Increased
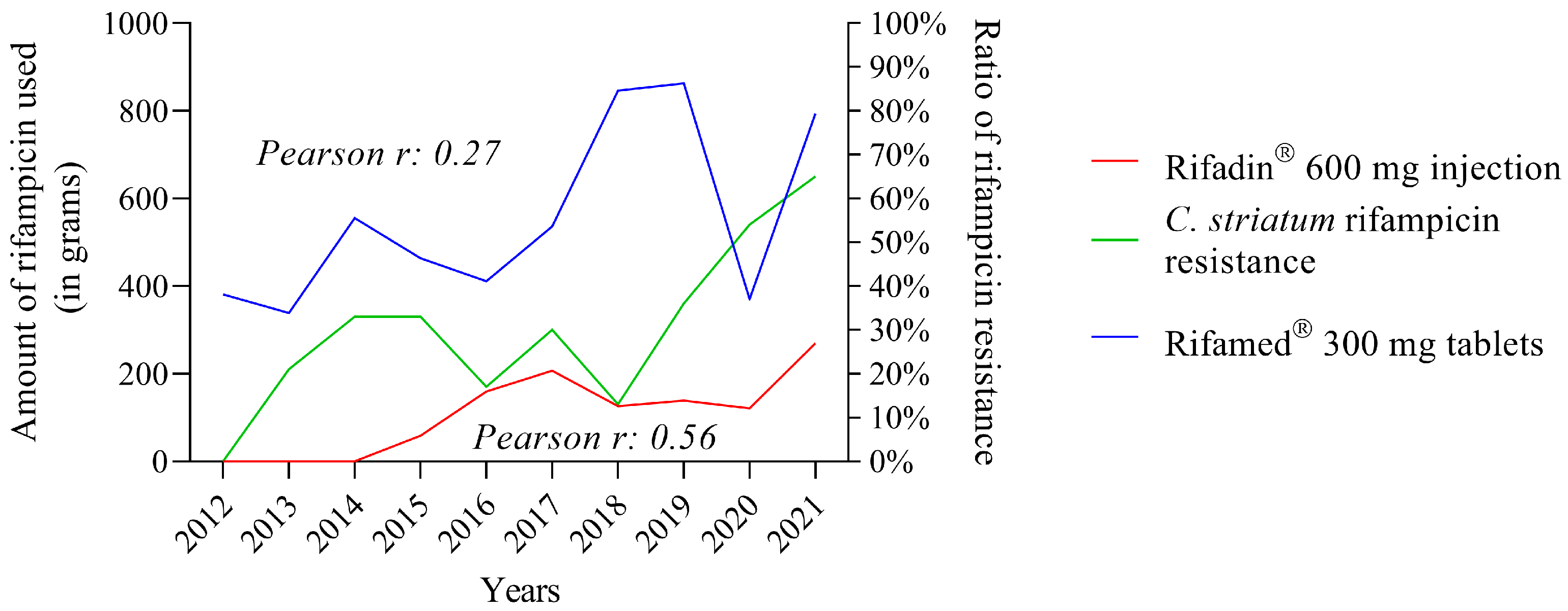
3.4. The Use of Some Rifampicin-Containing Drugs Correlates Better with Increased Resistance Than Others
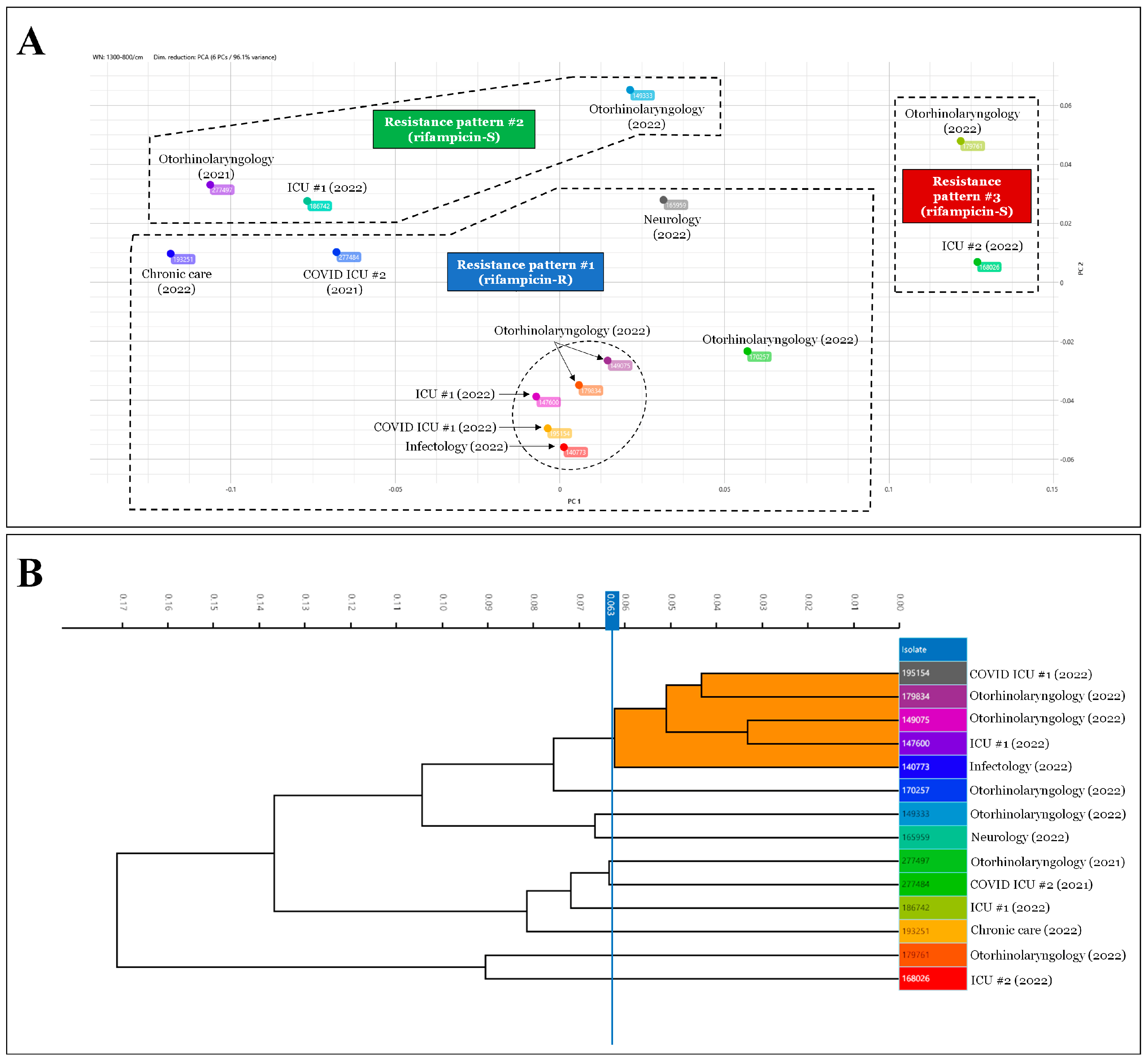
3.5. The IRBT Analysis Confirms That Rifampicin-Resistant C. striatum Strains Belong to Different Clones Than Sensitive Ones
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, R.; Reboli, A.C. Other Coryneform Bacteria and Rhodococci. In Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases; Elsevier Inc.: Philadelphia, PA, USA, 2015; Volume 2, pp. 2373–2382. [Google Scholar]
- Funke, G.; Bernard, K.A. Coryneform Gram-Positive Rods. In Manual of Clinical Microbiology; American Society for Microbiology Press: Washington, DC, USA, 2015; Volume 1, pp. 474–503. [Google Scholar]
- Shariff, M.; Aditi, A.; Beri, K. Corynebacterium striatum: An Emerging Respiratory Pathogen. J. Infect. Dev. Ctries 2018, 12, 581–586. [Google Scholar] [CrossRef]
- Charalampous, T.; Alcolea-Medina, A.; Snell, L.B.; Williams, T.G.S.; Batra, R.; Alder, C.; Telatin, A.; Camporota, L.; Meadows, C.I.S.; Wyncoll, D.; et al. Evaluating the Potential for Respiratory Metagenomics to Improve Treatment of Secondary Infection and Detection of Nosocomial Transmission on Expanded COVID-19 Intensive Care Units. Genome Med. 2021, 13, 182. [Google Scholar] [CrossRef] [PubMed]
- McMullen, A.R.; Anderson, N.; Wallace, M.A.; Shupe, A.; Burnham, C.-A.D. When Good Bugs Go Bad: Epidemiology and Antimicrobial Resistance Profiles of Corynebacterium striatum, an Emerging Multidrug-Resistant, Opportunistic Pathogen. Antimicrob. Agents Chemother. 2017, 61, e01111-17. [Google Scholar] [CrossRef] [Green Version]
- Boltin, D.; Katzir, M.; Bugoslavsky, V.; Yalashvili, I.; Brosh-Nissimov, T.; Fried, M.; Elkayam, O. Corynebacterium striatum—A Classic Pathogen Eluding Diagnosis. Eur. J. Intern. Med. 2009, 20, e49–e52. [Google Scholar] [CrossRef]
- Oliva, A.; Belvisi, V.; Iannetta, M.; Andreoni, C.; Mascellino, M.T.; Lichtner, M.; Vullo, V.; Mastroianni, C.M. Pacemaker Lead Endocarditis Due to Multidrug-Resistant Corynebacterium striatum Detected with Sonication of the Device. J. Clin. Microbiol. 2010, 48, 4669–4671. [Google Scholar] [CrossRef] [Green Version]
- Fernández Guerrero, M.L.; Molins, A.; Rey, M.; Romero, J.; Gadea, I. Multidrug-Resistant Corynebacterium striatum Endocarditis Successfully Treated with Daptomycin. Int. J. Antimicrob. Agents 2012, 40, 373–374. [Google Scholar] [CrossRef]
- Wong, K.Y.; Chan, Y.C.; Wong, C.Y. Corynebacterium striatum as an Emerging Pathogen. J. Hosp. Infect. 2010, 76, 371–372. [Google Scholar] [CrossRef]
- Werth, B.J.; Hahn, W.O.; Butler-Wu, S.M.; Rakita, R.M. Emergence of High-Level Daptomycin Resistance in Corynebacterium striatum in Two Patients with Left Ventricular Assist Device Infections. Microb. Drug Resist. 2016, 22, 233–237. [Google Scholar] [CrossRef] [Green Version]
- Hahn, W.O.; Werth, B.J.; Butler-Wu, S.M.; Rakita, R.M. Multidrug-Resistant Corynebacterium striatum Associated with Increased Use of Parenteral Antimicrobial Drugs. Emerg. Infect. Dis. 2016, 22, 1908–1914. [Google Scholar] [CrossRef] [Green Version]
- Campanile, F.; Carretto, E.; Barbarini, D.; Grigis, A.; Falcone, M.; Goglio, A.; Venditti, M.; Stefani, S. Clonal Multidrug-Resistant Corynebacterium striatum Strains, Italy. Emerg. Infect. Dis. 2009, 15, 75–78. [Google Scholar] [CrossRef]
- de Arriba, J.J.; Blanch, J.J.; Mateos, F.; Martínez-Alfaro, E.; Solera, J. Corynebacterium striatum First Reported Case of Prosthetic Valve Endocarditis. J. Infect. 2002, 44, 193. [Google Scholar] [CrossRef]
- Melero-Bascones, M.; Munoz, P.; Rodriguez-Creixems, M.; Bouza, E. Corynebacterium striatum: An Undescribed Agent of Pacemaker-Related Endocarditis. Clin. Infect. Dis. 1996, 22, 576–577. [Google Scholar] [CrossRef] [Green Version]
- Silva-Santana, G.; Silva, C.M.F.; Olivella, J.G.B.; Silva, I.F.; Fernandes, L.M.O.; Sued-Karam, B.R.; Santos, C.S.; Souza, C.; Mattos-Guaraldi, A.L. Worldwide Survey of Corynebacterium striatum Increasingly Associated with Human Invasive Infections, Nosocomial Outbreak, and Antimicrobial Multidrug-Resistance, 1976–2020. Arch. Microbiol. 2021, 203, 1863–1880. [Google Scholar] [CrossRef]
- Alibi, S.; Ferjani, A.; Boukadida, J.; Cano, M.E.; Fernández-Martínez, M.; Martínez-Martínez, L.; Navas, J. Occurrence of Corynebacterium striatum as an Emerging Antibiotic-Resistant Nosocomial Pathogen in a Tunisian Hospital. Sci. Rep. 2017, 7, 9704. [Google Scholar] [CrossRef] [Green Version]
- Orosz, L.; Sóki, J.; Kókai, D.; Burián, K. Corynebacterium striatum—Got Worse by a Pandemic? Pathogens 2022, 11, 685. [Google Scholar] [CrossRef]
- Leyton, B.; Ramos, J.N.; Baio, P.V.P.; Veras, J.F.C.; Souza, C.; Burkovski, A.; Mattos-Guaraldi, A.L.; Vieira, V.V.; Abanto Marin, M. Treat Me Well or Will Resist: Uptake of Mobile Genetic Elements Determine the Resistome of Corynebacterium striatum. Int. J. Mol. Sci. 2021, 22, 7499. [Google Scholar] [CrossRef]
- Yoon, S.; Kim, H.; Lee, Y.; Kim, S. Bacteremia Caused by Corynebacterium amycolatum with a Novel Mutation in GyrA Gene That Confers High-Level Quinolone Resistance. Ann. Lab. Med. 2011, 31, 47–48. [Google Scholar] [CrossRef] [Green Version]
- Reddy, B.; Chaudhury, A.; Kalawat, U.; Jayaprada, R.; Reddy, G.; Ramana, B. Isolation, Speciation, and Antibiogram of Clinically Relevant Non-Diphtherial Corynebacteria (Diphtheroids). Indian J. Med. Microbiol. 2012, 30, 52–57. [Google Scholar] [CrossRef]
- Ramos, J.N.; Souza, C.; Faria, Y.V.; da Silva, E.C.; Veras, J.F.C.; Baio, P.V.P.; Seabra, S.H.; de Oliveira Moreira, L.; Hirata Júnior, R.; Mattos-Guaraldi, A.L.; et al. Bloodstream and Catheter-Related Infections Due to Different Clones of Multidrug-Resistant and Biofilm Producer Corynebacterium striatum. BMC Infect. Dis. 2019, 19, 672. [Google Scholar] [CrossRef] [Green Version]
- Souza, C.D.; Faria, Y.V.; Sant’Anna, L.D.; Viana, V.G.; Seabra, S.H.; Souza, M.C.; Vieira, V.V.; Hirata Júnior, R.; Moreira, L.D.; Mattos-Guaraldi, A.L. Biofilm Production by Multiresistant Corynebacterium striatum Associated with Nosocomial Outbreak. Mem. Inst. Oswaldo Cruz. 2015, 110, 242–248. [Google Scholar] [CrossRef] [Green Version]
- Mhade, S.; Panse, S.; Tendulkar, G.; Awate, R.; Narasimhan, Y.; Kadam, S.; Yennamalli, R.M.; Kaushik, K.S. AMPing Up the Search: A Structural and Functional Repository of Antimicrobial Peptides for Biofilm Studies, and a Case Study of Its Application to Corynebacterium striatum, an Emerging Pathogen. Front. Cell Infect. Microbiol. 2021, 11, 803774. [Google Scholar] [CrossRef] [PubMed]
- De Souza, C.; Mota, H.F.; Faria, Y.V.; Cabral, F.d.O.; de Oliveira, D.R.; Sant’Anna, L.d.O.; Nagao, P.E.; Santos, C.d.S.; Moreira, L.O.; Mattos-Guaraldi, A.L. Resistance to Antiseptics and Disinfectants of Planktonic and Biofilm-Associated Forms of Corynebacterium striatum. Microb. Drug Resist. 2020, 26, 1546–1558. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Wang, Y.; Du, X.; Cui, J.; Wang, K.; Zhang, L.; Han, Y. Rapid Transmission of Multidrug-Resistant Corynebacterium striatum among Susceptible Patients in a Tertiary Hospital in China. J. Infect. Dev. Ctries 2016, 10, 1299–1305. [Google Scholar] [CrossRef] [Green Version]
- Pollard, C.A.; Morran, M.P.; Nestor-Kalinoski, A.L. The COVID-19 Pandemic: A Global Health Crisis. Physiol. Genom. 2020, 52, 549–557. [Google Scholar] [CrossRef]
- Ripa, M.; Galli, L.; Poli, A.; Oltolini, C.; Spagnuolo, V.; Mastrangelo, A.; Muccini, C.; Monti, G.; De Luca, G.; Landoni, G.; et al. Secondary Infections in Patients Hospitalized with COVID-19: Incidence and Predictive Factors. Clin. Microbiol. Infect. 2021, 27, 451–457. [Google Scholar] [CrossRef] [PubMed]
- Fattorini, L.; Creti, R.; Palma, C.; Pantosti, A. Unit of Antibiotic Resistance and Special Pathogens; Unit of Antibiotic Resistance and Special Pathogens of the Department of Infectious Diseases, Istituto Superiore di Sanità, Rome Bacterial Coinfections in COVID-19: An Underestimated Adversary. Ann. Ist. Super Sanita 2020, 56, 359–364. [Google Scholar] [CrossRef]
- Fiorillo, L.; Meto, A.; Cicciù, F.; De Stefano, R. An Eventual SARS-CoV-2 Infection Prevention Protocol in the Medical Setting and Dental Office. Int. J. Environ. Res. Public Health 2021, 18, 2593. [Google Scholar] [CrossRef]
- Marino, A.; Campanella, E.; Stracquadanio, S.; Ceccarelli, M.; Zagami, A.; Nunnari, G.; Cacopardo, B. Corynebacterium striatum Bacteremia during SARS-CoV-2 Infection: Case Report, Literature Review, and Clinical Considerations. Infect. Dis. Rep. 2022, 14, 383–390. [Google Scholar] [CrossRef]
- Shilts, M.H.; Rosas-Salazar, C.; Strickland, B.A.; Kimura, K.S.; Asad, M.; Sehanobish, E.; Freeman, M.H.; Wessinger, B.C.; Gupta, V.; Brown, H.M.; et al. Severe COVID-19 Is Associated with an Altered Upper Respiratory Tract Microbiome. Front. Cell Infect. Microbiol. 2022, 11, 781968. [Google Scholar] [CrossRef]
- Howard, P.; Twycross, R.; Grove, G.; Charlesworth, S.; Mihalyo, M.; Wilcock, A. Rifampin (INN Rifampicin). J. Pain Symptom Manag. 2015, 50, 891–895. [Google Scholar] [CrossRef]
- Lorente, L. Antimicrobial-Impregnated Catheters for the Prevention of Catheter-Related Bloodstream Infections. World J. Crit. Care Med. 2016, 5, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Cultrera, R.; Barozzi, A.; Libanore, M.; Marangoni, E.; Pora, R.; Quarta, B.; Spadaro, S.; Ragazzi, R.; Marra, A.; Segala, D.; et al. Co-Infections in Critically Ill Patients with or without COVID-19: A Comparison of Clinical Microbial Culture Findings. Int. J. Environ. Res. Public Health 2021, 18, 4358. [Google Scholar] [CrossRef]
- Shinohara, D.R.; dos Santos Saalfeld, S.M.; Martinez, H.V.; Altafini, D.D.; Costa, B.B.; Fedrigo, N.H.; Tognim, M.C.B. Outbreak of Endemic Carbapenem-Resistant Acinetobacter baumannii in a Coronavirus Disease 2019 (COVID-19)—Specific Intensive Care Unit. Infect. Control Hosp. Epidemiol. 2021, 43, 815–817. [Google Scholar] [CrossRef] [PubMed]
- Gottesman, T.; Fedorowsky, R.; Yerushalmi, R.; Lellouche, J.; Nutman, A. An Outbreak of Carbapenem-Resistant Acinetobacter baumannii in a COVID-19 Dedicated Hospital. Infect. Prev. Pract. 2021, 3, 100113. [Google Scholar] [CrossRef]
- Durán-Manuel, E.M.; Cruz-Cruz, C.; Ibáñez-Cervantes, G.; Bravata-Alcantará, J.C.; Sosa-Hernández, O.; Delgado-Balbuena, L.; León-García, G.; Cortés-Ortíz, I.A.; Cureño-Díaz, M.A.; Castro-Escarpulli, G.; et al. Clonal Dispersion of Acinetobacter baumannii in an Intensive Care Unit Designed to Patients COVID-19. J. Infect. Dev. Ctries 2021, 15, 58–68. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Zhu, K.; Jin, D.; Shen, W.; Liu, C.; Zhou, H.; Zhang, R. Evaluation of IR Biotyper for Carbapenem-Resistant Pseudomonas aeruginosa Typing and Its Application Potential for the Investigation of Nosocomial Infection. Front. Microbiol. 2023, 14, 1068872. [Google Scholar] [CrossRef]
- Hu, Y.; Zhou, H.; Lu, J.; Sun, Q.; Liu, C.; Zeng, Y.; Zhang, R. Evaluation of the IR Biotyper for Klebsiella pneumoniae Typing and Its Potentials in Hospital Hygiene Management. Microb. Biotechnol. 2021, 14, 1343–1352. [Google Scholar] [CrossRef]
- Eucast: Disk Diffusion Methodology. Available online: https://www.eucast.org/ast_of_bacteria/disk_diffusion_methodology (accessed on 10 December 2022).
- De Socio, G.V.; Rubbioni, P.; Botta, D.; Cenci, E.; Belati, A.; Paggi, R.; Pasticci, M.B.; Mencacci, A. Measurement and Prediction of Antimicrobial Resistance in Bloodstream Infections by ESKAPE Pathogens and Escherichia coli. J. Glob. Antimicrob. Resist. 2019, 19, 154–160. [Google Scholar] [CrossRef]
- Folliero, V.; Dell’Annunziata, F.; Roscetto, E.; Cammarota, M.; De Filippis, A.; Schiraldi, C.; Catania, M.R.; Casolaro, V.; Perrella, A.; Galdiero, M.; et al. Niclosamide as a Repurposing Drug against Corynebacterium striatum Multidrug-Resistant Infections. Antibiotics 2022, 11, 651. [Google Scholar] [CrossRef]
- Noussair, L.; Salomon, E.; El Sayed, F.; Duran, C.; Bouchand, F.; Roux, A.-L.; Gaillard, J.-L.; Bauer, T.; Rottman, M.; Dinh, A. Monomicrobial Bone and Joint Infection Due to Corynebacterium striatum: Literature Review and Amoxicillin-Rifampin Combination as Treatment Perspective. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 1269–1278. [Google Scholar] [CrossRef]
- Shah, M.; Murillo, J.L. Successful Treatment of Corynebacterium striatum Endocarditis with Daptomycin plus Rifampin. Ann. Pharmacother. 2005, 39, 1741–1744. [Google Scholar] [CrossRef] [PubMed]
- Alibi, S.; Ramos-Vivas, J.; Ben Selma, W.; Ben Mansour, H.; Boukadida, J.; Navas, J. Virulence of Clinically Relevant Multidrug Resistant Corynebacterium striatum Strains and Their Ability to Adhere to Human Epithelial Cells and Inert Surfaces. Microb. Pathog. 2021, 155, 104887. [Google Scholar] [CrossRef]
- Nudel, K.; Zhao, X.; Basu, S.; Dong, X.; Hoffmann, M.; Feldgarden, M.; Allard, M.; Klompas, M.; Bry, L. Genomics of Corynebacterium striatum, an Emerging Multidrug-Resistant Pathogen of Immunocompromised Patients. Clin. Microbiol. Infect. 2018, 24, 1016.e7–1016.e13. [Google Scholar] [CrossRef] [Green Version]
- Adékambi, T.; Drancourt, M.; Raoult, D. The RpoB Gene as a Tool for Clinical Microbiologists. Trends Microbiol. 2009, 17, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Országos Gyógyszerészeti és Élelmezés-egészségügyi Intézet. Available online: https://ogyei.gov.hu/gyogyszeradatbazis (accessed on 10 December 2022).
- Machowska, A.; Stålsby Lundborg, C. Drivers of Irrational Use of Antibiotics in Europe. Int. J. Environ. Res. Public Health 2019, 16, 27. [Google Scholar] [CrossRef] [Green Version]
- Correlation Coefficients. Available online: https://www.andrews.edu/~calkins/math/edrm611/edrm05.htm (accessed on 10 December 2022).
- Rifadin for Infusion 600 mg—Summary of Product Characteristics (SmPC)—(Emc). Available online: https://www.medicines.org.uk/emc/medicine/6435/SPC/Rifadin+For+Infusion+600mg/#gref (accessed on 10 December 2022).
- Kon, H.; Temkin, E.; Elmalih, P.; Keren-Paz, A.; Ben-David, D.; Najjar-Debbiny, R.; Gottesman, T.; Carmeli, Y. Analysis of Four Carbapenem-Resistant Acinetobacter Baumannii Outbreaks Using Fourier-Transform Infrared Spectroscopy. Infect. Control. Hosp. Epidemiol. 2022, 1–3. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Statistical Indicators | C. striatum Rifamicin Resistance Ratio vs. Rifampicin Eye Drops | C. striatum Rifamicin Resistance Ratio vs. Rifamed® 150 mg Tablets | C. striatum Rifamicin Resistance Ratio vs. Rifamed® 300 mg Tablets | C. striatum Rifamicin Resistance Ratio vs. Rifazid® 300 mg Tablets | C. striatum Rifamicin Resistance Ratio vs. Rifadin® 600 mg Injection | C. striatum Rifamicin Resistance Ratio vs. Rifampicin 50 mg Capsule |
|---|---|---|---|---|---|---|
| Pearson’s r-value | −0.5793 | −0.5331 | 0.2714 | −0.5825 | 0.5576 | −0.2639 |
| 95% confidence interval | −0.8858 to 0.07929 | −0.8705 to 0.1453 | −0.4321 to 0.7695 | −0.8869 to 0.07441 | −0.1109 to 0.8787 | −0.7662 to 0.4386 |
| R squared | 0.3355 | 0.2842 | 0.07364 | 0.3393 | 0.3110 | 0.06964 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orosz, L.; Lengyel, G.; Makai, K.; Burián, K. Prescription of Rifampicin for Staphylococcus aureus Infections Increased the Incidence of Corynebacterium striatum with Decreased Susceptibility to Rifampicin in a Hungarian Clinical Center. Pathogens 2023, 12, 481. https://doi.org/10.3390/pathogens12030481
Orosz L, Lengyel G, Makai K, Burián K. Prescription of Rifampicin for Staphylococcus aureus Infections Increased the Incidence of Corynebacterium striatum with Decreased Susceptibility to Rifampicin in a Hungarian Clinical Center. Pathogens. 2023; 12(3):481. https://doi.org/10.3390/pathogens12030481
Chicago/Turabian StyleOrosz, László, György Lengyel, Klára Makai, and Katalin Burián. 2023. "Prescription of Rifampicin for Staphylococcus aureus Infections Increased the Incidence of Corynebacterium striatum with Decreased Susceptibility to Rifampicin in a Hungarian Clinical Center" Pathogens 12, no. 3: 481. https://doi.org/10.3390/pathogens12030481