

Prevalence of Intestinal Parasitosis in Guinea: Systematic Review of the Literature and Meta-Analysis
 , and
, and
Abstract
:1. Introduction
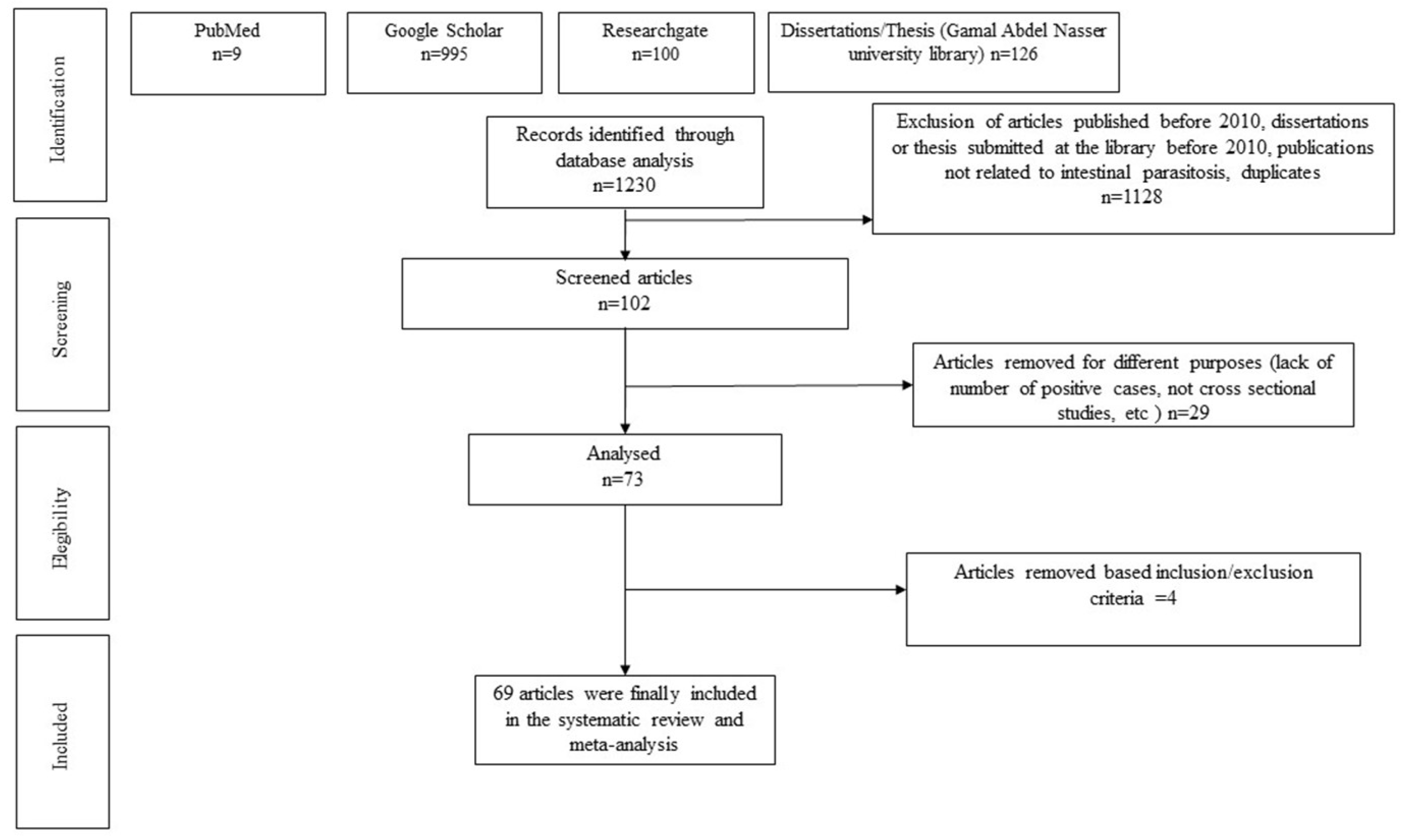
2. Methods
2.1. Documentary Search Strategy
2.2. Study Selection Criteria
- Language of publication/written: English or French
- Year of publication/report: from 2010 until 2020
- Study design: observational studies (cross-sectional, case-control, cohort).
- Outcome: prevalence of intestinal parasites and/or associated factors
- Study population: not restriction
- Study setting: at institution or community based
- Study country: Guinea
- Diagnostic modality: stool examination
- Type of parasite: either protozoa or helminths or both
- Types of articles: both published and unpublished including dissertations or theses accessible in the database of the UGAN in Conakry.
- Types of publication: peer-reviewed full-text articles.
- Exclusion criteria:
- Publications dating before 2010
- Publications reporting prevalence after antiparasitic treatment.
- Duplicates articles
- Dissertations of graduate students deposited in university libraries in Conakry before 2010
- Articles and dissertations on intestinal parasitosis carried out outside Guinea
- Articles that failed to report the number of study participants and number of cases
2.3. Search Strategy
2.4. Data Extraction
2.5. Statistical Analysis
2.6. Protocols and Registration
3. Results
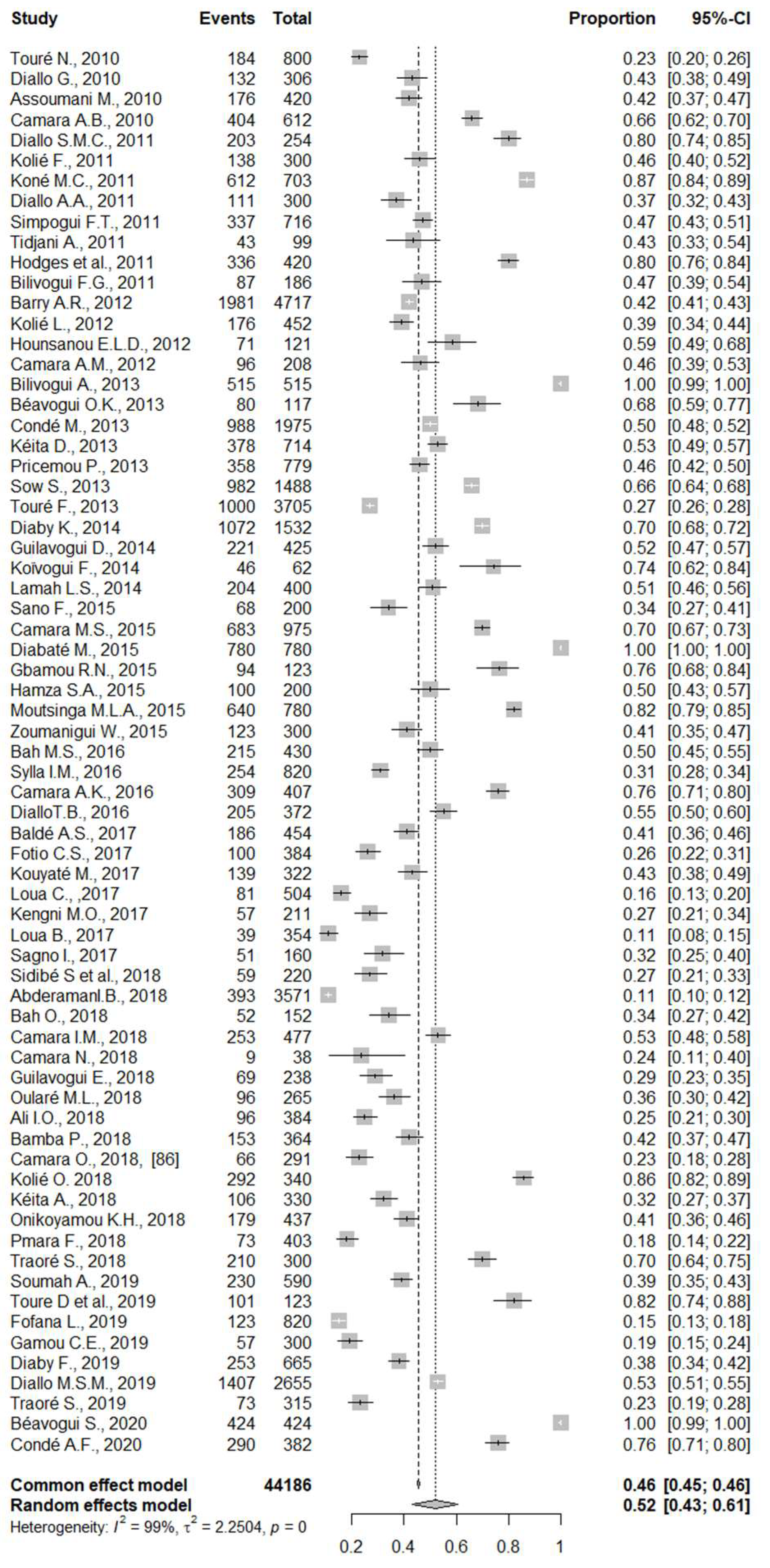
4. Pooled Prevalence of Intestinal Parasitic Infections in Guinea
5. Subgroup Analysis
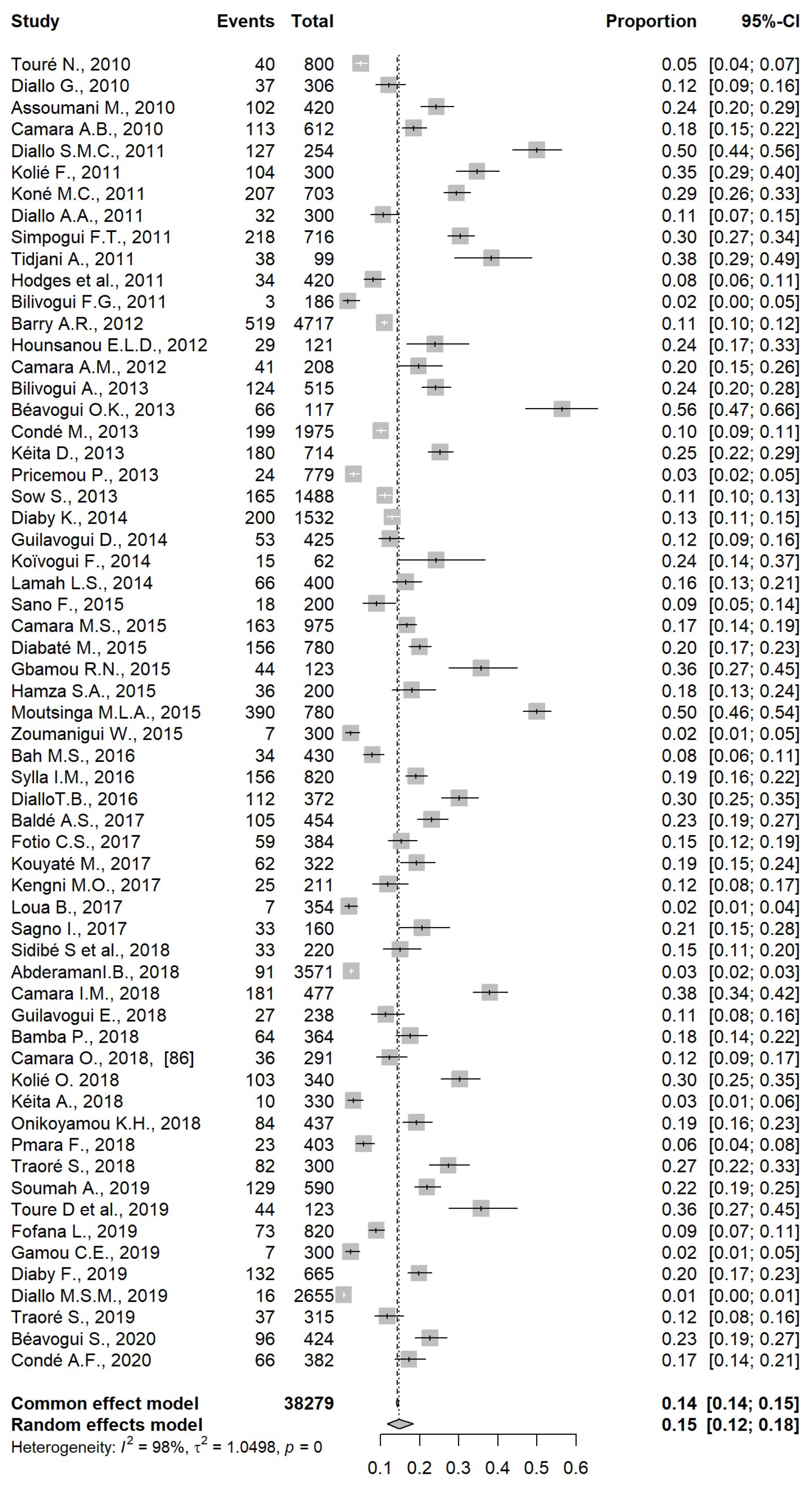
5.1. Analysis by Type of Intestinal Parasitic Infections
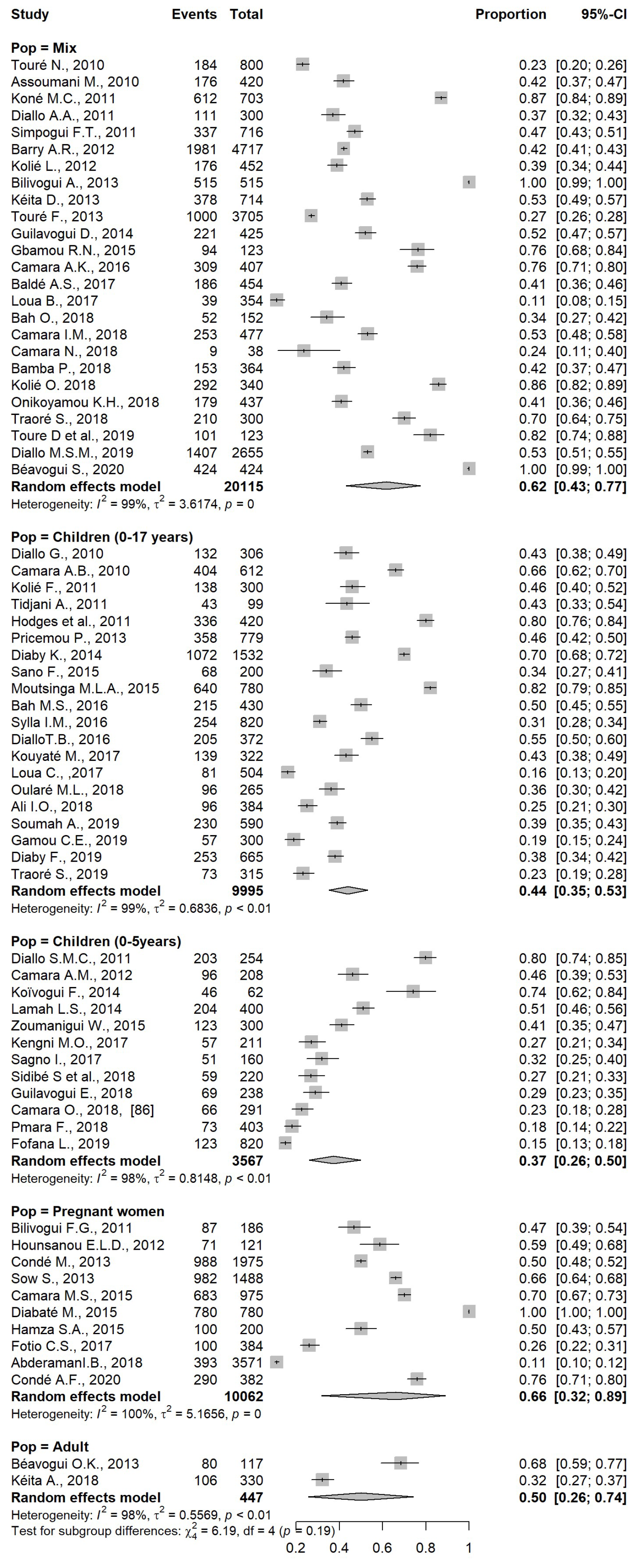
5.2. Analysis by Type of Population
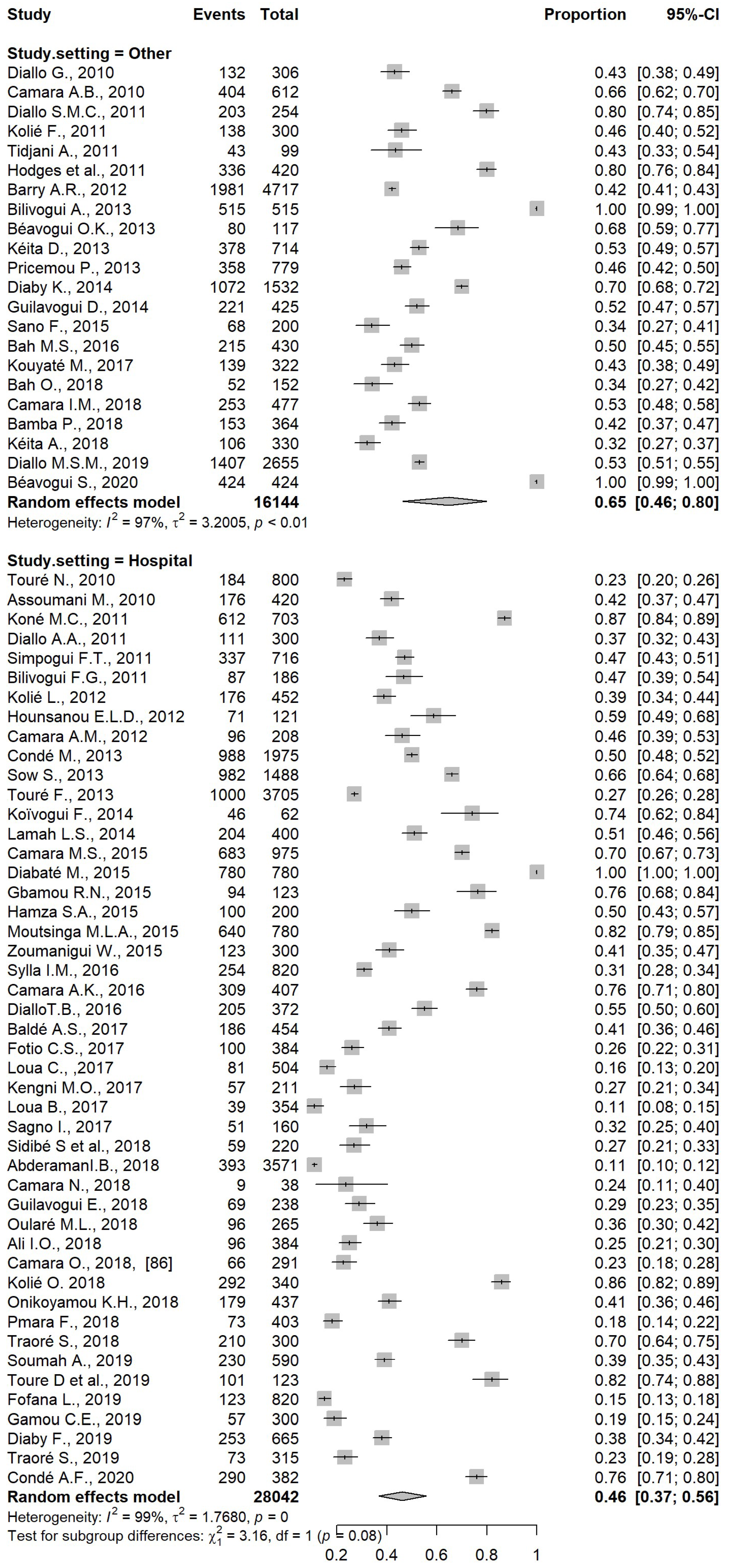
5.3. Analysis by Study Setting
5.4. Analysis by Region
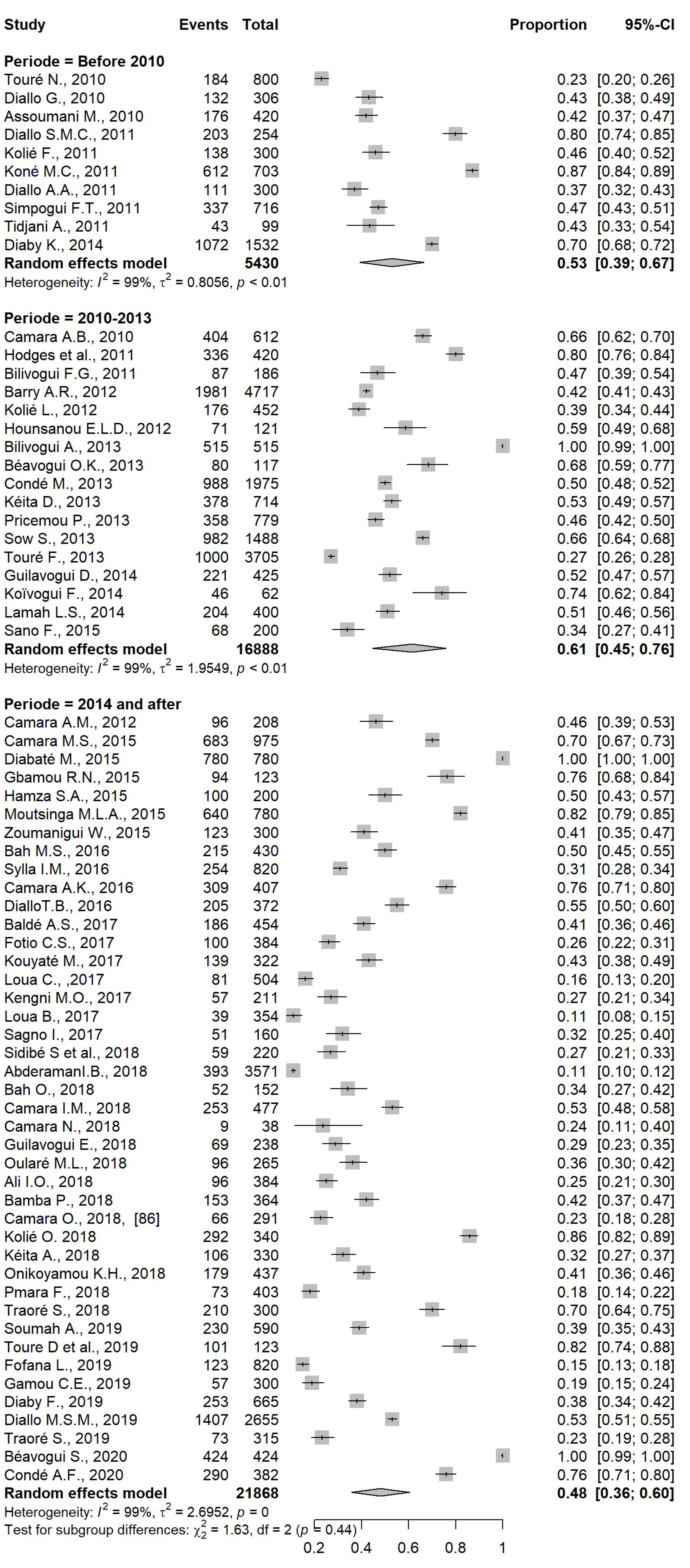
5.5. Analysis by Period
5.6. Other Parasites
6. Discussion
7. Strengths and Limitations of the Study
8. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Molyneux, D.H.; Savioli, L.; Engels, D. Neglected tropical diseases: Progress towards addressing the chronic pandemic. Lancet 2017, 389, 312–325. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Accelerating Work to Overcome the Global Impact of Neglected Tropical Diseases: A Roadmap for Implementation: Executive Summary. 2012. Available online: https://apps.who.int/iris/handle/10665/70809 (accessed on 1 January 2023).
- Sidibe, S.; Delamou, A.; Camara, B.; Magassouba, A.S.; Ravi, N.; Beavogui, A.H. Intestinal parasitic infections among acute malnourished children during ebola at Ratoma Medical Center of Conakry. Cent. Afr. J. Public Health 2018, 4, 59–64. [Google Scholar]
- Gyorkos, T.W.; Camara, B.; Kokoskin, E.; Carabin, H.; Prouty, R. Survey of parasitic prevalence in school-aged children in Guinea. Sante 1996, 6, 377–381. [Google Scholar] [PubMed]
- Eyayu, T.; Kiros, T.; Workineh, L.; Sema, M.; Damtie, S.; Hailemichael, W.; Dejen, E.; Tiruneh, T. Prevalence of intestinal parasitic infections and associated factors among patients attending at Sanja Primary Hospital, Northwest Ethiopia: An institutional-based cross-sectional study. PLoS ONE 2021, 16, e0247075. [Google Scholar] [CrossRef] [PubMed]
- Nithiuthai, S.; Anantaphruti, M.T.; Waikagul, J.; Gajadhar, A. Waterborne zoonotic helminthiases. Vet. Parasitol. 2004, 126, 167–193. [Google Scholar] [CrossRef]
- Aula, O.P.; McManus, D.P.; Jones, M.K.; Gordon, C.A. Schistosomiasis with a Focus on Africa. Trop. Med. Infect. Dis. 2021, 6, 109. [Google Scholar]
- Ali, S.A.; Niaz, S.; Aguilar-Marcelino, L.; Ali, W.; Ali, M.; Khan, A.; Amir, S.; Nasreen; Alanazi, A.D.; Cossio-Bayugar, R.; et al. Prevalence of Ascaris lumbricoides in contaminated faecal samples of children residing in urban areas of Lahore, Pakistan. Sci. Rep. 2020, 10, 21815. [Google Scholar] [CrossRef]
- Umbrello, G.; Pinzani, R.; Bandera, A.; Formenti, F.; Zavarise, G.; Arghittu, M.; Girelli, D.; Maraschini, A.; Muscatello, A.; Marchisio, P.; et al. Hookworm infection in infants: A case report and review of literature. Ital. J. Pediatr. 2021, 47, 26. [Google Scholar] [CrossRef]
- Hajissa, K.; Islam, M.A.; Sanyang, A.M.; Mohamed, Z. Prevalence of intestinal protozoan parasites among school children in Africa: A systematic review and meta-analysis. PLoS Negl. Trop. Dis. 2022, 16, e0009971. [Google Scholar] [CrossRef]
- Certad, G.; Viscogliosi, E.; Chabé, M.; Cacciò, S.M. Pathogenic mechanisms of Cryptosporidium and Giardia. Trends Parasitol. 2017, 33, 561–576. [Google Scholar] [CrossRef]
- Erismann, S.; Knoblauch, A.M.; Diagbouga, S.; Odermatt, P.; Gerold, J.; Shrestha, A.; Tarnagda, G.; Savadogo, B.; Schindler, C.; Utzinger, J.; et al. Prevalence of intestinal parasitic infections and associated risk factors among schoolchildren in the Plateau Central and Centre-Ouest regions of Burkina Faso. Parasites Vectors 2016, 9, 554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diongue, K.; Ndiaye, M.; Seck, M.C.; Diallo, M.A.; Ndiaye, Y.D.; Badiane, A.S.; Ndiaye, D. Distribution of Parasites Detected in Stool Samples of Patients in Le Dantec University Hospital of Dakar, Senegal, from 2011 to 2015. J. Trop. Med. 2017, 2017, 8296313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adoubryn, K.D.; Kouadio-Yapo, C.; Ouhon, J.; Aka, D.; Bintto, F.; Assoumou, A. Intestinal parasites in children in Biankouma, Ivory Coast (mountaineous western region): Efficacy and safety of praziquantel and albendazole. Med. Sante Trop. 2012, 22, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Yoseph, A.; Beyene, H. The high prevalence of intestinal parasitic infections is associated with stunting among children aged 6-59 months in Boricha Woreda, Southern Ethiopia: A cross-sectional study. BMC Public Health 2020, 20, 1270. [Google Scholar] [CrossRef] [PubMed]
- Ministère de la Santé, Direction Nationale des Grandes Endémies et de la et Lutte contre la Maladie (DNGELM). Plan directeur de la lutte contre les maladies tropicales négligées en Guinée (2019–2023). 2018. Available online: https://portail.sante.gov.gn/wp-content/uploads/2020/09/PD-Corrig%C3%A9-MLO-2.pdf (accessed on 1 January 2023).
- Ministère de la Santé. Plan National de Développement Sanitaire (PNDS)-2015-2024-Guinée. 2015. Available online: https://portail.sante.gov.gn/wp-content/uploads/2022/08/Plan_National-de-D%C3%A9veloppement-Sanitaire-2015-2024-Ao%C3%BBt-2015.pdf (accessed on 1 January 2023).
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria. 2021. Available online: https://www.R-project.org/ (accessed on 1 January 2023).
- Touré, N. Fréquence de L’amibiase Intestinale dans les Services de Médecine Générale à L’hôpital National Ignace Deen; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2010. [Google Scholar]
- Diallo, G. Prévalence des Parasitoses Intestinales chez les Elèves de L’école Primaire de Touguiwondy; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2010. [Google Scholar]
- Assoumani, M. Prévalence des Helminthiases Intestinales au CMC de Coleah (Commune de Matam, Conakry); Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2010. [Google Scholar]
- Camara, A.B. Prévalence des Parasitoses Intestinales chez les Enfants de 6 à 14 ans au Quartier Sinanya (Commune de Kindia); Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2010. [Google Scholar]
- Diallo, S.M.C. Prévalence des Parasitoses Intestinales chez les élèves de L’école Primaire de Coléah Centre (Commune de Matam); Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2011. [Google Scholar]
- Kolié, F. Prévalence des Helminthiases Intestinales à L’école Primaire Publique de Wanindara (Commune de Ratoma); Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2011. [Google Scholar]
- Koné, M.C. Prévalence des Parasitoses Intestinales au CMC de Matam; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2011. [Google Scholar]
- Diallo, A.A. Fréquence des Parasitoses Intestinales au CMC de Ratoma; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2011. [Google Scholar]
- Simpogui, F.T. Fréquence des Parasitoses Intestinales chez les Patients en Consultation au CMC de Flamboyant, Commune de Ratoma; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2011. [Google Scholar]
- Tidjani, A. Prévalence des Parasitoses Intestinales chez les Enfants du Village D’enfants SOS de Conakry; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2011. [Google Scholar]
- Hodges, M.; Koroma, M.M.; Baldé, M.S.; Turay, H.; Fofanah, I.; Divall, M.J.; Winkler, M.S.; Zhang, Y. Current status of schistosomiasis and soil-transmitted helminthiasis in Beyla and Macenta Prefectures, Forest Guinea. Trans. R. Soc. Trop. Med. Hyg. 2011, 105, 672–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bilivogui, F.G. Prévalence des Parasitoses Intestinales chez les Femmes Enceintes, en Consultation au Centre de Santé de Gbessia Port 1; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2011. [Google Scholar]
- Barry, A.R. Profil des Helminthiases Intestinales Dans la Zone Minière de la Compagnie de Bauxites de Kindia (Simbaya et Débélé) de 2005 à 2010; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2012. [Google Scholar]
- Kolié, L. Prévalence des Bilharzioses à L’hôpital Régional de N’Zérékoré; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2012. [Google Scholar]
- Hounsanou, E.L.D. Les parasitoses Intestinales chez les Femmes Enceintes: Fréquence et Profil Epidémiologique au CMC de Coléah; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2012. [Google Scholar]
- Camara, A.M. Gastroentérites Aigues chez les Enfants de 0 à 5 ans: Aspects Epidémiologiques, Cliniques et Thérapeutiques au Service de Pédiatrie de L’hôpital Régional de Mamou; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2012. [Google Scholar]
- Bilivogui, A. Prévalence et Facteurs Déterminants de L’endémicité des Schistosomiases dans la Sous-Préfecture de Koyamah (Macenta); Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2013. [Google Scholar]
- Béavogui, O.K. Prévalence des Helminthiases Intestinales et des Facteurs Déterminants leur Endémicité chez les Etudiants de l’Université Thierno Amadou Diallo de Conakry; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2013. [Google Scholar]
- Condé, M. Utilisation des Antiparasitaires Intestinaux chez les Femmes Enceintes au Service de Maternité des CMC de Flamboyant et Matam; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2013. [Google Scholar]
- Kéita, D. Prévalence des Helminthiases Intestinales et Leur Endémicité au Port Autonome de Conakry; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2013. [Google Scholar]
- Pricemou, P. Prévalence et Facteurs Déterminants de L’endémicité de la Schistosomiase Intestinale Dans la Sous-Préfecture de Boola; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2013. [Google Scholar]
- Sow, S. Utilisation des Antiparasitaires intestinaux chez les Femmes Enceintes au Service de Maternité de L’hôpital National Donka; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2013. [Google Scholar]
- Touré, F. Profil des Antiparasitaires Utilisés au Service de Médecine Générale et Pédiatrique du CNFSA Jean Paul II; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2013. [Google Scholar]
- Diaby, K. Profil des Helminthiases Intestinales Dans la Zone Minière de Kintinia (Siguiri); Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2014. [Google Scholar]
- Guilavogui, D. Prévalence et Facteurs Déterminants de L’endémicité des Schistosomiases dans la Sous-Préfecture de Sérédou (Macneta); Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2014. [Google Scholar]
- Koïvogui, F. Malnutrition Aigüe et Parasitoses Intestinales chez les Enfants de 6 à 59 mois au Service de Pédiatrie à L’hôpital Régional de N’Zérékoré; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2014. [Google Scholar]
- Lamah, L.S. Prévalence des Parasitoses Intestinales au Service de Pédiatrie de L’hôpital Régional de N’Zérékoré; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2014. [Google Scholar]
- Sano, F. Prévalence des Helminthiases Intestinales chez les Enfants de L’école Primaire de Sonfonia centre (Conakry); Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2015. [Google Scholar]
- Camara, M.S. Enquête sur la Prescription des Antiparasitaires Intestinaux chez les Femmes Enceintes au Service de Maternité de L’hôpital Préfectoral de Siguiri; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2015. [Google Scholar]
- Diabaté, M. Enquête sur la Prescription des Antiparasitaires Intestinaux chez les Femmes Enceintes à L’hôpital Régional de N’Zérékoré; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2015. [Google Scholar]
- Gbamou, R.N. Prévalence des Parasitoses Intestinales chez les Personnes Vivantes avec le VIH/TB au Service de Pneumo-Phtisiologie de Conakry; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2015. [Google Scholar]
- Hamza, S.A. Prévalence des Parasitoses Intestinales Anemiantes chez les Femmes Enceintes reçus en Consultation à L’hôpital Régional Alpha Oumar Diallo de Kindia; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2015. [Google Scholar]
- Moutsinga, M.L.A. Etude Restrospective des Helminthiases Intestinales Chez les Enfants de 3 à 17 ans reçus en Consultation au Centre de Santé Arc-en-ciel de Lambagni, Commune de Ratoma; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2015. [Google Scholar]
- Zoumanigui, W. Fréquence des Diarrhées D’origine Parasitaire au Service de Pédiatrie Chez les Enfants de 0 à 5 ans à L’hôpital Préfectoral de Macenta; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2015. [Google Scholar]
- Bah, M.S. Prévalence des Helminthiases Intestinales chez les Elèves de L’école Primaire de Tangama et Alpha Yaya dans la Commune Urbaine de Dalaba; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2016. [Google Scholar]
- Sylla, I.M. Enquête sur la Prescription des Antihelminthiques à la Pédiatrie de L’hôpital Préfectoral de Gueckédou; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2016. [Google Scholar]
- Camara, A.K. Prévalence des Helminthes Intestinaux Anemiantes chez les Patients Reçus en Consultation au CMC de Matam; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2016. [Google Scholar]
- Diallo, T.B. Prévalence et Aspect Epidémiologique des Helminthiases Intestinales Chez les Enfants âgés de 5-15 Ans Reçus au Laboratoire de L’hôpital Régional de Labé; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2016. [Google Scholar]
- Baldé, A.S. Prévalence des Parasitoses Intestinales Anemiantes chez les Patients Reçus en Consultation à L’hôpital Régional de Labé; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2017. [Google Scholar]
- Fotio, C.S. Prévalence des Parasitoses Intestinales chez la Femme Enceinte au CMC de Matam; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2017. [Google Scholar]
- Kouyaté, M. Prévalence des Helminthiases Intestinales et Facteurs de Leur Endémicité à l’école Primaire de Sangoyah; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2017. [Google Scholar]
- Loua, C. Enquête sur la Prescription des Antihelminthiques au Service de Pédiatrie de l’Hôpital régional de N’Zérékoré; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2017. [Google Scholar]
- Kengni, M.O. Prévalence des Diarrhées D’origine Parasitaire chez les Enfants âgés de 0 à 5 ans au Service de Pédiatrie du CMC de Matam; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2017. [Google Scholar]
- Loua, B. Prévalence des Parasitoses Intestinales au CMC de Matam; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2017. [Google Scholar]
- Sagno, I. Diarrhées Aigües chez les enfants âgés de à 0 à 59 mois: Aspects Epidémiologiques, Cliniques et Thérapeutiques au Service de pédiatrie de L’hôpital Préfectoral de Lola; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2017. [Google Scholar]
- Abderaman, I.B. Enquête Rétrospective sur la Prescription des Antiparasitaires chez les Femmes Enceintes au CMC de la Minière; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2018. [Google Scholar]
- Bah, O. Évolution Epidémiologique de la Shistosomiase à la de la Shistosoma Mansoni à Tatagui, Commune Urbaine de Kindia; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2018. [Google Scholar]
- Camara, I.M. Étude de la Dissémination des géo Helminthes dans le District de Samoreyah, Commune Rurale de Damakaniyah, Kindia; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2018. [Google Scholar]
- Camara, N. Diarrhée au Cours de l’Infection par le VIH/SIDA dans le Service d’Hématologie de l’Hôpital National Ignace-Deen: Prévalence, Clinique et Etiologie; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2018. [Google Scholar]
- Guilavogui, E. Prévalence des Parasitoses Intestinales chez Les enfants d’âge pré-Scolaire au Centre de Santé Madina de Conakry; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2018. [Google Scholar]
- Oularé, M.L. Les diarrhées de L’enfant au Service de Pédiatrie de L’hôpital Préfectoral de Kissidougou: Aspects épidémiologiques, cliniques et thérapeutiques; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2018. [Google Scholar]
- Ali, I.O. Prévalence des Helminthiases Intestinales chez les Enfants âgés de 2 à 14 ans Reçus en Consultation au Centre Mère-enfant Bernard Kouchner de Coronthie; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2018. [Google Scholar]
- Bamba, P. Prévalence des Helminthiases Intestinales dans la Zone Minière de Kamsar; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2018. [Google Scholar]
- Camara, O. Diarrhée Aiguë Chez les Enfants de 0 a 5 ans: Aspect Epidémiologique, Clinique et Thérapeutique au Service de Pédiatrie du CMC de Matam; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2018. [Google Scholar]
- Kolié, O. Prévalence des Parasitoses Intestinales à L’hôpital Régional de Kankan; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2018. [Google Scholar]
- Kéita, A. Prévalence du Parasitisme Intestinal en Milieu Carcéral de la Maison Centrale de Conakry; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2018. [Google Scholar]
- Onikoyamou, K.H. Prévalence de la Shistosomiase chez les Enfants reçus en Consulation à L’hôpital Régional de N’Zérékoré; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2018. [Google Scholar]
- Mara, F. Diarrhées Aigües chez les Enfants âgés de 0 à 59 mois au Service de Pédiatrie à L’hôpital Préfectoral de Kissidougou: Aspects Epidémiologiques, Cliniques et Thérapeutiques; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2018. [Google Scholar]
- Traoré, S. Prévalence des Parasitoses Intestinales chez les Patients Reçus en Consultation à la Clinique Nimba de Kamsar; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2018. [Google Scholar]
- Soumah, A. Prévalence des Helminthiases Intestinales Chez les Enfants de 0 à 15 ans Reçus en Consultation à L’hôpital Régional de Mamou; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2019. [Google Scholar]
- Toure, D.; Samoura, A.; Camara, L.; Camara, A.; Samoura, S.; Diallo, T. Intestinal Parasitoses in Co-infected Patients Tuberculosis/HIV: First investigation in Guinea. Jaccr Infect. 2019, 1, 16–21. [Google Scholar]
- Fofana, L. Gastro-Entérites Aigües Chez les Enfants de 0 à 5 ans au Service de Pédiatrie à L’hôpital Régional de Kanka: Aspects Epidémiologiques, Cliniques et Thérapeutiques; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2019. [Google Scholar]
- Gamou, C.E. Prévalence des Helminthiases Intestinales chez les Enfants d’âge Scolaire reçus en Consultation au Service de Pédiatrie à L’hôpital Préfectoral de Coyah; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2019. [Google Scholar]
- Diaby, F. Enquête sur la Prescription des Anti-Helminthiques au Service de Pédiatrie de L’hôpital Régional de Kindia; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2019. [Google Scholar]
- Diallo, M.S.M. Prévalence des Shistosomiases Mansoni dans la Commune Urbaine de N’Zérékoré; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2019. [Google Scholar]
- Traoré, S. Profil Epidémiologique des Parasitoses Intestinales chez les Enfants d’âge Scolaire Reçus au MCM Matam; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2019. [Google Scholar]
- Béavogui, S. Prévalence des Helminthiases Intestinales chez Les Enfants D’âge Scolaire dans le Quartier Bouzie, Commune Urbaine de Macenta; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2020. [Google Scholar]
- Condé, A.F. Analyse de la Prescription des Antiparasitaires Intestinaux chez les Femmes Enceintes au Service de Maternité du CMC de Ratoma; Bibliothèque Universitaire de l’Université Gamal Abdel Nasser: Conakry, Guinea, 2020. [Google Scholar]
- Clapier, I. Les bilharzioses dans la région militaire de la Guinée. Bull. Soc. Pathol. Exot. 1916, 9, 739–4717. [Google Scholar]
- Nozais, J.P. Results of a parasitologic survey carried out in 21 villages in Konkouré Valley (French Guinea). Preliminary study. Bull. Soc. Pathol. Exot. Fil. 1986, 79, 409–413. [Google Scholar]
- Jia, T.W.; Melville, S.; Utzinger, J.; King, C.H.; Zhou, X.N. Soil-transmitted helminth reinfection after drug treatment: Asystematic review and meta-analysis. PLoS Negl. Trop. Dis. 2012, 6, e1621. [Google Scholar] [CrossRef] [Green Version]
- Chávez-Ruvalcaba, F.; Chávez-Ruvalcaba, M.I.; Moran Santibañez, K.; Muñoz-Carrillo, J.L.; León Coria, A.; Reyna Martínez, R. Foodborne Parasitic Diseases in the Neotropics—A Review. Helminthologia 2021, 58, 119–133. [Google Scholar] [CrossRef] [PubMed]
- Mari, L.; Ciddio, M.; Casagrandi, R.; Perez-Saez, J.; Bertuzzo, E.; Rinaldo, A.; Sokolow, S.H.; De Leo, G.A.; Gatto, M. Heterogeneity in schistosomiasis transmission dynamics. J. Theor. Biol. 2017, 432, 87–99. [Google Scholar] [CrossRef] [PubMed]
- Augusto, G.; Nalá, R.; Casmo, V.; Sabonete, A.; Mapaco, L.; Monteiro, J. Geographic distribution and prevalence of schistosomiasis and soil-transmitted helminths among schoolchildren in Mozambique. Am. J. Trop. Med. Hyg. 2009, 81, 799–803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sacolo-Gwebu, H.; Chimbari, M.; Kalinda, C. Prevalence and risk factors of schis- tosomiasis and soil-transmitted helminthiases among preschool aged children (1–5 years) in rural KwaZulu-Natal, South Africa: A cross-sectional study. Infect. Dis. Poverty 2019, 8, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silver, Z.A.; Kaliappan, S.P.; Samuel, P.; Venugopal, S.; Kang, G.; Sarkar, R.; Ajjampur, S.S.R. Geographical distribution of soil transmitted helminths and the effects of community type in South Asia and South East Asia—A systematic review. PLoS Negl. Trop. Dis. 2018, 12, e0006153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ibrahim, T.; Zemene, E.; Asres, Y.; Seyoum, D.; Tiruneh, A.; Gedefaw, L.; Mekonnen, Z. Epidemiology of soil-transmitted helminths and S. mansoni: A base-line survey among school children, Ejaji, Ethiopia. J. Infect. Dev. Ctries. 2018, 12, 1134–1141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aemiro, A.; Menkir, S.; Tegen, D.; Tola, G. Prevalence of soil-transmitted helminthes and associated risk factors among people of Ethiopia: A systematic review and meta-analysis. Infect. Dis. 2022, 15, 11786337211055437. [Google Scholar] [CrossRef]
- Mekonnen, H.S.; Ekubagewargies, D.T. Prevalence and factors associated with intestinal parasites among under-five children attending Woreta Health Center, Northwest Ethiopia. BMC Infect. Dis. 2019, 19, 256. [Google Scholar] [CrossRef] [Green Version]
- Pazmiño, F.A.; Mora-Salamanca, A.F.; Mahecha, B.S.P.; Moreno, E.J.P.; Olivera, M.J.; Ospina, A.K.; López, M.C. Prevalence of intestinal parasitism in preschool and school children in Colombia: Systematic review and meta-analysis. Trop. Med. Int. Health 2022, 27, 781–794. [Google Scholar] [CrossRef]
- Khan, W.; Panhwar, W.A.; Mehmood, S.A.; Ahmed, S.; Ahmed, M.S.; Khan, N.; Khan, M.M.; Akram, W.; Ullah, S.; Imran. Pinworm infection in school children of four districts of Malakand region, Khyber Pakhtunkhwa, Pakistan. Braz. J. Biol. 2021, 82, e238769. [Google Scholar] [CrossRef]
- Wendt, S.; Trawinski, H.; Schubert, S.; Rodloff, A.C.; Mössner, J.; Lübbert, C. The diagnosis and treatment of pinworm infection. Dtsch. Arztebl. Int. 2019, 116, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Sangaré, I.; Guiguemdé, K.T.; Zida, A.; Sirima, C.; Sawadogo, P.M.; Cissé, M.; Assogba, S.B.; Guiguemdé, T.R.; Bamba, S. Prevalence of intestinal parasitic infections among pregnant women in Bobo-Dioulasso (Burkina Faso). Ann. Parasitol. 2021, 67, 489–497. [Google Scholar] [PubMed]
- Alula, G.A.; Munshea, A.; Nibret, E. Prevalence of intestinal parasitic infections and associated risk factors among pregnant women attending prenatal care in the Northwestern Ethiopia. Biomed. Res. Int. 2021, 2021, 3387742. [Google Scholar] [CrossRef] [PubMed]
- Wekesa, A.W.; Mulambalah, C.S.; Muleke, C.I.; Odhiambo, R. Intestinal helminth infections in pregnant women attending antenatal clinic at Kitale District Hospital, Kenya. J. Parasitol. Res. 2014, 2014, 823923. [Google Scholar] [CrossRef] [PubMed]
- Animaw, Z.; Melese, A.; Demelash, H.; Seyoum, G.; Abebe, A. Intestinal parasitic infections and associated factors among pregnant women in Ethiopia: A systematic review and meta-analysis. BMC Pregnancy Childbirth 2021, 21, 474. [Google Scholar] [CrossRef]
- Pan American Health Organization. Soil Transmitted Helminthiasis. Available online: https://www.paho.org/en/topics/soil-transmitted-helminthiasis (accessed on 1 January 2023).
- Ministère de la Santé et de l’Hygiène Publique. Analyse de la Situation des Maladies Tropicales Négligées en Guinée; Guinée. 2010. Available online: https://portail.sante.gov.gn/wp-content/uploads/2020/04/RTI-Analyse-Situation-2010.pdf (accessed on 1 January 2023).
- Pocaterra, L.A.; Ferrara, G.; Peñaranda, R.; Rojas, E.; Pérez-Chacón, G.; Hernán, A.; Certad, G.; Goldstein, C.; Núñez, L. Improved detection of Strongyloides stercoralis in modified agar plate cultures. Am. J. Trop. Med. Hyg. 2017, 96, 863–865. [Google Scholar] [CrossRef]
- Fletcher, S.M.; McLaws, M.L.; Ellis, J.T. Prevalence of gastrointestinal pathogens in developed and developing countries: Systematic review and meta-analysis. J. Public Health Res. 2013, 2, 42–53. [Google Scholar] [CrossRef] [Green Version]
- O’Leary, J.K.; Sleator, R.D.; Lucey, B. Cryptosporidium spp. diagnosis and research in the 21st century. Food Waterborne Parasitol. 2021, 24, e00131. [Google Scholar] [CrossRef]
- Nikolay, B.; Brooker, S.J.; Pullan, R.L. Sensitivity of diagnostic tests for human soil-transmitted helminth infections: A meta-analysis in the absence of a true gold standard. Int. J. Parasitol. 2014, 44, 765–774. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Guideline: Preventive Chemotherapy to Control Soil-Transmitted Helminth Infections in At-Risk Population Groups; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Target Population | Prevention Deworming Program | Frequency of Preventive Deworming | Administered Drugs (Doses) | |
|---|---|---|---|---|
| Before 2010 | No | No specific program | NA | Prazinquatel (600 mg), Mebendazol (500 mg) |
| 2010–2013 | Children between 5 and 12 years old assisting school and adults | One-time programs | Not periodically | Prazinquatel (600 mg), Albendazole (400 mg) or Mebendazol (500 mg) |
| After 2014 | Populations aged 5 years and older | Mass treatment integrated in campaigns for lymphatic filariasis and onchocerciasis | Once a year | Prazinquatel (600 mg), Albendazole (400 mg) or Mebendazol (500 mg) |
| Rank | Study Population Type (Age if Children) | Year of Observation | Study Area | Study Setting | Nb Included (Prevalence %) | Type of Parasite (Number of Cases) | Diagnostic Technique | References |
|---|---|---|---|---|---|---|---|---|
| 1 | Adult and children (1–17 years) | 2006 | Conakry (Urban) | Hospital | 800 (23) | S. stercoralis (4), A. duodenale (42), A. lumbricoides (40), E. histolytica (27), E. vermicularis (3), S. mansoni (6), Tapeworm (11), Trichine (32), T. intestinalis (21) | A, D | Touré N., 2010, PharmD [20] |
| 2 | Children (1–17 years) | 2008–2009 | Conakry (Urban) | School | 306 (43) | S. stercoralis (11), A. duodenale (24), A. lumbricoides (37), E. histolytica (21), E. vermicularis (3), S. mansoni (1), Tapeworm (6), Trichine (20), T. intestinalis (9) | A, D | Diallo G., 2010, PharmD [21] |
| 3 | Adult and children (1–17 years) | 2009 | Conakry (Urban) | Hospital | 420 (42) | S. stercoralis (11), A. duodenale (41), A. lumbricoides (102), S. mansoni (8), Tapeworm (6), T. trichiura (7) | A, D | Assoumani M., 2010, PharmD [22] |
| 4 | Children (6–14 years) | 2010 | Lower Guinea (Kindia, Urban) | Community | 612 (66) | S. stercoralis (9), A. duodenale (89), A. lumbricoides (113), E. histolytica (22), E. vermicularis (2), S. mansoni (86), Tapeworm (20), T. trichiura (12), T. intestinalis (48) | A, D | Camara A.B., 2010, PharmD [23] |
| 5 | Children (0–5 years) | 2007 | Conakry (Urban) | School | 254 (80) | S. stercoralis (1), A. duodenale (23), A. lumbricoides (127), E. histolytica (7), S. mansoni (9), T. trichiura (26), T. intestinalis (9) | A, D | Diallo S.M.C., 2011, PharmD [24] |
| 6 | Children (5–17 years) | 2008 | Conakry (Urban) | School | 300 (46) | S. stercoralis (2), A. duodenale (5), A. lumbricoides (104), E. histolytica (4), H. nana (3), S. mansoni (5), Tapeworm (3), T. trichiura (2), T. intestinalis (10) | A, D | Kolié F., 2011, PharmD [25] |
| 7 | Adults and children (1–17 years) | 2008 | Conakry (Urban) | Hospital | 703 (87) | S. stercoralis (13), A. duodenale (73), A. lumbricoides (207), E. histolytica (105), E. vermicularis (58), Tapeworm (62), T. intestinalis (92) | A, D | Koné M.C., 2011, PharmD [26] |
| 8 | Adults and children (1–17 years) | 2009 | Conakry (Urban) | Hospital | 300 (37) | S. stercoralis (5), A. duodenale (6), A. lumbricoides (32), E. histolytica (21), E. vermicularis (5), H. nana (5), S. mansoni (7), Tapewrom (26), T. trichiura(4) | A, D | Diallo A.A., 2011, PharmD [27] |
| 9 | Adults and children (1–17 years) | 2009 | Conakry (Urban) | Hospital | 716 (47) | S. stercoralis (6), A. duodenale (8), A. lumbricoides (218), E. histolytica (58), E. vermicularis (1), S. mansoni (5), Tapeworm (39), T. trichiura (1), T. intestinalis (1) | A, D | Simpogui F.T., 2011, PharmD [28] |
| 10 | Children (2–17 years) | 2009 | Conakry (Urban) | Orphanat | 99 (43) | A. lumbricoides (38), S. mansoni (1), Tapeworm (4) | A, D | Tidjani A., 2011, PharmD [29] |
| 11 | Children (9–14 years) | 2010 | Forest Guinea (Beyla and Macenta, Mixed) | School or community | 420 (80) | A. duodenale (101), A. lumbricoides (34), S. mansoni (278), T. trichiura (10) | A, C | Hodges et al., 2011 [30] |
| 12 | Pregnant women | 2011 | Conakry (Urban) | Hospital | 186 (47) | A. duodenale (10), A. lumbricoides (3), E. histolytica (4), E. vermicularis (5), S. mansoni (48), Tapeworm (8), T. trichiura (6), T. intestinalis (3) | A, D | Bilivogui F.G., 2011, PharmD [31] |
| 13 | Adults and children (1–17 years) | 2010 | Conakry and Lower Guinea (Kindia, Urban) | Community | 4717 (42) | S. stercoralis (87), A. duodenale (556), A. lumbricoides (519), E. vermicularis (26), S. mansoni (242), Tapeworm (242), T. trichiura (303) | A, D | Barry A.R., 2012, PharmD [32] |
| 14 | Adults and children (0–15 years) | 2010 | Forest Guinea (N’Zérékoré, Urban) | Hospital | 452 (39) | S. stercoralis (12), S. mansoni (165) | A, C | Kolié L., 2012, PharmD [33] |
| 15 | Pregnant women | 2011 | Conakry (Urban) | Hospital | 121 (59) | S. stercoralis (12), A. duodenale (5), A. lumbricoides (29), E. histolytica (11), S. mansoni (3), Tapeworm (5), T. intestinalis (6) | A, D | Hounsanou E.L.D., 2012, PharmD [34] |
| 16 | Children (0–5 years) | 2012 | Middle Guinea (Mamou, Mixed) | Hospital | 208 (46) | S. stercoralis (15), A. lumbricoides (41), E. histolytica (1), E. vermicularis (8), G. intestinalis (17), S. mansoni (1), T. trichiura (7), T. intestinalis (6) | X | Camara A.M., 2012, MD [35] |
| 17 | Adult and children (1–17 years) | 2012 | Forest Guinea (Macenta, Mixed | Community | 515 (100) | A. duodenale (156), A. lumbricoides (124), E. vermicularis (12), S. mansoni (203), Tapeworm (10), Trichine (10) | A, D | Bilivogui A., 2013, PharmD [36] |
| 18 | Adults | 2012 | Conakry (Urban) | University | 117 (68) | A. duodenale (1), A. lumbricoides (66), E. vermicularis (1), H. nana (1), Tapeworm (10) | A, D | Béavogui O.K., 2013, PharmD [37] |
| 19 | Pregnant women (15–17 years) | 2012 | Conakry (Urban) | Hospital | 1975 (50) | S. stercoralis (139), A. duodenale (159), A. lumbricoides (199), E. histolytica (70), E. vermicularis (90), S. mansoni (50), Tapeworm (109), T. trichiura (179) | X | Condé M., 2013, PharmD [38] |
| 20 | Adults and children (0–17 years) | 2012 | Conakry (Urban) | Community | 714 (53) | S. stercoralis (6), A. duodenale (35), A. lumbricoides (180), E. vermicularis (10), F. buski (50), H. nana (30), T. trichiura (70) | A, D | Kéita D., 2013, PharmD [39] |
| 21 | Children (1–17 years) | 2012 | Forest Guinea (Beyla, Mixed) | Community | 779 (46) | A. duodenale (53), A. lumbricoides (24), S. mansoni (273), Tapeworm (7), Trichine (2) | A, D | Pricemou P., 2013, PharmD [40] |
| 22 | Pregnant women | 2012 | Conakry (Conakry, Urban) | Hospital | 1488 (66) | S. stercoralis (93), A. duodenale (103), A. lumbricoides (165), E. histolytica (203), E. vermicularis (133), S. mansoni (145), Tapeworm (57), T. intestinalis (83) | A, B, D | Sow S., 2013, PharmD [41] |
| 23 | Adults and children (1–17 years) | 2012 | Conakry (Urban) | Hospital | 3705 (27) | Helminths (1000) | X | Touré F., 2013, PharmD [42] |
| 24 | Children (1–17 years) | 1989 | Upper Guinea (Siguiri, Mixed | Community | 1532 (70) | S. stercoralis (66), A. duodenale (298), A. lumbricoides (200), E. histolytica (65), G. intestinalis 6), H. nana (62), S. mansoni (119), Tapeworm (147), Trichine (113) | A, C, D | Diaby K., 2014, PharmD [43] |
| 25 | Adults and children (1–17 years) | 2012 | Forest Guinea (Macenta, Mixed) | Community | 425 (52) | A. duodenale (74), A. lumbricoides (53), E. histolytica (11), E. vermicularis (8), S. mansoni (66), Tapeworm (5), Trichine (2) | A, D | Guilavogui D., 2014, PharmD [44] |
| 26 | Malnourished children (0–5 years) | 2013 | Forest Guinea (N’Zérékoré, Urban) | Hospital | 62 (74) | S. stercoralis (1), A. duodenale (9), A. lumbricoides (15), E. histolytica (5), E. vermicularis (4), G. intestinalis (4), S. mansoni (5), Tapeworm (3) | A, D | Koïvogui F., 2014, MD [45] |
| 27 | Children (0–5 years) | 2013 | Forest Guinea (N’Zérékoré, Urban) | Hospital | 400 (51) | A. duodenale (60), A. lumbricoides (66), S. mansoni (39), Tapeworm (6), T. trichiura (12), T. intestinalis (22) | A, D | Lamah L.S., 2014, PharmD [46] |
| 28 | Children (1–17 years) | 2013 | Conakry (Urban) | School | 200 (34) | A. duodenale (14), A. lumbricoides (18), H. nana (10), T. trichiura (6), T. intestinalis (20) | A, D | Sano F., 2015, PharmD [47] |
| 29 | Pregnant women (1–17 years) | 2014 | Upper Guinea (Siguiri, Mixed) | Hospital | 975 (70) | S. stercoralis (110), A. duodenale (128), A. lumbricoides (163), E. histolytica (52), E. vermicularis (87), S. mansoni (43), Tapeworm (99) | X | Camara M.S., 2015, PharmD [48] |
| 30 | Pregnant women | 2014 | Forest Guinea (N’Zérékoré, Mixed) | Hospital | 780 (100) | S. stercoralis (126), A. duodenale (144), A. lumbricoides (156), S. mansoni (179), Tapeworm (71), T. trichiura (96), T. intestinalis (8) | A, D | Diabaté M., 2015, PharmD [49] |
| 31 | Adults and children VIH and TB (16–17 years) | 2014 | Conakry (Urban) | Hospital | 123 (76) | S. stercoralis (1), A. duodenale (8), A. lumbricoides (44), Cryptosporidium (34), E. vermicularis (3), G. intestinalis (1), H. nana (1), I. belli (1), S. mansoni (1) | A, D, E | Gbamou R.N., 2015, PharmD [50] |
| 32 | Pregnant women (13–17 years) | 2014 | Lower Guinea (Kindia, Urban) | Hospital | 200 (50) | S. stercoralis (10), A. duodenale (13), A. lumbricoides (36), E. histolytica (10), S. mansoni (9), Tapeworm (10), T. trichiura (12) | A | Hamza S.A., 2015, MSc [51] |
| 33 | Children (3–17 years) | 2014 | Conakry (Urban) | Hospital | 780 (82) | S. stercoralis (7), A. duodenale (13), A. lumbricoides (390), E. vermicularis (7), H. nana (52), S. mansoni (20), Tapeworm (13), T. trichiura (138) | A, F | Moutsinga M.L.A., 2015, MSc [52] |
| 34 | Children (0–5 years) | 2014 | Forest Guinea (Macenta, Mixed) | Hospital | 300 (41) | S. stercoralis (3), A. duodenale (22), A. lumbricoides (7), E. histolytica (32), S. mansoni (10), Tapeworm (23), T. trichiura (11), T. intestinalis (15) | A, B | Zoumanigui W., 2015, PharmD [53] |
| 35 | Children (1–17 years) | 2015 | Middle Guinea (Dalaba, Mixed) | School | 430 (50) | S. stercoralis (19), A. duodenale (5), A. lumbricoides (34), S. mansoni (69), Tapeworm (84), T. trichiura 2) | A, D | Bah M.S., 2016, PharmD [54] |
| 36 | Children (0–15 years) | 2015 | Forest Guinea (Guéckedou, Mixed) | Hospital | 820 (31) | A. duodenale (26), A. lumbricoides (156), S. mansoni (64), Tapeworm (4) | X | Sylla I.M., 2016, MD [55] |
| 37 | Adults and children (1–17 years) | 2015–2016 | Conakry (Urban) | Hospital | 407 (76) | S. stercoralis (53), A. duodenale (40), A. lumbricoides (62), S. mansoni (47), Tapeworm (62), T. trichiura (47) | A | Camara A.K., 2016, MSc [56] |
| 38 | Children (5–15 years) | 2017 | Middle Guinea (Labé, Urban) | Hospital | 372 (55) | S. stercoralis (5), A. lumbricoides (112), S. mansoni (11), Tapeworm (75) | A, B, D | DialloT.B., 2016, PharmD [57] |
| 39 | Adults and children (1–17 years) | 2016 | Middle Guinea (Labé, Urban) | Hospital | 454 (41) | A. duodenale (12), A. lumbricoides (105), E. histolytica (6), E. vermicularis (4), S. mansoni (10), Tapeworm (46), T. trichiura (3) | A | Baldé A.S., 2017, MSc [58] |
| 40 | Pregnant women | 2016 | Conakry (Urban) | Hospital | 384 (26) | S. stercoralis (2), A. duodenale (11), A. lumbricoides (59), B. coli (1), E. histolytica (1), S. mansoni (7), Tapeworm (15), Trichine (3), T. intestinalis (1) | A, D | Fotio C.S., 2017, PharmD [59] |
| 41 | Children (1–17 years) | 2016 | Conakry (Urban) | School | 322 (43) | S. stercoralis (3), A. duodenale (5), A. lumbricoides (62), E. vermicularis (19), S. mansoni (7), Tapeworm (22), T. trichiura (21) | A, D | Kouyaté M., 2017, PharmD [60] |
| 42 | Children (0–15 years) | 2016 | Forest Guinea (N’Zérékoré, Mixed) | Hospital | 504 (16) | Helminths (79) | X | Loua C., 2017, PharmD [61] |
| 43 | Children (0–5 years) | 2017 | Conakry (Urban) | Hospital | 211 (27) | A. duodenale (6), A. lumbricoides (25), E. histolytica (9), S. mansoni (1), Tapeworm (11), T. intestinalis (5) | A, D | Kengni M.O., 2017, PharmD [62] |
| 44 | Adults and children (1–17 years) | 2017 | Conakry (Urban) | Hospital | 354 (11) | S. stercoralis (2), A. lumbricoides (7), E. histolytica (7), E. vermicularis (1), S. mansoni (11), Tapeworm (9), T. trichiura (1) | A, B, D | Loua B., 2017, PharmD [63] |
| 45 | Children (0–5 years) | 2017 | Forest Guinea (Lola, Urban) | Hospital | 160 (32) | A. lumbricoides (33), E. histolytica (15), Tapeworm (3) | A | Sagno I., 2017 MD [64] |
| 46 | Malnourished children (0–3 years) | 2015 | Conakry (Urban) | Hospital | 220 (27) | A. lumbricoides (33), B. coli (11), E. vermicularis (13), Tapeworm (2) | A, D | Sidibé S et al., 2018 [3] |
| 47 | Pregnant women (16–42 years) | 2016 | Conakry (Urban) | Hospital | 3571 (11) | S. stercoralis (27), A. duodenale (28), A. lumbricoides (91), E. histolytica (125), E. vermicularis (36), S. mansoni (29), Tapeworm (34), T. trichiura (23) | X | AbderamanI.B, 2018, PharmD [65] |
| 48 | Adults and children (1–17 years) | 2016 | Lower Guinea (Kindia, Urban) | Community | 152 (34) | S. mansoni (52) | A, C | Bah O., 2018 Master [66] |
| 49 | Adults and children (1–17 years) | 2016 | Lower Guinea (Kindia, Mixed) | Community | 477 (53) | S. stercoralis (5), A. duodenale (65), A. lumbricoides (181), T. trichiura (1) | A, C, D | Camara I.M., 2018, Master [67] |
| 50 | Human immunodeficiency virus (HIV) + adults and children (5–17 years) | 2016 | Conakry (Urban) | Hospital | 38 (24) | S. stercoralis (1), A. duodenale (1), E. histolytica (3), G. intestinalis (1), S. mansoni (1), T. intestinalis (2) | X | Camara N., 2018, MD [68] |
| 51 | Children (3–5 years) | 2016 | Conakry (Urban) | Hospital | 238 (29) | S. stercoralis (3), A. duodenale (4), A. lumbricoides (27), E. histolytica (13), E. vermicularis (10), G. intestinalis (6), Tapeworm (3), T. trichiura (3) | A, D | Guilavogui E., 2018, PharmD [69] |
| 52 | Children (0–15 years) | 2016–2017 | Forest Guinea (Kissidougou, Urban) | Hospital | 265 (25) | A. duodenale (48), E. histolytica (9), S. mansoni (10) | A, F | Oularé M.L., 2018, MD [70] |
| 53 | Children (2–14 years) | 2017 | Conakry (Urban) | Hospital | 384 (25) | S. stercoralis (5), A. lumbricoides (6), H. diminuta (13), H. nana (24), S. mansoni (15), Tapeworm (23), T. trichiura (11) | A, B, D | Ali I.O., 2018, PharmD [71] |
| 54 | Adults and children (1–17 years) | 2017 | Lower Guinea (Kamsar, Mixed) | Community | 364 (42) | S. stercoralis (10), A. duodenale (19), A. lumbricoides (64), E. vermicularis (9), S. mansoni (11), Tapeworm (26), Trichine (12) | A, D | Bamba P., 2018, PharmD [72] |
| 55 | Children (0–5 years) | 2017 | Conakry (Urban) | Hospital | 291 (25) | A. lumbricoides (36), E. histolytica (32), Tapeworm (4) | A | Camara O., 2018, MD [73] |
| 56 | Adults and children (5–17 years) | 2017 | Upper Guinea (Kankan, Urban= | Hospital | 340 (86) | S. stercoralis (1), A. duodenale (91), A. lumbricoides (103), F. s buski (1), S. mansoni (88), Tapeworm (8) | A, C, D | Kolié O. 2018, PharmD [74] |
| 57 | Adults jailed | 2017 | Conakry (Urban) | Jail | 330 (32) | S. stercoralis (7), A. duodenale (37), A. lumbricoides (10), E. histolytica (1), S. mansoni (47), Tapeworm (1), Trichine (2) | A, D | Kéita A., 2018, PharmD [75] |
| 58 | Adults and children (0–17 years) | 2017 | Forest Guinea (N’Zérékoré, Mixed) | Hospital | 437 (41) | S. stercoralis (12), A. duodenale (56), A. lumbricoides (84), E. histolytica (2), Tapeworm (20), T. trichiura (6), | A, C | Onikoyamou K.H., 2018, MSc [76] |
| 59 | Children (0–5 years) | 2017 | Forest Guinea (Kissidougou, Urban) | Hospital | 403 (18) | A. duodenale (12), A. lumbricoides (23), E. histolytica (7), S. mansoni (19), Tapeworm (11) | X | Mara F., 2018, MD [77] |
| 60 | Adults and children (2–17 years) | 2017 | Lower Guinea (Kamsar, Urban) | Hospital | 300 (70) | S. stercoralis (1), A. duodenale (23), A. lumbricoides (82), E. histolytica (27), E. vermicularis (65), S. mansoni (1), Tapeworm (8), T. trichiura (3) | A | Traoré S., 2018, MSc [78] |
| 61 | Children (0–15 years) | 2017–2018 | Middle Guinea (Mamou, Mixed) | Hospital | 590 (39) | A. duodenale (35), A. lumbricoides (129), S. mansoni (67) | A, C, D | Soumah A., 2019, MSc [79] |
| 62 | Adults and children living with HIV (16–17 years) | 2014 | Conakry (Urban) | Hospital | 123 (82) | S. stercoralis (1), A. duodenale (8), A. lumbricoides (44), Cryptosporidium (33), E. histolytica (8) E. vermicularis (3), G. intestinalis (1), H. nana (1), I. belli (1), S. mansoni (2) | A, D, E | Toure D et al., 2019 [80] |
| 63 | Children (0–5 years) | 2016 | Upper Guinea (Kankan, Mixed) | Hospital | 820 (15) | A. lumbricoides (73), E. histolytica (38), G. intestinalis (16) | A | Fofana L., 2019, MD [81] |
| 64 | Children (5–15 years) | 2017 | Lower Guinea (Coyah, Mixed) | Hospital | 300 (19) | S. stercoralis (7), A. duodenale (27), A. lumbricoides (7), H. nana (2), S. mansoni (13), T. trichiura (2) | A, B, D | Gamou C.E., 2019, PharmD [82] |
| 65 | Children (0–14 years) | 2018 | Lower Guinea (Kindia, Urban) | Hospital | 665 (38) | A. duodenale (37), A. lumbricoides (132), E. vermicularis (53), Tapeworm (29) | A, D | Diaby F., 2019, PharmD [83] |
| 66 | Adults and Children (1–17 years) | 2018 | Forest Guinea (N’Zérékoré, Mixed) | Community | 2655 (53) | S. stercoralis (1), A. duodenale (10), A. lumbricoides (16), E. histolytica (3), E. vermicularis (1), Tapeworm (30), Trichine (3), T. trichiura (1), T. intestinalis (3), S. mansoni (1330) | A | Diallo M.S.M., 2019, Master [84] |
| 67 | Children (5–15 years) | 2019 | Conakry (Urban) | Hospital | 315 (23) | S. stercoralis (1), A. duodenale (8), A. lumbricoides (37), Balantidium coli (1), E. histolytica (7) S. mansoni (3), Tapeworm (11), T. intestinalis (5) | A, C, D | Traoré S., 2019, PharmD [85] |
| 68 | Adults and children (6–12 years) | 2017 | Forest Guinea (Macenta, Urban) | Community | 424 (100) | S. stercoralis (69), A. duodenale (26), A. lumbricoides (96), S. mansoni (24), Tapeworm (128), Trichine (81) | A, C, D | Béavogui S., 2020, PharmD [86] |
| 69 | Pregnant women | 2019 | Conakry (Urban) | Hospital | 382 (76) | S. stercoralis (43), A. duodenale (81), A. lumbricoides (66), E. histolytica (40) E. vermicularis (41), Tapeworm (6), T. trichiura (15) | X | Condé A.F., 2020, PharmD [87] |
| Parasites | N° of Studies | Sample Size | Cases | Prevalence (%) (95% CI) * | Heterogeneity | |
|---|---|---|---|---|---|---|
| p-Value | I2 (%) | |||||
| A. lumbricoides | 61 | 38,279 | 5477 | 15 (12, 18) | 0 | 98 |
| A. duodenale | 57 | 36,849 | 3114 | 6 (5, 8) | 0 | 97 |
| S. mansoni | 55 | 35,256 | 3966 | 5 (3, 7) | 0 | 99 |
| E. histolytica | 37 | 22,374 | 1044 | 4 (3, 5) | <0.01 | 93 |
| Tapeworms | 53 | 35,095 | 1677 | 3 (2, 4) | <0.01 | 96 |
| H. nana | 10 | 4573 | 188 | 3 (2, 5) | <0.01 | 73 |
| E. vermicularis | 34 | 26,965 | 816 | 2 (1, 3) | <0.01 | 95 |
| S. stercoralis | 46 | 31,785 | 1028 | 2 (1, 3) | <0.01 | 95 |
| T. trichiura | 32 | 24,193 | 1041 | 2 (1, 3) | <0.01 | 95 |
| G. intestinalis | 8 | 3144 | 52 | 2 (1, 4) | <0.01 | 86 |
| T. intestinalis | 20 | 10,977 | 369 | 2 (1, 4) | <0.01 | 91 |
| Trichine | 13 | 9068 | 280 | 1 (0, 3) | <0.01 | 95 |
| Prevalence * with 95% CI ** | ||||||
|---|---|---|---|---|---|---|
| Conakry | Lower Guinea | Forest Guinea | Middle Guinea | Upper Guinea | p Value | |
| S. stercoralis | 1 (1, 2) | 2 (1, 2) | 1 (0, 6) | 4 (2, 6) | 1 (0, 1) | 0.21 |
| A. duodenale | 4 (3, 5) | 9 (6, 12) | 9 (5, 17) | 3 (1, 6) | 22 (18, 28) | <0.01 *** |
| A. lumbricoides | 19 (14, 26) | 17 (9, 31) | 10 (5, 17) | 19 (13, 28) | 16 (8, 27) | <0.01 *** |
| E. vermicularis | 1 (1, 3) | 4 (1, 16) | 1 (0, 6) | 2 (1, 5) | 5 (3, 6) | <0.01 *** |
| S. mansoni | 1 (1, 2) | 5 (1, 19) | 15 (8, 27) | 4 (1, 11) | 15 (6, 31) | <0.01 *** |
| Tapeworms | 3 (2, 4) | 4 (3, 6) | 2 (1, 5) | 16 (11, 22) | 5 (2, 13) | <0.01 *** |
| Trichine | 0 (0, 13) | 3 (2, 6) | 1 (0, 5) | - | 7 (6, 9) | <0.01 *** |
| T. trichiura | 3 (1, 6) | 1 (0, 2) | 1 (0, 4) | 1 (0, 3) | - | <0.01 *** |
| H. nana | 3 (2, 6) | 1 (0, 2) | - | - | 4 (3, 5) | 0.04 *** |
| G. intestinalis | 2 (1, 3) | - | 6 (2, 16) | 8 (5, 13) | 1 (0, 3) | <0.01 *** |
| E. histolytica | 5 (3, 7) | 6 (3, 11) | 2 (1, 6) | 1 (1, 2) | 4 (3, 5) | <0.01 *** |
| T. intestinalis | 3 (2, 6) | 8 (6, 10) | 1 (0, 11) | 3 (1, 6) | - | <0.01 *** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guilavogui, T.; Verdun, S.; Koïvogui, A.; Viscogliosi, E.; Certad, G. Prevalence of Intestinal Parasitosis in Guinea: Systematic Review of the Literature and Meta-Analysis. Pathogens 2023, 12, 336. https://doi.org/10.3390/pathogens12020336
Guilavogui T, Verdun S, Koïvogui A, Viscogliosi E, Certad G. Prevalence of Intestinal Parasitosis in Guinea: Systematic Review of the Literature and Meta-Analysis. Pathogens. 2023; 12(2):336. https://doi.org/10.3390/pathogens12020336
Chicago/Turabian StyleGuilavogui, Timothé, Stéphane Verdun, Akoï Koïvogui, Eric Viscogliosi, and Gabriela Certad. 2023. "Prevalence of Intestinal Parasitosis in Guinea: Systematic Review of the Literature and Meta-Analysis" Pathogens 12, no. 2: 336. https://doi.org/10.3390/pathogens12020336