
Effects of Exercise Frequency with Complex Contrast Training on Measures of Physical Fitness in Active Adult Males

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
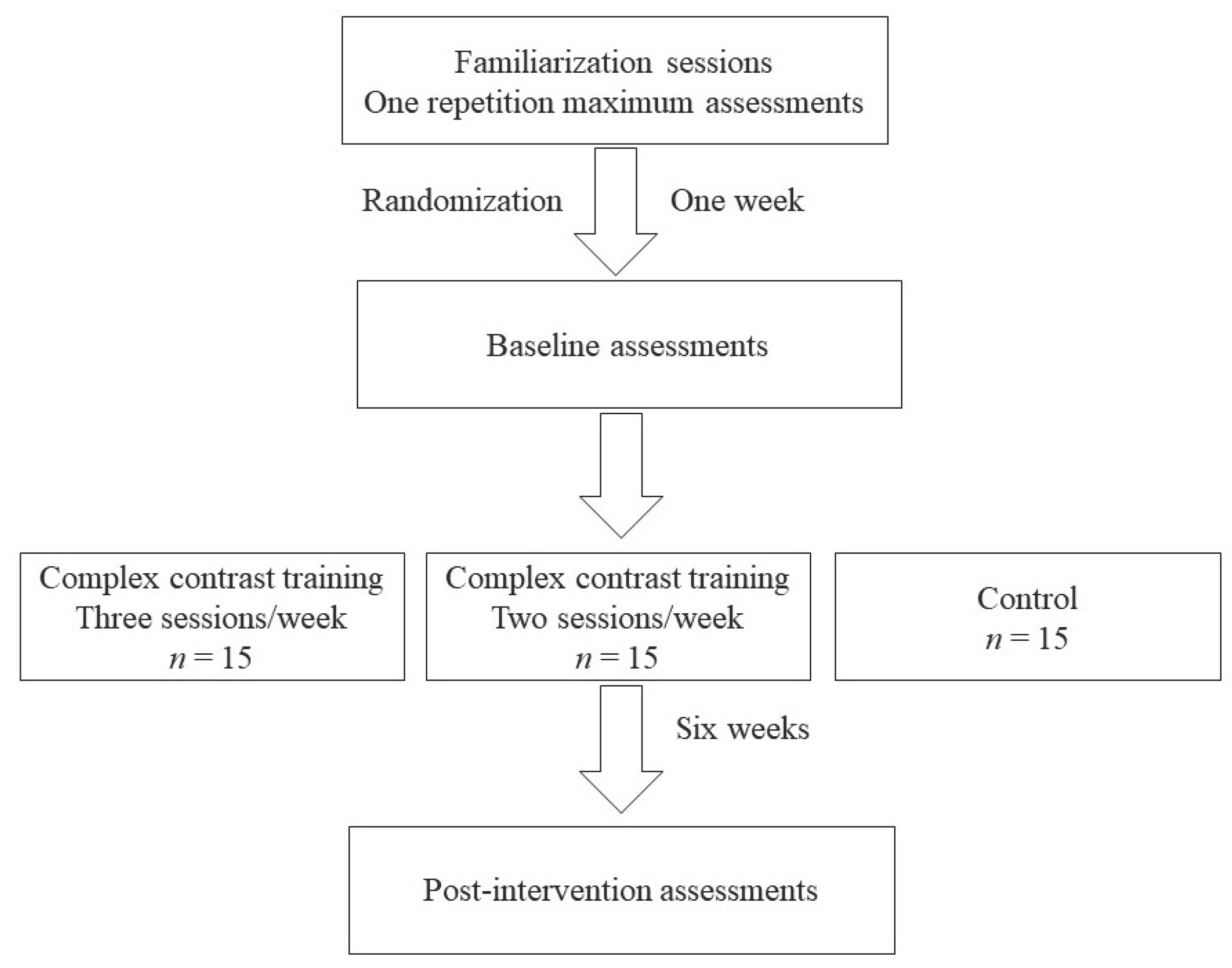
2.1. Experimental Design
2.2. Participants
2.3. Load Measurement for Training Prescription
2.4. Training Intervention
2.5. Physical Fitness Tests
2.5.1. Speed
2.5.2. Upper Limb Muscle Power
2.5.3. Lower Limb Muscle Power
2.5.4. Change-of-Direction Speed
2.5.5. Muscle Strength
2.6. Statistical Analysis
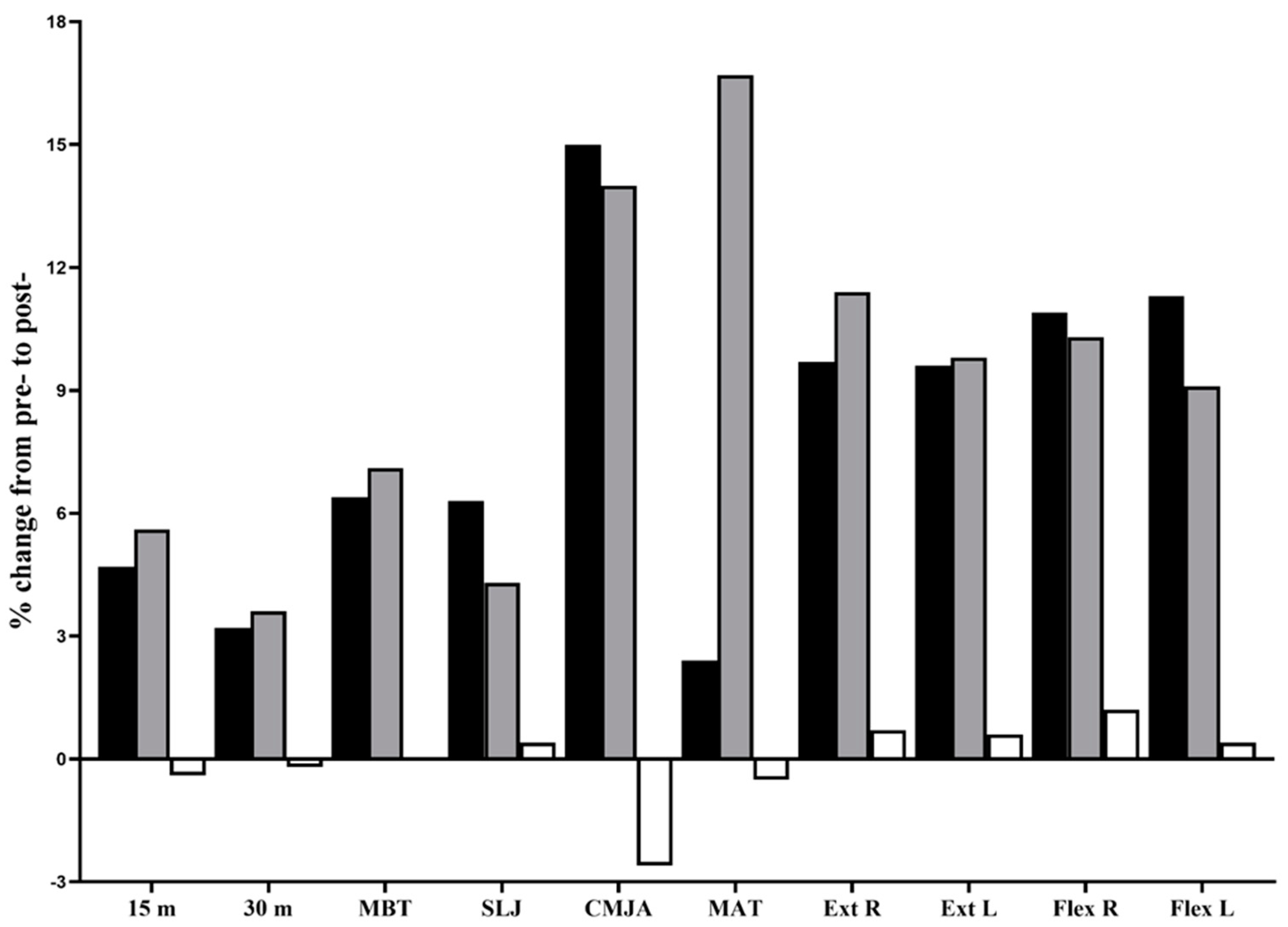
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Farley, J.B.; Stein, J.; Keogh, J.W.L.; Woods, C.T.; Milne, N. The relationship between physical fitness qualities and sport-specific technical skills in female, team-based ball players: A systematic review. Sports Med. Open 2020, 6, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sortwell, A.; Behringer, M.; Granacher, U.; Trimble, K.; Forte, P.; Neiva, H.; Clemente-Suárez, V.; Ramirez-Campillo, R.; Konukman, F.; Tufekcioglu, E.; et al. Advancing Sports Science and Physical Education Research Through a Shared Understanding of the Term Motor Performance Skills: A Scoping Review with Content Analysis. Int. J. Kinesiol. Sports Sci. 2022, 10, 18–27. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Liguori, G.; Feiro, Y.; Fountaine, C.; Roy, B.A. ACSM’s Guidelines for Exercise Testing and Prescription, 11th ed.; Wolters Kluwer Health: Philadelphia, PA, USA, 2021. [Google Scholar]
- Caspersen, C.J.; Powell, K.E.; Christenson, G.M. Physical activity, exercise, and physical fitness: Definitions and distinctions for health-related research. Public Health Rep. 1985, 100, 126–131. [Google Scholar]
- Ramirez-Campillo, R.; Moran, J.; Chaabene, H.; Granacher, U.; Behm, D.G.; García-Hermoso, A.; Izquierdo, M. Methodological characteristics and future directions for plyometric jump training research: A scoping review update. Scand. J. Med. Sci. Sport. 2020, 30, 983–997. [Google Scholar] [CrossRef]
- Vieira, A.F.; Umpierre, D.; Teodoro, J.L.; Lisboa, S.C.; Baroni, B.M.; Izquierdo, M.; Cadore, E.L. Effects of resistance training performed to failure or not to failure on muscle strength, hypertrophy, and power output: A systematic review with meta-analysis. J. Strength Cond. Res. 2021, 35, 1165–1175. [Google Scholar] [CrossRef]
- Cormier, P.; Freitas, T.T.; Loturco, I.; Turner, A.; Virgile, A.; Haff, G.G.; Blazevich, A.J.; Agar-Newman, D.; Henneberry, M.; Baker, D.G.; et al. Within session exercise sequencing during programming for complex training: Historical perspectives, terminology, and training considerations. Sports Med. 2022, 52, 2371–2389. [Google Scholar] [CrossRef]
- Turner, A.N.; Comfort, P.; McMahon, J.; Bishop, C.; Chavda, S.; Read, P.; Mundy, P.; Lake, J. Developing powerful athletes, part 1: Mechanical underpinnings. Strength Cond. J. 2020, 42, 30–39. [Google Scholar] [CrossRef]
- Case, M.J.; Knudson, D.V.; Downey, D.L. Barbell squat relative strength as an identifier for lower extremity injury in collegiate athletes. J. Strength Cond. Res. 2020, 34, 1249–1253. [Google Scholar] [CrossRef]
- Haff, G.G.; Nimphius, S. Training principles for power. Strength Cond. J. 2012, 34, 2–12. [Google Scholar] [CrossRef] [Green Version]
- Thapa, R.K.; Lum, D.; Moran, J.; Ramirez-Campillo, R. Effects of complex training on sprint, jump, and change of direction ability of soccer players: A systematic review and meta-analysis. Front. Psychol. 2021, 11, 627869. [Google Scholar] [CrossRef] [PubMed]
- Thapa, R.K.; Narvariya, P.; Weldon, A.; Talukdar, K.; Ramirez-Campillo, R. Can complex contrast training interventions improve aerobic endurance, maximal strength, and repeated sprint ability in soccer players? A systematic review and meta-analysis. Montenegrin J. Sports Sci. Med. 2022, 11, 45–55. [Google Scholar] [CrossRef]
- Juárez, D.; González-Ravé, J.M.; Navarro, F. Effects of complex vs non complex training programs on lower body maximum strength and power. Isokinet. Exerc. Sci. 2009, 17, 233–241. [Google Scholar] [CrossRef]
- Stasinaki, A.N.; Gloumis, G.; Spengos, K.; Blazevich, A.J.; Zaras, N.; Georgiadis, G.; Karampatsos, G.; Terzis, G. Muscle strength, power, and morphologic adaptations after 6 weeks of compound vs. complex training in healthy men. J. Strength Cond. Res. 2015, 29, 2559–2569. [Google Scholar] [CrossRef]
- Alemdaroğlu, U.; Dündar, U.; Köklü, Y.; Aşci, A.; Findikoğlu, G. The effect of exercise order incorporating plyometric and resistance training on isokinetic leg strength and vertical jump performance: A comparative study. Isokinet. Exerc. Sci. 2013, 21, 211–217. [Google Scholar] [CrossRef] [Green Version]
- Hammami, M.; Gaamouri, N.; Cherni, Y.; Gaied, S.; Chelly, M.S.; Hill, L.; Nikolaidis, P.T.; Knechtle, B. Effects of complex strength training with elastic band program on repeated change of direction in young female handball players: Randomized control trial. Int. J. Sports Sci. Coach 2022, 7, 1396–1407. [Google Scholar] [CrossRef]
- Blazevich, A.J.; Babault, N. Post-activation potentiation versus post-activation performance enhancement in humans: Historical perspective, underlying mechanisms, and current issues. Front. Physiol. 2019, 10, 1359. [Google Scholar] [CrossRef] [Green Version]
- Thapa, R.K.; Kumar, A.; Kumar, G.; Narvariya, P. A combination of ballistic exercises with slow and fast stretch-shortening cycle induces post-activation performance enhancement. Trends Sport. Sci. 2020, 27, 203–211. [Google Scholar] [CrossRef]
- Phillips, S.M.; Tipton, K.D.; Aarsland, A.; Wolf, S.E.; Wolfe, R.R. Mixed muscle protein synthesis and breakdown after resistance exercise in humans. Am. J. Physiol. 1997, 273, E99–E107. [Google Scholar] [CrossRef]
- Damas, F.; Angleri, V.; Phillips, S.M.; Witard, O.C.; Ugrinowitsch, C.; Santanielo, N.; Soligon, S.D.; Costa, L.A.R.; Lixandrão, M.E.; Conceição, M.S.; et al. Myofibrillar protein synthesis and muscle hypertrophy individualized responses to systematically changing resistance training variables in trained young men. J. Appl. Physiol. 2019, 127, 806–815. [Google Scholar] [CrossRef]
- Dankel, S.J.; Mattocks, K.T.; Jessee, M.B.; Buckner, S.L.; Mouser, J.G.; Counts, B.R.; Laurentino, G.C.; Loenneke, J.P. Frequency: The overlooked resistance training variable for inducing muscle hypertrophy? Sports Med. 2017, 47, 799–805. [Google Scholar] [CrossRef] [PubMed]
- Erickson, C.R.; Vukovich, M.D. Osteogenic index and changes in bone markers during a jump training program: A pilot study. Med. Sci. Sport. Exerc. 2010, 42, 1485–1492. [Google Scholar] [CrossRef] [PubMed]
- Pareja-Blanco, F.; Rodríguez-Rosell, D.; Aagaard, P.; Sánchez-Medina, L.; Ribas-Serna, J.; Mora-Custodio, R.; Otero-Esquina, C.; Yáñez-García, J.M.; González-Badillo, J.J. Time course of recovery from resistance exercise with different set configurations. J. Strength Cond. Res. 2020, 34, 2867–2876. [Google Scholar] [CrossRef]
- Shea, C.H.; Lai, Q.; Black, C.; Park, J.-H. Spacing practice sessions across days benefits the learning of motor skills. Hum. Mov. Sci. 2000, 19, 737–760. [Google Scholar] [CrossRef]
- Grgic, J.; Schoenfeld, B.J.; Davies, T.B.; Lazinica, B.; Krieger, J.W.; Pedisic, Z. Effect of resistance training frequency on gains in muscular strength: A systematic review and meta-analysis. Sports Med 2018, 48, 1207–1220. [Google Scholar] [CrossRef] [PubMed]
- Ramirez-Campillo, R.; Moran, J.; Oliver, J.L.; Pedley, J.S.; Lloyd, R.S.; Granacher, U. Programming plyometric-jump training in soccer: A review. Sports 2022, 10, 94. [Google Scholar] [CrossRef]
- Begg, C.; Cho, M.; Eastwood, S.; Horton, R.; Moher, D.; Olkin, I.; Pitkin, R.; Rennie, D.; Schulz, K.F.; Simel, D.; et al. Improving the quality of reporting of randomized controlled trials. The CONSORT statement. JAMA 1996, 276, 637–639. [Google Scholar] [CrossRef] [PubMed]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [Green Version]
- Smart, N.A.; Waldron, M.; Ismail, H.; Giallauria, F.; Vigorito, C.; Cornelissen, V.; Dieberg, G. Validation of a new tool for the assessment of study quality and reporting in exercise training studies: TESTEX. Int. J. Evid. Based Healthc. 2015, 13, 9–18. [Google Scholar] [CrossRef]
- Faude, O.; Roth, R.; Di Giovine, D.; Zahner, L.; Donath, L. Combined strength and power training in high-level amateur football during the competitive season: A randomised-controlled trial. J. Sports Sci. 2013, 31, 1460–1467. [Google Scholar] [CrossRef]
- Singh, G.; Kushwah, G.S.; Singh, T.; Thapa, R.K.; Granacher, U.; Ramirez-Campillo, R. Effects of sand-based plyometric-jump training in combination with endurance running on outdoor or treadmill surface on physical fitness in young adult males. J. Sports Sci. Med. 2022, 21, 277–286. [Google Scholar] [CrossRef] [PubMed]
- Stockbrugger, B.A.; Haennel, R.G. Validity and reliability of a medicine ball explosive power test. J. Strength Cond. Res. 2001, 15, 431–438. [Google Scholar] [PubMed]
- Singh, G.; Kushwah, G.; Singh, T.; Ramirez-Campillo, R.; Thapa, R.K. Effects of six weeks outdoor versus treadmill running on physical fitness and body composition in recreationally active young males: A pilot study. PeerJ 2022, 10, e13791. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, MI, USA, 1988. [Google Scholar]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Macaluso, F.; Isaacs, A.W.; Myburgh, K.H. Preferential type II muscle fiber damage from plyometric exercise. J. Athl. Train. 2012, 47, 414–420. [Google Scholar] [CrossRef] [Green Version]
- Ali, K.; Verma, S.; Ahmad, I.; Singla, D.; Saleem, M.; Hussain, M.E. Comparison of complex versus contrast training on steroid hormones and sports performance in male soccer players. J. Chiropr. Med. 2019, 18, 131–138. [Google Scholar] [CrossRef]
- Hammami, M.; Negra, Y.; Shephard, R.J.; Chelly, M.S. The effect of standard strength vs. contrast strength training on the development of sprint, agility, repeated change of direction, and jump in junior male soccer players. J. Strength Cond. Res. 2017, 31, 901–912. [Google Scholar] [CrossRef]
- Cormier, P.; Freitas, T.T.; Rubio-Arias, J.; Alcaraz, P.E. Complex and contrast training: Does strength and power training sequence affect performance-based adaptations in team sports? a systematic review and meta-analysis. J. Strength Cond. Res. 2020, 34, 1461–1479. [Google Scholar] [CrossRef]
- Sale, D.G. Influence of exercise and training on motor unit activation. Exerc. Sport Sci. Rev. 1987, 15, 95–151. [Google Scholar] [CrossRef]
- Hamarsland, H.; Moen, H.; Skaar, O.J.; Jorang, P.W.; Rødahl, H.S.; Rønnestad, B.R. Equal-volume strength training with different training frequencies induces similar muscle hypertrophy and strength improvement in trained participants. Front. Physiol. 2021, 12, 789403. [Google Scholar] [CrossRef] [PubMed]
- Ralston, G.W.; Kilgore, L.; Wyatt, F.B.; Buchan, D.; Baker, J.S. Weekly training frequency effects on strength gain: A meta-analysis. Sports Med. Open 2018, 4, 36. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| CCT-2 (n = 15) | CCT-3 (n = 15) | CG (n = 15) | p-Value | |
|---|---|---|---|---|
| Age (yrs) | 21.9 ± 2.3 | 21.1 ± 1.9 | 21.3 ± 1.8 | 0.494 |
| Body height (cm) | 177.1 ± 7.5 | 171.9 ± 8.2 | 172.5 ± 5.8 | 0.112 |
| Body mass (kg) | 69.4 ± 7.6 | 62.7 ± 7.1 | 67.0 ± 5.0 | 0.028 |
| CCT-2 | CCT-3 | p-Value | |
|---|---|---|---|
| Squat 1-RM | 107.0 ± 17.6 | 100.3 ± 11.3 | 0.227 |
| Squat relative 1-RM | 1.55 ± 0.22 | 1.62 ± 0.23 | 0.414 |
| Lunge 1-RM | 63.7 ± 14.7 | 58.0 ± 8.6 | 0.208 |
| Lunge relative 1-RM | 0.92 ± 0.19 | 0.93 ± 0.16 | 0.840 |
| Romanian deadlift 1-RM | 89.0 ± 19.6 | 83.7 ± 12.2 | 0.378 |
| Romanian deadlift relative 1-RM | 1.28 ± 0.23 | 1.35 ± 0.22 | 0.421 |
| Bench press 1-RM | 73.0 ± 12.4 | 67.3 ± 10.8 | 0.193 |
| Bench press relative 1-RM | 1.05 ± 0.15 | 1.08 ± 0.18 | 0.648 |
| High-Load Low-Velocity Exercises | Low-Load High-Velocity Exercises | |||
|---|---|---|---|---|
| Exercise | Repetitions per Set * | Exercise | Repetitions per Set | |
| Weeks 1–2 | Squat | 15 | Squat jump | 6 |
| 65% 1 RM | Romanian deadlift | 15 | Kettlebell swing | 10 |
| Barbell lunge | 15 | Barbell high knees | 15 s | |
| Bench press | 15 | Plyo push-up | 6 | |
| Weeks 3–4 | Squat | 10 | Squat jump | 8 |
| 75% 1 RM | Romanian deadlift | 10 | Kettlebell swing | 10 |
| Barbell lunge | 10 | Barbell high knees | 20 s | |
| Bench press | 10 | Plyo push-up | 8 | |
| Weeks 5–6 | Squat | 6 | Squat jump | 10 |
| 85% 1 RM | Romanian deadlift | 6 | Kettlebell swing | 10 |
| Barbell lunge | 6 | Barbell high knees | 25 s | |
| Bench press | 6 | Plyo push-up | 10 | |
| Complex Contrast Training Group (n = 15; 2 Sessions/Week) (CCT-2) | Complex Contrast Training Group (n = 15; 3 Sessions/Week) (CCT-3) | Active Control Group (CG) (n = 15) | Time × Group | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Pre-Test | Post-Test | p-Value (g) Magnitude | Pre-Test | Post-Test | p-Value (g) Magnitude | Pre-Test | Post-Test | p-Value (g) Magnitude | p-Value (ɳp2) | |
| Mean ± Standard Deviation | Mean ± Standard Deviation | Mean ± Standard Deviation | ||||||||
| Speed | ||||||||||
| 15 m sprint (s) | 2.74 ± 0.14 | 2.61 ± 0.12 | <0.001 (0.97) Moderate | 2.88 ± 0.12 | 2.72 ± 0.11 | <0.001 (1.35) Large | 2.80 ± 0.2 | 2.81 ± 0.19 | 0.697 (0.05) Trivial | <0.001 (0.52) Large |
| 30 m sprint (s) | 4.68 ± 0.23 | 4.53 ± 0.22 | <0.001 (0.65) Moderate | 4.77 ± 0.18 | 4.60 ± 0.20 | <0.001 (0.87) Moderate | 4.61 ± 0.30 | 4.62 ± 0.25 | 0.582 (0.04) Trivial | <0.001 (0.57) Large |
| Muscle Power | ||||||||||
| Medicine ball throw | 11.7 ± 1.5 | 12.4 ± 1.5 | <0.001 (0.49) Small | 10.1 ± 1.3 | 10.8 ± 1.4 | <0.001 (0.52) Small | 10.9 ± 1.4 | 10.9 ± 1.2 | 0.942 (0.00) Trivial | <0.001 (0.51) Large |
| Standing long jump (m) | 2.4 ± 0.1 | 2.6 ± 0.1 | <0.001 (1.12) Moderate | 2.4 ± 0.2 | 2.5 ± 0.2 | <0.001 (0.63) Small | 2.3 ± 0.2 | 2.3 ± 0.2 | 0.86 (0.05) Trivial | <0.001 (0.54) Large |
| CMJ with arm thrust (cm) | 44.5 ± 3.9 | 51.2 ± 4.2 | <0.001 (1.61) Large | 38.0 ± 4.1 | 43.4 ± 5.6 | <0.001 (1.06) Moderate | 37.5 ± 4.3 | 36.5 ± 3.4 | 0.104 (0.20) Small | <0.001 (0.70) Large |
| Change-of-direction speed | ||||||||||
| Modified agility T-test (s) | 5.84 ± 0.20 | 5.70 ± 0.19 | <0.001 (0.70) Moderate | 6.39 ± 0.26 | 5.32 ± 0.37 | <0.001 (3.26) Very large | 6.11 ± 0.32 | 6.14 ± 0.3 | 0.729 (0.09) Trivial | <0.001 (0.78) Large |
| Muscle strength | ||||||||||
| PT knee extension (right) (N.m) | 168.9 ± 23 | 185.3 ± 27.3 | <0.001 (0.63) Small | 160.8 ± 58.4 | 179.1 ± 59 | <0.001 (0.30) Small | 177.7 ± 43.1 | 178.9 ± 42.5 | 0.413 (0.03) Trivial | <0.001 (0.69) Large |
| PT knee extension (left) (N.m) | 170.0 ± 28.1 | 186.3 ± 30.4 | <0.001 (0.54) Small | 170.3 ± 57.4 | 187 ± 59.2 | <0.001 (0.28) Small | 181.7 ± 38 | 182.7 ± 37.9 | 0.407 (0.03) Trivial | <0.001 (0.73) Large |
| PT knee flexion (right) (N.m) | 110.1 ± 26.4 | 122.1 ± 27.4 | <0.001 (0.43) Small | 102.1 ± 25.9 | 112.6 ± 28.8 | <0.001 (0.37) Small | 102.5 ± 26.6 | 103.7 ± 26.1 | 0.251 (0.04) Trivial | <0.001 (0.63) Large |
| PT knee flexion (left) (N.m) | 103.9 ± 20.6 | 115.6 ± 22.8 | <0.001 (0.52) Small | 100.9 ± 25.4 | 110.1 ± 26.1 | <0.001 (0.35) Small | 99.5 ± 23.2 | 99.9 ± 22.4 | 0.676 (0.02) Trivial | <0.001 (0.65) Large |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kumar, G.; Pandey, V.; Thapa, R.K.; Weldon, A.; Granacher, U.; Ramirez-Campillo, R. Effects of Exercise Frequency with Complex Contrast Training on Measures of Physical Fitness in Active Adult Males. Sports 2023, 11, 11. https://doi.org/10.3390/sports11010011
Kumar G, Pandey V, Thapa RK, Weldon A, Granacher U, Ramirez-Campillo R. Effects of Exercise Frequency with Complex Contrast Training on Measures of Physical Fitness in Active Adult Males. Sports. 2023; 11(1):11. https://doi.org/10.3390/sports11010011
Chicago/Turabian StyleKumar, Gopal, Vivek Pandey, Rohit K. Thapa, Anthony Weldon, Urs Granacher, and Rodrigo Ramirez-Campillo. 2023. "Effects of Exercise Frequency with Complex Contrast Training on Measures of Physical Fitness in Active Adult Males" Sports 11, no. 1: 11. https://doi.org/10.3390/sports11010011