Effects of Malocclusion on Maximal Aerobic Capacity and Athletic Performance in Young Sub-Elite Athletes


 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
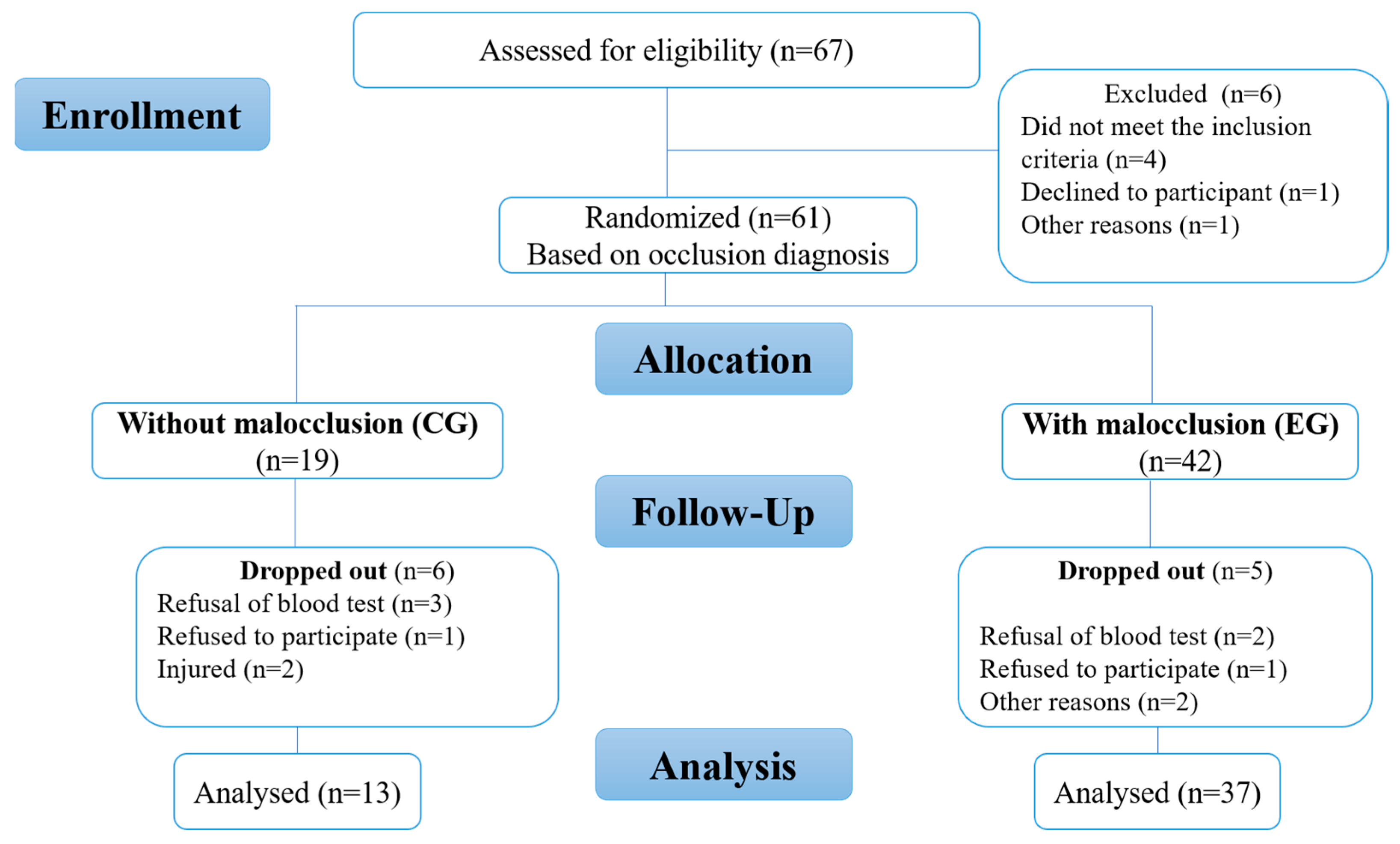
2.1. Study Design
2.2. Inclusion and Exclusion Criteria of Participants
2.3. Procedures
2.4. Maximal Aerobic Capacity
2.5. Blood Pressure and Heart Rate Measurements
2.6. Blood Lactate Measurements
2.7. Statistical Analyses
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Desgorces, F.-D.; Berthelot, G.; Helou, N.E.; Thibault, V.; Guillaume, M.; Tafflet, M.; Hermine, O.; Toussaint, J.-F. From Oxford to Hawaii Ecophysiological Barriers Limit Human Progression in Ten Sport Monuments. PLoS ONE 2008, 3, e3653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, A.G.; Folland, J.P. Similarity of Polygenic Profiles Limits the Potential for Elite Human Physical Performance. J. Physiol. 2008, 586 Pt 1, 113–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isableu, B.; Ohlmann, T.; Cremieux, J.; Amblard, B. Selection of Spatial Frame of Reference and Postural Control Variability. Exp. Brain Res. 1997, 114, 584–589. [Google Scholar] [CrossRef]
- Johnston, R.B.; Howard, M.E.; Cawley, P.W.; Losse, G.M. Effect of Lower Extremity Muscular Fatigue on Motor Control Performance. Med. Sci. Sport Exerc. 1998, 30, 1703–1707. [Google Scholar] [CrossRef] [PubMed]
- Lamendin, H.; Guendouz, B. Sante Bucco-Dentaire et Performances Sportives. Médecine D’afrique Noire 1990, 37, 680–682. [Google Scholar]
- Picart, P. Occlusion Dentaire, Posture et Performances Sportives. Ph.D. Thesis, Université de Lorraine, Lorraine, France, 2015; p. 116. [Google Scholar]
- Baldini, A.; Beraldi, A.; Nota, A.; Danelon, F.; Ballanti, F.; Longoni, S. Gnathological Postural Treatment in a Professional Basketball Player: A Case Report and an Overview of the Role of Dental Occlusion on Performance. Ann. Stomatol. 2012, 3, 51–58. [Google Scholar]
- Golomer, E.; Crémieux, J.; Dupui, P.; Isableu, B.; Ohlmann, T. Visual Contribution to Self-Induced Body Sway Frequencies and Visual Perception of Male Professional Dancers. Neurosci. Lett. 1999, 267, 189–192. [Google Scholar] [CrossRef]
- Vuillerme, N.; Danion, F.; Forestier, N.; Nougier, V. Postural Sway under Muscle Vibration and Muscle Fatigue in Humans. Neurosci. Lett. 2002, 333, 131–135. [Google Scholar] [CrossRef]
- Cabrera-Domínguez, M.E.; Domínguez-Reyes, A.; Pabón-Carrasco, M.; Pérez-Belloso, A.J.; Coheña-Jiménez, M.; Galán-González, A.F. Dental Malocclusion and Its Relation to the Podal System. Front. Pediatr. 2021, 9, 654229. [Google Scholar] [CrossRef]
- Sport et Santé Bucco-Dentaire—2011. Available online: https://docplayer.fr/9579536-Sport-et-sante-bucco-dentaire.html (accessed on 30 July 2021).
- Asgari, I.; Soltani, S.; Sadeghi, S.M. Effects of Iron Products on Decay, Tooth Microhardness, and Dental Discoloration: A Systematic Review. Arch. Pharm. Pract. 2020, 11, 60–82. [Google Scholar]
- Alamri, A.M.; Alshammery, H.M.; Almughamis, M.A.; Alissa, A.S.; Almadhi, W.H.; Alsharif, A.M. Dental Recession Aetiology, Classification and Management. Arch. Pharm. Pract. 2019, 10, 28–31. [Google Scholar]
- Kharalampos, M. Comprehensive Patient Rehabilitation While Performing Immediate Dental Implant Placement with the Use of Information-Wave Therapy (Literature Overview). J. Adv. Pharm. Educ. Res. 2020, 10, 11–14. [Google Scholar]
- Bulgakova, A.I.; Vasilyeva, N.A.; Vasilyev, E.A. The Clinical and Immunological Rationale for the Use of Prolonged Action Dental Ointment in Periodontology. J. Adv. Pharm. Educ. Res. 2019, 9, 65–69. [Google Scholar]
- Rodríguez, S.G.; Rodríguez, M.L.; Ramos, L.P. Modifications of the dental occlusion and its relation with the body posture in Orthodontics. Bibliographic review. Rev. Habanera De Cienc. Médicas 2017, 16, 371–386. [Google Scholar]
- Scharnweber, B.; Adjami, F.; Schuster, G.; Kopp, S.; Natrup, J.; Erbe, C.; Ohlendorf, D. Influence of Dental Occlusion on Postural Control and Plantar Pressure Distribution. Cranio 2017, 35, 358–366. [Google Scholar] [CrossRef] [PubMed]
- Leroux, E.; Leroux, S.; Maton, F.; Ravalec, X.; Sorel, O. Influence of Dental Occlusion on the Athletic Performance of Young Elite Rowers: A Pilot Study. Clinics 2018, 73, e453. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, M.; Kikutani, T.; Okada, G.; Kawamura, T.; Kimura, M.; Akagawa, Y. The Effect of Tooth Loss on Body Balance Control among Community-Dwelling Elderly Persons. Int. J. Prosthodont. 2009, 22, 136–139. [Google Scholar]
- Hoppe, C.B.; Oliveira, J.A.P.; Grecca, F.S.; Haas, A.N.; Gomes, M.S. Association between Chronic Oral Inflammatory Burden and Physical Fitness in Males: A Cross-Sectional Observational Study. Int. Endod. J. 2017, 50, 740–749. [Google Scholar] [CrossRef]
- Sakaguchi, K.; Mehta, N.R.; Abdallah, E.F.; Forgione, A.G.; Hirayama, H.; Kawasaki, T.; Yokoyama, A. Examination of the Relationship between Mandibular Position and Body Posture. Cranio 2007, 25, 237–249. [Google Scholar] [CrossRef]
- Clauzade, M. Orthoposturodontie. Actual. Odonto-Stomatol. 2007, 240, 387–405. [Google Scholar] [CrossRef]
- Alves, D.C.B.; Anjos, V.D.L.D.; Giovannini, J.F.B.G.; Lima, R.P.E.; Mendonça, S.M.S. Odontologia no Esporte: Conhecimento e Hábitos de Atletas do Futebol e Basquetebol Sobre Saúde Bucal. Rev. Bras. Med. Esporte 2017, 23, 407–411. [Google Scholar] [CrossRef] [Green Version]
- D’Ercole, S.; Tieri, M.; Martinelli, D.; Tripodi, D. The Effect of Swimming on Oral Health Status: Competitive versus Non-Competitive Athletes. J. Appl. Oral Sci. 2016, 24, 107–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashley, P.; Iorio, A.D.; Cole, E.; Tanday, A.; Needleman, I. Oral Health of Elite Athletes and Association with Performance: A Systematic Review. Br. J. Sports Med. 2015, 49, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, J.; Ashley, P.; Petrie, A.; Needleman, I. Oral Health and Performance Impacts in Elite and Professional Athletes. Community Dent. Oral Epidemiol. 2018, 46, 563–568. [Google Scholar] [CrossRef] [PubMed]
- Moon, H.-J.; Lee, Y.-K. The Relationship Between Dental Occlusion/Temporomandibular Joint Status and General Body Health: Part 1. Dental Occlusion and TMJ Status Exert an Influence on General Body Health. J. Altern. Complement. Med. 2011, 17, 995–1000. [Google Scholar] [CrossRef] [Green Version]
- Iwasaki, H.; Inaba, R.; Iwata, H. Biting force and physical fitness in athletes. Nihon Eiseigaku Zasshi 1994, 49, 654–659. [Google Scholar] [CrossRef] [Green Version]
- Ohlendorf, D.; Seebach, K.; Hoerzer, S.; Nigg, S.; Kopp, S. The Effects of a Temporarily Manipulated Dental Occlusion on the Position of the Spine: A Comparison during Standing and Walking. Spine J. 2014, 14, 2384–2391. [Google Scholar] [CrossRef]
- Jakush, J. Divergent Views: Can Dental Therapy Enhance Athletic Performance? J. Am. Dent. Assoc. 1982, 104, 292–298. [Google Scholar] [CrossRef]
- Sforza, C.; Tartaglia, G.M.; Solimene, U.; Morgun, V.; Kaspranskiy, R.R.; Ferrario, V.F. Occlusion, Sternocleidomastoid Muscle Activity, and Body Sway: A Pilot Study in Male Astronauts. CRANIO® 2006, 24, 43–49. [Google Scholar] [CrossRef]
- Abduljabbar, T.; Mehta, N.R.; Forgione, A.G.; Clark, R.E.; Kronman, J.H.; Munsat, T.L.; George, P. Effect of Increased Maxillo-Mandibular Relationship on Isometric Strength in TMD Patients with Loss of Vertical Dimension of Occlusion. CRANIO® 1997, 15, 57–67. [Google Scholar] [CrossRef]
- AL-Abbasi, H.; Mehta, N.R.; Forgione, A.G.; Clark, R.E. The Effect of Vertical Dimension and Mandibular Position on Isometric Strength of the Cervical Flexors. CRANIO® 1999, 17, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Santander, H.; Miralles, R.; Jimenez, A.; Zuñiga, C.; Rocabado, M.; Moya, H. Influence of Stabilization Occlusal Splint on Craniocervical Relationships. Part II: Electromyographic Analysis. CRANIO® 1994, 12, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Ceneviz, C.; Mehta, N.R.; Forgione, A.; Sands, M.J.; Abdallah, E.F.; Lobo Lobo, S.; Mavroudi, S. The Immediate Effect of Changing Mandibular Position on the EMG Activity of the Masseter, Temporalis, Sternocleidomastoid, and Trapezius Muscles. CRANIO® 2006, 24, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Takada, Y.; Miyahara, T.; Tanaka, T.; Ohyama, T.; Nakamura, Y. Modulation of H Reflex of Pretibial Muscles and Reciprocal Ia Inhibition of Soleus Muscle During Voluntary Teeth Clenching in Humans. J. Neurophysiol. 2000, 83, 2063–2070. [Google Scholar] [CrossRef] [Green Version]
- Grosdent, S.; O’Thanh, R.; Domken, O.; Lamy, M.; Croisier, J.-L. Dental Occlusion Influences Knee Muscular Performances in Asymptomatic Females. J. Strength Cond. Res. 2014, 28, 492–498. [Google Scholar] [CrossRef] [PubMed]
- Gangloff, P.; Louis, J.P.; Perrin, P.P. Dental Occlusion Modifies Gaze and Posture Stabilization in Human Subjects. Neurosci. Lett. 2000, 293, 203–206. [Google Scholar] [CrossRef] [PubMed]
- Maurer, C.; Stief, F.; Jonas, A.; Kovac, A.; Groneberg, D.A.; Meurer, A.; Ohlendorf, D. Influence of the Lower Jaw Position on the Running Pattern. PLoS ONE 2015, 10, e0135712. [Google Scholar] [CrossRef] [Green Version]
- Budd, S.C.; Egea, J.-C. Dental Occlusion and Athletic Performance. In Sport and Oral Health: A Concise Guide; Springer: Berlin/Heidelberg, Germany, 2017. [Google Scholar] [CrossRef]
- De Souza, J.J.; Grande, R.S.; Bahls, R.; Santos, F.A. Evaluation of the Oral Health Conditions of Volleyball Athletes. Rev. Bras. Med. Esporte 2020, 26, 239–242. [Google Scholar] [CrossRef]
- Kragt, L.; Moen, M.H.; Van Den Hoogenband, C.-R.; Wolvius, E.B. Oral Health among Dutch Elite Athletes Prior to Rio 2016. Phys. Sport 2019, 47, 182–188. [Google Scholar] [CrossRef] [Green Version]
- Needleman, I.; Ashley, P.; Petrie, A.; Fortune, F.; Turner, W.; Jones, J.; Niggli, J.; Engebretsen, L.; Budgett, R.; Donos, N.; et al. Oral Health and Impact on Performance of Athletes Participating in the London 2012 Olympic Games: A Cross-Sectional Study. Br. J. Sports Med. 2013, 47, 1054–1058. [Google Scholar] [CrossRef] [Green Version]
- Do Nascimento, B.L.; Zen, I.R.; Demenech, L.S.; de Oliveira Mazzetto, N.C.; Spada, P.C.P. Knowledge of Triathlon Athletes about the Relationship between Oral Health and Performance. RSBO 2015, 12, 352–355. [Google Scholar]
- Manson, J. Influence de L’occlusion sur les Performances Sportives. Ph.D. Thesis, University of Nantes, Nantes, France, 2010. [Google Scholar]
- De Souza, L.A.; Elmadjian, T.R.; Brito e Dias, R.; Coto, N.P. Prevalence of Malocclusions in the 13–20-Year-Old Categories of Football Athletes. Braz. Oral Res. 2011, 25, 19–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKay, A.K.A.; Stellingwerff, T.; Smith, E.S.; Martin, D.T.; Mujika, I.; Goosey-Tolfrey, V.L.; Sheppard, J.; Burke, L.M. Defining Training and Performance Caliber: A Participant Classification Framework. Int. J. Sport. Physiol. Perform. 2022, 17, 317–331. [Google Scholar] [CrossRef] [PubMed]
- Cazorla, G. 3. Evaluation des capacités aérobies. In Evaluation des Capacites Physiologiques et Physiques; AREAPS: Marrakech, Morocco, 2014; p. 20. [Google Scholar]
- Stergiou, G.S.; Palatini, P.; Asmar, R.; Ioannidis, J.P.; Kollias, A.; Lacy, P.; McManus, R.J.; Myers, M.G.; Parati, G.; Shennan, A.; et al. Recommendations and Practical Guidance for Performing and Reporting Validation Studies According to the Universal Standard for the Validation of Blood Pressure Measuring Devices by the Association for the Advancement of Medical Instrumentation/European Society of Hypertension/International Organization for Standardization (AAMI/ESH/ISO). J. Hypertens. 2019, 37, 459. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.-G.; Bu, P.-L.; Chen, L.-Y.; Chen, X.; Chen, Y.-Y.; Cheng, W.-L.; Chu, S.-L.; Cui, Z.-Q.; Dai, Q.-Y.; Feng, Y.-Q.; et al. 2019 Chinese Hypertension League Guidelines on Home Blood Pressure Monitoring. J. Clin. Hypertens. 2020, 22, 378–383. [Google Scholar] [CrossRef] [Green Version]
- Gar, C.; Rottenkolber, M.; Haenelt, M.; Potzel, A.L.; Kern-Matschilles, S.; Then, C.; Seissler, J.; Bidlingmaier, M.; Lechner, A. Altered Metabolic and Hormonal Responses to Moderate Exercise in Overweight/Obesity. Metabolism 2020, 107, 154219. [Google Scholar] [CrossRef]
- Eberhard, J.; Stiesch, M.; Kerling, A.; Bara, C.; Eulert, C.; Hilfiker-Kleiner, D.; Hilfiker, A.; Budde, E.; Bauersachs, J.; Kück, M.; et al. Moderate and Severe Periodontitis Are Independent Risk Factors Associated with Low Cardiorespiratory Fitness in Sedentary Non-Smoking Men Aged between 45 and 65 Years. J. Clin. Periodontol. 2014, 41, 31–37. [Google Scholar] [CrossRef]
- Gelb, H.; Mehta, N.R.; Forgione, A.G. Relationship of Muscular Strength to Jaw Posture in Sports Dentistry. N. Y. State Dent. J. 1995, 61, 58–66. [Google Scholar]
- Gay-Escoda, C.; Vieira-Duarte-Pereira, D.-M.; Ardèvol, J.; Pruna, R.; Fernandez, J.; Valmaseda-Castellón, E. Study of the Effect of Oral Health on Physical Condition of Professional Soccer Players of the Football Club Barcelona. Med. Oral Patol. Oral Cir. Bucal 2011, 16, e436–e439. [Google Scholar] [CrossRef] [Green Version]
- Okuyama, N.; Yamaga, T.; Yoshihara, A.; Nohno, K.; Yoshitake, Y.; Kimura, Y.; Shimada, M.; Nakagawa, N.; Nishimuta, M.; Ohashi, M.; et al. Influence of Dental Occlusion on Physical Fitness Decline in a Healthy Japanese Elderly Population. Arch. Gerontol. Geriatr. 2011, 52, 172–176. [Google Scholar] [CrossRef]
- Didier, H.; Assandri, F.; Gaffuri, F.; Cavagnetto, D.; Abate, A.; Villanova, M.; Maiorana, C. The Role of Dental Occlusion and Neuromuscular Behavior in Professional Ballet Dancers’ Performance: A Pilot Study. Healthcare 2021, 9, 251. [Google Scholar] [CrossRef] [PubMed]
- Cesanelli, L.; Cesaretti, G.; Ylaitė, B.; Iovane, A.; Bianco, A.; Messina, G. Occlusal Splints and Exercise Performance: A Systematic Review of Current Evidence. Int. J. Environ. Res. Public Health 2021, 18, 10338. [Google Scholar] [CrossRef] [PubMed]
- Parrini, S.; Rossini, G.; Nebiolo, B.; Airale, M.; Franceschi, A.; Cugliari, G.; Deregibus, A.; Castroflorio, T. Variations in Athletic Performance with Occlusal Splint in Track and Field Athletes: A Randomized Clinical Trial. J. Sport. Med. Phys. Fit. 2022, 62, 375–381. [Google Scholar] [CrossRef]
- Dias, A.A.; Redinha, L.A.; Silva, L.M.; Pezarat-Correia, P.C. Effects of Dental Occlusion on Body Sway, Upper Body Muscle Activity and Shooting Performance in Pistol Shooters. Appl. Bionics Biomech. 2018, 2018, e9360103. [Google Scholar] [CrossRef] [PubMed]
- Ekuni, D.; Takeuchi, N.; Furuta, M.; Tomofuji, T.; Morita, M. Relationship between Malocclusion and Heart Rate Variability Indices in Young Adults: A Pilot Study. Methods Inf. Med. 2011, 50, 358–363. [Google Scholar] [CrossRef]
- Maixner, W.; Greenspan, J.D.; Dubner, R.; Bair, E.; Mulkey, F.; Miller, V.; Knott, C.; Slade, G.D.; Ohrbach, R.; Diatchenko, L.; et al. Potential Autonomic Risk Factors for Chronic TMD: Descriptive Data and Empirically Identified Domains from the OPPERA Case-Control Study. J. Pain 2011, 12 (Suppl. S11), T75–T91. [Google Scholar] [CrossRef] [Green Version]
- Santana, M.D.R.; de Souza, A.C.A.; de Abreu, L.C.; Valenti, V.E. Association between Oral Variables and Heart Rate Variability. Int. Arch. Med. 2013, 6, 49. [Google Scholar] [CrossRef] [Green Version]
- Roi, G.S.; Sisca, G.; Perondi, F.; Diamante, A.; Nanni, G. Post Competition Blood Lactate Accumulation. J. Sport. Sci. 2004, 22, 560. Available online: https://scholar.google.com/scholar_lookup?journal=Journal+of+Sports+Sciences&title=Post+competition+blood+lactate+accumulation+during+a+first+league+soccer+season&author=G.S.+Roi&author=G.+Sisca&author=F.+Perondi&author=A.+Diamante&author=G.+Nanni&volume=22&publication_year=2004&pages=560& (accessed on 27 February 2022).
- Aslan, A.; Acikada, C.; Güvenç, A.; Gören, H.; Hazir, T.; Özkara, A. Metabolic Demands of Match Performance in Young Soccer Players. J. Sport. Sci. Med. 2012, 11, 170–179. [Google Scholar]
- Svensson, M.; Drust, B. Testing Soccer Players. J. Sport. Sci. 2005, 23, 601–618. [Google Scholar] [CrossRef]
- De Souza, J.J.; Leite, J.S.; Bahls, R.; Grande, R.S.; Santos, F.A. Clinical and Behavioral Conditions in Oral Health of Volleyball and Soccer Athletes: A Cross-Sectional Study. Braz. J. Oral Sci. 2021, 20, e213400. [Google Scholar] [CrossRef]
- Michalakis, K.X.; Kamalakidis, S.N.; Pissiotis, A.L.; Hirayama, H. The Effect of Clenching and Occlusal Instability on Body Weight Distribution, Assessed by a Postural Platform. Biomed. Res. Int. 2019, 2019, 7342541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Julià-Sánchez, S.; Álvarez-Herms, J.; Cirer-Sastre, R.; Corbi, F.; Burtscher, M. The Influence of Dental Occlusion on Dynamic Balance and Muscular Tone. Front. Physiol. 2019, 10, 1626. [Google Scholar] [CrossRef] [PubMed]
- Ackerman, J.L. Orthodontics: Art, Science, or Trans-Science? Angle Orthod. 1974, 44, 243–250. [Google Scholar] [CrossRef]
- Fleming, P.S.; Seehra, J.; Polychronopoulou, A.; Fedorowicz, Z.; Pandis, N. Cochrane and Non-Cochrane Systematic Reviews in Leading Orthodontic Journals: A Quality Paradigm? Eur. J. Orthod. 2013, 35, 244–248. [Google Scholar] [CrossRef]
- Klages, U.; Bruckner, A.; Zentner, A. Dental Aesthetics, Self-Awareness, and Oral Health-Related Quality of Life in Young Adults. Eur. J. Orthod. 2004, 26, 507–514. [Google Scholar] [CrossRef] [Green Version]
- Helm, S.; Petersen, P.E.; Kreiborg, S.; Solow, B. Effect of Separate Malocclusion Traits on Concern for Dental Appearance. Community Dent. Oral Epidemiol. 1986, 14, 217–220. [Google Scholar] [CrossRef]
- Mahmood, T.M.A.; Kareem, F.A. Psychological Impact of Dental Aesthetics for Kurdish Young Adults Seeking Orthodontic Treatment. Int. J. Health Rehabil. Sci. IJHRS 2013, 2, 28–37. [Google Scholar]
- Hamdan, A.M.; Al-Omari, I.K.; Al-Bitar, Z.B. Ranking Dental Aesthetics and Thresholds of Treatment Need: A Comparison between Patients, Parents, and Dentists. Eur. J. Orthod. 2007, 29, 366–371. [Google Scholar] [CrossRef] [Green Version]
- Aksakalli, S.; Temucin, F.; Pamukcu, A.; Ezirganlı, S.; Kazancioglu, H.O.; Malkoc, M.A. Effectiveness of Two Different Splints to Treat Temporomandibular Disorders. J. Orofac. Orthop. 2015, 76, 318–327. [Google Scholar] [CrossRef]
- Zonnenberg, A.J.J.; Mulder, J. The Efficacy of a Specific Stabilization Splint. Cranio 2014, 32, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Wänman, A.; Marklund, S. Treatment Outcome of Supervised Exercise, Home Exercise and Bite Splint Therapy, Respectively, in Patients with Symptomatic Disc Displacement with Reduction: A Randomised Clinical Trial. J. Oral Rehabil. 2020, 47, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Conti, P.C.R.; da Mota Corrêa, A.S.; Lauris, J.R.P.; Stuginski-Barbosa, J. Management of Painful Temporomandibular Joint Clicking with Different Intraoral Devices and Counseling: A Controlled Study. J. Appl. Oral. Sci. 2015, 23, 529–535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zou, J.; Meng, M.; Law, C.S.; Rao, Y.; Zhou, X. Common Dental Diseases in Children and Malocclusion. Int. J. Oral Sci. 2018, 10, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alqahtan, I.M.; Azizkhan, R.A.; Alyawer, L.T.; Alanazi, S.S.; Ahmed, R.; Alhazmi, L.S.; Bsher, F.F.; Zahran, L.M.; Aljahdali, R.A.; Alqwizany, R.R.; et al. An Overview of Diagnosis and Management of Malocclusion: Literature Review. Ann. Dent. Spec. 2020, 8, 62. [Google Scholar]
- Zebrick, B.; Teeramongkolgul, T.; Nicot, R.; Horton, M.J.; Raoul, G.; Ferri, J.; Vieira, A.R.; Sciote, J.J. ACTN3 R577X Genotypes Associate with Class II and Deepbite Malocclusions. Am. J. Orthod. Dentofac. Orthop. 2014, 146, 603–611. [Google Scholar] [CrossRef] [Green Version]
- North, K.N.; Beggs, A.H. Deficiency of a Skeletal Muscle Isoform of Alpha-Actinin (Alpha-Actinin-3) in Merosin-Positive Congenital Muscular Dystrophy. Neuromuscul. Disord. 1996, 6, 229–235. [Google Scholar] [CrossRef]
- Zouhal, H.; Coso, J.D.; Jayavel, A.; Tourny, C.; Ravé, G.; Jebabli, N.; Clark, C.C.T.; Barthélémy, B.; Hackney, A.C.; Abderrahman, A.B. Association between ACTN3 R577X Genotype and Risk of Non-Contact Injury in Trained Athletes: A Systematic Review. J. Sport Health Sci. 2021, S2095-2546(21)00074-0. [Google Scholar] [CrossRef]
- Houweling, P.J.; Papadimitriou, I.D.; Seto, J.T.; Pérez, L.M.; Coso, J.D.; North, K.N.; Lucia, A.; Eynon, N. Is Evolutionary Loss Our Gain? The Role of ACTN3 p.Arg577Ter (R577X) Genotype in Athletic Performance, Ageing, and Disease. Hum. Mutat. 2018, 39, 1774–1787. [Google Scholar] [CrossRef]
- Hogarth, M.W.; Garton, F.C.; Houweling, P.J.; Tukiainen, T.; Lek, M.; Macarthur, D.G.; Seto, J.T.; Quinlan, K.G.R.; Yang, N.; Head, S.I.; et al. Analysis of the ACTN3 Heterozygous Genotype Suggests That α-Actinin-3 Controls Sarcomeric Composition and Muscle Function in a Dose-Dependent Fashion. Hum. Mol. Genet. 2016, 25, 866–877. [Google Scholar] [CrossRef] [Green Version]
- Seto, J.T.; Lek, M.; Quinlan, K.G.R.; Houweling, P.J.; Zheng, X.F.; Garton, F.; MacArthur, D.G.; Raftery, J.M.; Garvey, S.M.; Hauser, M.A.; et al. Deficiency of α-Actinin-3 Is Associated with Increased Susceptibility to Contraction-Induced Damage and Skeletal Muscle Remodeling. Hum. Mol. Genet. 2011, 20, 2914–2927. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, N.; Schindeler, A.; McDonald, M.M.; Seto, J.T.; Houweling, P.J.; Lek, M.; Hogarth, M.; Morse, A.R.; Raftery, J.M.; Balasuriya, D.; et al. α-Actinin-3 Deficiency Is Associated with Reduced Bone Mass in Human and Mouse. Bone 2011, 49, 790–798. [Google Scholar] [CrossRef]
- Cunha, A.; Nelson-Filho, P.; Marañón-Vásquez, G.A.; de Carvalho Ramos, A.G.; Dantas, B.; Sebastiani, A.M.; Silvério, F.; Omori, M.A.; Rodrigues, A.S.; Teixeira, E.C.; et al. Genetic Variants in ACTN3 and MYO1H Are Associated with Sagittal and Vertical Craniofacial Skeletal Patterns. Arch. Oral Biol. 2019, 97, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Bichara, L.M.; Aragón, M.L.; Brandão, G.A.; Normando, D. Factors influencing orthodontic treatment time for non-surgical Class III malocclusion. J. Appl. Oral Sci. 2016, 24, 431–436. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Anthropometric Data | With Malocclusion (Mean ± SD) | Without Malocclusion (Mean ± SD) | 95% CI of Difference | p-Value (t-Test) |
|---|---|---|---|---|
| Age (years) | 15.1 ± 1.5 | 14.7 ± 1.9 | (−1.43, 0.65) | 0.46 |
| Body height (cm) | 170 ± 10 | 177 ± 12 | (−0.004, 0.14) | 0.06 |
| Body Mass (kg) | 62.5 ± 9.9 | 69.5 ± 10.9 | (0.17, 13.8) | 0.04 |
| BMI (kg/m2) | 19.25 ± 1.9 | 19.42 ± 1.7 | (−1.05, 1.42) | 0.76 |
| Biological Parameters (Not Normally Distributed) | With Malocclusion Median (IQR (Q1–Q3)) | Without Malocclusion Median (IQR (Q1–Q3)) | 95% CI of Difference | p-Value (Mann–Whitney Test) |
|---|---|---|---|---|
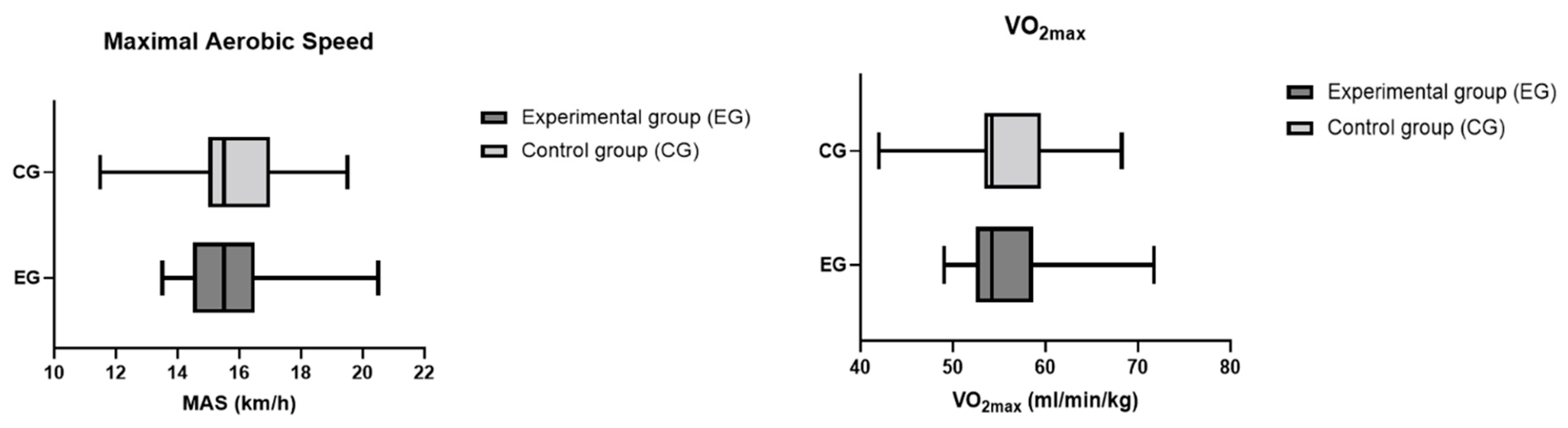
| Maximal aerobic speed (km/h) | 15.5 (14.5–16.5) | 15.5 (15–17) | (−1.00, 1.00) | 0.47 |
| VO2max (mL/min/kg) | 54.2 (52.5–58.6) | 54.2 (53.4–59.5) | (−3.50, 3.50) | 0.62 |
| Biological Parameters (Normally Distributed) | With Malocclusion (Mean ± SD) | Without Malocclusion (Mean ± SD) | t, df | 95% CI of Difference | p-Value (t-Test) |
|---|---|---|---|---|---|
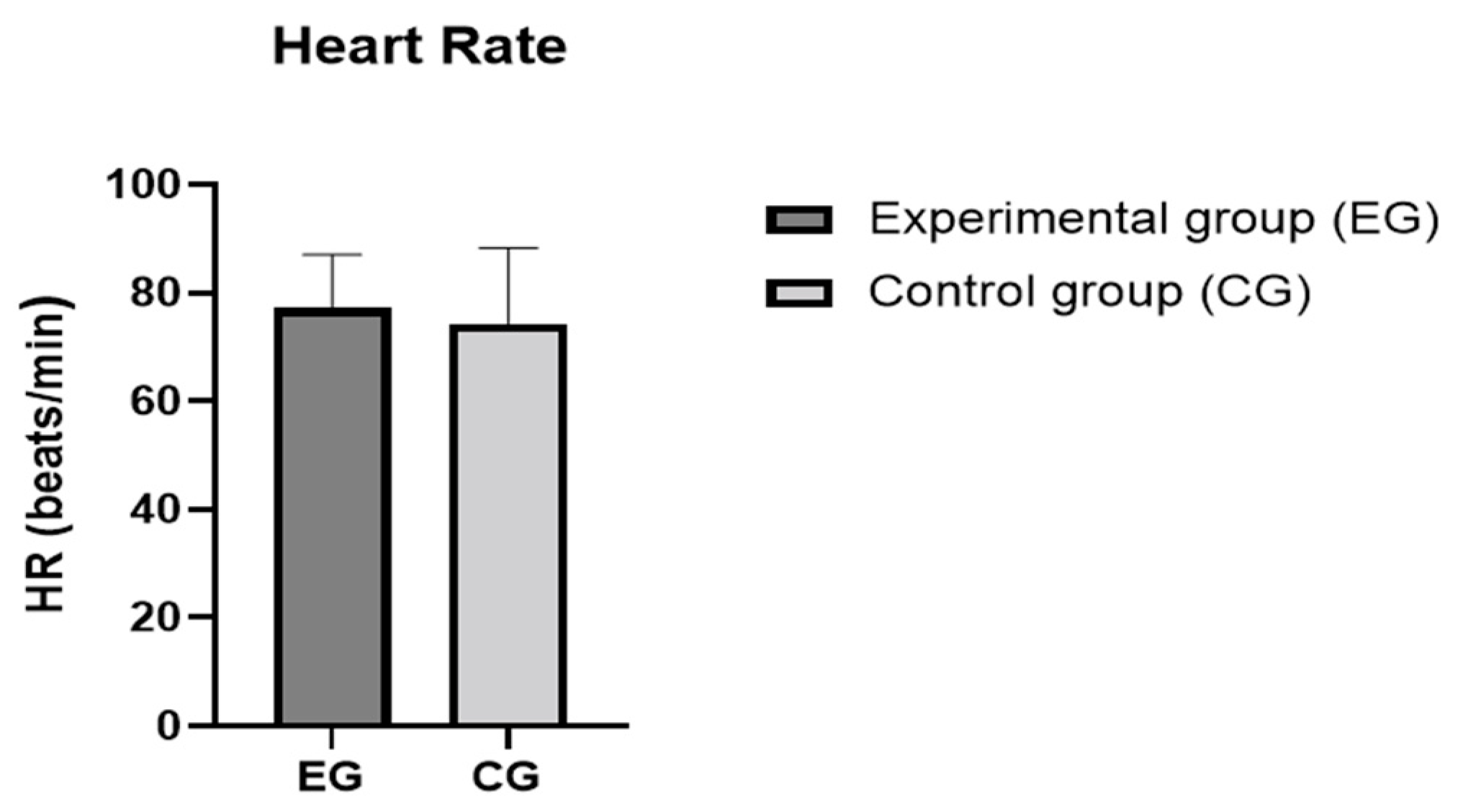
| Resting heart rate (beats/min) | 77.1 ± 9.9 | 74.3 ± 14.0 | 0.80, 48 | (−10.01, 4.35) | 0.43 |
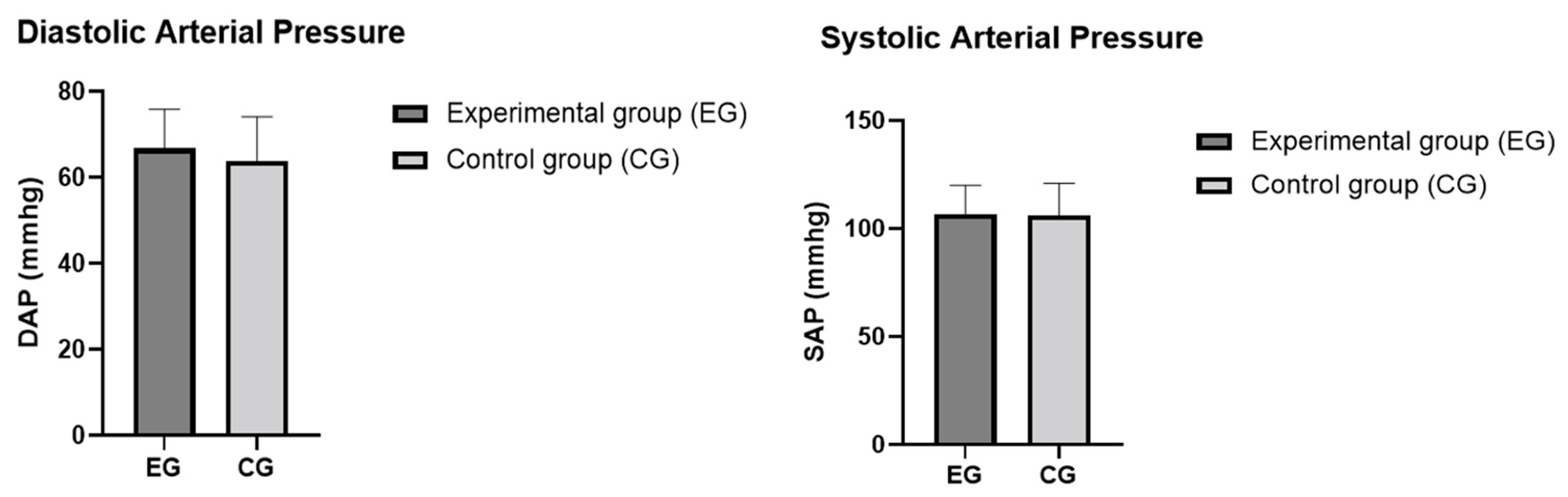
| Systolic arterial pressure (mmHg) | 106.6 ± 13.4 | 106.2 ± 14.8 | 0.10, 48 | (−9.42, 8.5) | 0.91 |
| Diastolic arterial pressure (mmHg) | 66.7 ± 9.1 | 63.9 ± 10.2 | 0.91, 48 | (−8.9, 3.32) | 0.36 |
| Lactate (before physical effort) (mmol/L) | 1.5 ± 0.4 | 1.3 ± 0.4 | 1.56, 48 | (−0.45, 0.06) | 0.12 |
| Lactate (after physical effort) (mmol/L) | 4.5 ± 2.36 | 4.06 ± 3.04 | 0.51, 48 | (−2.10, 1.24) | 0.60 |
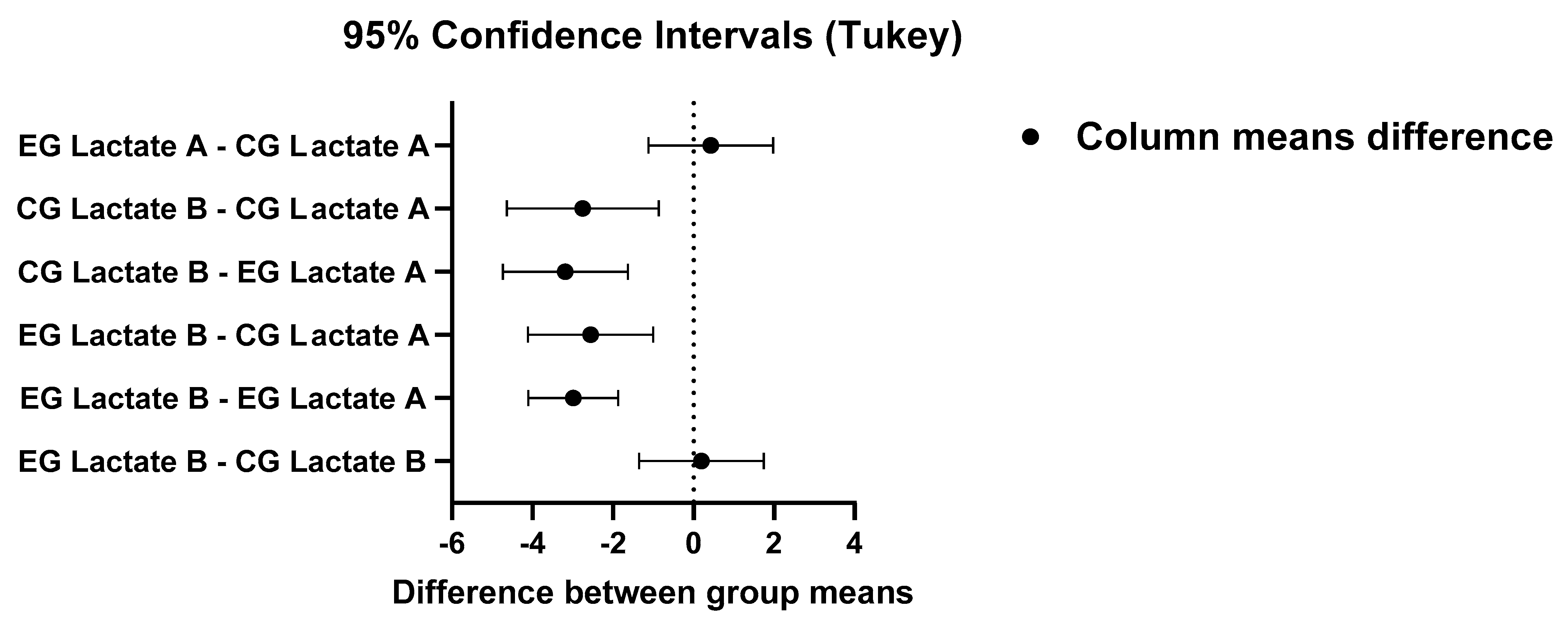
| Tukey’s Multiple Comparison Test | Mean Difference | 95% CI of Difference | Significant | Adjusted p-Value |
|---|---|---|---|---|
| EG Lactate B vs. CG Lactate B | 0.2 | (−1.35, 1.75) | ns | 0.98 |
| EG Lactate B vs. EG Lactate A | −2.10 | (−4.10, −1.87) | **** | <0.0001 |
| EG Lactate B vs. CG Lactate A | −2.55 | (−4.10, −1.005) | *** | 0.0002 |
| CG Lactate B vs. EG Lactate A | −3.18 | (−4.73, −1.63) | **** | <0.0001 |
| CG Lactate B vs. CG Lactate A | −2.75 | (−4.64, −0.86) | ** | 0.001 |
| EG Lactate A vs. CG Lactate A | 0.43 | (−1.12, 1.10) | ns | 0.88 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
El Ouali, E.M.; Zouhal, H.; Bahije, L.; Ibrahimi, A.; Benamar, B.; Kartibou, J.; Saeidi, A.; Laher, I.; El Harane, S.; Granacher, U.; et al. Effects of Malocclusion on Maximal Aerobic Capacity and Athletic Performance in Young Sub-Elite Athletes. Sports 2023, 11, 71. https://doi.org/10.3390/sports11030071
El Ouali EM, Zouhal H, Bahije L, Ibrahimi A, Benamar B, Kartibou J, Saeidi A, Laher I, El Harane S, Granacher U, et al. Effects of Malocclusion on Maximal Aerobic Capacity and Athletic Performance in Young Sub-Elite Athletes. Sports. 2023; 11(3):71. https://doi.org/10.3390/sports11030071
Chicago/Turabian StyleEl Ouali, El Mokhtar, Hassane Zouhal, Loubna Bahije, Azeddine Ibrahimi, Bahae Benamar, Jihan Kartibou, Ayoub Saeidi, Ismail Laher, Sanae El Harane, Urs Granacher, and et al. 2023. "Effects of Malocclusion on Maximal Aerobic Capacity and Athletic Performance in Young Sub-Elite Athletes" Sports 11, no. 3: 71. https://doi.org/10.3390/sports11030071