
HPV and Cervical Cancer: A Review of Epidemiology and Screening Uptake in the UK


{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Epidemiology of Cervical Cancer
3. Introduction of HPV
3.1. HPV Subtypes
3.2. HPV Transmission
4. Pathophysiology of HPV-Related Malignancy
5. Other Risk Factors
5.1. Smoking
5.2. Oral Contraceptive Pill
5.3. Immunosuppression
5.4. Sexual Behavioural Factors
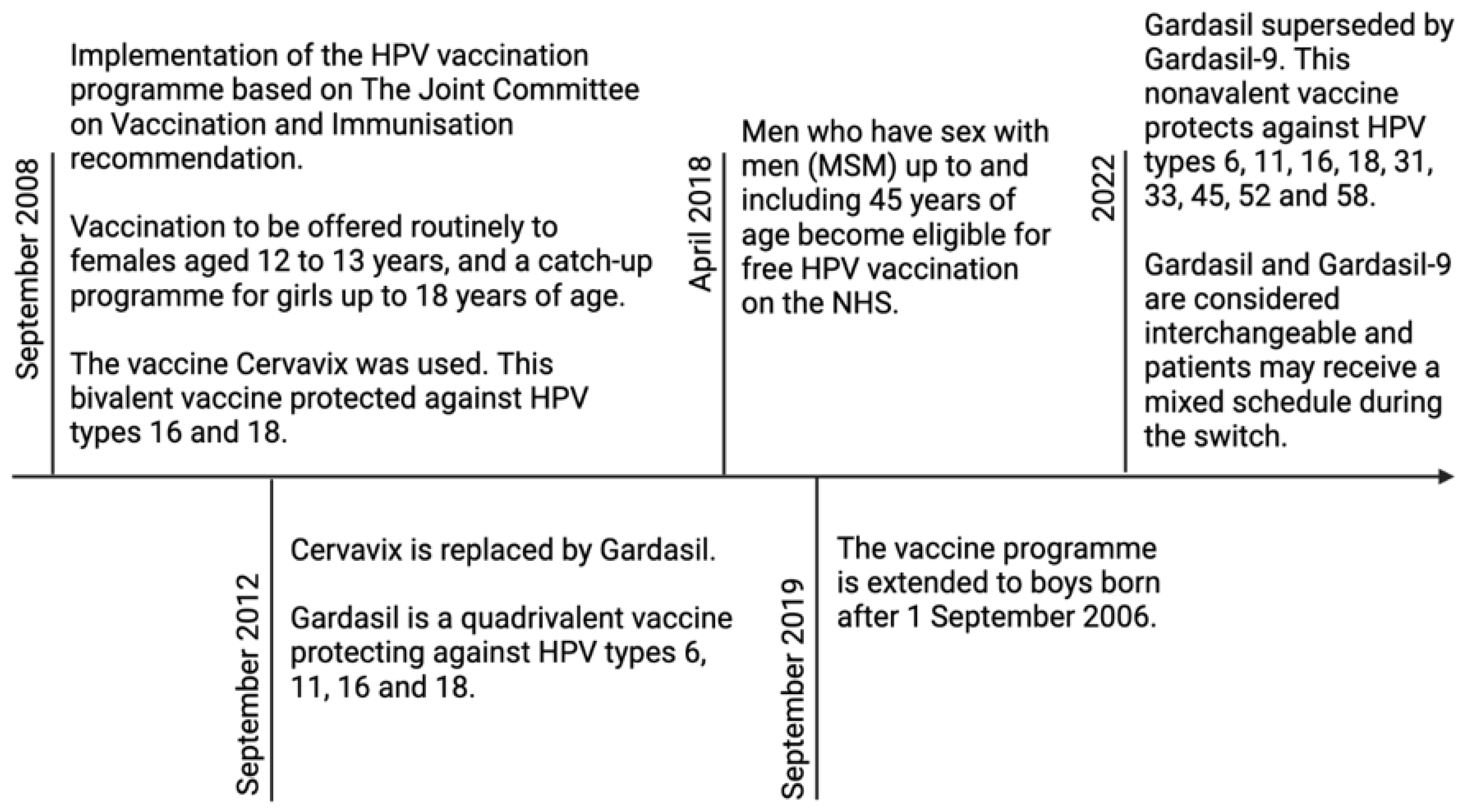
6. Current NHS Programmes—HPV Vaccination
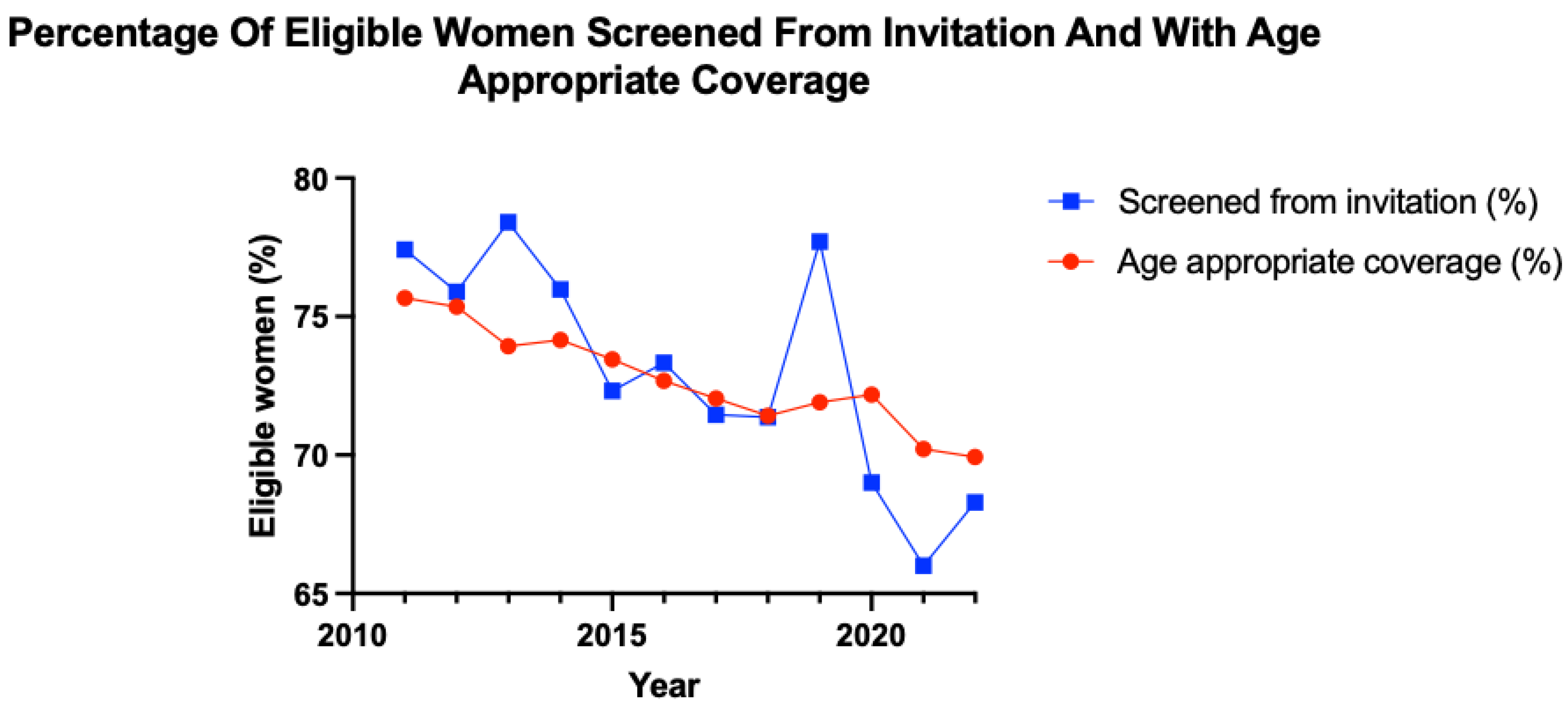
7. Current NHS Programmes—Cervical Cancer Screening
8. The Effect of Coronavirus Pandemic on Cervical Cancer Screening Uptake
9. Socioeconomic Factors on Cervical Cancer Screening Uptake
10. Future Direction
11. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Luckett, R.; Feldman, S. Impact of 2-, 4- and 9-valent HPV vaccines on morbidity and mortality from cervical cancer. Hum. Vaccin. Immunother. 2015, 12, 1332–1342. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA. Cancer. J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Cervical Cancer Statistics. Cancer Research UK. 2015. Available online: https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/cervical-cancer (accessed on 9 January 2023).
- Okunade, K.S. Human Papillomavirus and Cervical Cancer. J. Obstet. Gynaecol. 2020, 40, 602–608. [Google Scholar] [CrossRef] [PubMed]
- Cohen, P.A.; Jhingran, A.; Oaknin, A.; Denny, L. Cervical cancer. Lancet 2019, 393, 169–182. [Google Scholar] [CrossRef]
- Boussios, S.; Seraj, E.; Zarkavelis, G.; Petrakis, D.; Kollas, A.; Kafantari, A.; Assi, A.; Tatsi, K.; Pavlidis, N.; Pentheroudakis, G. Management of patients with recurrent/advanced cervical cancer beyond first line platinum regimens: Where do we stand? A literature review. Crit. Rev. Oncol. Hematol. 2016, 108, 164–174. [Google Scholar] [CrossRef] [PubMed]
- McLachlan, J.; Boussios, S.; Okines, A.; Glaessgen, D.; Bodlar, S.; Kalaitzaki, R.; Taylor, A.; Lalondrelle, S.; Gore, M.; Kaye, S.; et al. The Impact of Systemic Therapy Beyond First-line Treatment for Advanced Cervical Cancer. Clin. Oncol. (R Coll. Radiol.) 2017, 29, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Ghose, A.; Gullapalli, S.V.N.; Chohan, N.; Bolina, A.; Moschetta, M.; Rassy, E.; Boussios, S. Applications of Proteomics in Ovarian Cancer: Dawn of a New Era. Proteomes 2022, 10, 16. [Google Scholar] [CrossRef]
- Ramírez-Torres, A.; Gil, J.; Contreras, S.; Ramírez, G.; Valencia-González, H.A.; Salazar-Bustamante, E.; Gómez-Caudillo, L.; García-Carranca, A.; Encarnación-Guevara, S. Quantitative Proteomic Analysis of Cervical Cancer Tissues Identifies Proteins Associated with Cancer Progression. Cancer Genom. Proteom. 2022, 19, 241–258. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Xu, H.; Zhang, L.; Qiao, Y. Cervical cancer: Epidemiology, risk factors and screening. Chin. J. Cancer. Res. 2020, 32, 720–728. [Google Scholar] [CrossRef]
- Green, J.; Berrington de Gonzalez, A.; Sweetland, S.; Beral, V.; Chilvers, C.; Crossley, B.; Deacon, J.; Hermon, C.; Jha, P.; Mant, D.; et al. Risk factors for adenocarcinoma and squamous cell carcinoma of the cervix in women aged 20-44 years: The UK National Case-Control Study of Cervical Cancer. Br. J. Cancer 2003, 89, 2078–2086. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Cervical Cancer. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/cervical-cancer (accessed on 9 January 2023).
- Pesola, F.; Sasieni, P. Impact of screening on cervical cancer incidence in England: A time trend analysis. BMJ. Open. 2019, 9, e026292. [Google Scholar] [CrossRef] [PubMed]
- Cervical Cancer Incidence Statistics. Cancer Research UK. 2015. Available online: https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/cervical-cancer/incidence (accessed on 19 December 2022).
- Tota, J.; Franco, E.L. Effectiveness of cervical cancer screening at different ages. Womens Health 2009, 5, 613–616. [Google Scholar] [CrossRef]
- Cervical Screening: Programme Overview. GOV.UK. 2021. Available online: https://www.gov.uk/guidance/cervical-screening-programme-overview (accessed on 31 December 2022).
- Mendes, D.; Mesher, D.; Pista, A.; Baguelin, M.; Jit, M. Understanding differences in cervical cancer incidence in Western Europe: Comparing Portugal and England. Eur. J. Public Health 2018, 28, 343–347. [Google Scholar] [CrossRef]
- Schiffman, M.H.; Castle, P. Epidemiologic Studies of a Necessary Causal Risk Factor: Human Papillomavirus Infection and Cervical Neoplasia. J. Natl. Cancer. Inst. 2003, 95, E2. [Google Scholar] [CrossRef] [PubMed]
- Mesher, D.; Cuschieri, K.; Hibbitts, S.; Jamison, J.; Sargent, A.; Pollock, K.G.; Powell, N.; Wilson, R.; McCall, F.; Fiander, A.; et al. Type-specific HPV prevalence in invasive cervical cancer in the UK prior to national HPV immunisation programme: Baseline for monitoring the effects of immunisation. J. Clin. Pathol. 2015, 68, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Huang, X.; Zhang, Y. Involvement of Human Papillomaviruses in Cervical Cancer. Front. Microbiol. 2018, 9, 2896. [Google Scholar] [CrossRef]
- Dempsey, A.F. Human Papillomavirus: The Usefulness of Risk Factors in Determining Who Should Get Vaccinated. Rev. Obstet. Gynecol. 2008, 1, 122–128. [Google Scholar]
- Jayasinghe, Y.; Garland, S.M. Genital warts in children: What do they mean? Arch. Dis. Child. 2006, 91, 696–700. [Google Scholar] [CrossRef]
- World Health Organization. Cervical Cancer Elimination Initiative. 2022. Available online: https://www.who.int/initiatives/cervical-cancer-elimination-initiative (accessed on 9 January 2023).
- Graham, S. Human papillomavirus: Gene expression, regulation and prospects for novel diagnostic methods and antiviral therapies. Future. Microbiol. 2010, 5, 1493–1506. [Google Scholar] [CrossRef]
- Jendoubi-Ferchichi, M.; Satouri, L.; Ghoul, F.; Malek-Mellouli, M.; Derbel, A.M.; Makni, M.K.; Reziga, H.; Baba, A.; Zili, M.; Segondy, M.; et al. Phylogeny and Classification of Human Papillomavirus (HPV)16 and HPV18 Variants Based on E6 and L1 genes in Tunisian Women with Cervical Lesions. Asian Pac. J. Cancer Prev. 2018, 19, 3361–3366. [Google Scholar] [CrossRef] [PubMed]
- Williams, V.M.; Filippova, M.; Soto, U.; Duerksen-Hughes, P.J. HPV-DNA integration and carcinogenesis: Putative roles for inflammation and oxidative stress. Future Virol. 2011, 6, 45–57. [Google Scholar] [CrossRef] [Green Version]
- Burd, E.M. Human Papillomavirus and Cervical Cancer. Clin. Microbiol. Rev. 2003, 16, 1–17. [Google Scholar] [CrossRef]
- Petca, A.; Borislavschi, A.; Zvanca, M.E.; Petca, R.C.; Sandru, F.; Dumitrascu, M.C. Non-sexual HPV transmission and role of vaccination for a better future (Review). Exp. Ther. Med. 2020, 20, 186. [Google Scholar] [CrossRef]
- Manini, I.; Montomoli, E. Epidemiology and prevention of Human Papillomavirus. Ann. Ig. 2018, 30, 28–32. [Google Scholar]
- Sabeena, S.; Bhat, P.; Kamath, V.; Arunkumar, G. Possible non-sexual modes of transmission of human papilloma virus. J. Obstet. Gynaecol. Res. 2017, 43, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Louie, K.S.; de Sanjose, S.; Diaz, M.; Castellsagué, X.; Herrero, R.; Meijer, C.J.; Shah, K.; Franceschi, S.; Muñoz, N.; Bosch, F.X.; et al. Early age at first sexual intercourse and early pregnancy are risk factors for cervical cancer in developing countries. Br. J. Cancer 2009, 100, 1191–1197. [Google Scholar] [CrossRef]
- Liu, Z.C.; Liu, W.D.; Liu, Y.H.; Ye, X.H.; Chen, S.D. Multiple Sexual Partners as a Potential Independent Risk Factor for Cervical Cancer: A Meta-analysis of Epidemiological Studies. Asian Pac. J. Cancer Prev. 2015, 16, 3893–3900. [Google Scholar] [CrossRef] [PubMed]
- Chesson, H.W.; Dunne, E.F.; Hariri, S.; Markowitz, L.E. The Estimated Lifetime Probability of Acquiring Human Papillomavirus in the United States. Sex. Transm. Dis. 2014, 41, 660–664. [Google Scholar] [CrossRef]
- Dugué, P.A.; Rebolj, M.; Hallas, J.; Garred, P.; Lynge, E. Risk of cervical cancer in women with autoimmune diseases, in relation with their use of immunosuppressants and screening: Population-based cohort study. Int. J. Cancer 2015, 136, E711–E719. [Google Scholar] [CrossRef]
- Balasubramaniam, S.D.; Balakrishnan, V.; Oon, C.E.; Kaur, G. Key Molecular Events in Cervical Cancer Development. Medicina 2019, 55, 384. [Google Scholar] [CrossRef] [PubMed]
- Song, D.; Li, H.; Li, H.; Dai, J. Effect of human papillomavirus infection on the immune system and its role in the course of cervical cancer. Oncol. Lett. 2015, 10, 600–606. [Google Scholar] [CrossRef]
- Horvath, C.A.; Boulet, G.A.; Renoux, V.M.; Delvenne, P.O.; Bogers, J.P.J. Mechanisms of cell entry by human papillomaviruses: An overview. Virol. J. 2010, 7, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richards, R.M.; Lowy, D.R.; Schiller, J.T.; Day, P.M. Cleavage of the papillomavirus minor capsid protein, L2, at a furin consensus site is necessary for infection. Proc. Natl. Acad. Sci. USA 2006, 103, 1522–1527. [Google Scholar] [CrossRef] [PubMed]
- Crosbie, E.J.; Einstein, M.H.; Franceschi, S.; Kitchener, H.C. Human papillomavirus and cervical cancer. Lancet 2013, 382, 889–899. [Google Scholar] [CrossRef] [PubMed]
- Shimada, M.; Yamashita, A.; Saito, M.; Ichino, M.; Kinjo, T.; Mizuki, N.; Klinman, D.M.; Okuda, K. The human papillomavirus E6 protein targets apoptosis-inducing factor (AIF) for degradation. Sci. Rep. 2020, 10, 14195. [Google Scholar] [CrossRef]
- White, E.A.; Münger, K.; Howley, P.M. High-Risk Human Papillomavirus E7 Proteins Target PTPN14 for Degradation. mBio 2016, 7, e01530-16. [Google Scholar] [CrossRef]
- Venuti, A.; Paolini, F.; Nasir, L.; Corteggio, A.; Roperto, S.; Campo, M.S.; Borzacchiello, G. Papillomavirus E5: The smallest oncoprotein with many functions. Mol. Cancer 2011, 10, 140. [Google Scholar] [CrossRef]
- Graham, S.V. The human papillomavirus replication cycle, and its links to cancer progression: A comprehensive review. Clin. Sci. 2017, 131, 2201–2221. [Google Scholar] [CrossRef]
- Fay, N.; Panté, N. Nuclear entry of DNA viruses. Front. Microbiol. 2015, 6, 467. [Google Scholar] [CrossRef]
- Wang, J.W.; Roden, R.B.S. Virus-like particles for the prevention of human papillomavirus-associated malignancies. Expert. Rev. Vaccines 2013, 12, 129–141. [Google Scholar] [CrossRef]
- Kirnbauer, R.; Booy, F.; Cheng, N.; Lowy, D.R.; Schiller, J.T. Papillomavirus L1 major capsid protein self-assembles into virus-like particles that are highly immunogenic. Proc. Natl. Acad. Sci. USA 1992, 89, 12180–12184. [Google Scholar] [CrossRef] [PubMed]
- International Collaboration of Epidemiological Studies of Cervical Cancer; Appleby, P.; Beral, V.; Berrington de González, A.; Colin, D.; Franceschi, S.; Goodhill, A.; Green, J.; Peto, J.; Plummer, M.; et al. Carcinoma of the cervix and tobacco smoking: Collaborative reanalysis of individual data on 13,541 women with carcinoma of the cervix and 23,017 women without carcinoma of the cervix from 23 epidemiological studies. Int. J. Cancer 2006, 118, 1481–1495. [Google Scholar] [PubMed]
- Roura, E.; Castellsagué, X.; Pawlita, M.; Travier, N.; Waterboer, T.; Margall, N.; Bosch, F.X.; de Sanjosé, S.; Dillner, J.; Gram, I.T.; et al. Smoking as a major risk factor for cervical cancer and pre-cancer: Results from the EPIC cohort. Int. J. Cancer 2014, 135, 453–466. [Google Scholar] [CrossRef] [PubMed]
- Vaccarella, S.; Herrero, R.; Snijders, P.J.; Dai, M.; Thomas, J.O.; Hieu, N.T.; Ferreccio, C.; Matos, E.; Posso, H.; de Sanjosé, S.; et al. IARC HPV Prevalence Surveys (IHPS) Study Group. Smoking and human papillomavirus infection: Pooled analysis of the International Agency for Research on Cancer HPV Prevalence Surveys. Int. J. Epidemiol. 2008, 37, 536–546. [Google Scholar] [CrossRef]
- Xi, L.F.; Koutsky, L.A.; Castle, P.E.; Edelstein, Z.R.; Meyers, C.; Ho, J.; Schiffman, M. Relationship between cigarette smoking and human papillomavirus type 16 and 18 DNA load. Cancer. Epidemiol. Biomark. Prev. 2009, 18, 3490–3496. [Google Scholar] [CrossRef]
- Koshiol, J.; Schroeder, J.; Jamieson, D.J.; Marshall, S.W.; Duerr, A.; Heilig, C.M.; Shah, K.V.; Klein, R.S.; Cu-Uvin, S.; Schuman, P.; et al. Smoking and Time to Clearance of Human Papillomavirus Infection in HIV-Seropositive and HIV-Seronegative Women. Am. J. Epidemiol. 2006, 164, 176–183. [Google Scholar] [CrossRef]
- Alam, S.; Conway, M.J.; Chen, H.S.; Meyers, C. The Cigarette Smoke Carcinogen Benzo[a]pyrene Enhances Human Papillomavirus Synthesis. J. Virol. 2008, 82, 1053–1058. [Google Scholar] [CrossRef]
- Wei, L.; Griego, A.M.; Chu, M.; Ozbun, M.A. Tobacco exposure results in increased E6 and E7 oncogene expression, DNA damage and mutation rates in cells maintaining episomal human papillomavirus 16 genomes. Carcinogenesis 2014, 35, 2373–2381. [Google Scholar] [CrossRef]
- Alam, S.; Bowser, B.S.; Conway, M.J.; Israr, M.; Ryndock, E.J.; Xi, L.F.; Meyers, C. Downregulation of Cdc2/CDK1 kinase activity induces the synthesis of noninfectious human papillomavirus type 31b virions in organotypic tissues exposed to benzo[a]pyrene. J. Virol. 2010, 84, 4630–4645. [Google Scholar] [CrossRef]
- Combined Pill. Your Contraception Guide. nhs.uk. 2020. Available online: https://www.nhs.uk/conditions/contraception/combined-contraceptive-pill/ (accessed on 10 January 2023).
- National Institute for Health and Care Excellence. Contraception—Combined Hormonal Methods: Scenario: Combined Oral Contraceptive. 2022. Available online: https://cks.nice.org.uk/topics/contraception-combined-hormonal-methods/management/combined-oral-contraceptive/ (accessed on 20 December 2022).
- Asthana, S.; Busa, V.; Labani, S. Oral contraceptives use and risk of cervical cancer-A systematic review & meta-analysis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 247, 163–175. [Google Scholar]
- Peng, Y.; Wang, X.; Feng, H.; Yan, G. Is oral contraceptive use associated with an increased risk of cervical cancer? An evidence-based meta-analysis. J. Obstet. Gynaecol. Res. 2017, 43, 913–922. [Google Scholar] [CrossRef] [PubMed]
- Anastasiou, E.; McCarthy, K.J.; Gollub, E.L.; Ralph, L.; van de Wijgert, J.H.H.M.; Jones, H.E. The relationship between hormonal contraception and cervical dysplasia/cancer controlling for human papillomavirus infection: A systematic review. Contraception 2022, 107, 1–9. [Google Scholar] [CrossRef]
- International Collaboration of Epidemiological Studies of Cervical Cancer; Appleby, P.; Beral, V.; Berrington de González, A.; Colin, D.; Franceschi, S.; Goodhill, A.; Green, J.; Peto, J.; Plummer, M.; et al. Cervical cancer and hormonal contraceptives: Collaborative reanalysis of individual data for 16,573 women with cervical cancer and 35,509 women without cervical cancer from 24 epidemiological studies. Lancet 2007, 370, 1609–1621. [Google Scholar] [PubMed]
- Roura, E.; Travier, N.; Waterboer, T.; de Sanjosé, S.; Bosch, F.X.; Pawlita, M.; Pala, V.; Weiderpass, E.; Margall, N.; Dillner, J.; et al. The Influence of Hormonal Factors on the Risk of Developing Cervical Cancer and Pre-Cancer: Results from the EPIC Cohort. PLoS. ONE 2016, 11, e0147029. [Google Scholar]
- Ramachandran, B. Functional association of oestrogen receptors with HPV infection in cervical carcinogenesis. Endocr. Relat. Cancer 2017, 24, R99–R108. [Google Scholar] [CrossRef] [PubMed]
- Munk, A.C.; Gudlaugsson, E.; Ovestad, I.T.; Lovslett, K.; Fiane, B.; Hidle, B.v.; Kruse, A.J.; Skaland, I.; Janssen, E.A.; Baak, J.P. Interaction of epithelial biomarkers, local immune response and condom use in cervical intraepithelial neoplasia 2-3 regression. Gynecol. Oncol. 2012, 127, 489–494. [Google Scholar] [CrossRef] [PubMed]
- Hogewoning, C.J.; Bleeker, M.C.; van den Brule, A.J.; Voorhorst, F.J.; Snijders, P.J.; Berkhof, J.; Westenend, P.J.; Meijer, C.J. Condom use promotes regression of cervical intraepithelial neoplasia and clearance of human papillomavirus: A randomized clinical trial. Int. J. Cancer 2003, 107, 811–816. [Google Scholar] [CrossRef] [PubMed]
- Winer, R.L.; Hughes, J.P.; Feng, Q.; O’Reilly, S.; Kiviat, N.B.; Holmes, K.K.; Koutsky, L.A. Condom use and the risk of genital human papillomavirus infection in young women. N. Engl. J. Med. 2006, 354, 2645–2654. [Google Scholar] [CrossRef]
- Moreno, V.; Bosch, F.X.; Muñoz, N.; Meijer, C.J.; Shah, K.V.; Walboomers, J.M.; Herrero, R.; Franceschi, S.; International Agency for Research on Cancer. Multicentric Cervical Cancer Study Group. Effect of oral contraceptives on risk of cervical cancer in women with human papillomavirus infection: The IARC multicentric case-control study. Lancet 2002, 359, 1085–1092. [Google Scholar] [CrossRef]
- Grulich, A.E.; van Leeuwen, M.T.; Falster, M.O.; Vajdic, C.M. Incidence of cancers in people with HIV/AIDS compared with immunosuppressed transplant recipients: A meta-analysis. Lancet 2007, 370, 59–67. [Google Scholar] [CrossRef]
- Dugué, P.A.; Rebolj, M.; Garred, P.; Lynge, E. Immunosuppression and risk of cervical cancer. Expert. Rev. Anticancer. Ther. 2013, 13, 29–42. [Google Scholar] [CrossRef]
- Hinten, F.; Meeuwis, K.A.; van Rossum, M.M.; de Hullu, J.A. HPV-related (pre)malignancies of the female anogenital tract in renal transplant recipients. Crit. Rev. Oncol. Hematol. 2012, 84, 161–180. [Google Scholar] [CrossRef] [PubMed]
- Meeuwis, K.A.; van Rossum, M.M.; van de Kerkhof, P.C.; Hoitsma, A.J.; Massuger, L.F.; de Hullu, J.A. Skin cancer and (pre)malignancies of the female genital tract in renal transplant recipients. Transpl. Int. 2010, 23, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Klitzke, S.; Wender, I.O.; Salcedo, M.P.; Pessini, S.A. Cervical cancer screening abnormalities in immunosuppressed renal transplant women: Case-control study in Southern Brazil. Arch. Gynecol. Obstet. 2020, 302, 649–655. [Google Scholar] [CrossRef]
- Chen, M.; Cui, Q.; Chen, M.; Xia, M.; Liu, D.; Chen, P.; Wang, C.; He, M. Risk of human papillomavirus infection and cervical intraepithelial lesions in Chinese renal transplant recipients. Front. Oncol. 2022, 12, 905548. [Google Scholar] [CrossRef]
- Stelzle, D.; Tanaka, L.F.; Lee, K.K.; Ibrahim Khalil, A.; Baussano, I.; Shah, A.S.V.; McAllister, D.A.; Gottlieb, S.L.; Klug, S.J.; Winkler, A.S.; et al. Estimates of the global burden of cervical cancer associated with HIV. Lancet. Glob. Health 2021, 9, e161–e169. [Google Scholar] [CrossRef]
- Massad, L.S.; Seaberg, E.C.; Wright, R.L.; Darragh, T.; Lee, Y.C.; Colie, C.; Burk, R.; Strickler, H.D.; Watts, D.H. Squamous cervical lesions in women with human immunodeficiency virus: Long-term follow-up. Obstet. Gynecol. 2008, 111, 1388–1393. [Google Scholar] [CrossRef] [PubMed]
- Abraham, A.G.; D’Souza, G.; Jing, Y.; Gange, S.J.; Sterling, T.R.; Silverberg, M.J.; Saag, M.S.; Rourke, S.B.; Rachlis, A.; Napravnik, S.; et al. Invasive Cervical Cancer Risk Among HIV-Infected Women: A North American multicohort collaboration prospective study. J. Acquir. Immune. Defic. Syndr. 2013, 62, 405–413. [Google Scholar] [CrossRef]
- Cervical Screening: Scenario: Cervical Screening. National Institute for Health and Care Excellence. 2022. Available online: https://cks.nice.org.uk/topics/cervical-screening/management/cervical-screening/ (accessed on 23 December 2022).
- International Collaboration of Epidemiological Studies of Cervical Cancer. Cervical carcinoma and sexual behavior: Collaborative reanalysis of individual data on 15,461 women with cervical carcinoma and 29,164 women without cervical carcinoma from 21 epidemiological studies. Cancer. Epidemiol. Biomarkers. Prev. 2009, 18, 1060–1069. [Google Scholar] [CrossRef]
- Children and the Law. NSPCC Learning. 2022. Available online: https://learning.nspcc.org.uk/child-protection-system/children-the-law/ (accessed on 8 January 2023).
- Quabius, E.S.; Fazel, A.; Knieling, C.; Gebhardt, S.; Laudien, M.; Moore, C.; Kühnel, A.; Hoppe, F.; Mlynski, R.; Heinrichs, A.; et al. No association between HPV-status in tonsillar tissue and sexual behavior of the patients in a northern German population—Critical view of the link between HPV natural history and HPV-driven carcinogenesis. Papillomavirus. Res. 2020, 10, 100207. [Google Scholar] [CrossRef]
- HPV Vaccine Overview. nhs.uk. 2019. Available online: https://www.nhs.uk/conditions/vaccinations/hpv-human-papillomavirus-vaccine/ (accessed on 8 January 2023).
- Bogaards, J.A.; Wallinga, J.; Brakenhoff, R.H.; Meijer, C.J.; Berkhof, J. Direct benefit of vaccinating boys along with girls against oncogenic human papillomavirus: Bayesian evidence synthesis. BMJ 2015, 350, h2016. [Google Scholar] [CrossRef] [PubMed]
- HPV Vaccination Recommendations. Centers for Disease Control and Prevention. 2021. Available online: https://www.cdc.gov/vaccines/vpd/hpv/hcp/recommendations.html (accessed on 10 January 2023).
- HPV Vaccine to Change in September 2012. GOV.UK. 2011. Available online: https://www.gov.uk/government/news/hpv-vaccine-to-change-in-september-2012 (accessed on 10 January 2023).
- Information on HPV Vaccination. GOV.UK. 2022. Available online: https://www.gov.uk/government/publications/hpv-vaccine-vaccination-guide-leaflet/information-on-hpv-vaccination (accessed on 10 January 2023).
- Joura, E.A.; Giuliano, A.R.; Iversen, O.E.; Bouchard, C.; Mao, C.; Mehlsen, J.; Moreira, E.D., Jr.; Ngan, Y.; Petersen, L.K.; Lazcano-Ponce, E.; et al. A 9-valent HPV vaccine against infection and intraepithelial neoplasia in women. N. Engl. J. Med. 2015, 372, 711–723. [Google Scholar] [CrossRef] [PubMed]
- Joura, E.A.; Garland, S.M.; Paavonen, J.; Ferris, D.G.; Perez, G.; Ault, K.A.; Huh, W.K.; Sings, H.L.; James, M.K.; Haupt, R.M.; et al. Effect of the human papillomavirus (HPV) quadrivalent vaccine in a subgroup of women with cervical and vulvar disease: Retrospective pooled analysis of trial data. BMJ 2012, 344, e1401. [Google Scholar] [CrossRef]
- Human Papillomavirus (HPV): The Green Book, Chapter 18a. GOV.UK. 2022. Available online: https://www.gov.uk/government/publications/human-papillomavirus-hpv-the-green-book-chapter-18a (accessed on 10 January 2023).
- Shi, L.; Sings, H.L.; Bryan, J.T.; Wang, B.; Wang, Y.; Mach, H.; Kosinski, M.; Washabaugh, M.W.; Sitrin, R.; Barr, E. GARDASIL: Prophylactic human papillomavirus vaccine development--from bench top to bed-side. Clin. Pharmacol. Ther. 2007, 81, 259–264. [Google Scholar] [CrossRef]
- Artemchuk, H.; Eriksson, T.; Poljak, M.; Surcel, H.M.; Dillner, J.; Lehtinen, M.; Faust, H. Long-term Antibody Response to Human Papillomavirus Vaccines: Up to 12 Years of Follow-up in the Finnish Maternity Cohort. J. Infect. Dis. 2019, 219, 582–589. [Google Scholar] [CrossRef] [PubMed]
- Hoes, J.; Pasmans, H.; Schurink-van ’t Klooster, T.M.; van der Klis, F.R.M.; Donken, R.; Berkhof, J.; de Melker, H.E. Review of long-term immunogenicity following HPV vaccination: Gaps in current knowledge. Hum. Vaccin. Immunother. 2022, 18, 1908059. [Google Scholar] [CrossRef]
- Petry, K.U.; Bollaerts, K.; Bonanni, P.; Stanley, M.; Drury, R.; Joura, E.; Kjaer, S.K.; Meijer, C.J.L.M.; Riethmuller, D.; Soubeyrand, B.; et al. Estimation of the individual residual risk of cervical cancer after vaccination with the nonavalent HPV vaccine. Hum. Vaccin. Immunother. 2018, 14, 1800–1806. [Google Scholar] [CrossRef]
- Lei, J.; Ploner, A.; Elfström, K.M.; Wang, J.; Roth, A.; Fang, F.; Sundström, K.; Dillner, J.; Sparén, P. HPV Vaccination and the Risk of Invasive Cervical Cancer. N. Engl. J. Med. 2020, 383, 1340–1348. [Google Scholar] [CrossRef]
- Landy, R.; Pesola, F.; Castañón, A.; Sasieni, P. Impact of cervical screening on cervical cancer mortality: Estimation using stage-specific results from a nested case–control study. Br. J. Cancer 2016, 115, 1140–1146. [Google Scholar] [CrossRef]
- Austoker, J. Cancer prevention in primary care. Screening for cervical cancer. BMJ 1994, 309, 241–248. [Google Scholar] [CrossRef]
- Sasieni, P.; Cuzick, J.; Farmery, E. Accelerated decline in cervical cancer mortality in England and Wales. Lancet 1995, 346, 1566–1567. [Google Scholar] [CrossRef]
- Canfell, K.; Barnabas, R.; Patnick, J.; Beral, V. The predicted effect of changes in cervical screening practice in the UK: Results from a modelling study. Br. J. Cancer 2004, 91, 530–536. [Google Scholar] [CrossRef] [PubMed]
- What Is Cervical Screening? Public Health Wales. 2022. Available online: https://phw.nhs.wales/services-and-teams/cervical-screening-wales/what-is-cervical-screening/ (accessed on 8 January 2023).
- Cervical Screening (Smear Test). NHS Inform. 2022. Available online: https://www.nhsinform.scot/healthy-living/screening/cervical/cervical-screening-smear-test (accessed on 8 January 2023).
- Labeit, A.; Peinemann, F.; Kedir, A. Cervical Cancer Screening Service Utilisation in UK. Sci. Rep. 2013, 3, 2362. [Google Scholar] [CrossRef] [PubMed]
- Naucler, P.; Ryd, W.; Törnberg, S.; Strand, A.; Wadell, G.; Elfgren, K.; Rådberg, T.; Strander, B.; Johansson, B.; Forslund, O.; et al. Human papillomavirus and Papanicolaou tests to screen for cervical cancer. N. Engl. J. Med. 2007, 357, 1589–1597. [Google Scholar] [CrossRef] [PubMed]
- Rijkaart, D.C.; Berkhof, J.; Rozendaal, L.; van Kemenade, F.J.; Bulkmans, N.W.; Heideman, D.A.; Kenter, G.G.; Cuzick, J.; Snijders, P.J.; Meijer, C.J. Human papillomavirus testing for the detection of high-grade cervical intraepithelial neoplasia and cancer: Final results of the POBASCAM randomised controlled trial. Lancet. Oncol. 2012, 13, 78–88. [Google Scholar] [CrossRef] [PubMed]
- Ronco, G.; Dillner, J.; Elfström, K.M.; Tunesi, S.; Snijders, P.J.; Arbyn, M.; Kitchener, H.; Segnan, N.; Gilham, C.; Giorgi-Rossi, P.; et al. Efficacy of HPV-based screening for prevention of invasive cervical cancer: Follow-up of four European randomised controlled trials. Lancet 2014, 383, 524–532. [Google Scholar] [CrossRef]
- What Is Cervical Screening? nhs.uk. 2020. Available online: https://www.nhs.uk/conditions/cervical-screening/ (accessed on 9 January 2023).
- What Is A Colposcopy? nhs.uk. 2022. Available online: https://www.nhs.uk/conditions/colposcopy/ (accessed on 8 January 2023).
- Manley, K.; Wills, A.K.; Morris, G.N.; Hogg, J.L.; López Bernal, A.; Murdoch, J.B. The impact of HPV cervical screening on negative large loop excision of the transformation zone (LLETZ): A comparative cohort study. Gynecol. Oncol. 2016, 141, 485–491. [Google Scholar] [CrossRef]
- Cervical Screening Programme, England—2021–2022 [NS]. NHS 75 Digital. 2022. Available online: https://digital.nhs.uk/data-and-information/publications/statistical/cervical-screening-annual/england-2021-2022 (accessed on 10 January 2023).
- Prime Minister’s Statement on Coronavirus (COVID-19): 16 March 2020. GOV.UK. 2020. Available online: https://www.gov.uk/government/speeches/pm-statement-on-coronavirus-16-march-2020 (accessed on 13 January 2023).
- Murphy, M.; Scott, L.J.; Salisbury, C.; Turner, A.; Scott, A.; Denholm, R.; Lewis, R.; Iyer, G.; Macleod, J.; Horwood, J. Implementation of remote consulting in UK primary care following the COVID-19 pandemic: A mixed-methods longitudinal study. Br. J. Gen. Pract. 2021, 71, e166–e177. [Google Scholar] [CrossRef]
- Knights, F.A.E.; Carter, J.; Deal, A.; Hargreaves, S. Face-to-face GP consultations: Avoiding digital exclusion of marginalised groups. BMJ 2021, 373, n1542. [Google Scholar] [CrossRef] [PubMed]
- Exploring the UK’s Digital Divide. Office for National Statistics. 2019. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/householdcharacteristics/homeinternetandsocialmediausage/articles/exploringtheuksdigitaldivide/2019-03-04 (accessed on 13 January 2023).
- Vose, J.M. Delay in Cancer Screening and Diagnosis During the COVID-19 Pandemic: What Is the Cost? Oncology 2020, 34, 343. [Google Scholar] [CrossRef]
- Revythis, A.; Shah, S.; Enyioma, S.; Ghose, A.; Patel, M.; Karathanasi, A.; Sanchez, E.; Boussios, S. The Experience of a Single NHS England Trust on the Impact of the COVID-19 Pandemic on Junior and Middle-Grade Doctors: What Is Next? Int. J. Environ. Res. Public Health 2021, 18, 10413. [Google Scholar] [CrossRef]
- Sud, A.; Torr, B.; Jones, M.E.; Broggio, J.; Scott, S.; Loveday, C.; Garrett, A.; Gronthoud, F.; Nicol, D.L.; Jhanji, S.; et al. Effect of delays in the 2-week-wait cancer referral pathway during the COVID-19 pandemic on cancer survival in the UK: A modelling study. Lancet. Oncol. 2020, 21, 1035–1044. [Google Scholar] [CrossRef]
- Douglas, E.; Waller, J.; Duffy, S.W.; Wardle, J. Socioeconomic inequalities in breast and cervical screening coverage in England: Are we closing the gap? J. Med. Screen. 2016, 23, 98–103. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, M.; O’Leary, E.; Waller, J.; Gallagher, P.; Martin, C.M.; O’Leary, J.J.; Sharp, L.; Irish Cervical Screening Research Consortium (CERVIVA). Socio-economic variations in anticipated adverse reactions to testing HPV positive: Implications for the introduction of primary HPV-based cervical screening. Prev. Med. 2018, 115, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Moser, K.; Patnick, J.; Beral, V. Inequalities in reported use of breast and cervical screening in Great Britain: Analysis of cross sectional survey data. BMJ 2009, 338, b2025. [Google Scholar] [CrossRef] [PubMed]
- Sabates, R.; Feinstein, L. The role of education in the uptake of preventative health care: The case of cervical screening in Britain. Soc. Sci. Med. 2006, 62, 2998–3010. [Google Scholar] [CrossRef]
- Sutton, S.; Rutherford, C. Sociodemographic and attitudinal correlates of cervical screening uptake in a national sample of women in Britain. Soc. Sci. Med. 2005, 61, 2460–2465. [Google Scholar] [CrossRef]
- Fonseca-Moutinho, J.A. Smoking and Cervical Cancer. ISRN. Obstet. Gynecol. 2011, 2011, 847684. [Google Scholar] [CrossRef]
- Hiscock, R.; Bauld, L.; Amos, A.; Fidler, J.A.; Munafò, M. Socioeconomic status and smoking: A review. Ann. N. Y. Acad. Sci. 2012, 1248, 107–123. [Google Scholar] [CrossRef] [PubMed]
- Vukovic, D.; Bjegović-Mikanović, V. Association between socio-economic status and sexual behavior of adolescents. Srp. Arh. Celok. Lek. 2007, 135, 321–325. [Google Scholar] [CrossRef]
- HPV Vaccination. Superdrug Health Clinic. 2023. Available online: https://healthclinics.superdrug.com/services/hpv-vaccination/ (accessed on 13 January 2023).
- Gardasil 9 (HPV Vaccine). LloydsPharmacy Online Doctor UK. 2023. Available online: https://onlinedoctor.lloydspharmacy.com/uk/hpv-vaccine/gardasil-9-vaccine (accessed on 13 January 2023).
- Falcaro, M.; Castañon, A.; Ndlela, B.; Checchi, M.; Soldan, K.; Lopez-Bernal, J.; Elliss-Brookes, L.; Sasieni, P. The effects of the national HPV vaccination programme in England, UK, on cervical cancer and grade 3 cervical intraepithelial neoplasia incidence: A register-based observational study. Lancet 2021, 398, 208–2092. [Google Scholar] [CrossRef] [PubMed]
- Delamothe, T. A centrally funded health service, free at the point of delivery. BMJ 2008, 336, 1410–1412. [Google Scholar] [CrossRef] [PubMed]
- Tranberg, M.; Bech, B.H.; Blaakær, J.; Jensen, J.S.; Svanholm, H.; Andersen, B. HPV self-sampling in cervical cancer screening: The effect of different invitation strategies in various socioeconomic groups—A randomized controlled trial. Clin. Epidemiol. 2018, 10, 1027–1036. [Google Scholar] [CrossRef]
- Sewali, B.; Okuyemi, K.S.; Askhir, A.; Belinson, J.; Vogel, R.I.; Joseph, A.; Ghebre, R.G. Cervical cancer screening with clinic-based Pap test versus home HPV test among Somali immigrant women in Minnesota: A pilot randomized controlled trial. Cancer Med. 2015, 4, 620–631. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, E.M.; Lothamer, H.; Garcia, C.; Marais, A.D.; Camacho, F.; Poulter, M.; Bullock, L.; Smith, J.S. Acceptability and Feasibility of Community-Based, Lay Navigator-Facilitated At-Home Self-Collection for Human Papillomavirus Testing in Underscreened Women. J. Womens Health 2020, 29, 596–602. [Google Scholar] [CrossRef]
- Giorgi Rossi, P.; Marsili, L.M.; Camilloni, L.; Iossa, A.; Lattanzi, A.; Sani, C.; Di Pierro, C.; Grazzini, G.; Angeloni, C.; Capparucci, P.; et al. The effect of self-sampled HPV testing on participation to cervical cancer screening in Italy: A randomised controlled trial (ISRCTN96071600). Br. J. Cancer 2011, 104, 248–254. [Google Scholar] [CrossRef]
- Wikström, I.; Lindell, M.; Sanner, K.; Wilander, E. Self-sampling and HPV testing or ordinary Pap-smear in women not regularly attending screening: A randomised study. Br. J. Cancer 2011, 105, 337–339. [Google Scholar] [CrossRef]
- World Health Organization. Human Papillomavirus (HPV) Self-Sampling as Part of Cervical Cancer Screening. 2022. Available online: https://www.who.int/publications-detail-redirect/WHO-SRH-2012 (accessed on 2 January 2023).
- Verdoodt, F.; Jentschke, M.; Hillemanns, P.; Racey, C.S.; Snijders, P.J.; Arbyn, M. Reaching women who do not participate in the regular cervical cancer screening programme by offering self-sampling kits: A systematic review and meta-analysis of randomised trials. Eur. J. Cancer 2015, 51, 2375–2385. [Google Scholar] [CrossRef]
- NHS Gives Women Human Papillomavirus Virus (HPV) Home Testing Kits to Cut Cancer Deaths. NHS 75 England. 2021. Available online: https://www.england.nhs.uk/2021/02/nhs-gives-women-hpv-home-testing-kits-to-cut-cancer-deaths/ (accessed on 13 January 2023).
- Sacks, R.J.; Copas, A.J.; Wilkinson, D.M.; Robinson, A.J. Uptake of the HPV vaccination programme in England: A cross-sectional survey of young women attending sexual health services. Sex. Transm. Infect. 2014, 90, 315–321. [Google Scholar] [CrossRef]
- Lee Mortensen, G.; Adam, M.; Idtaleb, L. Parental attitudes towards male human papillomavirus vaccination: A pan-European cross-sectional survey. BMC Public Health 2015, 15, 624. [Google Scholar] [CrossRef] [PubMed]
- Gottvall, M.; Stenhammar, C.; Grandahl, M. Parents’ views of including young boys in the Swedish national school-based HPV vaccination programme: A qualitative study. BMJ Open. 2017, 7, e014255. [Google Scholar] [CrossRef] [PubMed]
- Castanon, A.; Rebolj, M.; Pesola, F.; Pearmain, P.; Stubbs, R. COVID-19 disruption to cervical cancer screening in England. J. Med. Screen. 2022, 29, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Davies, J.M.; Spencer, A.; Macdonald, S.; Dobson, L.; Haydock, E.; Burton, H.; Angelopoulos, G.; Martin-Hirsch, P.; Wood, N.J.; Thangavelu, A.; et al. Cervical cancer and COVID-an assessment of the initial effect of the pandemic and subsequent projection of impact for women in England: A cohort study. BJOG 2022, 129, 1133–1139. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, S.; Ismail, A.; Pappas-Gogos, G.; Boussios, S. HPV and Cervical Cancer: A Review of Epidemiology and Screening Uptake in the UK. Pathogens 2023, 12, 298. https://doi.org/10.3390/pathogens12020298
Choi S, Ismail A, Pappas-Gogos G, Boussios S. HPV and Cervical Cancer: A Review of Epidemiology and Screening Uptake in the UK. Pathogens. 2023; 12(2):298. https://doi.org/10.3390/pathogens12020298
Chicago/Turabian StyleChoi, Sunyoung, Ayden Ismail, George Pappas-Gogos, and Stergios Boussios. 2023. "HPV and Cervical Cancer: A Review of Epidemiology and Screening Uptake in the UK" Pathogens 12, no. 2: 298. https://doi.org/10.3390/pathogens12020298