
Changes in Group B Streptococcus Colonization among Pregnant Women before and after the Onset of the COVID-19 Pandemic in Brazil
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Collection of Anovaginal Samples
2.2. Detection and Isolation of GBS
2.3. Characterization of GBS Strains
2.4. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Group B Streptococcus Vaccine Development Technology Roadmap: Priority Activities for Development, Testing, Licensure and Global Availability of Group B Streptococcus Vaccines; World Health Organization: Geneva, Switzerland, 2017.
- Seale, A.C.; Bianchi-Jassir, F.; Russell, N.J.; Kohli-Lynch, M.; Tann, C.J.; Hall, J.; Madrid, L.; Blencowe, H.; Cousens, S.; Baker, C.J.; et al. Estimates of the Burden of Group B Streptococcal Disease Worldwide for Pregnant Women, Stillbirths, and Children. Clin. Infect. Dis. 2017, 65, S200–S219. [Google Scholar] [CrossRef] [PubMed]
- Zanini da Rocha, J.; Feltraco, J.; Radin, V.; Vitola Gonçalves, C.; Almeida da Silva, P.E.; Von Groll, A. Streptococcus agalactiae colonization and screening approach in high-risk pregnant women in southern Brazil. J. Infect. Dev. Ctries. 2020, 14, 332–340. [Google Scholar] [CrossRef] [PubMed]
- Shabayek, S.; Spellerberg, B. Group B Streptococcal Colonization, Molecular Characteristics, and Epidemiology. Front. Microbiol. 2018, 9, 437. [Google Scholar] [CrossRef] [PubMed]
- Baker, C.J.; Rench, M.A.; Fernandez, M.; Paoletti, L.C.; Kasper, D.L.; Edwards, M.S. Safety and immunogenicity of a bivalent group B streptococcal conjugate vaccine for serotypes II and III. J. Infect. Dis. 2003, 188, 66–73. [Google Scholar] [CrossRef]
- Slotved, H.-C.; Kong, F.; Lambertsen, L.; Sauer, S.; Gilbert, G.L. Serotype IX, a Proposed New Streptococcus agalactiae Serotype. J. Clin. Microbiol. 2007, 45, 2929–2936. [Google Scholar] [CrossRef] [PubMed]
- Nobbs, A.H.; Lamont, R.J.; Jenkinson, H.F. Streptococcus Adherence and Colonization. Microbiol. Mol. Biol. Rev. 2009, 73, 407–450. [Google Scholar] [CrossRef] [PubMed]
- Melin, P.; Efstratiou, A. Group B streptococcal epidemiology and vaccine needs in developed countries. Vaccine 2013, 31, D31–D42. [Google Scholar] [CrossRef] [PubMed]
- Dzanibe, S.; Madhi, S.A. Systematic review of the clinical development of group B streptococcus serotype-specific capsular polysaccharide-based vaccines. Expert Rev. Vaccines 2018, 17, 635–651. [Google Scholar] [CrossRef] [PubMed]
- ACOG. Prevention of Group B Streptococcal Early-Onset Disease in Newborns. 2020. Available online: https://www.acog.org/en/clinical/clinical-guidance/committee-opinion/articles/2020/02/prevention-of-group-b-streptococcal-early-onset-disease-in-newborns (accessed on 20 April 2022).
- World Health Organization. Group B Streptococcus Vaccine: Full Value Vaccine Assessment; Licence: CC BY-NC-SA 3.0 IGO; World Health Organization: Geneva, Switzerland, 2021.
- Costa. Prevenção da Doença Perinatal pelo Estreptococo do Grupo B—PDF Free Download. 2011. Available online: https://docplayer.com.br/154886-Prevencao-da-doenca-perinatal-pelo-estreptococo-do-grupo-b.html (accessed on 22 April 2022).
- Dahesh, S.; Hensler, M.E.; Van Sorge, N.M.; Gertz, R.E.; Schrag, S.; Nizet, V.; Beall, B.W. Point mutation in the group B streptococcal pbp2x gene conferring decreased susceptibility to beta-lactam antibiotics. Antimicrob. Agents Chemother. 2008, 52, 2915–2918. [Google Scholar] [CrossRef]
- Kimura, K.; Nagano, N.; Nagano, Y.; Suzuki, S.; Wachino, J.; Shibayama, K.; Arakawa, Y. High frequency of fluoroquinolone- and macrolide-resistant streptococci among clinically isolated group B streptococci with reduced penicillin susceptibility. J. Antimicrob. Chemother. 2013, 68, 539–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Do Nascimento, C.S.; dos Santos, N.F.B.; Ferreira, R.C.C.; Taddei, C.R. Streptococcus agalactiae in pregnant women in Brazil: Prevalence, serotypes, and antibiotic resistance. Braz. J. Microbiol. 2019, 50, 943–952. [Google Scholar] [CrossRef] [PubMed]
- Raabe, V.N.; Shane, A.L. Group B Streptococcus (Streptococcus agalactiae). Microbiol. Spectr. 2019, 7. [Google Scholar] [CrossRef] [PubMed]
- Hayes, K.; O’Halloran, F.; Cotter, L. A review of antibiotic resistance in Group B Streptococcus: The story so far. Crit. Rev. Microbiol. 2020, 46, 253–269. [Google Scholar] [CrossRef] [PubMed]
- Lu, B.; Chen, X.; Wang, J.; Wang, D.; Zeng, J.; Li, Y.; Li, D.; Zhu, F.; Cui, Y.; Huang, L. Molecular characteristics and antimicrobial resistance in invasive and noninvasive Group B Streptococcus between 2008 and 2015 in China. Diagn. Microbiol. Infect. Dis. 2016, 86, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Francois Watkins, L.K.; McGee, L.; Schrag, S.J.; Beall, B.; Jain, J.H.; Pondo, T.; Farley, M.M.; Harrison, L.H.; Zansky, S.M.; Baumbach, J.; et al. Epidemiology of Invasive Group B Streptococcal Infections Among Nonpregnant Adults in the United States, 2008–2016. JAMA Intern. Med. 2019, 179, 479–488. [Google Scholar] [CrossRef]
- CDC. Antibiotic Resistance Threats in the United States, 2019; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2019. [CrossRef]
- Wang, H.; Paulson, K.R.; Pease, S.A.; Watson, S.; Comfort, H.; Zheng, P.; Aravkin, A.Y.; Bisignano, C.; Barber, R.M.; Alam, T.; et al. Estimating excess mortality due to the COVID-19 pandemic: A systematic analysis of COVID-19-related mortality, 2020–2021. Lancet 2022, 399, 1513–1536. [Google Scholar] [CrossRef]
- Takemoto, M.; Menezes, M.O.; Andreucci, C.B.; Knobel, R.; Sousa, L.; Katz, L.; Fonseca, E.B.; Nakamura-Pereira, M.; Magalhães, C.G.; Diniz, C.S.G.; et al. Clinical characteristics and risk factors for mortality in obstetric patients with severe COVID-19 in Brazil: A surveillance database analysis. BJOG Int. J. Obstet. Gynaecol. 2020, 127, 1618–1626. [Google Scholar] [CrossRef]
- Takemoto, M.L.S.; Nakamura-Pereira, M.; Menezes, M.O.; Katz, L.; Knobel, R.; Amorim, M.M.R.; Andreucci, C.B. Higher case fatality rate among obstetric patients with COVID-19 in the second year of pandemic in Brazil: Do new genetic variants play a role? medRxiv 2021. [Google Scholar] [CrossRef]
- Lai, C.-C.; Yu, W.-L. The COVID-19 pandemic and tuberculosis in Taiwan. J. Infect. 2020, 81, e159–e161. [Google Scholar] [CrossRef]
- Sakamoto, H.; Ishikane, M.; Ueda, P. Seasonal Influenza Activity During the SARS-CoV-2 Outbreak in Japan. JAMA 2020, 323, 1969–1971. [Google Scholar] [CrossRef]
- Juan, H.-C.; Chao, C.-M.; Lai, C.-C.; Tang, H.-J. Decline in invasive pneumococcal disease during COVID-19 pandemic in Taiwan. J. Infect. 2021, 82, 282–327. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.-C.; Chen, S.-Y.; Ko, W.-C.; Hsueh, P.-R. Increased antimicrobial resistance during the COVID-19 pandemic. Int. J. Antimicrob. Agents 2021, 57, 106324. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Baño, J.; Rossolini, G.M.; Schultsz, C.; Tacconelli, E.; Murthy, S.; Ohmagari, N.; Holmes, A.; Bachman, T.; Goossens, H.; Canton, R.; et al. Key considerations on the potential impacts of the COVID-19 pandemic on antimicrobial resistance research and surveillance. Trans. R. Soc. Trop. Med. Hyg. 2021, 115, 1122–1129. [Google Scholar] [CrossRef] [PubMed]
- Zavala-Flores, E.; Salcedo-Matienzo, J.; Zavala-Flores, E.; Salcedo-Matienzo, J. Medicación prehospitalaria en pacientes hospitalizados por COVID-19 en un hospital público de Lima-Perú. Acta Médica Peru. 2020, 37, 393–395. [Google Scholar] [CrossRef]
- Ghosh, S.; Bornman, C.; Zafer, M.M. Antimicrobial Resistance Threats in the emerging COVID-19 pandemic: Where do we stand? J. Infect. Public Health 2021, 14, 555–560. [Google Scholar] [CrossRef]
- Sermo. Sermo, Breaking results: Sermo’s COVID-19 real time barometer study Wave I: March 25–27. 2022. Available online: https://public-cdn.sermo.com/covid19/c8/be4e/4edbd4/dbd4ba4ac5a3b3d9a479f99cc5/wave-i-sermo-covid-19-global-analysis-final.pdf (accessed on 22 April 2022).
- ASM. Guidelines for the Detection and Identification of Group B Streptococcus. 2020. Available online: https://asm.org/Guideline/Guidelines-for-the-Detection-and-Identification-of (accessed on 22 April 2022).
- Botelho, A.C.N.; Oliveira, J.G.; Damasco, A.P.; Santos, K.T.B.; Ferreira, A.F.M.; Rocha, G.T.; Marinho, P.S.; Bornia, R.B.G.; Pinto, T.C.A.; Américo, M.A.; et al. Streptococcus agalactiae carriage among pregnant women living in Rio de Janeiro, Brazil, over a period of eight years. PLoS ONE 2018, 13, e0196925. [Google Scholar] [CrossRef]
- CLSI. M100Ed32|Performance Standards for Antimicrobial Susceptibility Testing, 32nd ed.; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2021; Available online: https://clsi.org/standards/products/microbiology/documents/m100/ (accessed on 22 April 2022).
- Le Doare, K.; O’Driscoll, M.; Turner, K.; Seedat, F.; Russell, N.J.; Seale, A.C.; Heath, P.T.; Lawn, J.E.; Baker, C.J.; Bartlett, L.; et al. Intrapartum Antibiotic Chemoprophylaxis Policies for the Prevention of Group B Streptococcal Disease Worldwide: Systematic Review. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2017, 65, S143–S151. [Google Scholar] [CrossRef]
- DATASUS. Informações de Saúde (TABNET)—DATASUS. Available online: https://datasus.saude.gov.br/informacoes-de-saude-tabnet/ (accessed on 22 April 2022).
- Nomura, M.L.; Passini Júnior, R.; Oliveira, U.M.; Calil, R. Colonização materna e neonatal por estreptococo do grupo B em situações de ruptura pré-termo de membranas e no trabalho de parto prematuro. Rev. Bras. Ginecol. E Obstetrícia 2009, 31, 397–403. [Google Scholar] [CrossRef]
- Marconi, C.; Rocchetti, T.T.; Rall, V.L.M.; de Carvalho, L.R.; Borges, V.T.M.; da Silva, M.G. Detection of Streptococcus agalactiae colonization in pregnant women by using combined swab cultures: Cross-sectional prevalence study. Sao Paulo Med. J. 2010, 128, 60–62. [Google Scholar] [CrossRef] [Green Version]
- Função, J.M.; Narchi, N.Z. A study of group B streptococcus in pregnant women of eastern São Paulo. Rev. Esc. Enferm. USP 2013, 47, 22–29. [Google Scholar] [CrossRef]
- Barbosa, N.G. Colonização Materna por Estreptococos do Grupo B: Prevalência e Suscetibilidade aos Antimicrobianos. 2016. Available online: http://www.periodicoseletronicos.ufma.br/index.php/revistahuufma/article/view/5601 (accessed on 15 March 2022).
- De Melo, S.C.C.S.; Costa, A.B.; da Silva, F.T.R.; Silva, N.M.M.G.; Tashima, C.M.; Cardoso, R.F.; de Pádua, R.A.F.; Previdelli, I.; de Barros Carvalho, M.D.; Pelloso, S.M.; et al. Prevalence of Streptococcus agalactiae colonization in pregnant women from the 18th Health Region of Paraná State. Rev. Inst. Med. Trop. São Paulo, 2018; 60, e2. [Google Scholar] [CrossRef]
- Kwatra, G.; Cunnington, M.C.; Merrall, E.; Adrian, P.V.; Ip, M.; Klugman, K.P.; Tam, W.H.; MAdhi, S.A. Prevalence of maternal colonisation with group B streptococcus: A systematic review and meta-analysis. Lancet Infect. Dis. 2016, 16, 1076–1084. [Google Scholar] [CrossRef]
- Furfaro, L.L.; Chang, B.J.; Payne, M.S. Perinatal Streptococcus agalactiae epidemiology and surveillence targets. Clin. Microbiol. Rev. 2018, 31, e00049-18. [Google Scholar] [CrossRef] [PubMed]
- Gizachew, M.; Tiruneh, M.; Moges, F.; Tessema, B. Streptococcus agalactiae maternal colonization, antibiotic resistance and serotype profiles in Africa: A meta-analysis. Ann. Clin. Microbiol. Antimicrob. 2019, 18, 14. [Google Scholar] [CrossRef] [PubMed]
- Genovese, C.; D’Angeli, F.; Di Salvatore, V.; Tempera, G.; Nicolosi, D. Streptococcus agalactiae in pregnant women: Serotype and antimicrobial susceptibility patterns over five years in Eastern Sicily (Italy). Eur. J. Clin. Microbiol. Infect. Dis. Off. Publ. Eur. Soc. Clin. Microbiol. 2020, 39, 2387–2396. [Google Scholar] [CrossRef] [PubMed]
- McGee, L.; Chochua, S.; Li, Z.; Mathis, S.; Rivers, J.; Metcalf, B.; Ryan, A.; Alden, N.; Farley, M.M.; Harisson, L.H.; et al. Multistate, Population-Based Distributions of Candidate Vaccine Targets, Clonal Complexes, and Resistance Features of Invasive Group B Streptococci Within the United States, 2015–2017. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2021, 72, 1004–1013. [Google Scholar] [CrossRef] [PubMed]
- Renato de Ávila, K.; Pignatari, A.C.C.; Kusano, E.J.U.; Rocchetti, T.T.; Fonseca, C.L.; Weckx, L.Y. Capsular genotype distribution of Group B Streptococcus colonization among at-risk pregnant women in Sao Paulo, Brazil. Braz. J. Infect. Dis. 2021, 25, 101586. [Google Scholar] [CrossRef]
- Hirai, N.; Kasahara, K.; Nakano, R.; Ogawa, Y.; Suzuki, Y.; Ogawa, M.; Hishiya, N.; Nakano, A.; Ichimura, S.; Yano, H.; et al. Clinical characteristics and molecular epidemiology of invasive Streptococcus agalactiae infections between 2007 and 2016 in Nara, Japan. PLoS ONE 2020, 15, e0240590. [Google Scholar] [CrossRef]
- Zhu, Y.; Wu, J.; Zheng, X.; Chen, L.; He, M.; Ma, S.; Lin, Y.; Lin, X.; Chen, C. Identification of Group B Streptococcus Serotypes and Genotypes in Late Pregnant Women and Neonates That Are Associated with Neonatal Early-Onset Infection in a South China Population. Front. Pediatr. 2020, 8, 265. [Google Scholar] [CrossRef]
- Kao, Y.; Tsai, M.-H.; Lai, M.-Y.; Chu, S.-M.; Huang, H.-R.; Chiang, M.-C.; Fu, R.-H.; Lu, J.-J.; Hsu, J.-F. Emerging serotype III sequence type 17 group B streptococcus invasive infection in infants: The clinical characteristics and impacts on outcomes. BMC Infect. Dis. 2019, 19, 538. [Google Scholar] [CrossRef]
- De Almeida Corrêa, A.B.; da Silva, L.G.; de Castro Abreu Pinto, T.; de Oliveira, I.C.M.; Fernandes, F.G.; da Costa, N.S.; Corrêa de Mattos, M.; Longo Fracalanzza, S.E.; Benchetrit, L.C. The genetic diversity and phenotypic characterisation of Streptococcus agalactiae isolates from Rio de Janeiro, Brazil. Mem. Inst. Oswaldo Cruz 2011, 106, 1002–1006. [Google Scholar] [CrossRef]
- Dutra, V.G.; Alves, V.M.N.; Olendzki, A.N.; Dias, C.A.G.; de Bastos, A.F.A.; Santos, G.O.; de Amorin, E.L.T.; Sousa, M.Â.B.; Santos, R.; Ribeiro, P.C.S.; et al. Streptococcus agalactiae in Brazil: Serotype distribution, virulence determinants and antimicrobial susceptibility. BMC Infect. Dis. 2014, 14, 323. [Google Scholar] [CrossRef] [PubMed]
- Pinto, T.C.A.; Costa, N.S.; Souza, A.R.V.; da Silva, L.G.; de Almeida Corrêa, A.B.; Fernandes, F.G.; MenezesOliveira, I.C.; Corrêade Mattos, M.; SoaresRosado, A.; Claude Benchetrit, L. Distribution of serotypes and evaluation of antimicrobial susceptibility among human and bovine Streptococcus agalactiae strains isolated in Brazil between 1980 and 2006. Braz. J. Infect. Dis. 2013, 17, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Da Cunha, V.; Davies, M.R.; Douarre, P.-E.; Rosinski-Chupin, I.; Margarit, I.; Spinali, S.; Perkins, T.; Lechat, P.; Dmytruk, N.; Sauvage, E.; et al. Streptococcus agalactiae clones infecting humans were selected and fixed through the extensive use of tetracycline. Nat. Commun. 2014, 5, 4544. [Google Scholar] [CrossRef] [PubMed]
- Clouse, K.; Shehabi, A.; Suleimat, A.M.; Faouri, S.; Khuri-Bulos, N.; Al Jammal, A.; Chappell, J.; Fortner, K.B.; Chamby, A.B.; Randis, T.M.; et al. High prevalence of Group B Streptococcus colonization among pregnant women in Amman, Jordan. BMC Pregnancy Childbirth 2019, 19, 177. [Google Scholar] [CrossRef] [PubMed]
- Spiel, M.H.; Hacker, M.R.; Haviland, M.J.; Mulla, B.; Roberts, E.; Dodge, L.E.; Young, B.C. Racial disparities in intrapartum group B Streptococcus colonization: A higher incidence of conversion in African American women. J. Perinatol. Off. J. Calif. Perinat. Assoc. 2019, 39, 433–438. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Aspects Evaluated | All (19 January to 21 March) n = 806 | Before COVID-19 (19 January to 20 March) n = 521 | After Onset of COVID-19 (20 May to 21 March) n = 285 | p-Value |
|---|---|---|---|---|
| Sociodemographic a | ||||
| Mean age | 29.5 (13–46 years old) | 29.6 (13–46 years old) | 29.4 (13–45 years old) | 0.8897 |
| Region of birth b | ||||
| Southeast | 77.7% (580/746) | 74.5% (361/485) | 83.9% (219/261) | 0.9978 |
| North | 0.8% (6/746) | 1% (5/485) | 0.4% (1/261) | |
| Northeast | 19.8 % (148/746) | 23.1% (112/485) | 13.8% (36/261) | |
| Midwest | 0.3% (2/746) | 0.2% (1/485) | 0.4% (1/261) | |
| South | 0.7% (5/746) | 0.8% (4/485) | 0.4% (1/261) | |
| Marital status | ||||
| Married | 47.9% (346/722) | 46.4% (219/472) | 50.8% (127/250) | 1.0000 |
| Single | 52.1 (376/722) | 53.6% (253/472) | 49.2% (123/250) | |
| Ethnicity c | ||||
| Black | 20.6% (158/766) | 20.2% (99/491) | 21.5% (59/275) | 1.0000 |
| Brown | 37.9% (290/766) | 40.3% (198/491) | 33.5% (92/275) | |
| White | 40.9% (313/766) | 38.9% (191/491) | 44.4% (122/275) | |
| Level of education d | ||||
| Basic education | 23.1% (163/707) | 26% (120/461) | 17.5% (43/246) | 0.9998 |
| High school | 59.5% (421/707) | 58.6% (270/461) | 61.4% (151/246) | |
| Higher education | 17.3% (122/707) | 15.2% (70/461) | 21.1% (52/246) | |
| Clinical a | ||||
| Previous preterm delivery | 9.6% (74/773) | 10.2% (51/498) | 8.4% (23/275) | 1.0000 |
| Previous neonatal death | 4.4% (33/757) | 4.1% (20/486) | 4.8% (13/271) | 1.0000 |
| Previous neonatal GBS infection | 0.4% (3/717) | 0.4% (2/461) | 0.4% (1/256) | 1.0000 |
| Vaginal discharge | 27.5% (200/728) | 27.3% (129/472) | 27.7% (71/256) | 1.0000 |
| Urinary tract infection | 23.4% (180/770) | 23.6% (118/500) | 23% (62/270) | 1.0000 |
| Use of antibiotics | 28.8% (218/757) | 29.2% (144/493) | 28% (74/264) | 1.0000 |
| Pre-existing pathologies | 55.7% (427/766) | 58.8% (291/495) | 50.2% (136/271) | 1.0000 |
| Aspects Evaluated | All Clinical Samples n = 806 | GBS Positive Samples n = 87 | GBS Negative Samples n = 719 | p-Value |
|---|---|---|---|---|
| Sociodemographic a | ||||
| Mean age | 29.5 (13–46 years old) | 29.8 (13–43 years old) | 29.5 (13–46 years old) | 0.9292 |
| Region of birth b | ||||
| Southeast | 77.7% (580/746) | 72.8% (59/81) | 78.3% (521/665) | 0.9999 |
| North | 0.8% (6/746) | 0% (0/81) | 0.9% (6/665) | |
| Northeast | 19.8 % (148/746) | 26% (21/81) | 19.1% (127/665) | |
| Midwest | 0.3% (2/746) | 0% (0/81) | 0.3% (2/665) | |
| South | 0.7% (5/746) | 0% (0/81) | 0.7% (5/665) | |
| Marital status | ||||
| Married | 47.9% (346/722) | 43.2% (35/81) | 45% (311/691) | 0.6662 |
| Single | 52.1 (376/722) | 56.8% (46/81) | 47.8% (330/691) | |
| Ethnicity c | ||||
| Black | 20.6% (158/766) | 24.1% (20/83) | 20.2% (138/683) | 0.9920 |
| Brown | 37.9% (290/766) | 33.7% (28/83) | 38.4% (262/683) | |
| White | 40.9% (313/766) | 42.2% (35/83) | 40.7% (278/683) | |
| Level of education d | ||||
| Basic education | 23.1% (163/707) | 32.4% (24/74) | 22% (139/633) | 0.9948 |
| High school | 59.5% (421/707) | 48.6% (36/74) | 60.8% (385/633) | |
| Higher education | 17.3% (122/707) | 17.6% (13/74) | 17.2% (109/633) | |
| Clinical a | ||||
| Previous preterm delivery | 9.6% (74/773) | 9.5% (8/84) | 9.6% (66/689) | 1.0000 |
| Previous prenatal death | 4.4% (33/757) | 2.4% (2/82) | 4.6% (31/675) | 1.0000 |
| Previous neonatal GBS infection | 0.4% (3/717) | 0% (0/77) | 0.5% (3/640) | 1.0000 |
| Vaginal discharge | 27.5% (200/728) | 30.5% (25/82) | 27.1% (175/646) | 1.0000 |
| Urinary tract infection | 23.4% (180/770) | 17.9% (15/84) | 24% (165/686) | 1.0000 |
| Use of antibiotics | 28.8% (218/757) | 20.5% (17/83) | 29.8% (201/674) | 1.0000 |
| Pre-existing pathologies | 55.7% (427/766) | 56.1% (46/82) | 55.7% (381/684) | 1.0000 |
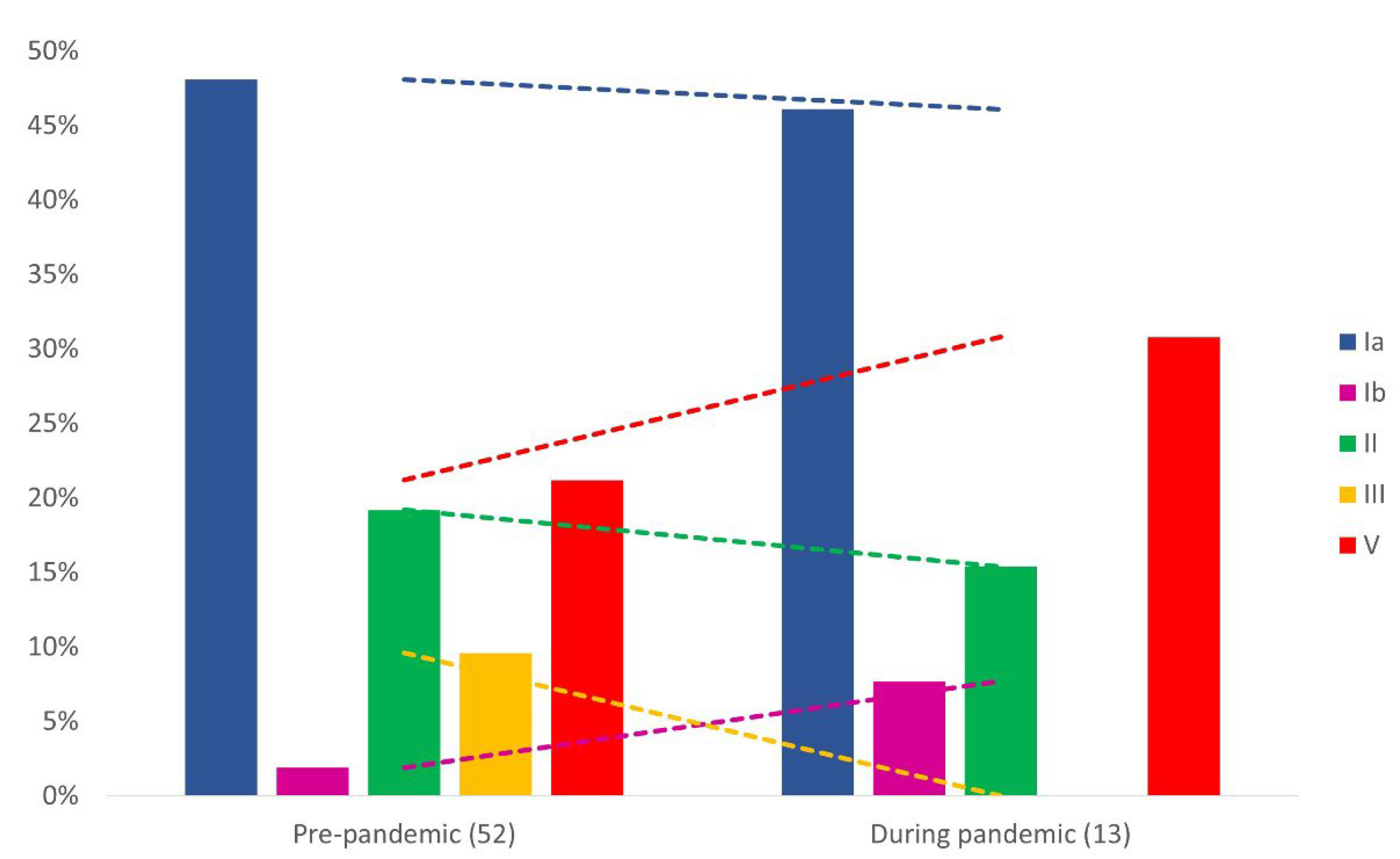
| Serotype | All NS a Strains (19 January to 21 March) n = 52 | NS Strains before COVID-19 (19 January to 20 March) n = 40 | NS Strains after Onset of COVID-19 (20 May to 21 March) n = 12 | p-Value b |
|---|---|---|---|---|
| Ia | 77.4% (24/31) | 76% (19/25) | 83.3% (5/6) | 1.0000 |
| Ib | 100% (2/2) | 100% (1/1) | 100% (1/1) | N/A c |
| II | 91.7% (11/12) | 90% (9/10) | 100% (2/2) | 1.0000 |
| III | 60% (3/5) | 60% (3/5) | 0% (0/0) | N/Ac |
| V | 80% (12/15) | 72.7% (8/11) | 100% (4/4) | 0.5165 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costa, N.S.; Rio-Tinto, A.; Pinto, I.B.F.; dos Santos Silva Alvim, D.C.; de Assis Rocha, A.; Oliveira, L.M.A.; Botelho, A.C.N.; Fracalanzza, S.E.L.; Teixeira, L.M.; Rezende-Filho, J.; et al. Changes in Group B Streptococcus Colonization among Pregnant Women before and after the Onset of the COVID-19 Pandemic in Brazil. Pathogens 2022, 11, 1104. https://doi.org/10.3390/pathogens11101104
Costa NS, Rio-Tinto A, Pinto IBF, dos Santos Silva Alvim DC, de Assis Rocha A, Oliveira LMA, Botelho ACN, Fracalanzza SEL, Teixeira LM, Rezende-Filho J, et al. Changes in Group B Streptococcus Colonization among Pregnant Women before and after the Onset of the COVID-19 Pandemic in Brazil. Pathogens. 2022; 11(10):1104. https://doi.org/10.3390/pathogens11101104
Chicago/Turabian StyleCosta, Natália Silva, André Rio-Tinto, Isabella Bittencourt Ferreira Pinto, Danielle Cristina dos Santos Silva Alvim, Amanda de Assis Rocha, Laura Maria Andrade Oliveira, Ana Caroline Nunes Botelho, Sergio Eduardo Longo Fracalanzza, Lucia Martins Teixeira, Jorge Rezende-Filho, and et al. 2022. "Changes in Group B Streptococcus Colonization among Pregnant Women before and after the Onset of the COVID-19 Pandemic in Brazil" Pathogens 11, no. 10: 1104. https://doi.org/10.3390/pathogens11101104