
Pyjamas, Polysomnography and Professional Athletes: The Role of Sleep Tracking Technology in Sport

 , ,
, ,
Abstract
:1. Introduction
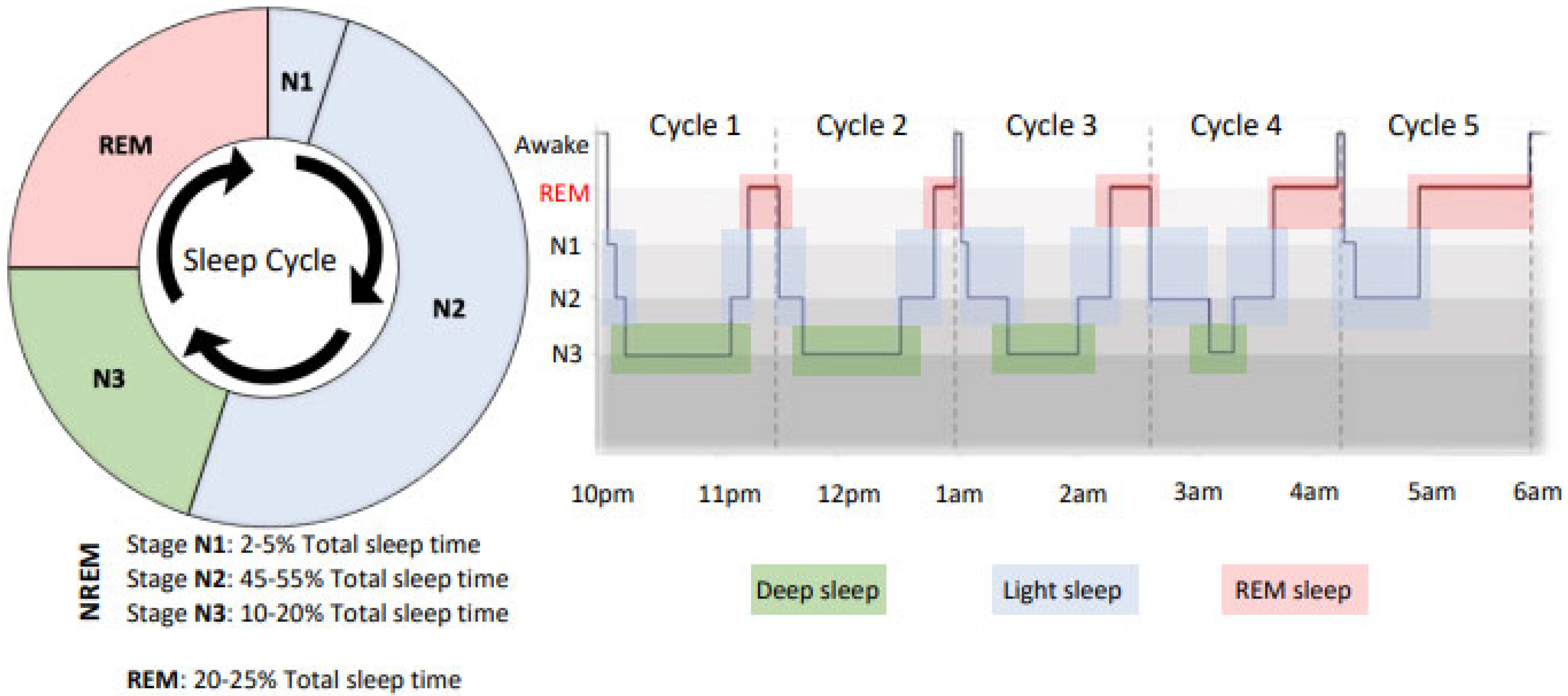
1.1. The Sleep Cycle and Its Importance to the Athlete
1.2. Sleep, Athlete Recovery, and Performance
1.3. Hierarchy of Sleep Assessment
1.4. Polysomnography and Other Clinical Sleep Tests
1.5. Wearable Devices
1.6. How Valid and Reliable Are the Measures Gained from Sleep Wearables?
1.7. Wrist-Worn Wearables
1.8. Finger-Worn Wearables
1.9. Clothing-Based Sleep Monitoring
1.10. Head-Worn Sensors
1.11. Nearables
1.12. Sleep Questionnaires and Diaries
1.13. Sleep Metrics Provided by Sleep Trackers
1.14. How Can We Use Data to Guide Changes in Sleep?
1.15. Limitations of Using Wearables in Athletes
1.16. Data Ownership and Privacy
1.17. Practical Recommendations for the Use of Sleep Wearables in Sport
2. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lastella, M.; Memon, A.R.; Vincent, G.E. Global Research Output on Sleep Research in Athletes from 1966 to 2019: A Bibliometric Analysis. Clocks Sleep 2020, 2, 99–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walsh, N.P.; Halson, S.L.; Sargent, C.; Roach, G.D.; Nédélec, M.; Gupta, L.; Leeder, J.; Fullagar, H.H.; Coutts, A.J.; Edwards, B.J.; et al. Sleep and the athlete: Narrative review and 2021 expert consensus recommendations. Br. J. Sport. Med. 2020, 55, 356–368. [Google Scholar] [CrossRef] [PubMed]
- McCarley, R.W. Neurobiology of REM and NREM sleep. Sleep Med. 2007, 8, 302–330. [Google Scholar] [CrossRef] [PubMed]
- Halson, S.L.; Juliff, L.E. Sleep, sport, and the brain. Prog. Brain Res. 2017, 234, 13–31. [Google Scholar] [PubMed]
- Knowles, O.E. No time to sleep on it–start exercising! J. Physiol. 2020, 598, 2059–2060. [Google Scholar] [CrossRef] [PubMed]
- Morrison, M.; Halson, S.L.; Weakley, J.; Hawley, J.A. Sleep, circadian biology and skeletal muscle interactions: Implications for metabolic health. Sleep Med. Rev. 2022, 66, 101700. [Google Scholar] [CrossRef]
- Rooyackers, O.E.; Nair, K.S. Hormonal regulation of human muscle protein metabolism. Annu. Rev. Nutr. 1997, 17, 457–485. [Google Scholar] [CrossRef]
- Czeisler, C.; Klerman, E. Circadian and sleep-dependent regulation of hormone release in humans. Recent Prog. Horm. Res. 1999, 54, 97–132. [Google Scholar]
- Besedovsky, L.; Lange, T.; Born, J. Sleep and immune function. Pflüg. Arch. Eur. J. Physiol. 2012, 463, 121–137. [Google Scholar] [CrossRef] [Green Version]
- Della Monica, C.; Johnsen, S.; Atzori, G.; Groeger, J.A.; Dijk, D.-J. Rapid eye movement sleep, sleep continuity and slow wave sleep as predictors of cognition, mood, and subjective sleep quality in healthy men and women, aged 20–84 years. Front. Psychiatry 2018, 9, 255. [Google Scholar] [CrossRef] [Green Version]
- Miller, K.E.; Gehrman, P.R. REM sleep: What is it good for? Curr. Biol. 2019, 29, R806–R807. [Google Scholar] [CrossRef]
- Pilcher, J.J.; Huffcutt, A.I. Effects of sleep deprivation on performance: A meta-analysis. Sleep 1996, 19, 318–326. [Google Scholar] [CrossRef]
- O’Donnell, S.; Beaven, C.M.; Driller, M.W. From pillow to podium: A review on understanding sleep for elite athletes. Nat. Sci. Sleep 2018, 10, 243–253. [Google Scholar] [CrossRef] [Green Version]
- Teece, A.R.; Argus, C.K.; Gill, N.; Beaven, M.; Dunican, I.C.; Driller, M.W. Sleep and performance during a preseason in elite rugby union athletes. Int. J. Environ. Res. Public Health 2021, 18, 4612. [Google Scholar] [CrossRef]
- Watson, A.M. Sleep and athletic performance. Curr. Sport. Med. Rep. 2017, 16, 413–418. [Google Scholar] [CrossRef]
- Miles, K.H.; Clark, B.; Fowler, P.M.; Miller, J.; Pumpa, K.L. Sleep practices implemented by team sport coaches and sports science support staff: A potential avenue to improve athlete sleep? J. Sci. Med. Sport 2019, 22, 748–752. [Google Scholar] [CrossRef]
- Dunican, I.C.; Walsh, J.; Higgins, C.C.; Jones, M.J.; Maddison, K.; Caldwell, J.A.; David, H.; Eastwood, P.R. Prevalence of sleep disorders and sleep problems in an elite super rugby union team. J. Sport. Sci. 2019, 37, 950–957. [Google Scholar] [CrossRef]
- Tuomilehto, H.; Vuorinen, V.-P.; Penttilä, E.; Kivimäki, M.; Vuorenmaa, M.; Venojärvi, M.; Airaksinen, O.; Pihlajamäki, J. Sleep of professional athletes: Underexploited potential to improve health and performance. J. Sport. Sci. 2017, 35, 704–710. [Google Scholar] [CrossRef]
- Caia, J.; Halson, S.L.; Scott, A.; Kelly, V.G. Obstructive sleep apnea in professional rugby league athletes: An exploratory study. J. Sci. Med. Sport 2020, 23, 1011–1015. [Google Scholar] [CrossRef]
- Laricchia, F. Number of Connected Wearable Devices Worldwide from 2016 to 2022. 2022. Available online: https://www.statista.com/statistics/487291/global-connected-wearable-devices/ (accessed on 23 August 2022).
- Fonseca, P.; Weysen, T.; Goelema, M.S.; Møst, E.I.; Radha, M.; Lunsingh Scheurleer, C.; van den Heuvel, L.; Aarts, R.M. Validation of photoplethysmography-based sleep staging compared with polysomnography in healthy middle-aged adults. Sleep 2017, 40, zsx097. [Google Scholar] [CrossRef]
- Scott, H.; Lack, L.; Lovato, N. A systematic review of the accuracy of sleep wearable devices for estimating sleep onset. Sleep Med. Rev. 2020, 49, 101227. [Google Scholar] [CrossRef] [PubMed]
- Chinoy, E.D.; Cuellar, J.A.; Huwa, K.E.; Jameson, J.T.; Watson, C.H.; Bessman, S.C.; Hirsch, D.A.; Cooper, A.D.; Drummond, S.P.; Markwald, R.R. Performance of seven consumer sleep-tracking devices compared with polysomnography. Sleep 2021, 44, zsaa291. [Google Scholar] [CrossRef] [PubMed]
- Chinoy, E.D.; Cuellar, J.A.; Jameson, J.T.; Markwald, R.R. Performance of Four Commercial Wearable Sleep-Tracking Devices Tested Under Unrestricted Conditions at Home in Healthy Young Adults. Nat. Sci. Sleep 2022, 14, 493. [Google Scholar] [CrossRef] [PubMed]
- de Zambotti, M.; Baker, F.C.; Willoughby, A.R.; Godino, J.G.; Wing, D.; Patrick, K.; Colrain, I.M. Measures of sleep and cardiac functioning during sleep using a multi-sensory commercially-available wristband in adolescents. Physiol. Behav. 2016, 158, 143–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Zambotti, M.; Claudatos, S.; Inkelis, S.; Colrain, I.M.; Baker, F.C. Evaluation of a consumer fitness-tracking device to assess sleep in adults. Chronobiol. Int. 2015, 32, 1024–1028. [Google Scholar] [CrossRef] [Green Version]
- Depner, C.M.; Cheng, P.C.; Devine, J.K.; Khosla, S.; De Zambotti, M.; Robillard, R.; Vakulin, A.; Drummond, S.P. Wearable technologies for developing sleep and circadian biomarkers: A summary of workshop discussions. Sleep 2020, 43, zsz254. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.-M.; Byun, W.; Keill, A.; Dinkel, D.; Seo, Y. Comparison of wearable trackers’ ability to estimate sleep. Int. J. Environ. Res. Public Health 2018, 15, 1265. [Google Scholar] [CrossRef] [Green Version]
- Miller, D.J.; Lastella, M.; Scanlan, A.T.; Bellenger, C.; Halson, S.L.; Roach, G.D.; Sargent, C. A validation study of the WHOOP strap against polysomnography to assess sleep. J. Sport. Sci. 2020, 38, 2631–2636. [Google Scholar] [CrossRef]
- Svensson, T.; Chung, U.-i.; Tokuno, S.; Nakamura, M.; Svensson, A.K. A validation study of a consumer wearable sleep tracker compared to a portable EEG system in naturalistic conditions. J. Psychosom. Res. 2019, 126, 109822. [Google Scholar] [CrossRef]
- Roberts, D.M.; Schade, M.M.; Mathew, G.M.; Gartenberg, D.; Buxton, O.M. Detecting sleep using heart rate and motion data from multisensor consumer-grade wearables, relative to wrist actigraphy and polysomnography. Sleep 2020, 43, zsaa045. [Google Scholar] [CrossRef]
- Evenson, K.R.; Goto, M.M.; Furberg, R.D. Systematic review of the validity and reliability of consumer-wearable activity trackers. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 159. [Google Scholar] [CrossRef]
- Driller, M.; McQuillan, J.; O’Donnell, S. Inter-device reliability of an automatic-scoring actigraph for measuring sleep in healthy adults. Sleep Sci. 2016, 9, 198–201. [Google Scholar] [CrossRef] [Green Version]
- Razjouyan, J.; Lee, H.; Parthasarathy, S.; Mohler, J.; Sharafkhaneh, A.; Najafi, B. Improving sleep quality assessment using wearable sensors by including information from postural/sleep position changes and body acceleration: A comparison of chest-worn sensors, wrist actigraphy, and polysomnography. J. Clin. Sleep Med. 2017, 13, 1301–1310. [Google Scholar] [CrossRef] [Green Version]
- Driller, M.W.; O’Donnell, S.; Tavares, F. What wrist should you wear your actigraphy device on? Analysis of dominant vs. non-dominant wrist actigraphy for measuring sleep in healthy adults. Sleep Sci. 2017, 10, 132–135. [Google Scholar] [CrossRef] [Green Version]
- De Zambotti, M.; Cellini, N.; Goldstone, A.; Colrain, I.M.; Baker, F.C. Wearable sleep technology in clinical and research settings. Med. Sci. Sport. Exerc. 2019, 51, 1538–1557. [Google Scholar] [CrossRef]
- Cay, G.; Ravichandran, V.; Sadhu, S.; Zisk, A.H.; Salisbury, A.; Solanki, D.; Mankodiya, K. Recent Advancement in Sleep Technologies: A Literature Review on Clinical Standards, Sensors, Apps, and AI Methods. IEEE Access 2022, 10, 104737–104756. [Google Scholar] [CrossRef]
- de Zambotti, M.; Rosas, L.; Colrain, I.M.; Baker, F.C. The sleep of the ring: Comparison of the ŌURA sleep tracker against polysomnography. Behav. Sleep Med. 2019, 17, 124–136. [Google Scholar] [CrossRef]
- Altini, M.; Kinnunen, H. The promise of sleep: A multi-sensor approach for accurate sleep stage detection using the oura ring. Sensors 2021, 21, 4302. [Google Scholar] [CrossRef]
- Scott, H.; Lovato, N.; Lack, L. The development and accuracy of the THIM wearable device for estimating sleep and wakefulness. Nat. Sci. Sleep 2021, 13, 39–53. [Google Scholar] [CrossRef]
- Andrew, T.L.; Rostaminia, S.; Homayounfar, S.Z.; Ganesan, D. Perspective—Longitudinal Sleep Monitoring for All: Payoffs, Challenges and Outlook. ECS Sens. Plus 2022, 1, 011602. [Google Scholar] [CrossRef]
- Kiaghadi, A.; Homayounfar, S.Z.; Gummeson, J.; Andrew, T.; Ganesan, D. Phyjama: Physiological sensing via fiber-enhanced pyjamas. Proc. ACM Interact. Mob. Wearable Ubiquitous Technol. 2019, 3, 1–29. [Google Scholar] [CrossRef]
- Miller, D.J.; Sargent, C.; Roach, G.D. A Validation of Six Wearable Devices for Estimating Sleep, Heart Rate and Heart Rate Variability in Healthy Adults. Sensors 2022, 22, 6317. [Google Scholar] [CrossRef] [PubMed]
- Arnal, P.J.; Thorey, V.; Debellemaniere, E.; Ballard, M.E.; Bou Hernandez, A.; Guillot, A.; Jourde, H.; Harris, M.; Guillard, M.; Van Beers, P. The Dreem Headband compared to polysomnography for electroencephalographic signal acquisition and sleep staging. Sleep 2020, 43, zsaa097. [Google Scholar] [CrossRef] [PubMed]
- Schutte-Rodin, S.; Deak, M.C.; Khosla, S.; Goldstein, C.A.; Yurcheshen, M.; Chiang, A.; Gault, D.; Kern, J.; O’Hearn, D.; Ryals, S. Evaluating consumer and clinical sleep technologies: An American Academy of Sleep Medicine update. J. Clin. Sleep Med. 2021, 17, 2275–2282. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, M.T. Sleep devices: Wearables and nearables, informational and interventional, consumer and clinical. Metabolism 2018, 84, 99–108. [Google Scholar] [CrossRef]
- Hsiou, D.A.; Gao, C.; Matlock, R.C.; Scullin, M.K. Validation of a nonwearable device in healthy adults with normal and short sleep durations. J. Clin. Sleep Med. 2022, 18, 751–757. [Google Scholar] [CrossRef]
- Kholghi, M.; Szollosi, I.; Hollamby, M.; Bradford, D.; Zhang, Q. A validation study of a ballistocardiograph sleep tracker EMFIT QS against polysomnography. J. Clin. Sleep Med. 2021, 18, 1203–1210. [Google Scholar] [CrossRef]
- Bender, A.M.; Lawson, D.; Werthner, P.; Samuels, C.H. The clinical validation of the athlete sleep screening questionnaire: An instrument to identify athletes that need further sleep assessment. Sport. Med. Open 2018, 4, 23. [Google Scholar] [CrossRef] [Green Version]
- Driller, M.W.; Mah, C.D.; Halson, S.L. Development of the athlete sleep behavior questionnaire: A tool for identifying maladaptive sleep practices in elite athletes. Sleep Sci. 2018, 11, 37–44. [Google Scholar] [CrossRef]
- Caia, J.; Thornton, H.R.; Kelly, V.G.; Scott, T.J.; Halson, S.L.; Cupples, B.; Driller, M.W. Does self-perceived sleep reflect sleep estimated via activity monitors in professional rugby league athletes? J. Sport. Sci. 2017, 36, 1492–1496. [Google Scholar] [CrossRef]
- Gavriloff, D.; Sheaves, B.; Juss, A.; Espie, C.A.; Miller, C.B.; Kyle, S.D. Sham sleep feedback delivered via actigraphy biases daytime symptom reports in people with insomnia: Implications for insomnia disorder and wearable devices. J. Sleep Res. 2018, 27, e12726. [Google Scholar] [CrossRef]
- Rahman, S.A.; Rood, D.; Trent, N.; Solet, J.; Langer, E.J.; Lockley, S.W. Manipulating sleep duration perception changes cognitive performance–an exploratory analysis. J. Psychsom. Res. 2020, 132, 109992. [Google Scholar] [CrossRef]
- Fullagar, H.H.; Skorski, S.; Duffield, R.; Meyer, T. The effect of an acute sleep hygiene strategy following a late-night soccer match on recovery of players. Chronobiol. Int. 2016, 33, 490–505. [Google Scholar] [CrossRef]
- O’Donnell, S.; Driller, M.W. Sleep-hygiene education improves sleep indices in elite female athletes. Int. J. Exerc. Sci. 2017, 10, 522–530. [Google Scholar]
- Caia, J.; Scott, T.J.; Halson, S.L.; Kelly, V.G. The influence of sleep hygiene education on sleep in professional rugby league athletes. Sleep Health 2018, 4, 364–368. [Google Scholar] [CrossRef]
- Driller, M.W.; Lastella, M.; Sharp, A.P. Individualized sleep education improves subjective and objective sleep indices in elite cricket athletes: A pilot study. J. Sport. Sci. 2019, 37, 2121–2125. [Google Scholar] [CrossRef]
- Baron, K.G.; Abbott, S.; Jao, N.; Manalo, N.; Mullen, R. Orthosomnia: Are some patients taking the quantified self too far? J. Clin. Sleep Med. 2017, 13, 351–354. [Google Scholar] [CrossRef] [Green Version]
- Verbeek, I.; Klip, E.C.; Declerck, A.C. The use of actigraphy revised: The value for clinical practice in insomnia. Percept. Mot. Ski. 2001, 92, 852–856. [Google Scholar] [CrossRef]
- Röddiger, T.; Clarke, C.; Breitling, P.; Schneegans, T.; Zhao, H.; Gellersen, H.; Beigl, M. Sensing with Earables: A Systematic Literature Review and Taxonomy of Phenomena. Proc. ACM Interact. Mob. Wearable Ubiquitous Technol. 2022, 6, 1–57. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Assessment Tool | Description | Advantages | Disadvantages | When to Use | Examples |
|---|---|---|---|---|---|
| Polysomnography (PSG) Level I | Gold standard for the assessment of sleep | Used to diagnose a sleep disorder | Not suitable or designed for longitudinal measures of sleep in athletes | Used to assess for the prevalence of sleep disorders such as sleep apnoea | Compumedics Somte, Philips Respironics Alice 6, Nahon Kohden PSG-1100 |
| Used for Multiple Sleep Latency Test and Maintenance of Wake Test | Not for evaluation of pre- versus post-interventions in sleep behaviours | Generally used for one to two nights | |||
| Method for determining sleep architecture (sleep stages) | Expensive and requires specialist expertise | Laboratory-based research | |||
| Intrusive and can be a bad night’s sleep for the individual | When investigating interventions that might influence sleep architecture | ||||
| Is not indicative of sleep behaviours | |||||
| Polysomnography (PSG) Level II | Used for home-based assessment of sleep disorders | Method for determining sleep architecture (sleep stages) | Not suitable for everyday use, but can do multiple nights in the home | Used to assess for the prevalence of sleep disorders such as sleep apnoea | Cerebra Sleep System, Sleep Profiler |
| Allows the person to sleep in their bed | Expensive and requires specialist expertise | When investigating interventions that might influence sleep architecture | |||
| Unattended, and some devices are self-applied | Intrusive and can be a bad night’s sleep for the person | For high-profile elite athletes that do not wish to attend a laboratory | |||
| Objective measure of sleep and sleep disorders | |||||
| Home Sleep Apnoea Testing (HSAT) Levels III–IV | Used for home-based assessment of sleep apnoea | Allows the person to sleep in their bed | Not suitable for everyday use, but can do multiple nights in the home | For sleep disorder assessments in different environments, e.g., at altitude | Remmers Sleep Recorder, ApneaLink |
| Objective measure of sleep-disordered breathing | Not for evaluation of pre- versus post-interventions in sleep behaviours | For high-profile elite athletes that do not wish to attend a laboratory | |||
| Do not have to attend a sleep laboratory | Expensive and requires specialist expertise | When pre-test probability deems Levels III–IV | |||
| Intrusive and can be a bad night’s sleep for the person | |||||
| Does not measure sleep using EEG | |||||
| Wearables | Wrist- or finger-worn actigraphy devices utilising accelerometery and/or sensors to determine sleep/wake periods and behaviours | Allows longitudinal measures of sleep (over a season) | Lack of validation for some devices | Can be used anytime; during a playing season, pre-season, or off-season | Readiband, Fitbit, ActiGraph, Whoop, ActiWatch, Oura, Garmin, Apple Watch |
| Physical activity trackers (FDA approved) | Not classified as medical devices | Recommended for at least 2 weeks to establish sleep behaviours | |||
| Used for assessment of circadian rhythm disorders, such as jet lag, shiftwork disorder, and phase delay | Does not assess sleep-related breathing disorders or movement disorders | ||||
| Relatively low cost and easy to use | Difficult to aggregate data, may require additional cost to aggregate and analyse | ||||
| Promote athlete and performance staff interaction and discussion | May not provide accurate representation of sleep stages | ||||
| Supports further evaluation or PSG for sleep disorders | Some devices require a scientist to score the data | ||||
| Many have automated scoring algorithms that can be instantly provided to a smartphone | Some devices require a sleep diary to completed in conjunction with wearing the device | ||||
| Minimally invasive | Algorithms and scores are not openly reported/validated | ||||
| Nearables and Smartphone Applications | Devices placed in proximity of the person sleeping, in the bed, or near the bed | Easy to use and often preferred to use instead of wearables or PSG | May measure sleep from bed partner | Beddit, Resmed+, Sleep Score, Sleep cycle applications | |
| Can increase awareness of sleep and sleep problems | May be impacted by pets in the bedroom | ||||
| Device does not have to be worn—minimally invasive | Lack of validation on many smartphone applications | ||||
| Validated Sleep-Related Questionnaires | Used to determine the potential prevalence of sleep disorders and problems | Low cost, easy to use, and requires no training or expertise | Not a clinical diagnosis and requires further assessment | Can be used anytime; during a playing season, pre-season, or off-season | Athlete Sleep Behaviour Questionnaire, Athlete Sleep Screening Questionnaire, PSQI, ESS, Berlin, ISI, Sleep Hygiene Index. |
| Used as a baseline of sleep behaviours and problems | Some not specific to the challenges that athletes face | ||||
| Can be used as a precursor for the potential prevalence of a sleep disorder | |||||
| Used for organisational and demographic reporting and potential health promotion or interventions | |||||
| Sleep Diaries | Self-reported reflective sleep timing based upon recall | Low cost, easy to use, and requires no training or expertise | People tend to overestimate sleep duration, underestimate sleep latency and wake time | Can be used anytime; during a playing season, pre-season, or off-season | |
| Well used in the research literature | Long-term adherence to filling out sleep diaries is generally poor | ||||
| Can provide interesting information on sleep timings (time at sleep and time at wake) | Difficult for coaches and leaders to take actions based upon this data as highly variable |
| Sleep Measure | Acronym | Units | Abbreviated | Measurement | Description |
|---|---|---|---|---|---|
| Sleep Onset Latency | SOL | Minutes | mins | Derived | Number of minutes from Time at Lights Out to Time at Sleep Onset |
| Sleep Onset Time | SOT | Time of day | hh:mm | Directly measured | Time of day when the first epoch of sleep occurs between Time at Lights Out and Time at Wake |
| Total Sleep Time | TST | Hours and Minutes | h:min | Derived | Number of minutes from Time at Sleep Onset to Time at Wake, minus number of minutes awake (WASO) |
| Wake After Sleep Onset | WASO | Minutes | mins | Directly measured | Number of minutes awake after Time at Sleep Onset |
| Wake Time | WT | Time of day | hh:mm | Directly measured | Time of day when awake with no further Sleep Duration |
| Sleep Efficiency | SE | Percentage | % | Derived | Sleep Duration divided by Time in Bed multiplied by 100 |
| Time in Bed | TIB | Hours and Minutes | h:min | Derived | The total time spent in bed, from Time at Lights Out to Time at Wake |
| Sleep Onset Variance | SOV | Hours and Minutes | h:min | Derived | Can be calculated using standard deviations or by using the sleep regularity index (SRI) |
| Wake Variance | WV | Hours and Minutes | h:min | Derived | Can be calculated using standard deviations or by using the sleep regularity index (SRI) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Driller, M.W.; Dunican, I.C.; Omond, S.E.T.; Boukhris, O.; Stevenson, S.; Lambing, K.; Bender, A.M. Pyjamas, Polysomnography and Professional Athletes: The Role of Sleep Tracking Technology in Sport. Sports 2023, 11, 14. https://doi.org/10.3390/sports11010014
Driller MW, Dunican IC, Omond SET, Boukhris O, Stevenson S, Lambing K, Bender AM. Pyjamas, Polysomnography and Professional Athletes: The Role of Sleep Tracking Technology in Sport. Sports. 2023; 11(1):14. https://doi.org/10.3390/sports11010014
Chicago/Turabian StyleDriller, Matthew W., Ian C. Dunican, Shauni E. T. Omond, Omar Boukhris, Shauna Stevenson, Kari Lambing, and Amy M. Bender. 2023. "Pyjamas, Polysomnography and Professional Athletes: The Role of Sleep Tracking Technology in Sport" Sports 11, no. 1: 14. https://doi.org/10.3390/sports11010014