
Maternal–Fetal Infections (Cytomegalovirus, Toxoplasma, Syphilis): Short-Term and Long-Term Neurodevelopmental Outcomes in Children Infected and Uninfected at Birth

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Definitions
2.2. Statistical Analysis
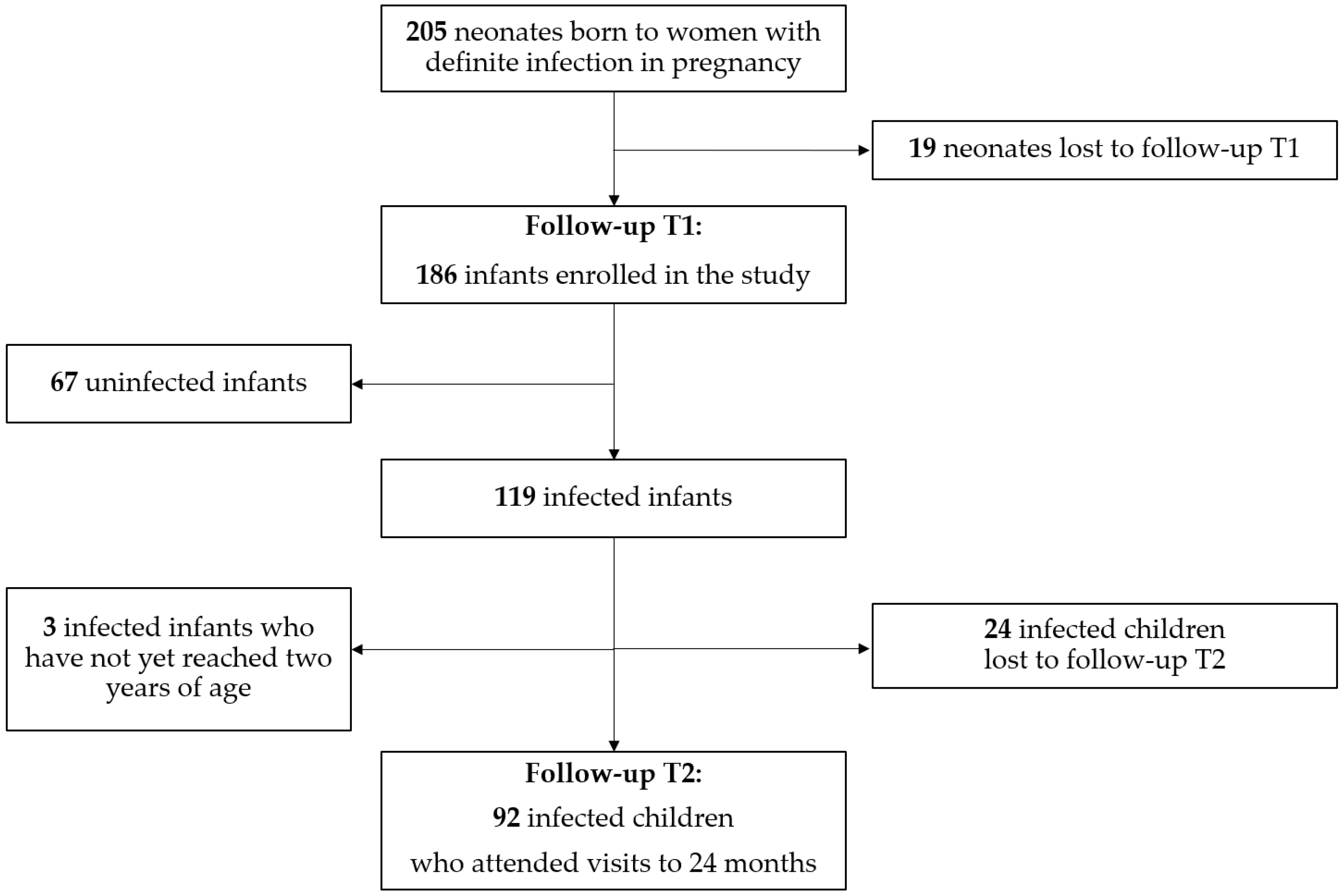
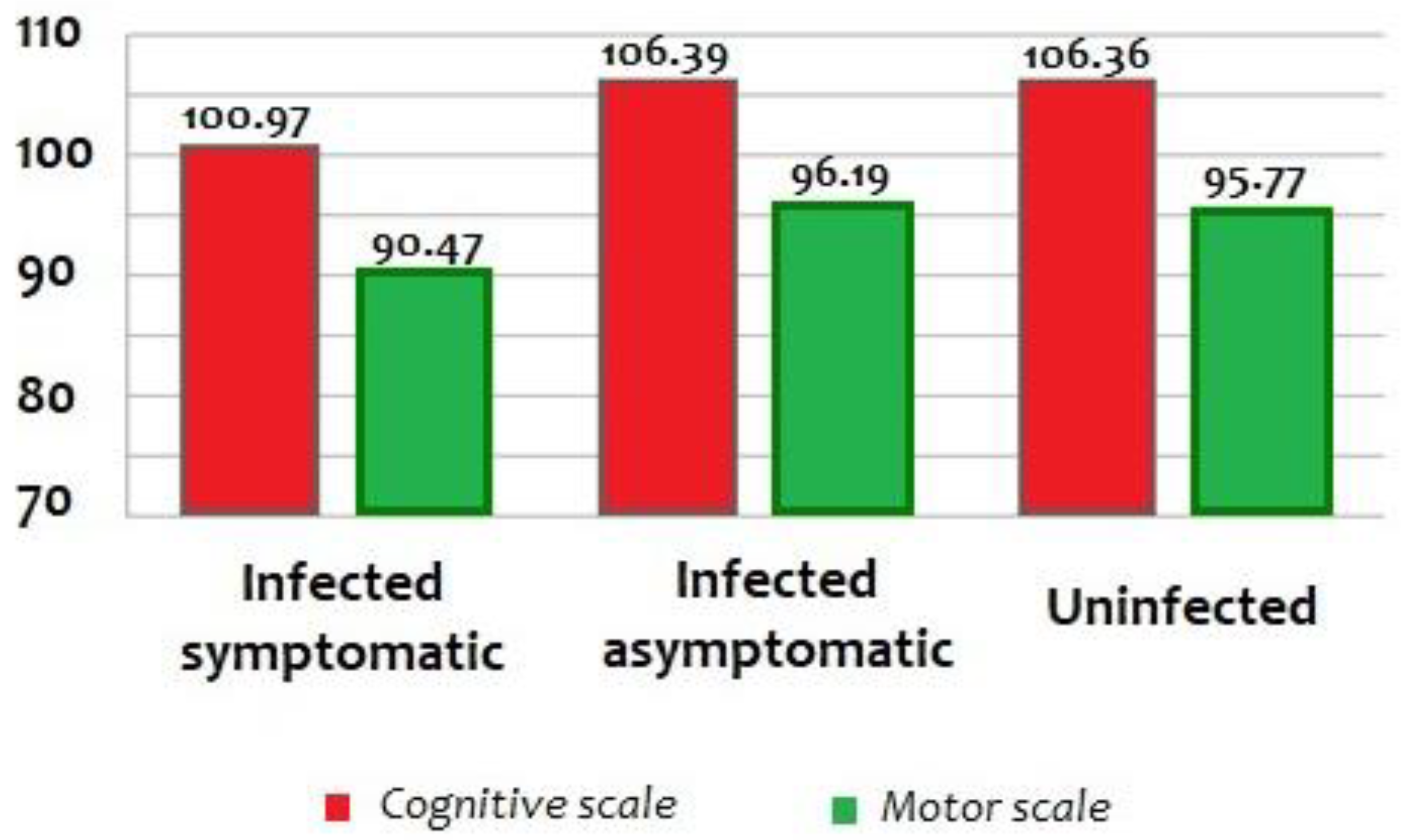
3. Results
Outcomes in Children with Congenital Infection
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ostrander, B.; Bale, J.F. Congenital and Perinatal Infections, 1st ed.; Elsevier B.V.: Amsterdam, The Netherlands, 2019; Volume 162. [Google Scholar]
- Auriti, C.; De Rose, D.U.; Santisi, A.; Martini, L.; Piersigilli, F.; Bersani, I.; Ronchetti, M.P.; Caforio, L. Pregnancy and viral infections: Mechanisms of fetal damage, diagnosis and prevention of neonatal adverse outcomes from cytomegalovirus to SARS-CoV-2 and Zika virus. Biochim. Biophys. Acta Mol. Basis Dis. 2021, 1867, 166198. [Google Scholar] [CrossRef] [PubMed]
- Buca, D.; Di Mascio, D.; Rizzo, G.; Giancotti, A.; D’Amico, A.; Leombroni, M.; Makatsarya, A.; Familiari, A.; Liberati, M.; Nappi, L.; et al. Outcome of fetuses with congenital cytomegalovirus infection and normal ultrasound at diagnosis: Systematic review and meta-analysis. Ultrasound Obstet. Gynecol. 2021, 57, 551–559. [Google Scholar] [CrossRef] [PubMed]
- Elkan Miller, T.; Weisz, B.; Yinon, Y.; Weissbach, T.; De Castro, H.; Avnet, H.; Hoffman, C.; Katorza, E.; Lipitz, S. Congenital cytomegalovirus infection following second and third trimester maternal infection is associated with mild childhood adverse outcome not predicted by prenatal imaging. J. Pediatric Infect. Dis. Soc. 2021, 10, 562–568. [Google Scholar] [CrossRef] [PubMed]
- Hijikata, M.; Okahashi, A.; Nagano, N.; Morioka, I. Clinical characteristics of congenital toxoplasmosis with poor outcome in Japan: A nationwide survey and literature review. Congenit. Anom. 2020, 60, 194–198. [Google Scholar] [CrossRef]
- Lim, J.; Yoon, S.J.; Shin, J.E.; Han, J.H.; Lee, S.M.; Eun, H.S.; Park, M.S.; Park, K.I. Outcomes of infants born to pregnant women with syphilis: A nationwide study in Korea. BMC Pediatrics 2021, 21, 47. [Google Scholar] [CrossRef] [PubMed]
- Verghese, V.P.; Hendson, L.; Singh, A.; Guenette, T.; Gratrix, J.; Robinson, J.L. Early Childhood Neurodevelopmental Outcomes in Infants Exposed to Infectious Syphilis in Utero. Pediatrics Infect. Dis. J. 2018, 37, 576–579. [Google Scholar] [CrossRef]
- Maltezou, P.G.; Kourlaba, G.; Kourkouni, Ε.; Luck, S.; Blázquez-Gamero, D.; Ville, Y.; Lilleri, D.; Dimopoulou, D.; Karalexi, M.; Papaevangelou, V. Maternal type of CMV infection and sequelae in infants with congenital CMV: Systematic review and meta-analysis. J. Clin. Virol. 2020, 129, 104518. [Google Scholar] [CrossRef]
- Uku, A.; Albujasim, Z.; Dwivedi, T.; Ladipo, Z.; Konje, J.C. Syphilis in pregnancy: The impact of “the Great Imitator”. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 259, 207–210. [Google Scholar] [CrossRef]
- Borges, M.; Magalhães Silva, T.; Brito, C.; Teixeira, N.; Roberts, C.W. How does toxoplasmosis affect the maternal-foetal immune interface and pregnancy? Parasite Immunol. 2019, 41, e12606. [Google Scholar] [CrossRef] [Green Version]
- Zammarchi, L.; Lazzarotto, T.; Andreoni, M.; Campolmi, I.; Pasquini, L.; Di Tommaso, M.; Simonazzi, G.; Tomasoni, L.R.; Castelli, F.; Galli, L.; et al. Management of cytomegalovirus infection in pregnancy: Is it time for valacyclovir? Clin. Microbiol. Infect. 2020, 26, 1151–1154. [Google Scholar] [CrossRef]
- Marsico, C.; Kimberlin, D.W. Congenital Cytomegalovirus infection: Advances and challenges in diagnosis, prevention and treatment. Ital. J. Pediatrics 2017, 43, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicloux, M.; Peterman, L.; Parodi, M.; Magny, J.F. Outcome and management of newborns with congenital cytomegalovirus infection. Arch. Ped. 2020, 27, 160–165. [Google Scholar] [CrossRef]
- Rawlinson, W.D.; Boppana, S.B.; Fowler, K.B.; Kimberlin, D.W.; Lazzarotto, T.; Alain, S.; Daly, K.; Doutré, S.; Gibson, L.; Giles, M.L.; et al. Congenital cytomegalovirus infection in pregnancy and the neonate: Consensus recommendations for prevention, diagnosis, and therapy. Lancet Infect. Dis. 2017, 17, e177–e188. [Google Scholar] [CrossRef]
- Bax, M.; Goldstein, M.; Rosenbaum, P.; Leviton, A.; Paneth, N.; Dan, B.; Jacobsson, B.; Damiano, D.; Executive Committee for the Definition of Cerebral Palsy. Proposed definition and classification of cerebral palsy, April 2005. Dev. Med. Child Neurol. 2005, 47, 571–576. [Google Scholar] [CrossRef] [PubMed]
- Bayley, N. The Bayley Scales of Infants and Toddler Development (BSID-III); Harcourt Assessment: San Antonio, TX, USA, 2006. [Google Scholar]
- Johnson, S.; Moore, T.; Marlow, N. Using the Bayley-III to assess neurodevelopmental delay: Which cut-off should be used? Pediatrics Res. 2014, 75, 670–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robson, A.G.; Nilsson, J.; Li, S.; Jalali, S.; Fulton, A.B.; Tormene, A.P.; Holder, G.E.; Brodie, S.E. ISCEV guide to visual electrodiagnostic procedures. Doc. Ophthalmol. 2018, 136, 1–26. [Google Scholar] [CrossRef] [Green Version]
- Scaioli, V.; Brinciotti, M.; Di Capua, M.; Lori, S.; Janes, A.; Pastorino, G.; Peruzzi, C.; Sergi, P.; Suppiej, A. A Multicentre Database for Normative Brainstem Auditory Evoked Potentials (BAEPs) in Children: Methodology for Data Collection and Evaluation. Open Neurol. J. 2009, 3, 72–84. [Google Scholar] [CrossRef] [Green Version]
- Boppana, S.B.; Fowler, K.B.; Pass, R.F.; Rivera, L.B.; Bradford, R.D.; Lakeman, F.D.; Britt, W.J. Congenital cytomegalovirus infection: Association between virus burden in infancy and hearing loss. J. Pediatrics 2005, 146, 817–823. [Google Scholar] [CrossRef]
- Korndewal, M.J.; Oudesluys-Murphy, A.M.; Kroes, A.; van der Sande, M.; de Melker, H.E.; Vossen, A. Long-term impairment attributable to congenital cytomegalovirus infection: A retrospective cohort study. Dev. Med. Child Neurol. 2017, 59, 1261–1268. [Google Scholar] [CrossRef]
- Chiopris, G.; Veronese, P.; Cusenza, F.; Procaccianti, M.; Perrone, S.; Daccò, V.; Colombo, C.; Esposito, S. Congenital cytomegalovirus infection: Update on diagnosis and treatment. Microorganisms 2020, 8, 1516. [Google Scholar] [CrossRef]
- Ronchi, A.; Zeray, F.; Lee, L.E.; Owen, K.E.; Shoup, A.G.; Garcia, F.; Vazquez, L.N.; Cantey, J.B.; Varghese, S.; Pugni, L.; et al. Evaluation of clinically asymptomatic high risk infants with congenital cytomegalovirus infection. J. Perinatol. 2020, 40, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Peyron, F.; L’ollivier, C.; Mandelbrot, L.; Wallon, M.; Piarroux, R.; Kieffer, F.; Hadjadj, E.; Paris, L.; Garcia-Meric, P. Maternal and congenital toxoplasmosis: Diagnosis and treatment recommendations of a French multidisciplinary working group. Pathogens 2019, 8, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adhikari, E.H. Syphilis in Pregnancy. Obstet Gynecol. 2020, 135, 1121–1135. [Google Scholar] [CrossRef] [PubMed]
- Medoro, A.K.; Sánchez, P.J. Syphilis in Neonates and Infants. Clin. Perinatol. 2021, 48, 293–309. [Google Scholar] [CrossRef] [PubMed]
- Al Malki, J.S.; Hussien, N.A.; Al Malki, F. Maternal toxoplasmosis and the risk of childhood autism: Serological and molecular small-scale studies. BMC Pediatrics 2021, 21, 133. [Google Scholar] [CrossRef]
- Peyron, F.; Garweg, J.G.; Wallon, M.; Descloux, E.; Rolland, M.; Barth, J. Long-term impact of treated congenital toxoplasmosis on quality of life and visual performance. Pediatrics Infect. Dis. J. 2011, 30, 597–600. [Google Scholar] [CrossRef]
- Xia, W.; Yan, H.; Zhang, Y.; Wang, C.; Gao, W.; Lv, C.; Wang, W.; Liu, Z. Congenital Human Cytomegalovirus Infection Inducing Sensorineural Hearing Loss. Front. Microbiol. 2021, 12, 649690. [Google Scholar] [CrossRef]
- Macedo de Resende, L.; Manzan Queiroz de Andrade, G.; Frasson de Azevedo, M.; Perissinoto, J.; Cheloni Vieira, A.B.; Congenital Toxoplasmosis Brazilian Group of the Universidade Federal de Minas Gerais. Congenital toxoplasmosis: Auditory and language outcomes in early diagnosed and treated children. Sci. Med. 2010, 20, 13–19. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Definitions | |
|---|---|
| Cytomegalovirus | Symptomatic infection Presence of one or more of these symptoms: thrombocytopenia, petechiae, hepatomegaly, splenomegaly, intrauterine growth restriction, hepatitis (raised transaminases or bilirubin), central nervous system involvement such as microcephaly, radiographic abnormalities consistent with cytomegalovirus central nervous system disease (ventriculomegaly, intracerebral calcifications, cortical or cerebellar malformations), abnormal cerebrospinal fluid indices for age, chorioretinitis, sensorineural hearing loss, the detection of cytomegalovirus DNA in cerebrospinal fluid isolated sensorineural hearing loss (≥21 decibels), and isolation of CMV or identification of viral DNA in urine or saliva or blood. Asymptomatic infection No apparent abnormalities to suggest congenital cytomegalovirus disease, normal hearing, and isolation of CMV or identification of viral DNA in urine or saliva or blood, and detection of specific CMV IgM in blood during the first 3 weeks of postnatal life, without overt clinical symptoms of the infection. |
| Toxoplasmosis | Symptomatic infection Presence of the classic triad of clinical signs: chorioretinitis, intracranial calcifications, and hydrocephalus and or microcephaly, intracranial calcifications, chorioretinitis, cataracts, convulsions, nystagmus, jaundice, petechiae, anemia, prematurity and severe intrauterine growth restriction, and the presence of positive specific IgG and/or IgM antibodies against Toxoplasma gondii. Asymptomatic infection Intrauterine infection without obvious signs of toxoplasmosis at birth on routine examination, with positive specific IgG and IgM antibodies against Toxoplasma gondii, or with an increasing specific IgG serum level. |
| Syphilis | Confirmed Proven or Highly Probable Congenital Syphilis Any neonate with • an abnormal physical examination that is consistent with congenital syphilis; • a serum quantitative nontreponemal serologic titer that is fourfold (or greater) higher than the mother’s titer at delivery (e.g., maternal titer = 1:2, neonatal titer ≥ 1:8 or maternal titer = 1:8, neonatal titer ≥ 1:32); • or a positive darkfield test or PCR of placenta, cord, lesions, or body fluids or a positive silver stain of the placenta or cord. Possible Congenital Syphilis Any neonate who has a normal physical examination and a serum quantitative nontreponemal serologic titer equal to or less than fourfold of the maternal titer at delivery (e.g., maternal titer = 1:8, neonatal titer ≤ 1:16) and one of the following: • The mother was not treated, was inadequately treated, or has no documentation of having received treatment. • The mother was treated with erythromycin or a regimen other than those recommended in these guidelines (i.e., a nonpenicillin G regimen). • The mother received the recommended regimen but treatment was initiated Congenital Syphilis Less Likely Any neonate who has a normal physical examination and a serum quantitative nontreponemal serologic titer equal or less than fourfold of the maternal titer at delivery (e.g., maternal titer = 1:8, neonatal titer ≤ 1:16) and both of the following are true: • The mother was treated during pregnancy, treatment was appropriate for the infection stage, and the treatment regimen was initiated ≥30 days before delivery. • The mother has no evidence of reinfection or relapse. Congenital Syphilis Unlikely Any neonate who has a normal physical examination and a serum quantitative nontreponemal serologic titer equal to or less than fourfold of the maternal titer at delivery and both of the following are true: • The mother’s treatment was adequate before pregnancy. • The mother’s nontreponemal serologic titer remained low and stable (i.e., serofast) before and during pregnancy and at delivery (e.g., VDRL ≤ 1:2 or RPR ≤ 1:4). |
| Clinical Characteristics at Birth | Symptomatic Infected Infants (n = 37) | Asymptomatic Infected Infants (n = 82) | Uninfected Infants (n = 67) | p-Value |
|---|---|---|---|---|
| Gender (males), n (%) | 23 (62.2%) | 46 (56.1%) | 30 (44.8%) | NS |
| Gestational age (week), mean ± SD | 37.39 ± 3.18 | 38.92 ± 2.04 | 38.86 ± 1.50 | 0.001 |
| Birth weight (g), mean ± SD | 2684.51 ± 769.91 | 3149.04 ± 570.81 | 3146.95 ± 488.56 | 0.000 |
| Birth weight small for gestational age, n (%) | 8 (21.6%) | 12 (14.6%) | 8 (11.9%) | 0.022 |
| Head circumference (cm), mean ± SD | 32.45 ± 3.02 | 34.37 ± 1.32 | 34.07 ± 1.40 | 0.000 |
| Head circumference small for gestational age, n (%) | 7 (18.9%) | 6 (7.3%) | 6 (9.0%) | 0.028 |
| Microcephaly, n (%) | 5 (13.5%) | 3 (3.7%) | 3 (4.5%) | 0.004 |
| Cesarean section, n (%) | 13 (35.1%) | 20 (24.4%) | 14 (20.9%) | NS |
| Apgar 5′, median (IQR) | 9 (9–10) | 9 (9–10) | 9 (9–10) | 0.019 |
| Normal Development in 119 Infected Patients | Abnormal Development in 119 Infected Patients | ||
|---|---|---|---|
| One Sequela | Sequelae > 2 | ||
| T1 No. (%) | T1 No. (%) | T1 No. (%) | |
| CMV (n = 84) | |||
| Asymptomatic at birth (n = 55) | 49/55 (89.1) | 6/55 (10.9) | 0/55 (0) |
| Symptomatic at birth (n = 29) | 13/29 (44.8) | 12/29 (41.4) | 4/29 (13.8) |
| TOXOPLASMA (n = 18) | |||
| Asymptomatic at birth (n = 12) | 11/12 (91.7) | 1/12 (8.3) | 0/12 (0.0) |
| Symptomatic at birth (n = 6) | 3/6 (50.0) | 2/6 (33.3) | 1/6 (16.7) |
| SYPHILIS (n = 17) | |||
| Asymptomatic at birth (n = 15) | 14/15 (93.3) | 1/15 (6.7) | 0/15 (0.0) |
| Symptomatic at birth (n = 2) | 0/2 (0.0) | 0/2 (0.0) | 2/2 (100.0) |
| TOTAL (n = 119) | |||
| Asymptomatic at birth (n = 82) | 74/82 (90.2) | 8/82 (9.8) | 0/82 (0.0) |
| Symptomatic at birth (n = 37) | 16/37 (43.2) | 14/37 (37.8) | 7/37 (18.9) |
| Type of Infection | Cognitive Delay (Score < 85) | Motor Impairment (Score < 85) | Mild SNHL | Severe SNHL | Mild Abnormal Vision | Severe Visual Impairment |
|---|---|---|---|---|---|---|
| CMV (n= 84) | 3 (3.6%) | 11 (13.1%) | 11 (13.1%) | 1 (1.2%) | 2 (2.4%) | 0 (0.0%) |
| Toxoplasma (n = 18) | 1 (5.6%) | 3 (16.6%) | 1 (5.6%) | 0 (0.0%) | 1 (5.6%) | 1 (5.6%) |
| Syphilis (n= 17) | 0 (0%) | 3 (17.6%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| Total (n= 119) | 4 (3.4%) | 17 (14.3%) | 12 (10.1%) | 1 (0.8%) | 3 (2.5%) | 1 (0.8%) |
| Normal Development in 92 Infected Patients | Abnormal Development in 92 Infected Patients | ||
|---|---|---|---|
| One Sequela | Sequelae > 2 | ||
| T2 No. (%) | T2 No. (%) | T2 No. (%) | |
| CMV (n = 69) | |||
| Asymptomatic at birth (n = 42) | 34/42 (81.0) | 8/42 (19.0) | 0/42 (0.0) |
| Symptomatic at birth (n = 27) | 8/27 (29.6) | 14/27 (51.9) | 5/27 (18.5) |
| TOXOPLASMA (n = 14) | |||
| Asymptomatic at birth (n = 8) | 4/8 (50.0) | 4/8 (50.0) | 0/8 (0.0) |
| Symptomatic at birth (n = 6) | 3/6 (50.0) | 1/6 (16.7) | 2/6 (33.3) |
| SYPHILIS (n = 9) | |||
| Asymptomatic at birth (n = 7) | 5/7 (71.4) | 2/7 (28.6) | 0/7 (0.0) |
| Symptomatic at birth (n = 2) | 0/2 (0.0) | 0/2 (0.0) | 2/2 (100.0) |
| TOTAL (n = 92) | |||
| Asymptomatic at birth (n = 57) | 43/57 (75.4) | 14/57 (24.6) | 0/57 (0.0) |
| Symptomatic at birth (N = 35) | 11/35 (31.4) | 15/35 (42.9) | 9/35 (25.7) |
| Type of Infection | Cognitive Delay (Score < 85) | Motor Impairment (Score < 85) | Mild SNHL | Severe SNHL | Mild Abnormal Vision | Severe Visual Impairment | Language Delay |
|---|---|---|---|---|---|---|---|
| CMV (n = 69) | 4 (5.8%) | 4 (5.8%) | 9 (13.0%) | 1 (1.4%) | 2 (2.%) | 0 (0.0%) | 18 (26.1%) |
| Toxoplasma (n = 14) | 2 (14.3%) | 2 (14.3%) | 0 (0.0%) | 0 (0.0%) | 1 (7.1%) | 1 (7.1%) | 5 (35.7%) |
| Syphilis (n = 9) | 1 (11.1%) | 1 (11.1%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 3 (33.3%) |
| Total (n = 92) | 7 (7.6%) | 7 (7.6%) | 9 (9.8%) | 1 (1.1%) | 3 (2.3%) | 1 (1.1%) | 26 (28.3%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Auriti, C.; Bucci, S.; De Rose, D.U.; Coltella, L.; Santisi, A.; Martini, L.; Maddaloni, C.; Bersani, I.; Lozzi, S.; Campi, F.; et al. Maternal–Fetal Infections (Cytomegalovirus, Toxoplasma, Syphilis): Short-Term and Long-Term Neurodevelopmental Outcomes in Children Infected and Uninfected at Birth. Pathogens 2022, 11, 1278. https://doi.org/10.3390/pathogens11111278
Auriti C, Bucci S, De Rose DU, Coltella L, Santisi A, Martini L, Maddaloni C, Bersani I, Lozzi S, Campi F, et al. Maternal–Fetal Infections (Cytomegalovirus, Toxoplasma, Syphilis): Short-Term and Long-Term Neurodevelopmental Outcomes in Children Infected and Uninfected at Birth. Pathogens. 2022; 11(11):1278. https://doi.org/10.3390/pathogens11111278
Chicago/Turabian StyleAuriti, Cinzia, Silvia Bucci, Domenico Umberto De Rose, Luana Coltella, Alessandra Santisi, Ludovica Martini, Chiara Maddaloni, Iliana Bersani, Simona Lozzi, Francesca Campi, and et al. 2022. "Maternal–Fetal Infections (Cytomegalovirus, Toxoplasma, Syphilis): Short-Term and Long-Term Neurodevelopmental Outcomes in Children Infected and Uninfected at Birth" Pathogens 11, no. 11: 1278. https://doi.org/10.3390/pathogens11111278