
Evaluation of Optimal Mechanical Ventilation Strategies for Schools for Reducing Risks of Airborne Viral Infection


Abstract
:1. Introduction
2. Materials and Methods
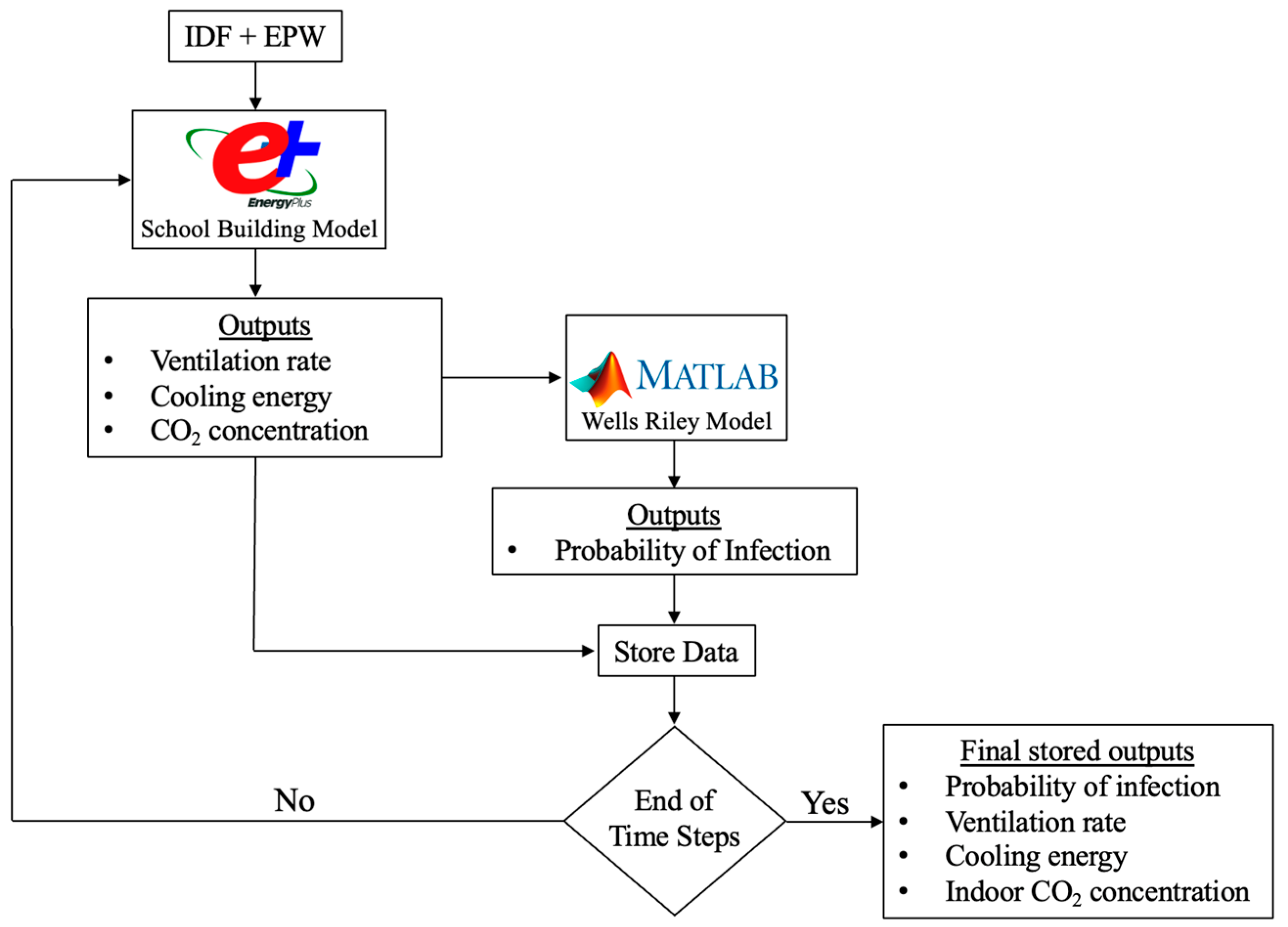
2.1. Analysis Methods
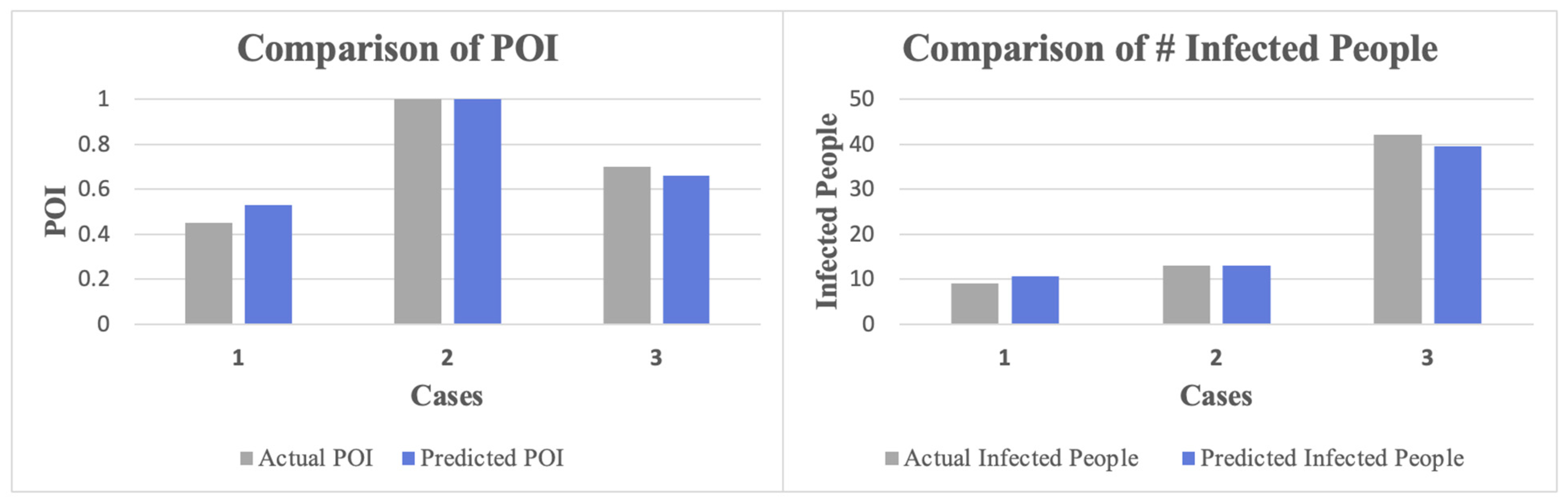
2.2. The Wells–Riley Model
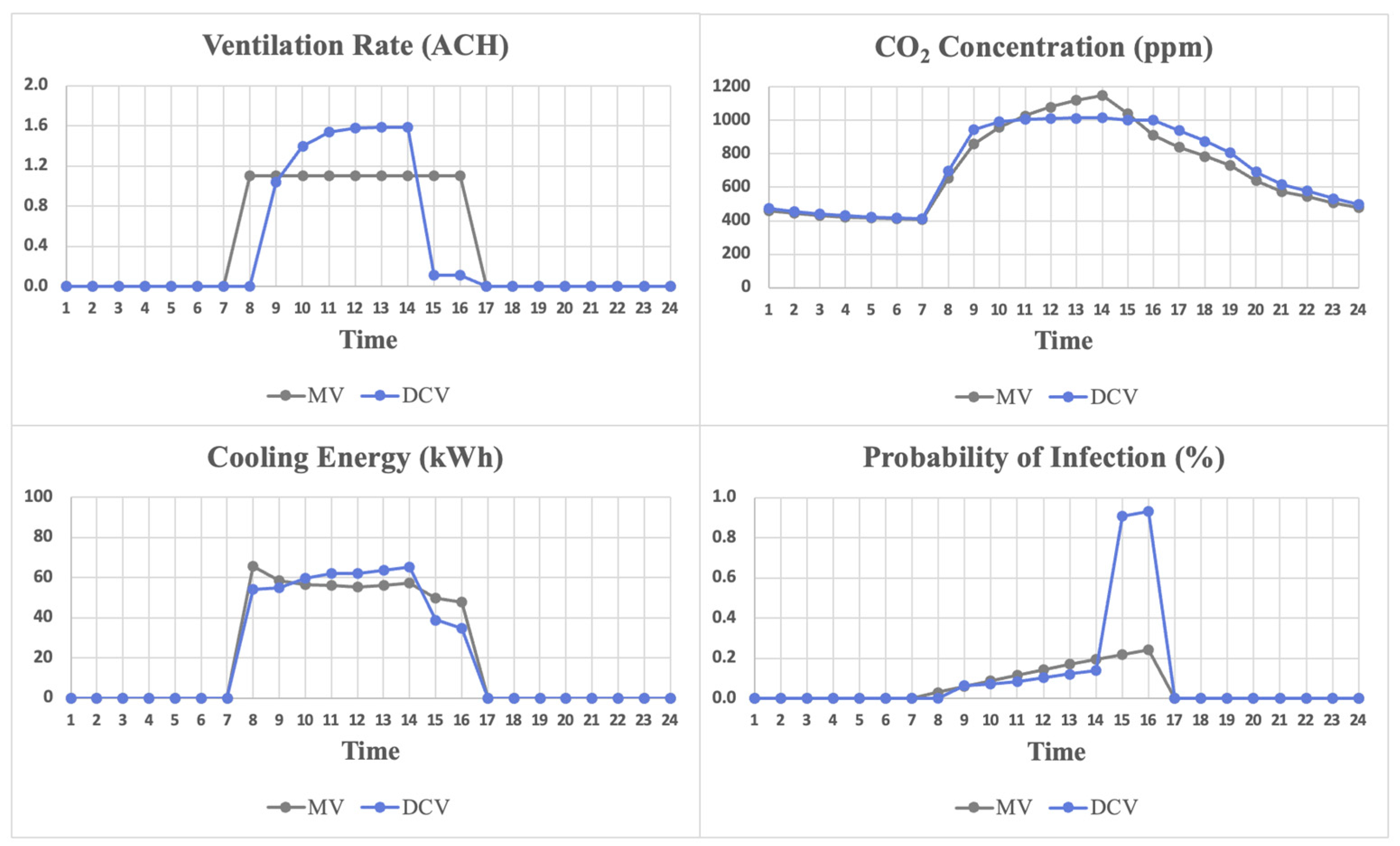
- Compare the performance of MV and demand control ventilation (DCV) systems using hourly simulations for a summer day (22 July) using the following as metrics: POI, CO2 concentration, and cooling energy use.
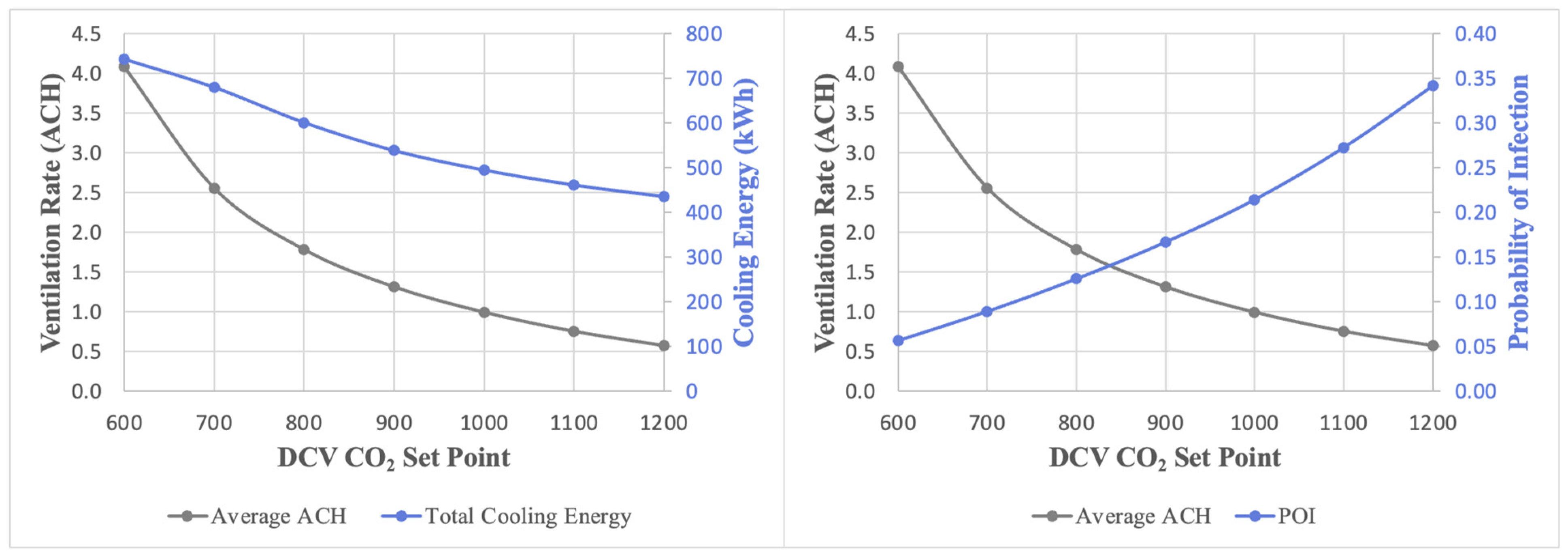
- Adjust the DCV set point (CO2 set point in ppm) and assess its effect on the probability of infection and cooling energy use.
- Perform a series of sensitivity analyses to determine the impacts of social distancing on the performance of MV and DCV including POI, indoor CO2 concentration, and cooling energy use.
- Establish any correlation between social distancing, number of infectors, and the resulting POI for MV.
- Assess variations in POI and cooling energy use for a range of ventilation rates and social distances for MV.
3. Results and Discussion
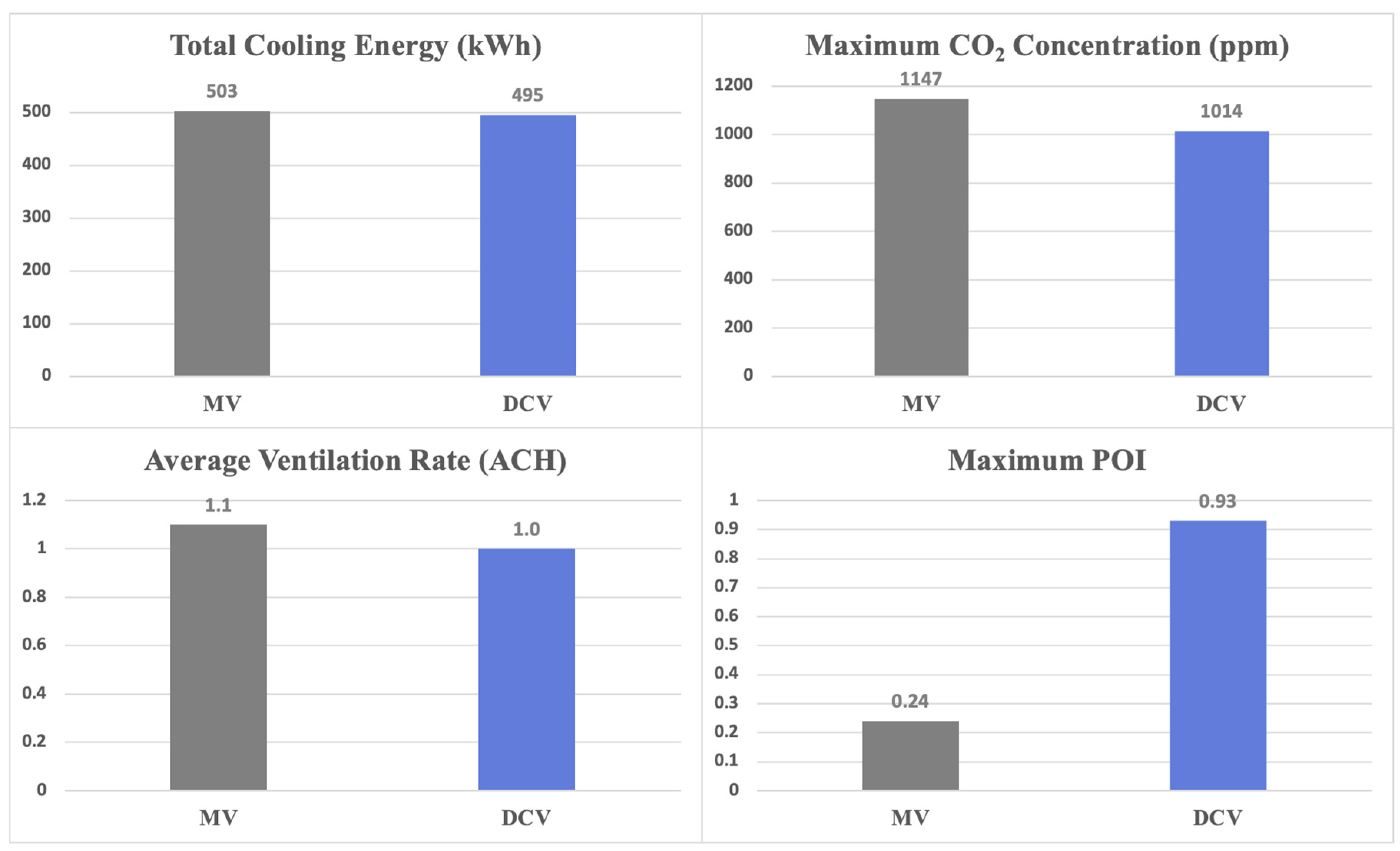
3.1. Performance Comparison for MV and DCV
- Will DCV be able to prevent high POI while still maintaining low cooling energy consumption compared to the conventional MV if the CO2 set points are adjusted?
- Will MV be able to outperform DCV considering cooling energy use and indoor air quality (i.e., CO2 concentration and infection risk) when optimized?
3.2. DCV Set Point Analysis
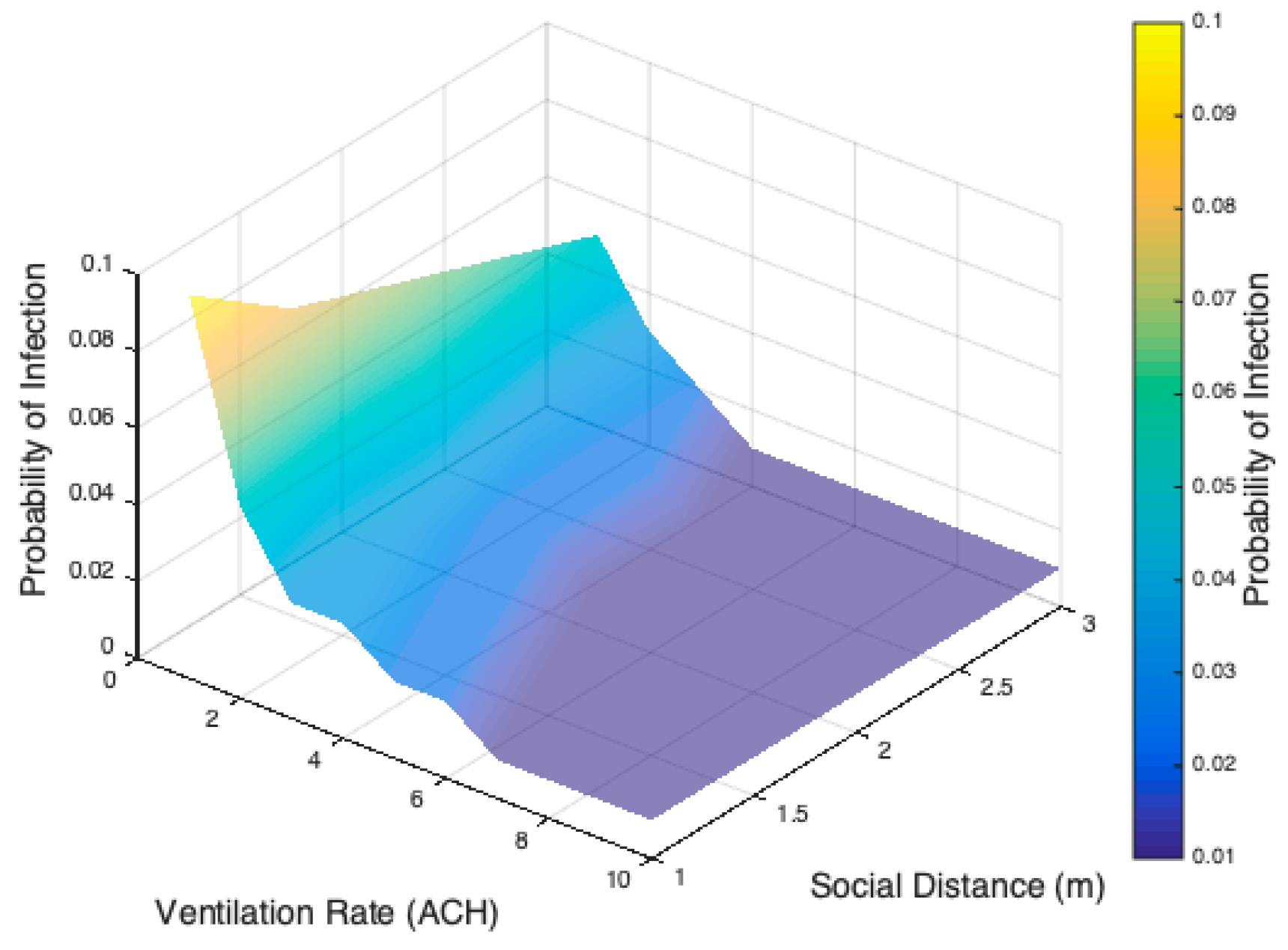
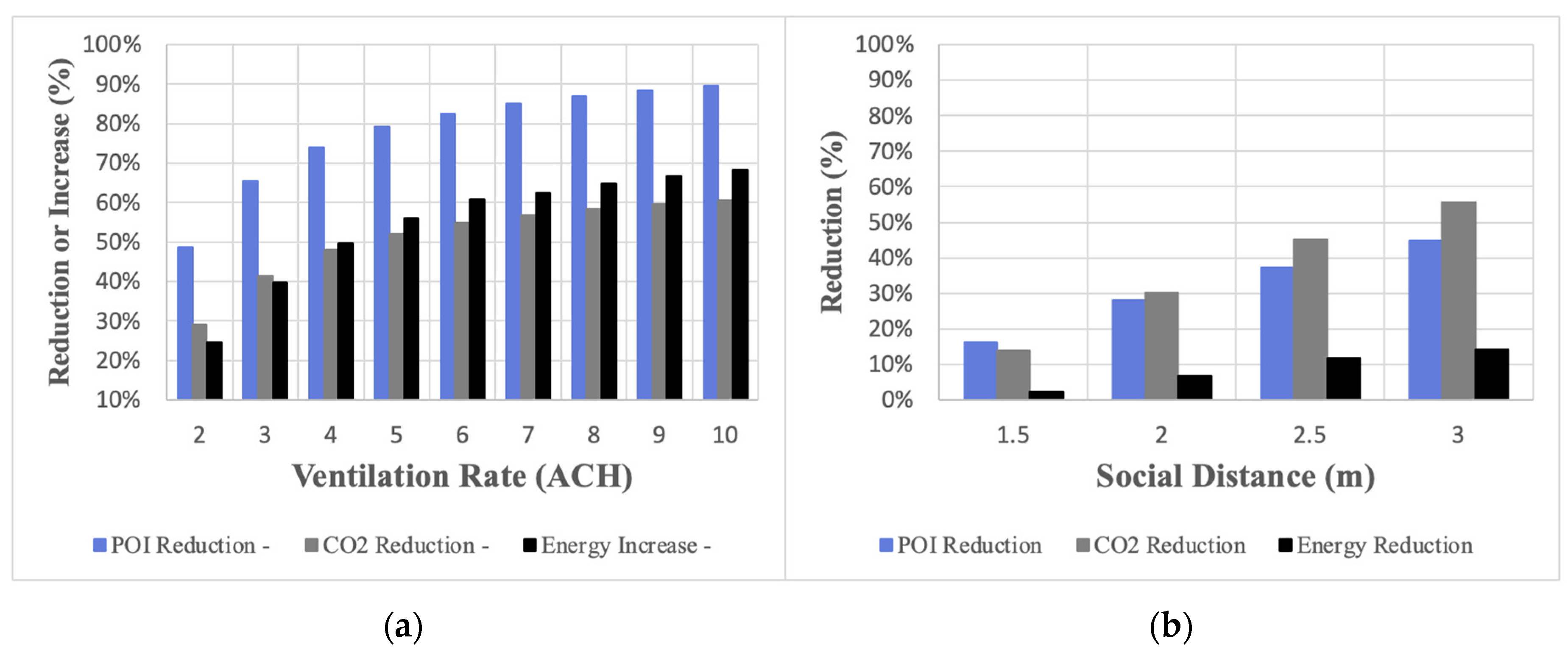
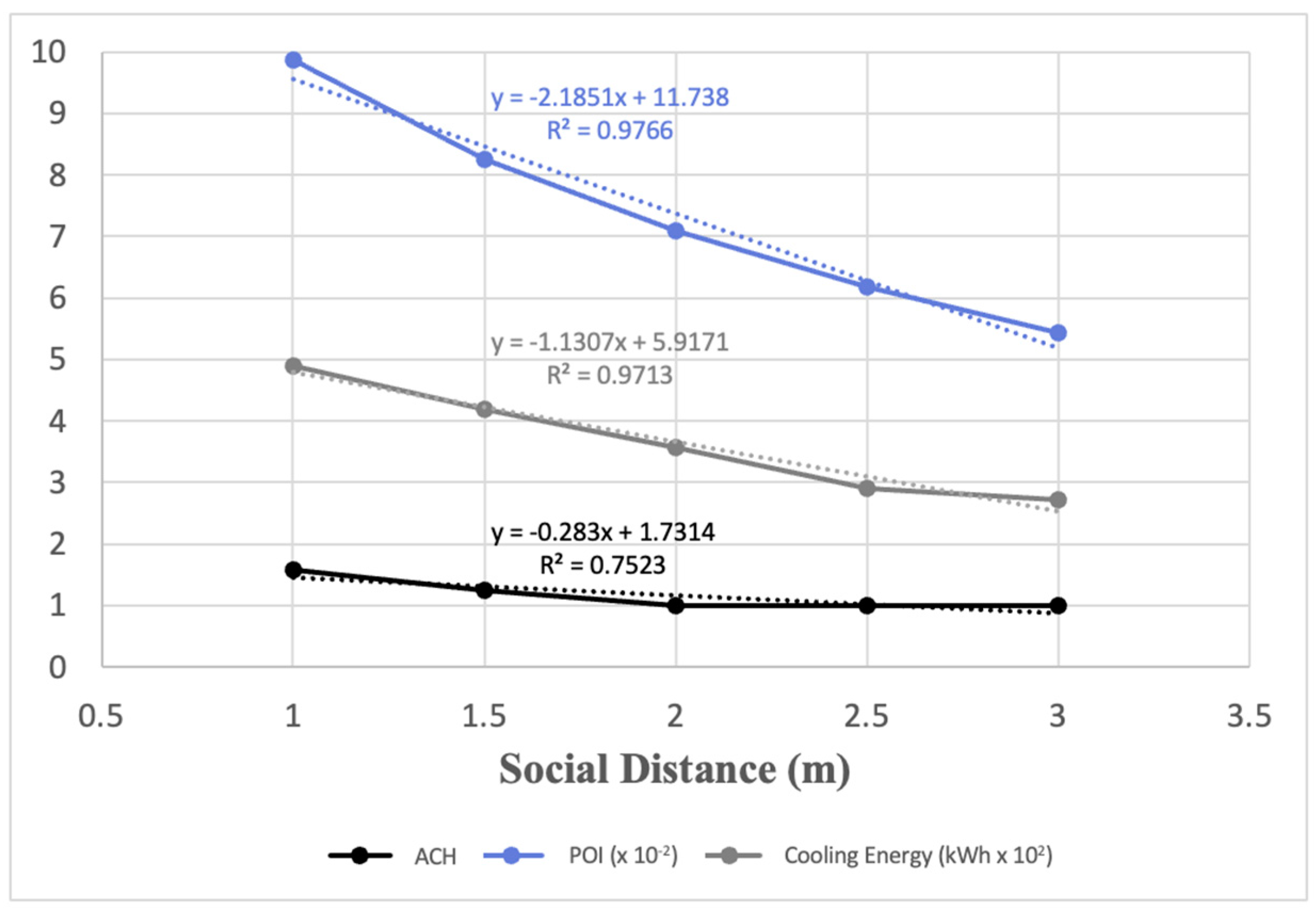
3.3. Sensitivity Analysis of MV
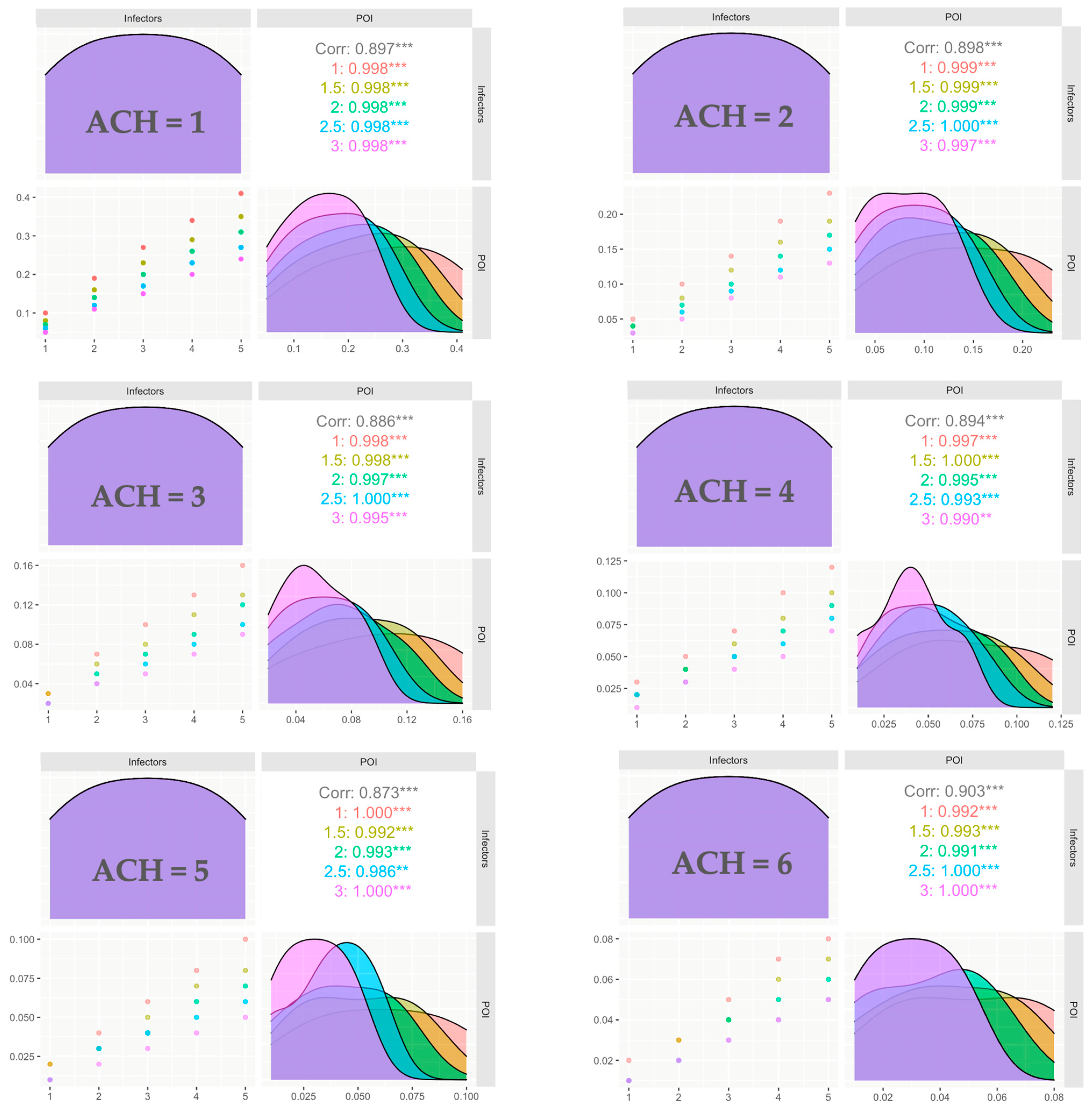
3.4. Impact of the Number of Infectors
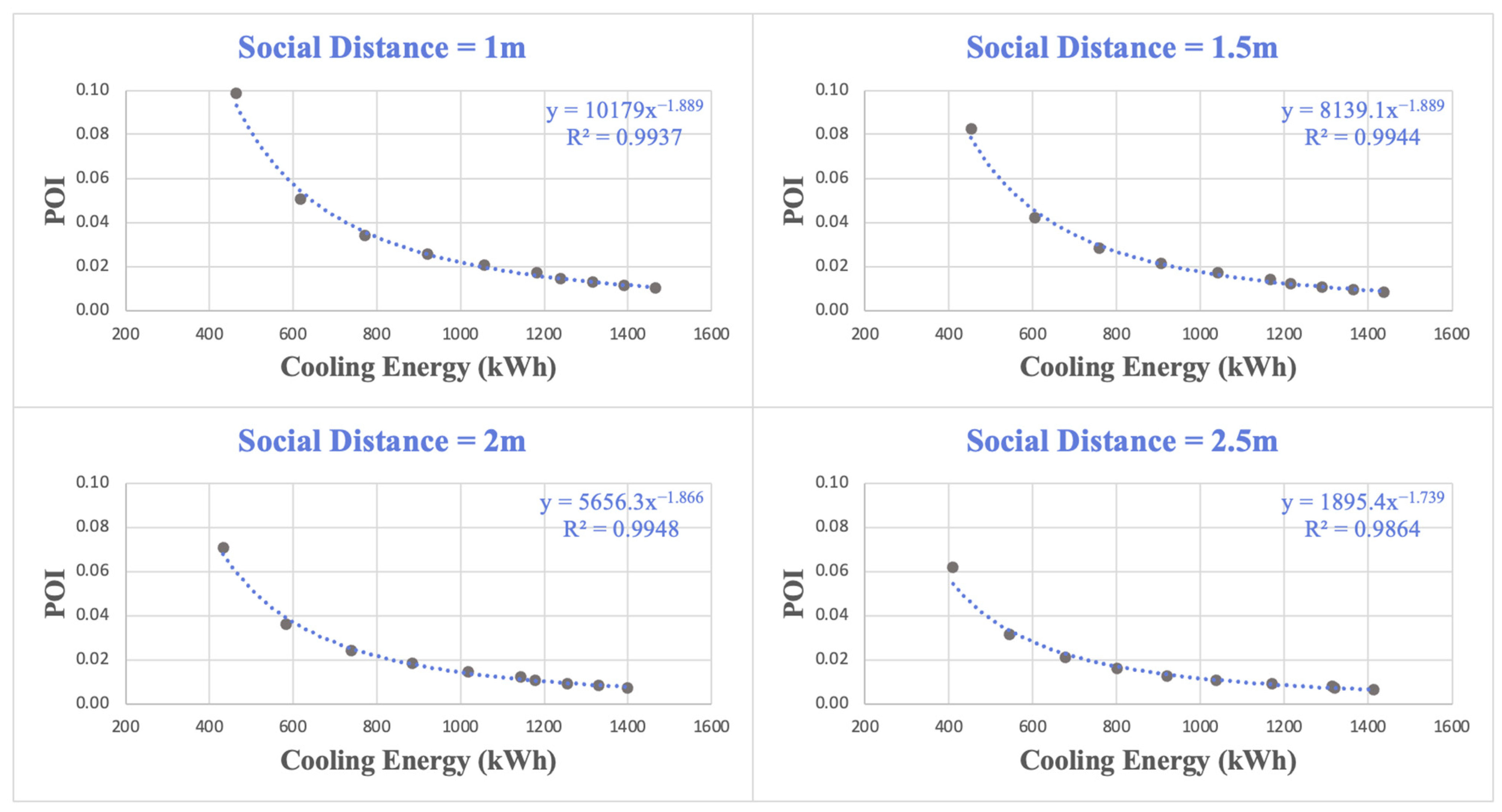
3.5. Correlation of POI and Cooling Energy
4. Conclusions
- When considering the risk of infection transmission, optimized MV could be more energy-efficient than the DCV system according to the findings of this study.
- Without adjusting its CO2 setting, the DCV system supplies low ventilation rates, resulting in significant POI increases within the school. However, adjusting the DCV set point from 1000 ppm to 600 ppm results in a significant POI reduction from 0.93 to 0.057, with a 50% increase in the total cooling energy needs.
- MV can reduce the POI to 0.051 when operating with a higher ventilation rate of 2 ACH, double the required rate by the ASHRAE standard 60.2 for schools. The DCV can lower the POI to 0.057 when operating with a 600 ppm set point and delivering a ventilation rate of 4 ACH. In this case, MV consumes 617 kWh/day while DCV needs 743 kWh/day.
- An optimal ventilation rate of 2 ACH and social distance of 2 m are recommended to deliver acceptable levels of POI, cooling energy use, and indoor CO2 concentration. These optimal settings would limit the POI to 0.036 while achieving the lowest cooling energy use of 583 kWh/day for the school.
- Increasing the ventilation rate is more effective in reducing the POI than increasing the social distancing. However, the reduction in POI occurs with an increase in cooling energy use when the ventilation rate is increased. For instance, increasing the social distance from 1 m to 2 m would lower the POI by 28%, while reducing the cooling energy need by 7%. On the other hand, increasing the ventilation rate from 1 ACH to 2 ACH would lower the POI by 49%, while increasing the cooling energy demand by 25%.
- The POI remains between 0.036 and 0.13 when operating with a 2 ACH ventilation rate and 2 m social distancing even if the number of infectors is increased from 1 to 5.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Berry, G.; Parsons, A.; Morgan, M.; Rickert, J.; Cho, H. A review of methods to reduce the probability of the airborne spread of COVID-19 in ventilation systems and enclosed spaces. Environ. Res. 2022, 203, 111765. [Google Scholar] [CrossRef]
- Schumacher, S.; Banda Sanchez, A.; Caspari, A.; Staack, K.; Asbach, C. Testing Filter-Based Air Cleaners with Surrogate Particles for Viruses and Exhaled Droplets. Atmosphere 2022, 13, 1538. [Google Scholar] [CrossRef]
- Miller, S.L.; Nazaroff, W.W.; Jimenez, J.L.; Boerstra, A.; Buonanno, G.; Dancer, S.J.; Kurnitski, J.; Marr, L.C.; Morawska, L.; Noakes, C. Transmission of SARS-CoV-2 by inhalation of respiratory aerosol in the Skagit Valley Chorale superspreading event. Indoor Air 2021, 31, 314–323. [Google Scholar] [CrossRef]
- Bisag, A.; Isabelli, P.; Laurita, R.; Bucci, C.; Capelli, F.; Dirani, G.; Gherardi, M.; Laghi, G.; Paglianti, A.; Sambri, V.; et al. Cold atmospheric plasma inactivation of aerosolized microdroplets containing bacteria and purified SARS-CoV-2 RNA to contrast airborne indoor transmission. Plasma Process. Polym. 2020, 17, 2000154. [Google Scholar] [CrossRef]
- World Health Organization. Infection Prevention and Control during Health Care When COVID-19 Is Suspected; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- ASHRAE ANSI/ASHRAE Standard 170-2017; Ventilation of Health Care Facilities. American Society of Heating, Refrigerating and Air-Conditioning Engineers, Inc.: Atlanta, GA, USA, 2017.
- Chen, C.Y.; Chen, P.H.; Chen, J.K.; Su, T.C. Recommendations for ventilation of indoor spaces to reduce COVID-19 transmission. J. Formos. Med. Assoc. 2021, 120, 2055–2060. [Google Scholar] [CrossRef]
- Aganovic, A.; Bi, Y.; Cao, G.; Drangsholt, F.; Kurnitski, J.; Wargocki, P. Estimating the impact of indoor relative humidity on SARS-CoV-2 airborne transmission risk using a new modification of the Wells-Riley model. Build. Environ. 2021, 205, 108278. [Google Scholar] [CrossRef]
- Dai, H.; Zhao, B. Association of infected probability of COVID-19 with ventilation rates in confined spaces: A Wells-Riley equation based investigation. Build. Simul. 2020, 13, 1321–1327. [Google Scholar] [CrossRef]
- Riley, E.; Murphy, G.; Riley, R. Airborne spread of measles in a suburban elementary school. Am. J. Epidemiol. 1978, 107, 421–432. [Google Scholar] [CrossRef] [PubMed]
- Gammaitoni, L.; Nucci, M.C. Using a mathematical model to evaluate the efficacy of TB control measures. Emerg. Infect. Dis. 1997, 3, 335–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, C.; Zhai, Z. The efficacy of social distance and ventilation effectiveness in preventing COVID-19 transmission. Sustain. Cities Soc. 2020, 62, 102390. [Google Scholar] [CrossRef] [PubMed]
- Sha, H.; Zhang, X.; Qi, D. Optimal control of high-rise building mechanical ventilation system for achieving low risk of COVID-19 transmission and ventilative cooling. Sustain. Cities Soc. 2021, 74, 103256. [Google Scholar] [CrossRef]
- Tang, H.; Pan, Z.; Li, C. Tempo-spatial infection risk assessment of airborne virus via CO2 concentration field monitoring in built environment. Build. Environ. 2022, 217, 109067. [Google Scholar] [CrossRef]
- Li, C.; Tang, H. Study on ventilation rates and assessment of infection risks of COVID-19 in an outpatient building. J. Build. Eng. 2021, 42, 103090. [Google Scholar] [CrossRef]
- Ai, Z.; Mak, C.; Gao, N.; Niu, J. Tracergasisasuitablesurrogateofexhaleddroplet nuclei for studying airborne transmission in the built environment. Build. Simul. 2020, 13, 489–496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, Y.; Li, Y.; Lin, M.; Liu, L.; Lin, B.; Zhou, H.; Lin, J.; Xu, H. Environmentalmonitoring and infection control of fever clinics in general hospitals during COVID-19 pandemic. Chin. Sci. Bull. 2020, 66, 475–485. [Google Scholar] [CrossRef]
- Kappelt, N.; Russell, H.S.; Kwiatkowski, S.; Afshari, A.; Johnson, M.S. Correlation of respiratory aerosols and metabolic carbon dioxide. Sustainability 2021, 13, 2203. [Google Scholar] [CrossRef]
- Schade, W.; Reimer, V.; Seipenbusch, M.; Willer, U. Experimental investigation of aerosol and CO2 dispersion for evaluation of COVID-19 infection risk in a concert hall. Int. J. Environ. Res. Public Health 2021, 18, 3037. [Google Scholar] [CrossRef] [PubMed]
- Rudnick, S.N.; Milton, D.K. Risk of indoor airborne infection transmission estimated from carbon dioxide concentration. Indoor Air 2003, 13, 237–245. [Google Scholar] [CrossRef]
- Cammarata, A.; Cammarata, G. Dynamic assessment of the risk of airborne viral infection. Indoor Air 2021, 31, 1759–1775. [Google Scholar] [CrossRef] [PubMed]
- Peng, Z.; Jimenez, J.L. Exhaled CO2 as a COVID-19 Infection Risk Proxy for Different Indoor Environments and Activities. Environ. Sci. Technol. Lett. 2021, 8, 392–397. [Google Scholar] [CrossRef]
- Stabile, L.; Pacitto, A.; Mikszewski, A.; Morawska, L.; Buonanno, G. Ventilation procedures to minimize the airborne transmission of viruses in classrooms. Build. Environ. 2021, 202, 108042. [Google Scholar] [CrossRef]
- Nair, A.N.; Anand, P.; George, A.; Mondal, N. A review of strategies and their effectiveness in reducing indoor airborne transmission and improving indoor air quality. Environ. Res. 2022, 213, 113579. [Google Scholar] [CrossRef]
- Afshari, A.; Hultmark, G.; Nielsen, P.V.; Maccarini, A. Ventilation System Design and the Coronavirus (COVID-19). Front. Built Environ. 2021, 7, 662489. [Google Scholar] [CrossRef]
- Eykelbosh, A. Indoor CO2 Sensors for COVID-19 Risk Mitigation: Current Guidance and Limitations; National Collaborating Centre for Environmental Health: Vancouver, BC, Canada, 2021; pp. 1–16. [Google Scholar]
- Yun, H.; Yang, J.; Seo, J.H.; Sohn, J.R. Methodology for sampling and detection of airborne coronavirus including SARS-CoV-2. Indoor Built Environ. 2022, 31, 1234–1241. [Google Scholar] [CrossRef]
- Bhardwaj, J.; Hong, S.; Jang, J.; Han, C.H.; Lee, J.; Jang, J. Recent advancements in the measurement of pathogenic airborne viruses. J. Hazard. Mater. 2021, 420, 126574. [Google Scholar] [CrossRef]
- Wang, J.; Huang, J.; Feng, Z.; Cao, S.J.; Haghighat, F. Occupant-density-detection based energy efficient ventilation system: Prevention of infection transmission. Energy Build. 2021, 240, 110883. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Cai, W. A novel CO2-based demand-controlled ventilation strategy to limit the spread of COVID-19 in the indoor environment. Build. Environ. 2022, 219, 109232. [Google Scholar] [CrossRef]
- Giampieri, A.; Ma, Z.; Ling-Chin, J.; Roskilly, A.P.; Smallbone, A.J. An overview of solutions for airborne viral transmission reduction related to HVAC systems including liquid desiccant air-scrubbing. Energy 2022, 244, 122709. [Google Scholar] [CrossRef]
- Schibuola, L.; Tambani, C. High energy efficiency ventilation to limit COVID-19 contagion in school environments. Energy Build. 2021, 240, 110882. [Google Scholar] [CrossRef] [PubMed]
- Alaidroos, A.; Almaimani, A.; Krarti, M.; Dahlan, A.; Maddah, R. Evaluation of the performance of demand control ventilation system for school buildings located in the hot climate of Saudi Arabia. Build. Simul. 2021, 15, 1067–1082. [Google Scholar] [CrossRef]
- Yan, S.; Wang, L.L.; Birnkrant, M.J.; Zhai, J.; Miller, S.L. Evaluating SARS-CoV-2 airborne quanta transmission and exposure risk in a mechanically ventilated multizone office building. Build. Environ. 2022, 219, 109184. [Google Scholar] [CrossRef] [PubMed]
- Alaidroos, A.; Almaimani, A.; Baik, A.; Al-Amodi, M.; Rahaman, K.R. Are historical buildings more adaptive to minimize the risks of airborne transmission of viruses and public health? A study of the hazzazi house in Jeddah (Saudi Arabia). Int. J. Environ. Res. Public Health 2021, 18, 3601. [Google Scholar] [CrossRef] [PubMed]
- Fageha, M.K.; Alaidroos, A. Performance Optimization of Natural Ventilation in Classrooms to Minimize the Probability of Viral Infection and Reduce Draught Risk. Sustainability 2022, 14, 4966. [Google Scholar] [CrossRef]
- Ministry of Municipal and Rural Affairs—KSA School’s Construction Requirements in KSA. 2019. Available online: http://tbc.sa:88/Etemad/municipalstipulations.pdf (accessed on 23 June 2021).
- Saudi Mechanical Code (SBC 501); Saudi Building Code National Committee: 2018, Riyadh, Kingdom of Saudi Arabia. Available online: https://da74f184-7160-42c1-9ed7-8f3b0ea674e6.filesusr.com/ugd/4069ce_936b663780c64fa7bf0e7e0ac4cc5d7f.pdf?index=true (accessed on 15 February 2023).
- ASHRAE Standard 62.1-2019; Ventilation for Acceptable Indoor Air Quality. American Society of Heating, Refrigerating and Air-Conditioning Engineers, Inc.: Atlanta, GA, USA, 2019.
- Li, Y.; Qian, H.; Hang, J.; Chen, X.; Cheng, P.; Ling, H.; Wang, S.; Liang, P.; Li, J.; Xiao, S.; et al. Probable airborne transmission of SARS-CoV-2 in a poorly ventilated restaurant. Build. Environ. 2021, 196, 107788. [Google Scholar] [CrossRef] [PubMed]
- Hijnen, D.; GeurtsvanKessel, C.; Marzano, A.V.; Eyerich, K.; Gim nez-Arnau, A.M.; Joly, P.; Vestergaard, C.; Sticherling, M.; Schmidt, E.; Lee, V.J. SARS-CoV-2 transmission from presymptomatic meeting attendee, Germany. Emerg. Infect. Dis. 2020, 26, 1935–1937. [Google Scholar] [CrossRef]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Floors | 2 |
| Gross Floor Area | 3123 m2 |
| Wall Construction | 2 cm plaster outside + 20 cm concrete hollow block + 5 cm expanded polystyrene + 2 cm plaster inside |
| Roof Construction | 1 cm built-up roofing + 20 cm concrete roof slab + 5 cm expanded polystyrene + 1.5 cm plaster inside |
| Window-to-Wall Ratio | 20% |
| Glazing Type | Double Clear with PVC framing |
| Air Infiltration | 0.7 ACH |
| Number of Students per Area in classrooms | 0.5/m2 |
| Lighting Power Density | 5 W/m2 |
| Equipment Power Density | 4.7 W/m2 |
| HVAC System | DX Packaged Air Handling Unit |
| Cooling Set Point | 23 °C |
| Ventilation System | Mechanical ventilation with fixed outdoor air fraction (15%) |
| Energy Efficiency Ratio (EER) | 8.5 |
| Case | Case Date | Place Type | Total Occupants | Primary Infected Cases | Secondary Infected Cases | V (m3) | n (ACH) | t (h) | p (m3/h) | q (quanta/h) |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 24 January 2020 | Restaurant | 21 | 1 | 9 | 127 | 0.6 | 1.25 | 1.1 | 42.1 |
| 2 | 20 February 2020 | Meeting room | 14 | 1 | ≥11 | 189 | 0.2 | 9.5 | 1.1 | 42.1 |
| 3 | 10 March 2020 | Choir hall | 61 | 1 | 33–53 | 810 | 0.35–1.05 | 2.5 | 1.1 | 195.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almaimani, A.; Alaidroos, A.; Krarti, M.; Qurnfulah, E.; Tiwari, A. Evaluation of Optimal Mechanical Ventilation Strategies for Schools for Reducing Risks of Airborne Viral Infection. Buildings 2023, 13, 871. https://doi.org/10.3390/buildings13040871
Almaimani A, Alaidroos A, Krarti M, Qurnfulah E, Tiwari A. Evaluation of Optimal Mechanical Ventilation Strategies for Schools for Reducing Risks of Airborne Viral Infection. Buildings. 2023; 13(4):871. https://doi.org/10.3390/buildings13040871
Chicago/Turabian StyleAlmaimani, Ayad, Alaa Alaidroos, Moncef Krarti, Emad Qurnfulah, and Alok Tiwari. 2023. "Evaluation of Optimal Mechanical Ventilation Strategies for Schools for Reducing Risks of Airborne Viral Infection" Buildings 13, no. 4: 871. https://doi.org/10.3390/buildings13040871