
Blood Flow Restriction Is Not Useful as Soccer Competition Recovery in Youth Male National-Level Soccer Players: A Crossover Randomised Controlled Trial



Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Testing
2.3.1. Countermovement Jump (CMJ) Test
2.3.2. Rating of Perceived Exertion (RPE)
2.3.3. Wellness Questionnaire (WQ)
2.4. Interventions
2.4.1. BFR Active Recovery Session (BFR Condition)
2.4.2. No-BFR Active Recovery Session (NoBFR Condition)
2.5. Statistical Analyses
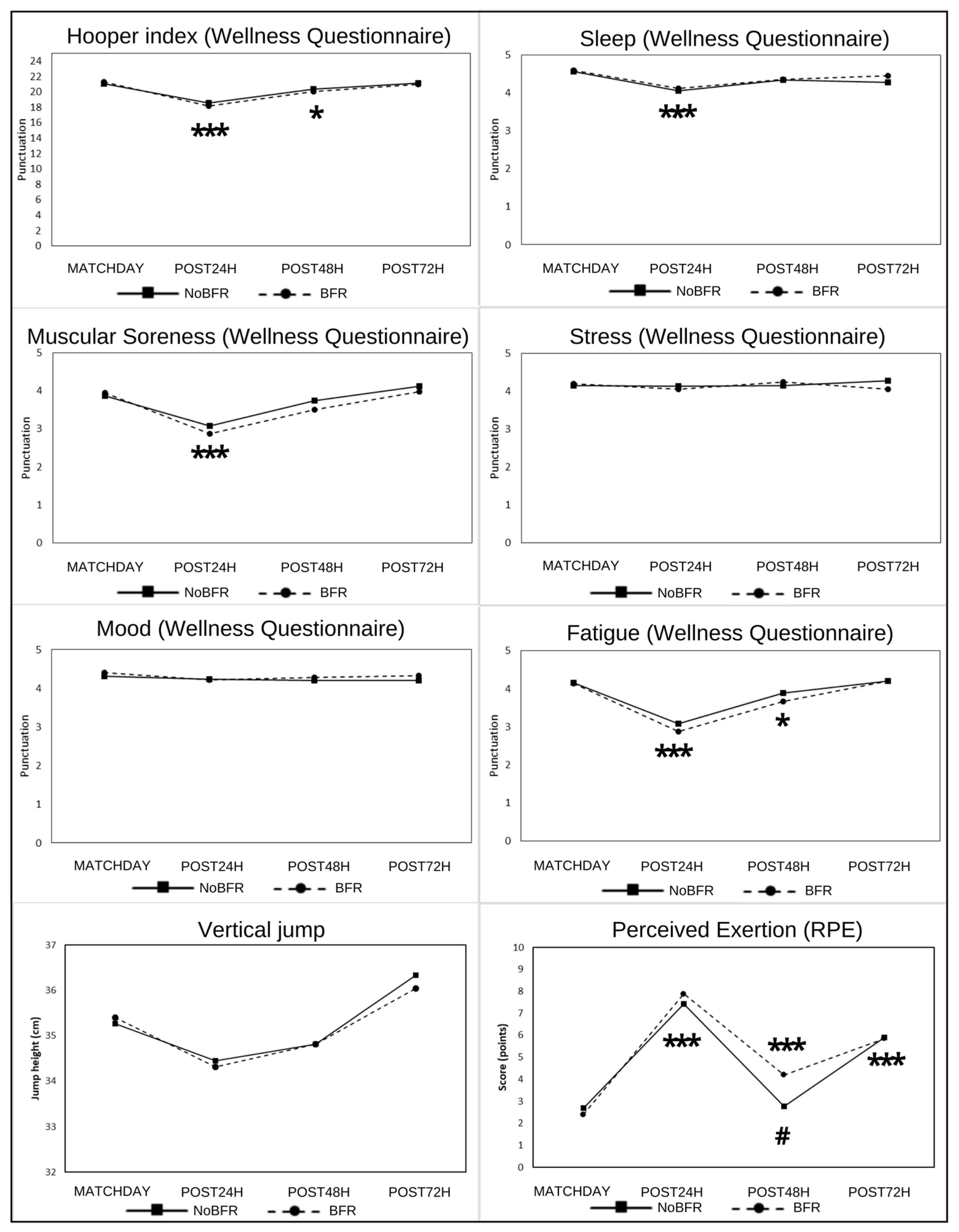
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Julian, R.; Page, R.M.; Harper, L.D. The Effect of Fixture Congestion on Performance During Professional Male Soccer Match-Play: A Systematic Critical Review with Meta-Analysis. Sport. Med. 2021, 51, 255–273. [Google Scholar] [CrossRef] [PubMed]
- Carling, C.; Dupont, G. Are declines in physical performance associated with a reduction in skill-related performance during professional soccer match-play? J. Sport. Sci. 2011, 29, 63–71. [Google Scholar] [CrossRef]
- Dellal, A.; Lago-Peñas, C.; Rey, E.; Chamari, K.; Orhant, E. The effects of a congested fixture period on physical performance, technical activity and injury rate during matches in a professional soccer team. Br. J. Sport. Med. 2015, 49, 390–394. [Google Scholar] [CrossRef]
- Calleja-González, J.; Mielgo-Ayuso, J.; Miguel-Ortega, Á.; Marqués-Jiménez, D.; Del Valle, M.; Ostojic, S.M.; Sampaio, J.; Terrados, N.; Refoyo, I. Post-exercise Recovery Methods Focus on Young Soccer Players: A Systematic Review. Front. Physiol. 2021, 12, 505149. [Google Scholar] [CrossRef]
- Rey, E.; Lago-Peñas, C.; Casáis, L.; Lago-Ballesteros, J. The effect of immediate post-training active and passive recovery interventions on anaerobic performance and lower limb flexibility in professional soccer players. J. Hum. Kinet. 2012, 31, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Castillo, D.; Raya-González, J.; Sarmento, H.; Clemente, F.M.; Yanci, J. Effects of including endurance and speed sessions within small-sided soccer games periodization on physical fitness. Biol. Sport 2021, 38, 291–299. [Google Scholar] [CrossRef] [PubMed]
- Arriel, R.A.; Rodrigues, J.F.; de Souza, H.L.R.; Meireles, A.; Leitão, L.F.M.; Crisafulli, A.; Marocolo, M. Ischemia–reperfusion intervention: From enhancements in exercise performance to accelerated performance recovery—A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2020, 17, 8161. [Google Scholar] [CrossRef]
- Scott, B.R.; Loenneke, J.P.; Slattery, K.M.; Dascombe, B.J. Blood flow restricted exercise for athletes: A review of available evidence. J. Sci. Med. Sport 2016, 19, 360–367. [Google Scholar] [CrossRef]
- Krzysztofik, M.; Wilk, M.; Wojdała, G.; Gołaś, A. Maximizing muscle hypertrophy: A systematic review of advanced resistance training techniques and methods. Int. J. Environ. Res. Public Health 2019, 16, 4897. [Google Scholar] [CrossRef]
- Borne, R.; Hausswirth, C.; Bieuzen, F. Relationship Between Blood Flow and Performance Recovery: A Randomized, Placebo-Controlled Study. Int. J. Sport. Physiol. Perform. 2017, 12, 152–160. [Google Scholar] [CrossRef]
- Altarriba-Bartes, A.; Peña, J.; Vicens-Bordas, J.; Milà-Villaroel, R.; Calleja-González, J. Post-competition recovery strategies in elite male soccer players. Effects on performance: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0240135. [Google Scholar] [CrossRef] [PubMed]
- Pignanelli, C.; Christiansen, D.; Burr, J.F. Blood flow restriction training and the high-performance athlete: Science to application. J. Appl. Physiol. 2021, 130, 1163–1170. [Google Scholar] [CrossRef] [PubMed]
- Daab, W.; Bouzid, M.A.; Lajri, M.; Bouchiba, M.; Rebai, H. Brief cycles of lower-limb occlusion accelerate recovery kinetics in soccer players. Phys. Sportsmed. 2021, 49, 143–150. [Google Scholar] [CrossRef]
- Patterson, S.D.; Swan, R.; Page, W.; Marocolo, M.; Jeffries, O.; Waldron, M. The effect of acute and repeated ischemic preconditioning on recovery following exercise-induced muscle damage. J. Sci. Med. Sport 2021, 24, 709–714. [Google Scholar] [CrossRef] [PubMed]
- Gibson, N.; Mahony, B.; Tracey, C.; Fawkner, S.; Murray, A. Effect of ischemic preconditioning on repeated sprint ability in team sport athletes. J. Sport. Sci. 2015, 33, 1182–1188. [Google Scholar] [CrossRef]
- Jeffries, O.; Waldron, M.; Pattison, J.R.; Patterson, S.D. Enhanced Local Skeletal Muscle Oxidative Capacity and Microvascular Blood Flow Following 7-Day Ischemic Preconditioning in Healthy Humans. Front. Physiol. 2018, 9, 463. [Google Scholar] [CrossRef]
- Aktaş, E.; Atay, Ç.; Deveci, M.A.; Arikan, M.; Toğral, G.; Yildirim, A. Impact of oxidative stress on early postoperative knee function and muscle injury biochemical markers: Is it possible to create an ischemic preconditioning effect in sequential ischemic surgical procedures? Acta Orthop. Traumatol. Turc. 2015, 49, 387–393. [Google Scholar] [CrossRef]
- Liu, G.S.; Richards, S.C.; Olsson, R.A.; Mullane, K.; Walsh, R.S.; Downey, J.M. Evidence that the adenosine A3 receptor may mediate the protection afforded by preconditioning in the isolated rabbit heart. Cardiovasc. Res. 1994, 28, 1057–1061. [Google Scholar] [CrossRef]
- Konstantinov, I.E.; Arab, S.; Kharbanda, R.K.; Li, J.; Cheung, M.M.H.; Cherepanov, V.; Downey, G.P.; Liu, P.P.; Cukerman, E.; Coles, J.G.; et al. The remote ischemic preconditioning stimulus modifies inflammatory gene expression in humans. Physiol. Genom. 2004, 19, 143–150. [Google Scholar] [CrossRef]
- Fernandez-Fernandez, J.; Sanz, D.; Sarabia, J.M.; Moya, M. The effects of sport-specific drills training or high-intensity interval training in young tennis players. Int. J. Sport. Physiol. Perform. 2017, 12, 90–98. [Google Scholar] [CrossRef]
- Alba-Jiménez, C.; Moreno-Doutres, D.; Peña, J. Trends Assessing Neuromuscular Fatigue in Team Sports: A Narrative Review. Sports 2022, 10, 33. [Google Scholar] [CrossRef] [PubMed]
- Bishop, C.; Turner, A.; Jordan, M.; Harry, J.; Loturco, I.; Lake, J.; Comfort, P. A Framework to Guide Practitioners for Selecting Metrics during the Countermovement and Drop Jump Tests. Strength Cond. J. 2022, 44, 95–103. [Google Scholar] [CrossRef]
- Nuhu, A.; Jelsma, J.; Dunleavy, K.; Burgess, T. Effect of the FIFA 11+ soccer specific warm up programme on the incidence of injuries: A cluster-randomised controlled trial. PLoS ONE 2021, 16, e0251839. [Google Scholar] [CrossRef] [PubMed]
- Anagnost, N.G.; Lates, A.; Taber, C. Validity of a Wireless Inertia Measurement Device in Quantifying Performance in Vertical Jumping Tests. In Proceedings of the 13th Annual Coaching and Sport Science College Conference, East Tennessee State University, Johnson City, TN; 2018. Available online: https://www.sportscienceed.com/2018-archive.html (accessed on 12 September 2022).
- Merrigan, J.J.; Stone, J.D.; Hornsby, W.G.; Hagen, J.A. Identifying Reliable and Relatable Force–Time Metrics in Athletes—Considerations for the Isometric Mid-Thigh Pull and Countermovement Jump. Sports 2021, 9, 4. [Google Scholar] [CrossRef]
- Ritchie, C. Rating of Perceived Exertion (RPE). J. Physiother. 2012, 58, 62. [Google Scholar] [CrossRef]
- Impellizzeri, F.M.; Rampinini, E.; Coutts, A.J.; Sassi, A.; Marcora, S.M. Use of RPE-based training load in soccer. Med. Sci. Sport. Exerc. 2004, 36, 1042–1047. [Google Scholar] [CrossRef]
- Mcguigan, M.R.; Foster, C. A New Approach to Monitoring Resistance Training. Natl. Strength Cond. Assoc. 2004, 26, 42–47. [Google Scholar] [CrossRef]
- Fessi, M.S.; Nouira, S.; Dellal, A.; Owen, A.; Elloumi, M.; Moalla, W. Changes of the psychophysical state and feeling of wellness of professional soccer players during pre-season and in-season periods. Res. Sport. Med. 2016, 24, 375–386. [Google Scholar] [CrossRef]
- Mclean, B.D.; Coutts, A.J.; Kelly, V.; Mcguigan, M.R.; Cormack, S.J. Neuromuscular, Endocrine, and Perceptual Fatigue Responses During Different Length Between-Match Microcycles in Professional Rugby League Players. Int. J. Sport. Physiol. Perform. 2010, 5, 367–383. [Google Scholar] [CrossRef]
- Hooper, S.L.; Mackinnon, L.T. Monitoring overtraining in athletes. Recommendations. Sport. Med. 1995, 20, 321–327. [Google Scholar] [CrossRef]
- Campos Vázquez, M.Á.; Toscano Bendala, F.J. Monitorización de la carga de entrenamiento, la condición física, la fatiga y el rendimiento durante el microciclo competitivo en fútbol. Rev. Prep. Física Fútbol 2014, 12, 23–36. [Google Scholar]
- Deely, C.; Tallent, J.; Bennett, R.; Woodhead, A.; Goodall, S.; Thomas, K.; Howatson, G. Etiology and Recovery of Neuromuscular Function Following Academy Soccer Training. Front. Physiol. 2022, 13, 1170. [Google Scholar] [CrossRef] [PubMed]
- Loenneke, J.P.; Allen, K.M.; Mouser, J.G.; Thiebaud, R.S.; Kim, D.; Abe, T.; Bemben, M.G. Blood flow restriction in the upper and lower limbs is predicted by limb circumference and systolic blood pressure. Eur. J. Appl. Physiol. 2015, 115, 397–405. [Google Scholar] [CrossRef] [PubMed]
- Kakhak, S.A.H.; Kianigul, M.; Haghighi, A.-H.; Nooghabi, M.J.; Scott, B.R. Performing Soccer-Specific Training with Blood Flow Restriction Enhances Physical Capacities in Youth Soccer Players. J. Strength Cond. Res. 2022, 36, 1972–1977. [Google Scholar] [CrossRef]
- Held, S.; Behringer, M.; Donath, L. Low intensity rowing with blood flow restriction over 5 weeks increases VO2max in elite rowers: A randomized controlled trial. J. Sci. Med. Sport 2020, 23, 304–308. [Google Scholar] [CrossRef]
- Kilgas, M.A.; Yoon, T.; McDaniel, J.; Phillips, K.C.; Elmer, S.J. Physiological Responses to Acute Cycling With Blood Flow Restriction. Front. Physiol. 2022, 13, 409. [Google Scholar] [CrossRef]
- Loenneke, J.P.; Thrower, A.D.; Balapur, A.; Barnes, J.T.; Pujol, T.J. The energy requirement of walking with restricted blood flow. Sport Sci. 2011, 4, 7–11. [Google Scholar]
- Jankowski, M.P.; Rau, K.K.; Ekmann, K.M.; Anderson, C.E.; Koerber, H.R. Comprehensive phenotyping of group III and IV muscle afferents in mouse. J. Neurophysiol. 2013, 109, 2374. [Google Scholar] [CrossRef]
- Willis, S.J.; Alvarez, L.; Borrani, F.; Millet, G.P. Oxygenation time course and neuromuscular fatigue during repeated cycling sprints with bilateral blood flow restriction. Physiol. Rep. 2018, 6, e13872. [Google Scholar] [CrossRef]
- Clarkson, M.J.; May, A.K.; Warmington, S.A. Is there rationale for the cuff pressures prescribed for blood flow restriction exercise? A systematic review. Scand. J. Med. Sci. Sport. 2020, 30, 1318–1336. [Google Scholar] [CrossRef]
- Williams, N.; Russell, M.; Cook, C.J.; Kilduff, L.P. The effect of lower limb occlusion on recovery following sprint exercise in academy rugby players. J. Sci. Med. Sport 2018, 21, 1095–1099. [Google Scholar] [CrossRef]
- Marynowicz, J.; Kikut, K.; Lango, M.; Horna, D.; Andrzejewski, M. Relationship between the session-RPE and external measures of training load in youth soccer training. J. Strength Cond. Res. 2020, 34, 2800–2804. [Google Scholar] [CrossRef]
- Fekri-Kurabbaslou, V.; Shams, S.; Amani-Shalamzari, S. Effect of different recovery modes during resistance training with blood flow restriction on hormonal levels and performance in young men: A randomized controlled trial. BMC Sports Sci. Med. Rehabil. 2022, 14, 47. [Google Scholar] [CrossRef]
- Page, W.; Swan, R.; Patterson, S.D. The effect of intermittent lower limb occlusion on recovery following exercise-induced muscle damage: A randomized controlled trial. J. Sci. Med. Sport 2017, 20, 729–733. [Google Scholar] [CrossRef]
- Northey, J.M.; Rattray, B.; Argus, C.K.; Etxebarria, N.; Driller, M.W. Vascular Occlusion and Sequential Compression for Recovery after Resistance Exercise. J. Strength Cond. Res. 2016, 30, 533–539. [Google Scholar] [CrossRef]
- Nedelec, M.; McCall, A.; Carling, C.; Legall, F.; Berthoin, S.; Dupont, G. The influence of soccer playing actions on the recovery kinetics after a soccer match. J. Strength Cond. Res. 2014, 28, 1517–1523. [Google Scholar] [CrossRef]
- Souza-Silva, E.; Christensen, S.W.; Hirata, R.P.; Larsen, R.G.; Graven-Nielsen, T. Blood flow after contraction and cuff occlusion is reduced in subjects with muscle soreness after eccentric exercise. Scand. J. Med. Sci. Sport. 2018, 28, 29–39. [Google Scholar] [CrossRef]
- Alderton, W.K.; Cooper, C.E.; Knowles, R.G. Nitric oxide synthases: Structure, function and inhibition. Biochem. J. 2001, 357, 593. [Google Scholar] [CrossRef] [PubMed]
- Hughes, L.; Paton, B.; Rosenblatt, B.; Gissane, C.; Patterson, S.D. Blood flow restriction training in clinical musculoskeletal rehabilitation: A systematic review and meta-analysis. Br. J. Sport. Med. 2017, 51, 1003–1011. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Kubota, A.; Nozu, S.; Ozaki, H.; Kishimoto, K.; Nishio, H.; Takazawa, Y. Effect of low-intensity exercise with blood flow restriction during rest intervals on muscle function and perception. Clin. Physiol. Funct. Imaging 2022, 42, 348–355. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| BFR | NoBFR | Between-Group Differences | ||
|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (95% CI) | ES (d) | |
| CMJ (cm) | ||||
| Pre24h | 35.39 (3.62) | 35.27 (3.06) | 0.13 (−1.21–1.62) | NS |
| PostMatch | 34.31 (4.01) | 34.45 (4.10) | 0.14 (−1.66–1.80) | NS |
| Post24h | 34.81 (4.15) | 34.81 (3.40) | 0.01 (−1.70–1.71) | NS |
| Post72h | 36.03 (4.29) | 36.33 (3.30) | 0.30 (−1.38–1.96) | NS |
| RPE (0–10 scale) | ||||
| Pre24h | 2.40 (1.00) | 2.69 (1.28) | 0.29 (−0.20–0.80) | NS |
| PostMatch | 7.87 (2.04) | 7.41 (2.11) | 0.46 (−0.40–1.36) | NS |
| Post24h | 4.20 (2.11) | 2.76 (1.73) | 1.43 (0.56–2.30) ** | 0.8 |
| Post72h | 5.90 (2.1) | 5.90 (1.8) | 0.05 (−0.85–0.94) | NS |
| Hooper index (5–25 points) | ||||
| MatchDay | 21.30 (3.08) | 21.05 (2.87) | 0.25 (−1.12–1.56) | NS |
| Post24h | 18.15 (2.76) | 18.56 (2.88) | 0.41 (−0.85–1.60) | NS |
| Post48h | 20.05 (2.65) | 20.33 (2.65) | 0.28 (−0.91–1.49) | NS |
| Post72h | 21.00 (2.77) | 21.10 (2.86) | 0.10 (−1.11–1.23) | NS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castilla-López, C.; Romero-Franco, N. Blood Flow Restriction Is Not Useful as Soccer Competition Recovery in Youth Male National-Level Soccer Players: A Crossover Randomised Controlled Trial. Sports 2023, 11, 99. https://doi.org/10.3390/sports11050099
Castilla-López C, Romero-Franco N. Blood Flow Restriction Is Not Useful as Soccer Competition Recovery in Youth Male National-Level Soccer Players: A Crossover Randomised Controlled Trial. Sports. 2023; 11(5):99. https://doi.org/10.3390/sports11050099
Chicago/Turabian StyleCastilla-López, Christian, and Natalia Romero-Franco. 2023. "Blood Flow Restriction Is Not Useful as Soccer Competition Recovery in Youth Male National-Level Soccer Players: A Crossover Randomised Controlled Trial" Sports 11, no. 5: 99. https://doi.org/10.3390/sports11050099