Barriers and Facilitators to Genetic Testing for Familial Hypercholesterolemia in the United States: A Review


Abstract
:1. Introduction
2. Methods
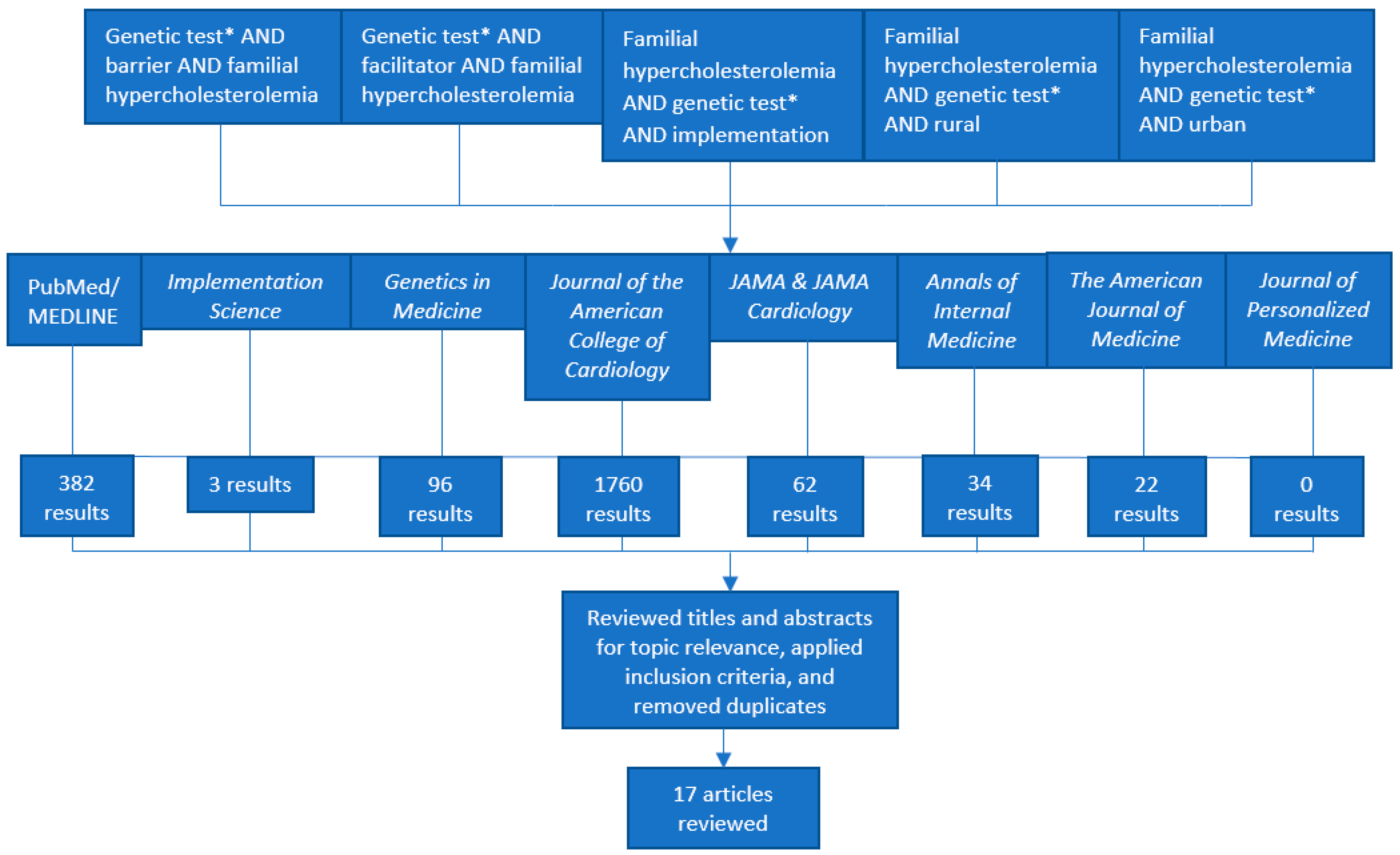
2.1. Search Strategy, Literature Selection, and Inclusion Criteria
2.2. Choice of Implementation Framework
2.3. Information Extraction
2.4. Analysis of Barriers and Facilitators
3. Results
3.1. CFIR Domain #1: Characteristics of Intervention
3.2. CFIR Domain #2: Outer Setting
3.3. CFIR Domain #3: Inner Setting
3.4. CFIR Domain #4: Characteristics of Individuals
3.5. CFIR Domain #5: Process
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Knowles, J.W.; Rader, D.J.; Khoury, M.J. Cascade Screening for Familial Hypercholesterolemia and the Use of Genetic Testing. JAMA 2017, 318, 381–382. [Google Scholar] [CrossRef] [PubMed]
- Knowles, J.W.; Stone, N.J.; Ballantyne, C.M. Familial Hypercholesterolemia and the 2013 American College of Cardiology/American Heart Association Guidelines: Myths, Oversimplification, and Misinterpretation Versus Facts. Am. J. Cardiol. 2015, 116, 481–484. [Google Scholar] [CrossRef] [PubMed]
- De Ferranti, S.D.; Rodday, A.M.; Mendelson, M.M.; Wong, J.B.; Leslie, L.K.; Sheldrick, R.C. Prevalence of Familial Hypercholesterolemia in the 1999 to 2012 United States National Health and Nutrition Examination Surveys (NHANES)CLINICAL PERSPECTIVE. Circulation 2016, 133, 1067–1072. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, A.C.; Hopkins, P.N.; Toth, P.P.; Ballantyne, C.M.; Rader, D.J.; Robinson, J.G.; Daniels, S.R.; Gidding, S.S.; de Ferranti, S.D.; Ito, M.K.; et al. Familial Hypercholesterolemia: Screening, diagnosis and management of pediatric and adult patients: Clinical guidance from the National Lipid Association Expert Panel on Familial Hypercholesterolemia. J. Clin. Lipidol. 2011, 5, S1–S8. [Google Scholar] [CrossRef] [PubMed]
- Yuan, G.; Wang, J.; Hegele, R.A. Heterozygous familial hypercholesterolemia: An underrecognized cause of early cardiovascular disease. CMAJ 2006, 174, 1124–1129. [Google Scholar] [CrossRef] [PubMed]
- Heart Disease Facts & Statistics. cdc.gov. Available online: https://www.cdc.gov/heartdisease/facts.htm (accessed on 31 May 2019).
- Akioyamen, L.E.; Genest, J.; Shan, S.D.; Reel, R.L.; Albaum, J.M.; Chu, A.; Tu, J.V. Estimating the prevalence of heterozygous familial hypercholesterolaemia: A systematic review and meta-analysis. BMJ Open 2017, 7, e016461. [Google Scholar] [CrossRef] [PubMed]
- Abul-Husn, N.S.; Manickam, K.; Jones, L.K.; Wright, E.A.; Hartzel, D.N.; Gonzaga-Jauregui, C.; O’Dushlaine, C.; Leader, J.B.; Kirchner, H.L.; Lindbuchler, D.M.; et al. Genetic identification of familial hypercholesterolemia within a single U.S. health care system. Science 2016, 354, aaf7000. [Google Scholar] [CrossRef] [PubMed]
- Sturm, A.C.; Knowles, J.W.; Gidding, S.S.; Ahmad, Z.S.; Ahmed, C.D.; Ballantyne, C.M.; Baum, S.J.; Bourbon, M.; Carrié, A.; Cuchel, M.; et al. Clinical Genetic Testing for Familial Hypercholesterolemia: JACC Scientific Expert Panel. J. Am. Coll. Cardiol. 2018, 72, 662–680. [Google Scholar] [CrossRef]
- Cirino, A.L.; Harris, S.; Lakdawala, N.K.; Michels, M.; Olivotto, I.; Day, S.M.; Abrams, D.J.; Charron, P.; Caleshu, C.; Semsarian, C.; et al. Role of Genetic Testing in Inherited Cardiovascular Disease: A Review. JAMA Cardiol. 2017, 2, 1153–1160. [Google Scholar] [CrossRef]
- Minicocci, I.; Pozzessere, S.; Prisco, C.; Montali, A.; di Costanzo, A.; Martino, E.; Martino, F.; Arca, M. Analysis of Children and Adolescents with Familial Hypercholesterolemia. J. Pediatrics 2017, 183, 100–107.e3. [Google Scholar] [CrossRef]
- Setia, N.; Saxena, R.; Sawhney, J.P.S.; Verma, I.C. Familial Hypercholesterolemia: Cascade Screening in Children and Relatives of the Affected. Indian J. Pediatr. 2018, 85, 339–343. [Google Scholar] [CrossRef] [PubMed]
- Séguro, F.; Rabès, J.-P.; Taraszkiewicz, D.; Ruidavets, J.-B.; Bongard, V.; Ferrières, J. Genetic diagnosis of familial hypercholesterolemia is associated with a premature and high coronary heart disease risk. Clin. Cardiol. 2018, 41, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Vohnout, B.; Gabcova, D.; Huckova, M.; Klimes, I.; Gasperikova, D.; Raslova, K. Genetic testing of familial hypercholesterolemia in a real clinical setting. Wien Klin. Wochenschr. 2016, 128, 916–921. [Google Scholar] [CrossRef] [PubMed]
- Amor-Salamanca, A.; Castillo, S.; Gonzalez-Vioque, E.; Dominguez, F.; Quintana, L.; Lluís-Ganella, C.; Escudier, J.M.; Ortega, J.; Lara-Pezzi, E.; Alonso-Pulpon, L.; et al. Genetically Confirmed Familial Hypercholesterolemia in Patients with Acute Coronary Syndrome. J. Am. Coll. Cardiol. 2017, 70, 1732–1740. [Google Scholar] [CrossRef] [PubMed]
- Sperlongano, S.; Gragnano, F.; Natale, F.; D’Erasmo, L.; Concilio, C.; Cesaro, A.; Golia, E.; Crisci, M.; Sperlongano, R.; Fimiani, F.; et al. Lomitapide in homozygous familial hypercholesterolemia: Cardiology perspective from a single-center experience. J. Cardiovasc. Med. 2018, 19, 83. [Google Scholar] [CrossRef] [PubMed]
- Pang, J.; Martin, A.C.; Bates, T.R.; Hooper, A.J.; Bell, D.A.; Burnett, J.R.; Norman, R.; Watts, G.F. Parent–child genetic testing for familial hypercholesterolaemia in an Australian context. J. Paediatr. Child Health 2018, 54, 741–747. [Google Scholar] [CrossRef]
- Wu, X.; Pang, J.; Wang, X.; Peng, J.; Chen, Y.; Wang, S.; Watts, G.F.; Lin, J. Reverse cascade screening for familial hypercholesterolemia in high-risk Chinese families. Clin. Cardiol. 2017, 40, 1169–1173. [Google Scholar] [CrossRef] [Green Version]
- Averna, M.; Cefalù, A.B.; Casula, M.; Noto, D.; Arca, M.; Bertolini, S.; Calandra, S.; Catapano, A.L.; Tarugi, P. Familial hypercholesterolemia: The Italian Atherosclerosis Society Network (LIPIGEN). Atheroscler. Suppl. 2017, 29, 11–16. [Google Scholar] [CrossRef]
- Jones, L.K.; Rahm, A.K.; Manickam, K.; Butry, L.; Lazzeri, A.; Corcoran, T.; Komar, D.; Josyula, N.S.; Pendergrass, S.A.; Sturm, A.C.; et al. Healthcare Utilization and Patients’ Perspectives After Receiving a Positive Genetic Test for Familial Hypercholesterolemia. Circ. Genom. Precis. Med. 2018, 11, e002146. [Google Scholar] [CrossRef]
- Stimulating Implementation Science in Genomics and Precision Medicine for Heart, Lung, Blood and Sleep Diseases: The Case of Familial Hypercholesterolemia. Blogs|CDC. Available online: https://blogs.cdc.gov/genomics/2018/06/05/stimulating-implementation/ (accessed on 28 September 2018).
- Roberts, M.C.; Mensah, G.A.; Khoury, M.J. Leveraging Implementation Science to Address Health Disparities in Genomic Medicine: Examples from the Field. Ethn. Dis. 2019, 29, 187–192. [Google Scholar] [CrossRef]
- FH 1|Tier 1 Genomic Applications Toolkit for Public Health Departments. Genomics|CDC. Available online: https://www.cdc.gov/genomics/implementation/toolkit/fh_1.htm (accessed on 21 October 2018).
- Tier1|Tier 1 Genomic Applications Toolkit for Public Health Departments. Genomics|CDC. Available online: https://www.cdc.gov/genomics/implementation/toolkit/tier1.htm (accessed on 21 October 2018).
- Hendricks-Sturrup, R.M.; Lu, C.Y. Understanding Implementation Challenges to Genetic Testing for Familial Hypercholesterolemia in the United States. J. Pers. Med. 2019, 9, 9. [Google Scholar] [CrossRef] [PubMed]
- Feature|Familial Hypercholesterolemia: Clinician and Patient Insights. Available online: https://www.acc.org/latest-in-cardiology/articles/2018/10/14/12/42/feature-familial-hypercholesterolemia-clinician-and-patient-insights (accessed on 30 November 2018).
- Delikurt, T.; Williamson, G.R.; Anastasiadou, V.; Skirton, H. A systematic review of factors that act as barriers to patient referral to genetic services. Eur. J. Hum. Genet. 2015, 23, 739–745. [Google Scholar] [CrossRef] [PubMed]
- George, R.; Kovak, K.; Cox, S.L. Aligning policy to promote cascade genetic screening for prevention and early diagnosis of heritable diseases. J. Genet. Couns. 2015, 24, 388–399. [Google Scholar] [CrossRef] [PubMed]
- Sturm, A.C. Cardiovascular Cascade Genetic Testing: Exploring the Role of Direct Contact and Technology. Front. Cardiovasc. Med. 2016, 3, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, C.Y.; Loomer, S.; Ceccarelli, R.; Mazor, K.M.; Sabin, J.; Clayton, E.W.; Ginsburg, G.S.; Wu, A.C. Insurance Coverage Policies for Pharmacogenomic and Multi-Gene Testing for Cancer. J. Pers. Med. 2018, 8, 19. [Google Scholar] [CrossRef] [PubMed]
- Prince, A.E.R. Prevention for those who can pay: Insurance reimbursement of genetic-based preventive interventions in the liminal state between health and disease. J. Law Biosci. 2015, 2, 365–395. [Google Scholar] [CrossRef] [PubMed]
- Literature Search: Databases and Gray Literature. NIH Library. Available online: https://www.nihlibrary.nih.gov/services/systematic-review-service/literature-search-databases-and-gray-literature (accessed on 31 May 2019).
- Rahm, A.K.; Cragun, D.; Hunter, J.E.; Epstein, M.M.; Lowery, J.; Lu, C.Y.; Pawloski, P.A.; Sharaf, R.N.; Liang, S.-Y.; Burnett-Hartman, A.N.; et al. Implementing universal Lynch syndrome screening (IMPULSS): Protocol for a multi-site study to identify strategies to implement, adapt, and sustain genomic medicine programs in different organizational contexts. BMC Health Serv. Res. 2018, 18, 824. [Google Scholar] [CrossRef] [PubMed]
- Orlando, L.A.; Sperber, N.R.; Voils, C.; Nichols, M.; Myers, R.A.; Wu, R.R.; Rakhra-Burris, T.; Levy, K.D.; Levy, M.; Pollin, T.I.; et al. Developing a Common Framework for Evaluating the Implementation of Genomic Medicine Interventions in Clinical Care: The IGNITE Network’s Common Measures Working Group. Genet. Med. 2018, 20, 655–663. [Google Scholar] [CrossRef]
- Sperber, N.R.; Carpenter, J.S.; Cavallari, L.H.; Damschroder, L.J.; Cooper-DeHoff, R.M.; Denny, J.C.; Ginsburg, G.S.; Guan, Y.; Horowitz, C.R.; Levy, K.D.; et al. Challenges and strategies for implementing genomic services in diverse settings: Experiences from the Implementing GeNomics In pracTicE (IGNITE) network. BMC Med. Genom. 2017, 10, 35. [Google Scholar] [CrossRef]
- Levy, K.D.; Blake, K.; Fletcher-Hoppe, C.; Franciosi, J.; Goto, D.; Hicks, J.K.; Holmes, A.M.; Kanuri, S.H.; Madden, E.B.; Musty, M.D.; et al. Opportunities to implement a sustainable genomic medicine program: Lessons learned from the IGNITE Network. Genet. Med. 2019, 21, 743. [Google Scholar] [CrossRef]
- Birken, S.A.; Powell, B.J.; Shea, C.M.; Haines, E.R.; Alexis Kirk, M.; Leeman, J.; Rohweder, C.; Damschroder, L.; Presseau, J. Criteria for selecting implementation science theories and frameworks: Results from an international survey. Implement. Sci. 2017, 12, 124. [Google Scholar] [CrossRef] [PubMed]
- Kirk, M.A.; Kelley, C.; Yankey, N.; Birken, S.A.; Abadie, B.; Damschroder, L. A systematic review of the use of the Consolidated Framework for Implementation Research. Implement. Sci. 2016, 11, 72. [Google Scholar] [CrossRef] [PubMed]
- Giudicessi, J.R.; Kullo, I.J.; Ackerman, M.J. Precision Cardiovascular Medicine: State of Genetic Testing. Mayo Clin. Proc. 2017, 92, 642–662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarraju, A.; Knowles, J.W. Genetic Testing and Risk Scores: Impact on Familial Hypercholesterolemia. Front. Cardiovasc. Med. 2019, 6. [Google Scholar] [CrossRef] [PubMed]
- Safarova, M.S.; Kullo, I.J. Lessening the Burden of Familial Hypercholesterolemia Using Health Information Technology. Circ. Res. 2018, 122, 26–27. [Google Scholar] [CrossRef] [PubMed]
- Migliara, G.; Baccolini, V.; Rosso, A.; D’Andrea, E.; Massimi, A.; Villari, P.; De Vito, C. Familial Hypercholesterolemia: A Systematic Review of Guidelines on Genetic Testing and Patient Management. Front. Public Health 2017, 5, 252. [Google Scholar] [CrossRef] [PubMed]
- Campbell, M.; Humanki, J.; Zierhut, H. A novel approach to screening for familial hypercholesterolemia in a large public venue. J. Community Genet. 2017, 8, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Khoury, M.J.; Bowen, M.S.; Clyne, M.; Dotson, W.D.; Gwinn, M.L.; Green, R.F.; Kolor, K.; Rodriguez, J.L.; Wulf, A.; Yu, W. From public health genomics to precision public health: A 20-year journey. Genet. Med. 2018, 20, 574–582. [Google Scholar] [CrossRef]
- Mues, K.E.; Bogdanov, A.N.; Monda, K.L.; Yedigarova, L.; Liede, A.; Kallenbach, L. How well can familial hypercholesterolemia be identified in an electronic health record database? Clin. Epidemiol. 2018, 10, 1667–1677. [Google Scholar] [CrossRef]
- Hasnie, A.A.; Kumbamu, A.; Safarova, M.S.; Caraballo, P.J.; Kullo, I.J. A Clinical Decision Support Tool for Familial Hypercholesterolemia Based on Physician Input. Mayo Clin. Proc. Innov. Qual. Outcomes 2018, 2, 103–112. [Google Scholar] [CrossRef]
- Knowles, J.W.; O’Brien, E.C.; Greendale, K.; Wilemon, K.; Genest, J.; Sperling, L.S.; Neal, W.A.; Rader, D.J.; Khoury, M.J. Reducing the burden of disease and death from familial hypercholesterolemia: A call to action. Am. Heart J. 2014, 168, 807–811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Welch, B.M.; Dere, W.; Schiffman, J.D. Family Health History: The Case for Better Tools. JAMA 2015, 313, 1711–1712. [Google Scholar] [CrossRef] [PubMed]
- Farwati, M.; Kumbamu, A.; Kochan, D.C.; Kullo, I.J. Patient and Provider Perspectives on a Decision Aid for Familial Hypercholesterolemia. J. Pers. Med. 2018, 8, 35. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, J.; Duprez, D.; Veach, P.M.; Zierhut, H.A. Barriers to the identification of familial hypercholesterolemia among primary care providers. J. Community Genet. 2018, 10, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Gleacher, A.A.; Olin, S.S.; Nadeem, E.; Pollock, M.; Ringle, V.; Bickman, L.; Douglas, S.; Hoagwood, K. Implementing a Measurement Feedback System in Community Mental Health Clinics: A Case Study of Multilevel Barriers and Facilitators. Adm. Policy Ment. Health 2016, 43, 426–440. [Google Scholar] [CrossRef]
- Lyon, A.R.; Lewis, C.C. Designing Health Information Technologies for Uptake: Development and Implementation of Measurement Feedback Systems in Mental Health Service Delivery. Adm. Policy Ment. Health 2016, 43, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Keith, R.E.; Crosson, J.C.; O’Malley, A.S.; Cromp, D.; Taylor, E.F. Using the Consolidated Framework for Implementation Research (CFIR) to produce actionable findings: A rapid-cycle evaluation approach to improving implementation. Implement. Sci. 2017, 12, 15. [Google Scholar] [CrossRef]
- Wang, X.; Jiang, L.; Sun, L.-Y.; Wu, Y.; Wen, W.-H.; Wang, X.-F.; Liu, W.; Zhou, Y.-J.; Wang, L.-Y. Genetically confirmed familial hypercholesterolemia in outpatients with hypercholesterolemia. J. Geriatr. Cardiol. 2018, 15, 434–440. [Google Scholar]


{kind=link}
| Keywords/Strings Used for Literature Search | Databases and Journals | Inclusion Criteria |
|---|---|---|
|
|
|
| CFIR Domain | |
|---|---|
| 1. Characteristics of Intervention | Key attributes of interventions influence the success of implementation. Includes adaptability, complexity, cost, design quality and packaging, evidence strength and quality, intervention source, relative advantage, and trialability. |
| 2. Outer Setting | External influences including cosmopolitanism, external policies and incentives, patient needs and resources, and peer pressure. |
| 3. Inner Setting | Active interacting facets within a setting that include structural characteristics, networks and communications, culture, implementation climate, and readiness for implementation. |
| 4. Characteristics of Individuals | The actions and behaviors of individuals. Includes individual identification with an organization, individual stage of change, knowledge and beliefs about the intervention, other personal attributes, and self-efficacy. |
| 5. Process | The process of implementing an intervention. Includes or involves behaviors of engagement, execution, planning, reflecting, and evaluation. |
| Consolidated Framework for Implementation Research (CFIR) Domain #1, Characteristics of Intervention | |
| Facilitators | Barriers |
|
|
| CFIR Domain #2, Outer Setting | |
| Facilitators | Barriers |
| |
| CFIR Domain #3, Inner Setting | |
| Facilitators | Barriers |
|
|
| CFIR Domain #4, Characteristics of Individuals | |
| Facilitators | Barriers |
|
|
| CFIR Domain #5, Process | |
| Facilitators | Barriers |
|
|
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hendricks-Sturrup, R.M.; Mazor, K.M.; Sturm, A.C.; Lu, C.Y. Barriers and Facilitators to Genetic Testing for Familial Hypercholesterolemia in the United States: A Review. J. Pers. Med. 2019, 9, 32. https://doi.org/10.3390/jpm9030032
Hendricks-Sturrup RM, Mazor KM, Sturm AC, Lu CY. Barriers and Facilitators to Genetic Testing for Familial Hypercholesterolemia in the United States: A Review. Journal of Personalized Medicine. 2019; 9(3):32. https://doi.org/10.3390/jpm9030032
Chicago/Turabian StyleHendricks-Sturrup, Rachele M., Kathleen M. Mazor, Amy C. Sturm, and Christine Y. Lu. 2019. "Barriers and Facilitators to Genetic Testing for Familial Hypercholesterolemia in the United States: A Review" Journal of Personalized Medicine 9, no. 3: 32. https://doi.org/10.3390/jpm9030032