
Tick-Borne Encephalitis Virus Seropositivity among Tick Infested Individuals in Serbia

 ,
,  ,
,  , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Selection of Healthy Blood Donor Samples
2.3. Tick Collection and Classification
2.4. Blood Sample Collection and Detection of Anti-TBEV Antibodies
2.5. Data and Statistical Analysis
3. Results
3.1. Patient Enrollment
3.2. Tick Infestation among Enrolled Patients
3.3. Clinical Course in Patients Infested with Ticks
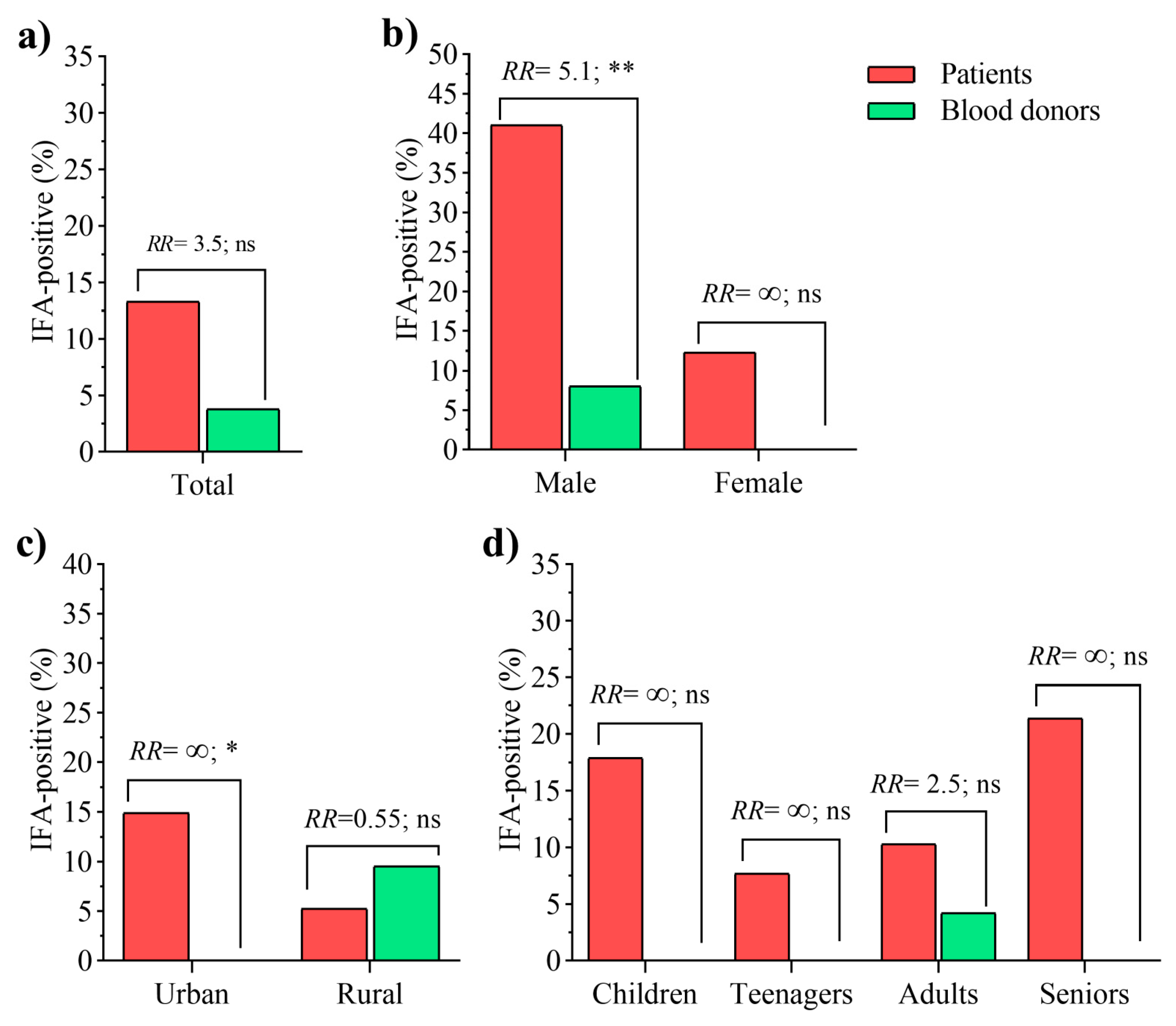
3.4. TBEV Seroprevalence in Patients and Healthy Donors
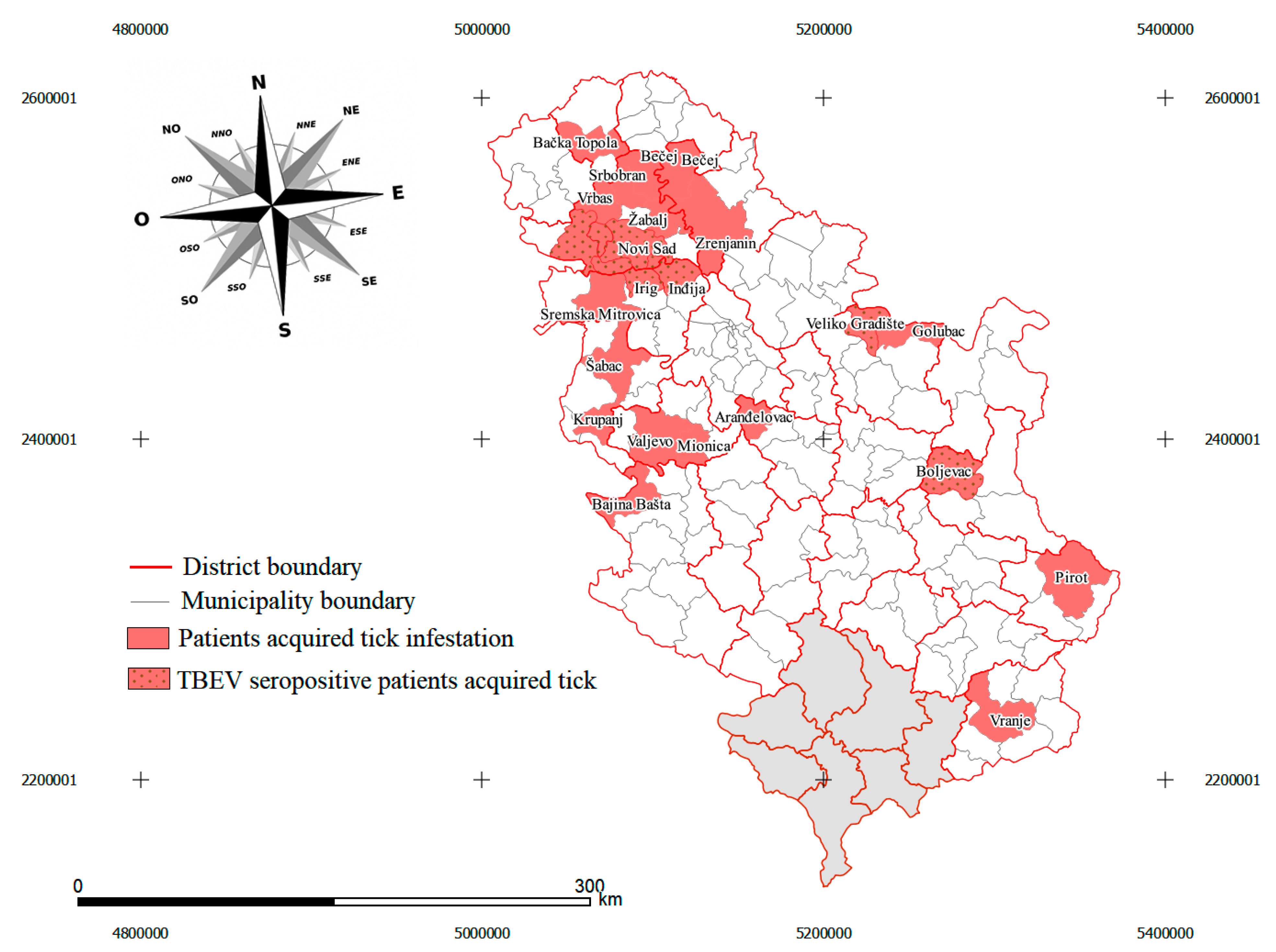
3.5. Identification of Potential TBEV Foci
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ruzek, D.; Avšič Županc, T.; Borde, J.; Chrdle, A.; Eyer, L.; Karganova, G.; Kholodilov, I.; Knap, N.; Kozlovskaya, L.; Matveev, A.; et al. Tick-Borne Encephalitis in Europe and Russia: Review of Pathogenesis, Clinical Features, Therapy, and Vaccines. Antivir. Res. 2019, 164, 23–51. [Google Scholar] [CrossRef] [PubMed]
- Kunze, U. The International Scientific Working Group on Tick-Borne Encephalitis (ISW TBE): Review of 17 Years of Activity and Commitment. Ticks Tick-Borne Dis. 2016, 7, 399–404. [Google Scholar] [CrossRef] [PubMed]
- Grard, G.; Moureau, G.; Charrel, R.N.; Lemasson, J.-J.; Gonzalez, J.-P.; Gallian, P.; Gritsun, T.S.; Holmes, E.C.; Gould, E.A.; de Lamballerie, X. Genetic Characterization of Tick-Borne Flaviviruses: New Insights into Evolution, Pathogenetic Determinants and Taxonomy. Virology 2007, 361, 80–92. [Google Scholar] [CrossRef]
- Knap, N.; Avšič-Županc, T. Factors Affecting the Ecology of Tick-Borne Encephalitis in Slovenia. Epidemiol. Infect. 2015, 143, 2059–2067. [Google Scholar] [CrossRef] [PubMed]
- Süss, J.; Klaus, C.; Diller, R.; Schrader, C.; Wohanka, N.; Abel, U. TBE Incidence versus Virus Prevalence and Increased Prevalence of the TBE Virus in Ixodes Ricinus Removed from Humans. Int. J. Med. Microbiol. 2006, 296, 63–68. [Google Scholar] [CrossRef]
- Chrdle, A.; Chmelík, V.; Růžek, D. Tick-Borne Encephalitis: What Travelers Should Know When Visiting an Endemic Country. Hum. Vaccines Immunother. 2016, 12, 2694–2699. [Google Scholar] [CrossRef] [Green Version]
- Rizzoli, A.; Tagliapietra, V.; Cagnacci, F.; Marini, G.; Arnoldi, D.; Rosso, F.; Rosà, R. Parasites and Wildlife in a Changing World: The Vector-Host- Pathogen Interaction as a Learning Case. Int. J. Parasitol. Parasites Wildl. 2019, 9, 394–401. [Google Scholar] [CrossRef] [PubMed]
- Bournez, L.; Umhang, G.; Moinet, M.; Boucher, J.-M.; Demerson, J.-M.; Caillot, C.; Legras, L.; Devillers, E.; Hansmann, Y.; Velay, A.; et al. Disappearance of TBEV Circulation among Rodents in a Natural Focus in Alsace, Eastern France. Pathogens 2020, 9, 930. [Google Scholar] [CrossRef]
- Lindblom, P.; Wilhelmsson, P.; Fryland, L.; Sjöwall, J.; Haglund, M.; Matussek, A.; Ernerudh, J.; Vene, S.; Nyman, D.; Andreassen, Å.; et al. Tick-Borne Encephalitis Virus in Ticks Detached from Humans and Follow-up of Serological and Clinical Response. Ticks Tick-Borne Dis. 2014, 5, 21–28. [Google Scholar] [CrossRef] [Green Version]
- Ilic, M.; Barbic, L.; Bogdanic, M.; Tabain, I.; Savic, V.; Kosanovic Licina, M.L.; Kaic, B.; Jungic, A.; Vucelja, M.; Angelov, V.; et al. Tick-Borne Encephalitis Outbreak Following Raw Goat Milk Consumption in a New Micro-Location, Croatia, June 2019. Ticks Tick-Borne Dis. 2020, 11, 101513. [Google Scholar] [CrossRef]
- Dobler, G.; Gniel, D.; Petermann, R.; Pfeffer, M. Epidemiology and Distribution of Tick-Borne Encephalitis. Wien. Med. Wochenschr. 2012, 162, 230–238. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Tick-Borne Encephalitis: Annual Epidemiological Report for 2018; ECDC: Stockholm, Sweden, 2019. [Google Scholar]
- Riccardi, N.; Antonello, R.M.; Luzzati, R.; Zajkowska, J.; Di Bella, S.; Giacobbe, D.R. Tick-Borne Encephalitis in Europe: A Brief Update on Epidemiology, Diagnosis, Prevention, and Treatment. Eur. J. Intern. Med. 2019, 62, 1–6. [Google Scholar] [CrossRef]
- Tkachev, S.E.; Babkin, I.V.; Chicherina, G.S.; Kozlova, I.V.; Verkhozina, M.M.; Demina, T.V.; Lisak, O.V.; Doroshchenko, E.K.; Dzhioev, Y.P.; Suntsova, O.V.; et al. Genetic Diversity and Geographical Distribution of the Siberian Subtype of the Tick-Borne Encephalitis Virus. Ticks Tick-Borne Dis. 2020, 11, 101327. [Google Scholar] [CrossRef]
- Nah, K.; Bede-Fazekas, Á.; Trájer, A.J.; Wu, J. The Potential Impact of Climate Change on the Transmission Risk of Tick-Borne Encephalitis in Hungary. BMC Infect. Dis. 2020, 20, 34. [Google Scholar] [CrossRef] [Green Version]
- Bordoski, M.; Gligić, A.; Bosković, R. Arbovirus infections in Serbia. Vojnosanit. Pregl. 1972, 29, 173–175. [Google Scholar] [PubMed]
- Potkonjak, A.; Petrović, T.; Ristanović, E.; Lalić, I.; Vračar, V.; Savić, S.; Turkulov, V.; Čanak, G.; Milošević, V.; Vidanović, D.; et al. Molecular Detection and Serological Evidence of Tick-Borne Encephalitis Virus in Serbia. Vector-Borne Zoonotic Dis. 2017, 17, 813–820. [Google Scholar] [CrossRef] [PubMed]
- Poluga, J.; Barac, A.; Katanic, N.; Rubino, S.; Milosevic, B.; Urosevic, A.; Mitrovic, N.; Kelic, I.; Micic, J.; Stevanovic, G. Tick-Borne Encephalitis in Serbia: A Case Series. J. Infect. Dev. Ctries. 2019, 13, 510–515. [Google Scholar] [CrossRef]
- Hrnjakovic-Cvjetkovic, I.; Cvjetkovic, D.; Patic, A.; Radovanov, J.; Kovacevic, G.; Milosevic, V. Tick-Borne Encephalitis Virus Infection in Humans. Med. Pregl. 2016, 69, 93–98. [Google Scholar] [CrossRef] [Green Version]
- Estrada-Peña, A.; Mihalca, A.D.; Petney, T.N. Ticks of Europe and North Africa: A Guide to Species Identification; Springer International Publishing: Berlin/Heidelberg, Germany, 2018; ISBN 978-3-319-63760-0. [Google Scholar]
- Gray, J.; Stanek, G.; Kundi, M.; Kocianova, E. Dimensions of Engorging Ixodes Ricinus as a Measure of Feeding Duration. Int. J. Med. Microbiol. 2005, 295, 567–572. [Google Scholar] [CrossRef]
- Thrusfield, M.V. Veterinary Epidemiology, 3rd ed.; Reissued in Paperback with Updates; Blackwell Science: Oxford, UK, 2007; ISBN 978-1-4051-5627-1. [Google Scholar]
- Beauté, J.; Spiteri, G.; Warns-Petit, E.; Zeller, H. Tick-Borne Encephalitis in Europe, 2012 to 2016. Eurosurveillance 2018, 23, 1800201. [Google Scholar] [CrossRef] [Green Version]
- Smura, T.; Tonteri, E.; Jääskeläinen, A.; von Troil, G.; Kuivanen, S.; Huitu, O.; Kareinen, L.; Uusitalo, J.; Uusitalo, R.; Hannila-Handelberg, T.; et al. Recent Establishment of Tick-Borne Encephalitis Foci with Distinct Viral Lineages in the Helsinki Area, Finland. Emerg. Microbes Infect. 2019, 8, 675–683. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Epidemiological Situation of Tick-Borne Encephalitis in the European Union and European Free Trade Association Countries; Publications Office: Stockholm, Sweden, 2012. [Google Scholar]
- Velay, A.; Solis, M.; Kack-Kack, W.; Gantner, P.; Maquart, M.; Martinot, M.; Augereau, O.; De Briel, D.; Kieffer, P.; Lohmann, C.; et al. A New Hot Spot for Tick-Borne Encephalitis (TBE): A Marked Increase of TBE Cases in France in 2016. Ticks Tick-Borne Dis. 2018, 9, 120–125. [Google Scholar] [CrossRef]
- Reusken, C.; Boonstra, M.; Rugebregt, S.; Scherbeijn, S.; Chandler, F.; Avšič-Županc, T.; Vapalahti, O.; Koopmans, M.; GeurtsvanKessel, C.H. An Evaluation of Serological Methods to Diagnose Tick-Borne Encephalitis from Serum and Cerebrospinal Fluid. J. Clin. Virol. 2019, 120, 78–83. [Google Scholar] [CrossRef]
- Petrović, T.; Šekler, M.; Petrić, D.; Vidanović, D.; Potkonjak, A.; Hrnjaković Cvjetković, I.; Savić, S.; Debeljak, Z.; Lazić, G.; Ignjatović Ćupina, A.; et al. Flaviviruses at the Territory of Serbia—Present Situation and Challenges. Arch. Vet. Med. 2019, 11, 53–70. [Google Scholar] [CrossRef]
- Siennicka, J.; Trzcińska, A.; Gut, W. Immunity against tick borne encephalitis virus (TBE) in population of forest workers in Bialowieza. Przegl. Epidemiol. 2010, 64, 303–305. [Google Scholar]
- Oehme, R.; Hartelt, K.; Backe, H.; Brockmann, S.; Kimmig, P. Foci of Tick-Borne Diseases in Southwest Germany. Int. J. Med. Microbiol. IJMM 2002, 291 (Suppl. 33), 22–29. [Google Scholar] [CrossRef]
- Borde, J.P.; Kaier, K.; Hehn, P.; Matzarakis, A.; Frey, S.; Bestehorn, M.; Dobler, G.; Chitimia-Dobler, L. The Complex Interplay of Climate, TBEV Vector Dynamics and TBEV Infection Rates in Ticks—Monitoring a Natural TBEV Focus in Germany, 2009–2018. PLoS ONE 2021, 16, e0244668. [Google Scholar] [CrossRef]
- Hubálek, Z. Epidemiology of Lyme Borreliosis. In Lyme Borreliosis; Karger: Basel, Switzerland, 2009; pp. 31–50. [Google Scholar]
- Toczylowski, K.; Bojkiewicz, E.; Barszcz, M.; Wozinska-Klepadlo, M.; Potocka, P.; Sulik, A. Etiology, Clinical Presentation and Incidence of Infectious Meningitis and Encephalitis in Polish Children. J. Clin. Med. 2020, 9, 2324. [Google Scholar] [CrossRef]
- Karelis, G.; Bormane, A.; Logina, I.; Lucenko, I.; Suna, N.; Krumina, A.; Donaghy, M. Tick-Borne Encephalitis in Latvia 1973-2009: Epidemiology, Clinical Features and Sequelae. Eur. J. Neurol. 2012, 19, 62–68. [Google Scholar] [CrossRef]
- Gritsun, T.S.; Lashkevich, V.A.; Gould, E.A. Tick-Borne Encephalitis. Antivir. Res. 2003, 57, 129–146. [Google Scholar] [CrossRef]
- Savić, S.; Vidić, B.; Lazić, S.; Lako, B.; Potkonjak, A.; Lepšanović, Z. Borrelia Burgdorferi in Ticks and Dogs in the Province of Vojvodina, Serbia. Parasite 2010, 17, 357–361. [Google Scholar] [CrossRef] [Green Version]
- Simin, V.; Lalošević, D.; Mijatović, D.; Tomanović, S.; Miljević, M.; Čabrilo, B.; Bogdan, I.; Banović, P. Borellia Burgdorferi Infection in Removed Ticks and Anti-Borrelia Antibodies in Infested Patients Admitted to the Pasteur Institute, Novi Sad. Vet. Glas. 2020, 74, 164–177. [Google Scholar] [CrossRef]
- Banović, P.; Díaz-Sánchez, A.A.; Galon, C.; Simin, V.; Mijatović, D.; Obregón, D.; Moutailler, S.; Cabezas-Cruz, A. Humans Infested with Ixodes Ricinus Are Exposed to a Diverse Array of Tick-Borne Pathogens in Serbia. Ticks Tick-Borne Dis. 2020, 101609. [Google Scholar] [CrossRef]
- Amicizia, D.; Domnich, A.; Panatto, D.; Lai, P.L.; Cristina, M.L.; Avio, U.; Gasparini, R. Epidemiology of Tick-Borne Encephalitis (TBE) in Europe and Its Prevention by Available Vaccines. Hum. Vaccines Immunother. 2013, 9, 1163–1171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mihalca, A.D.; Sándor, A.D. The Role of Rodents in the Ecology of Ixodes Ricinus and Associated Pathogens in Central and Eastern Europe. Front. Cell. Infect. Microbiol. 2013, 3. [Google Scholar] [CrossRef] [Green Version]
- Karbowiak, G.; Biernat, B. The Role of Particular Tick Developmental Stages in the Circulation of Tick-Borne Pathogens Affecting Humans in Central Europe. 2. Tick-Borne Encephalitis Virus. Ann. Parasitol. 2016, 62, 3–9. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Risk Group | Patients | Blood Donors |
|---|---|---|
| Gender | ||
| Male | 56 | 25 |
| Female | 57 | 25 |
| Total | 113 | 50 |
| Age | ||
| Children | 28 | 0 |
| Teenagers | 13 | 2 |
| Adults | 58 | 48 |
| Seniors | 14 | 0 |
| Total | 113 | 50 |
| Settlement | ||
| Urban | 94 | 29 |
| Rural | 19 | 21 |
| Total | 113 | 50 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Banović, P.; Obregón, D.; Mijatović, D.; Simin, V.; Stankov, S.; Budakov-Obradović, Z.; Bujandrić, N.; Grujić, J.; Sević, S.; Turkulov, V.; et al. Tick-Borne Encephalitis Virus Seropositivity among Tick Infested Individuals in Serbia. Pathogens 2021, 10, 301. https://doi.org/10.3390/pathogens10030301
Banović P, Obregón D, Mijatović D, Simin V, Stankov S, Budakov-Obradović Z, Bujandrić N, Grujić J, Sević S, Turkulov V, et al. Tick-Borne Encephalitis Virus Seropositivity among Tick Infested Individuals in Serbia. Pathogens. 2021; 10(3):301. https://doi.org/10.3390/pathogens10030301
Chicago/Turabian StyleBanović, Pavle, Dasiel Obregón, Dragana Mijatović, Verica Simin, Srdjan Stankov, Zorana Budakov-Obradović, Nevenka Bujandrić, Jasmina Grujić, Siniša Sević, Vesna Turkulov, and et al. 2021. "Tick-Borne Encephalitis Virus Seropositivity among Tick Infested Individuals in Serbia" Pathogens 10, no. 3: 301. https://doi.org/10.3390/pathogens10030301