
Pharmacogenetic Analysis Enables Optimization of Pain Therapy: A Case Report of Ineffective Oxycodone Therapy
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Case Presentation
4. Discussion and Pharmaceutical Assessment
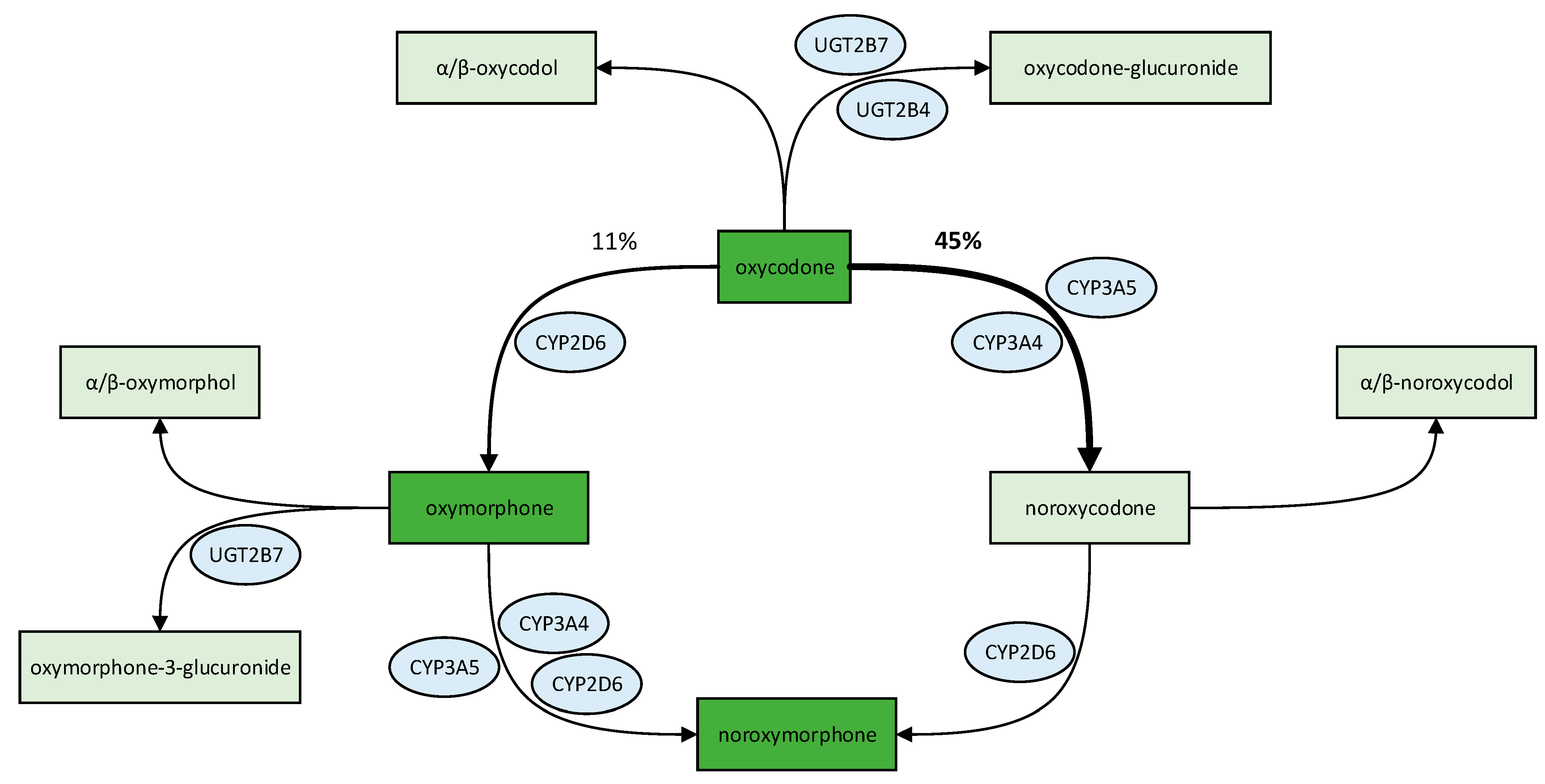
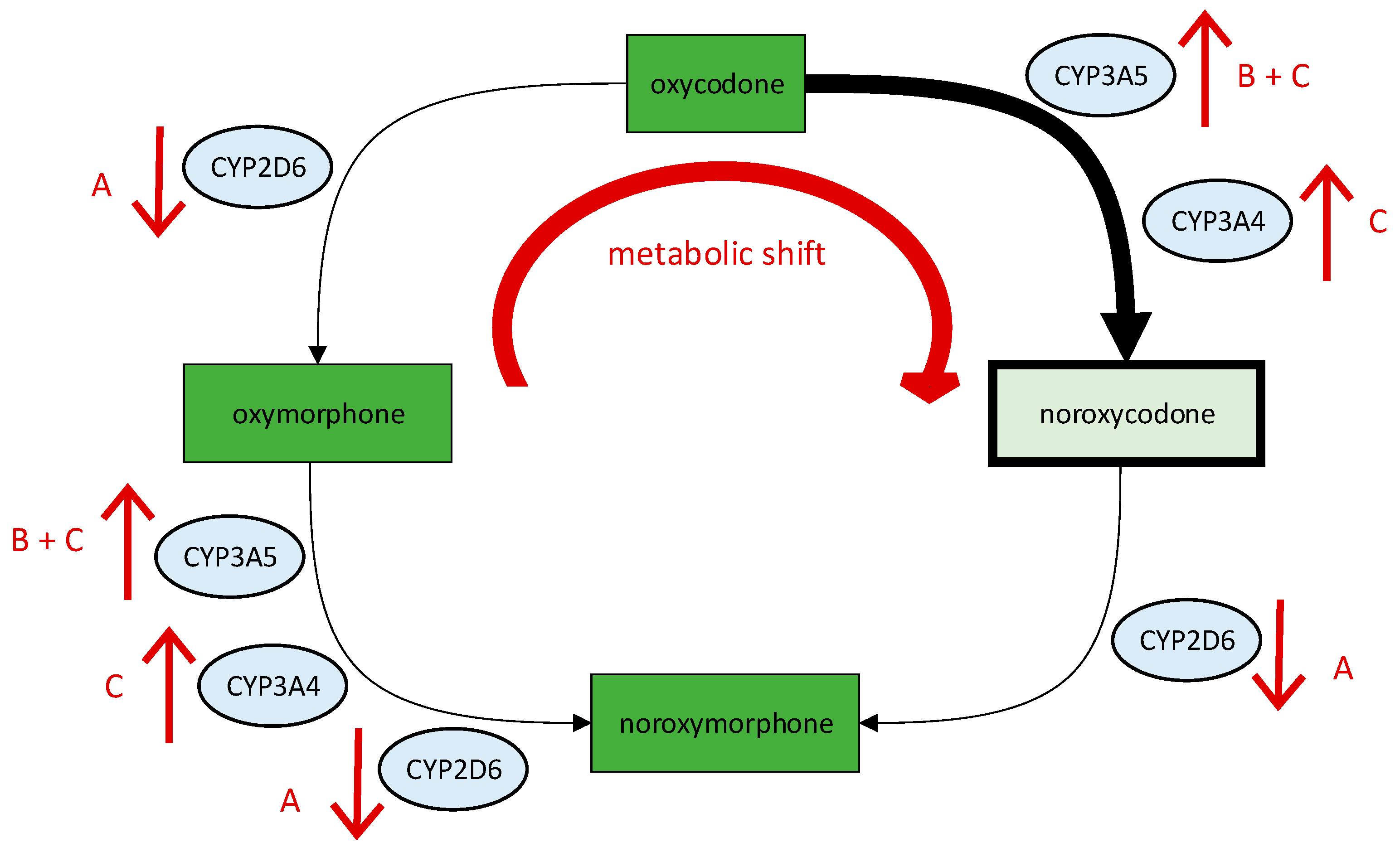
4.1. Assessment of Oxycodone
4.2. Assessment of Fentanyl and Morphine
4.3. Assessment of Non-Opioid Analgesics
4.4. Pharmaceutical Recommendation and Outcome
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Meucci, R.D.; Fassa, A.G.; Faria, N.M.X. Prevalence of chronic low back pain: Systematic review. Rev. Saude Publica 2015, 49, 1. [Google Scholar] [CrossRef]
- Wu, P.H.; Kim, H.S.; Jang, I.-T. Intervertebral Disc Diseases PART 2: A Review of the Current Diagnostic and Treatment Strategies for Intervertebral Disc Disease. Int. J. Mol. Sci. 2020, 21, 2135. [Google Scholar] [CrossRef]
- Greitemann, B. S2k-Leitlinie zur Versorgung bei Bandscheibenvorfällen mit Radikulärer Symptomatik: Leitlinie zur Konservativen, Operativen und Rehabilitativen Versorgung bei Bandscheibenvorfällen mit Radikulärer Symptomatik. Available online: https://www.awmf.org/uploads/tx_szleitlinien/033-048l_S2k_Konservative-operative_rehabilitative-Versorgung-Bandscheibenvorfall-radikulae_2021-06_01.pdf (accessed on 1 April 2023).
- Schofferman, J.; Mazanec, D. Evidence-informed management of chronic low back pain with opioid analgesics. Spine J. 2008, 8, 185–194. [Google Scholar] [CrossRef]
- Deyo, A.R.; Von Korff, M.; Duhrkoop, D. Opioids for low back pain. BMJ 2015, 350, g6380. [Google Scholar] [CrossRef]
- Gouveia, N.; Rodrigues, A.; Ramiro, S.; Eusébio, M.; Machado, P.M.; Canhão, H.; Branco, J.C. The Use of Analgesic and Other Pain-Relief Drugs to Manage Chronic Low Back Pain: Results from a National Survey. Pain Pract. 2017, 17, 353–365. [Google Scholar] [CrossRef]
- Benjeddou, M.; Peiró, A.M. Pharmacogenomics and prescription opioid use. Pharmacogenomics 2021, 22, 235–245. [Google Scholar] [CrossRef]
- Crews, K.R.; Monte, A.A.; Huddart, R.; Caudle, K.E.; Kharasch, E.D.; Gaedigk, A.; Dunnenberger, H.M.; Leeder, J.S.; Callaghan, J.T.; Samer, C.F.; et al. Clinical Pharmacogenetics Implementation Consortium Guideline for CYP2D6, OPRM1, and COMT Genotypes and Select Opioid Therapy. Clin. Pharmacol. Ther. 2021, 110, 888–896. [Google Scholar] [CrossRef]
- Matic, M.; Nijenhuis, M.; Soree, B.; de Boer-Veger, N.J.; Buunk, A.-M.; Houwink, E.J.F.; Mulder, H.; Rongen, G.A.P.J.M.; van der Weide, J.; Wilffert, B.; et al. Dutch Pharmacogenetics Working Group (DPWG) guideline for the gene–drug interaction between CYP2D6 and opioids (codeine, tramadol and oxycodone). Eur. J. Hum. Genet. 2021, 30, 1105–1113. [Google Scholar] [CrossRef]
- Ko, T.-M.; Wong, C.-S.; Wu, J.-Y.; Chen, Y.-T. Pharmacogenomics for personalized pain medicine. Acta Anaesthesiol. Taiwanica 2016, 54, 24–30. [Google Scholar] [CrossRef]
- McDonnell, J.M.; Rigney, B.; Storme, J.; Ahern, D.P.; Cunniffe, G.; Butler, J.S. Pharmacogenetic profiling and individualised therapy in the treatment of degenerative spinal conditions. Ir. J. Med. Sci. 2022, in press. [Google Scholar] [CrossRef]
- Cairoli, F.R.; Appiani, F.; Sambade, J.M.; Comandé, D.; Arteaga, L.C.; Ciapponi, A. Efficacy and safety of opioid therapy guided by pharmacogenetics: A systematic review. Pharmacogenomics 2021, 22, 573–586. [Google Scholar] [CrossRef]
- Kaya-Akyüzlü, D.; Özkan-Kotiloğlu, S.; Bal, C.; Yalçın-Şahiner, Ş.; Avcıoğlu, G.; Danışman, M. Effects of UGT2B7 rs7662029 and rs7439366 polymorphisms on sublingual buprenorphine metabolism in heroin addicts: An improved PCR-RFLP assay for the detection of rs7662029 polymorphism. Environ. Toxicol. Pharmacol. 2022, 94, 103902. [Google Scholar] [CrossRef]
- PharmGKB. PGx Gene-Specific Information Tables. Available online: https://www.pharmgkb.org/page/pgxGeneRef (accessed on 28 April 2023).
- Ballester, P.; Muriel, J.; Peiró, A.M. CYP2D6 phenotypes and opioiD Metabolism: The panth to personalized analgesiaYYYY). Expert. Opin. Drug Metab. Toxicol. 2022, 18, 261–275. [Google Scholar] [CrossRef]
- Umukoro, N.N.; Aruldhas, B.W.; Rossos, R.; Pawale, D.; Renschler, J.S.; Sadhasivam, S. Pharmacogenomics of oxycodone: A narrative literature review. Pharmacogenomics 2021, 22, 275–290. [Google Scholar] [CrossRef]
- Lalovic, B.; Phillips, B.; Risler, L.L.; Howald, W.; Shen, D.D. Quantitative Contribution of CYP2D6 and CYP3A to oxycodone metabolism in human liver and intestinal microsomes. Drug Metab. Dispos. 2004, 32, 447–454. [Google Scholar] [CrossRef]
- Lalovic, B.; Kharasch, E.; Hoffer, C.; Risler, L.; Liu-Chen, L.; Shen, D.D. Pharmacokinetics and pharmacodynamics of oral oxycodone in healthy human subjects: Role of circulating active metabolites. Clin. Pharmacol. Ther. 2006, 79, 461–479. [Google Scholar] [CrossRef]
- Romand, S.; Spaggiari, D.; Marsousi, N.; Samer, C.; Desmeules, J.; Daali, Y.; Rudaz, S. Characterization of oxycodone in vitro metabolism by human cytochromes P450 and UDP-glucuronosyltransferases. J. Pharm. Biomed. Anal. 2017, 144, 129–137. [Google Scholar] [CrossRef]
- Coffman, B.L.; King, C.D.; Rios, G.R.; Tephly, T.R. The glucuronidation of opioids, other xenobiotics, and androgens by human UGT2B7Y(268) and UGT2B7H(268). Drug Metab. Dispos. 1998, 26, 73–77. [Google Scholar]
- Swissmedic. Product Information—Stocrin. Available online: http://www.swissmedicinfo.ch/ (accessed on 1 April 2023).
- Andreassen, T.N.; Eftedal, I.; Klepstad, P.; Davies, A.; Bjordal, K.; Lundström, S.; Kaasa, S.; Dale, O. Do CYP2D6 genotypes reflect oxycodone requirements for cancer patients treated for cancer pain? A cross-sectional multicentre study. Eur. J. Clin. Pharmacol. 2012, 68, 55–64. [Google Scholar] [CrossRef]
- Zwisler, S.T.; Enggaard, T.P.; Mikkelsen, S.; Brosen, K.; Sindrup, S.H. Impact of the CYP2D6 genotype on post-operative intravenous oxycodone analgesia. Acta Anaesthesiol. Scand. 2010, 54, 232–240. [Google Scholar] [CrossRef]
- Stamer, U.M.; Zhang, L.; Book, M.; Lehmann, L.E.; Stuber, F.; Musshoff, F. CYP2D6 Genotype Dependent Oxycodone Metabolism in Postoperative Patients. PLoS ONE 2013, 8, e60239. [Google Scholar] [CrossRef]
- Zwisler, S.T.; Enggaard, T.P.; Noehr-Jensen, L.; Pedersen, R.S.; Mikkelsen, S.; Nielsen, F.; Brosen, K.; Sindrup, S.H. The Hypoalgesic Effect of Oxycodone in Human Experimental Pain Models in Relation to the CYP2D6 Oxidation Polymorphism. Basic Clin. Pharmacol. Toxicol. 2009, 104, 335–344. [Google Scholar] [CrossRef]
- Samer, C.; Daali, Y.; Wagner, M.; Hopfgartner, G.; Eap, C.; Rebsamen, M.; Rossier, M.; Hochstrasser, D.; Dayer, P.; Desmeules, J. Genetic polymorphisms and drug interactions modulating CYP2D6 and CYP3A activities have a major effect on oxycodone analgesic efficacy and safety. Br. J. Pharmacol. 2010, 160, 919–930. [Google Scholar] [CrossRef]
- Susce, M.T.; Murray-Carmichael, E.; de Leon, J. Response to hydrocodone, codeine and oxycodone in a CYP2D6 poor metabolizer. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2006, 30, 1356–1358. [Google Scholar] [CrossRef]
- Foster, A.; Mobley, E.; Wang, Z. Complicated Pain Management in a CYP450 2D6 Poor Metabolizer. Pain Pract. 2007, 7, 352–356. [Google Scholar] [CrossRef]
- Maddocks, I.; Somogyi, A.; Abbott, F.; Hayball, P.; Parker, D. Attenuation of morphine-induced delirium in palliative care by substitution with infusion of oxycodone. J. Pain Symptom Manag. 1996, 12, 182–189. [Google Scholar] [CrossRef]
- Klimas, R.; Witticke, D.; El Fallah, S.; Mikus, G. Contribution of oxycodone and its metabolites to the overall analgesic effect after oxycodone administration. Expert Opin. Drug Metab. Toxicol. 2013, 9, 517–528. [Google Scholar] [CrossRef]
- Naito, T.; Takashina, Y.; Yamamoto, K.; Tashiro, M.; Ohnishi, K.; Kagawa, Y.; Kawakami, J. CYP3A5*3 Affects Plasma Disposition of Noroxycodone and Dose Escalation in Cancer Patients Receiving Oxycodone. J. Clin. Pharmacol. 2011, 51, 1529–1538. [Google Scholar] [CrossRef]
- Kuehl, P.; Zhang, J.; Lin, Y.; Lamba, J.; Assem, M.; Schuetz, J.; Watkins, P.B.; Daly, A.; Wrighton, S.A.; Hall, S.D.; et al. Sequence diversity in CYP3A promoters and characterization of the genetic basis of polymorphic CYP3A5 expression. Nat. Genet. 2001, 27, 383–391. [Google Scholar] [CrossRef]
- Hustert, E.; Haberl, M.; Burk, O.; Wolbold, R.; He, Y.-Q.; Klein, K.; Nuessler, A.C.; Neuhaus, P.; Klattig, J.; Eiselt, R.; et al. The genetic determinants of the CYP3A5 polymorphism. Pharmacogenetics 2001, 11, 773–779. [Google Scholar] [CrossRef]
- Bachmann, F.; Duthaler, U.; zu Schwabedissen, H.E.M.; Puchkov, M.; Huwyler, J.; Haschke, M.; Krähenbühl, S. Metamizole is a Moderate Cytochrome P450 Inducer Via the Constitutive Androstane Receptor and a Weak Inhibitor of CYP1A2. Clin. Pharmacol. Ther. 2021, 109, 1505–1516. [Google Scholar] [CrossRef]
- Burk, O.; Koch, I.; Raucy, J.; Hustert, E.; Eichelbaum, M.; Brockmöller, J.; Zanger, U.M.; Wojnowski, L. The Induction of Cytochrome P450 3A5 (CYP3A5) in the Human Liver and Intestine Is Mediated by the Xenobiotic Sensors Pregnane X Receptor (PXR) and Constitutively Activated Receptor (CAR). J. Biol. Chem. 2004, 279, 38379–38385. [Google Scholar] [CrossRef]
- Sawyer, M.B.; Innocenti, F.; Das, S.; Cheng, C.; Ramírez, J.; Pantle-Fisher, F.H.; Rn, C.W.; Badner, J.; Pei, D.; Boyett, J.M.; et al. A pharmacogenetic study of uridine diphosphate–glucuronosyltransferase 2B7 in patients receiving morphine. Clin. Pharmacol. Ther. 2003, 73, 566–574. [Google Scholar] [CrossRef]
- Trescot, A.M.; Datta, S.; Lee, M.; Hansen, H. Opioid pharmacology. Pain Physician 2008, 11, S133–S153. [Google Scholar] [CrossRef]
- Zhang, Y.; Wang, D.; Johnson, A.D.; Papp, A.C.; Sadée, W. Allelic Expression Imbalance of Human mu Opioid Receptor (OPRM1) Caused by Variant A118G. J. Biol. Chem. 2005, 280, 32618–32624. [Google Scholar] [CrossRef]
- Choi, S.-W.; Lam, D.M.; Wong, S.S.; Shiu, H.H.; Wang, A.X.; Cheung, C.-W. Effects of Single Nucleotide Polymorphisms on Surgical and Postsurgical Opioid Requirements: A Systematic Review and Meta-Analysis. Clin. J. Pain 2017, 33, 1117–1130. [Google Scholar] [CrossRef]
- Zwisler, S.T.; Enggaard, T.P.; Noehr-Jensen, L.; Mikkelsen, S.; Verstuyft, C.; Becquemont, L.; Sindrup, S.H.; Brosen, K. The antinociceptive effect and adverse drug reactions of oxycodone in human experimental pain in relation to genetic variations in the OPRM1 and ABCB1 genes. Fundam. Clin. Pharmacol. 2009, 24, 517–524. [Google Scholar] [CrossRef]
- Cajanus, K.; Kaunisto, M.A.; Tallgren, M.; Jokela, R.; Kalso, E. How Much Oxycodone Is Needed for Adequate Analgesia After Breast Cancer Surgery: Effect of the OPRM1 118A>G Polymorphism. J. Pain 2014, 15, 1248–1256. [Google Scholar] [CrossRef]
- Olsen, M.B.; Jacobsen, L.M.; Schistad, E.I.; Pedersen, L.M.; Rygh, L.J.; Røe, C.; Gjerstad, J. Pain Intensity the First Year after Lumbar Disc Herniation Is Associated with the A118G Polymorphism in the Opioid Receptor Mu 1 Gene: Evidence of a Sex and Genotype Interaction. J. Neurosci. 2012, 32, 9831–9834. [Google Scholar] [CrossRef]
- Boström, E.; Simonsson, U.S.; Hammarlund-Udenaes, M. Oxycodone Pharmacokinetics and Pharmacodynamics in the Rat in the Presence of the P-Glycoprotein Inhibitor PSC833. J. Pharm. Sci. 2005, 94, 1060–1066. [Google Scholar] [CrossRef]
- Metcalf, M.D.; Rosicky, A.D.; Hassan, H.E.; Eddington, N.D.; Coop, A.; Cunningham, C.W.; Mercer, S.L. Opioids and efflux transporters. Part 4: Influence of N-substitution on P-glycoprotein substrate activity of noroxymorphone analogues. Bioorganic Med. Chem. Lett. 2014, 24, 3592–3595. [Google Scholar] [CrossRef]
- Zwisler, S.T.; Enggaard, T.P.; Mikkelsen, S.; Verstuyft, C.; Becquemont, L.; Sindrup, S.H.; Brosen, K. Lack of Association of OPRM1 and ABCB1 Single-Nucleotide Polymorphisms to Oxycodone Response in Postoperative Pain. J. Clin. Pharmacol. 2012, 52, 234–242. [Google Scholar] [CrossRef]
- Zubieta, J.-K.; Heitzeg, M.M.; Smith, Y.R.; Bueller, J.A.; Xu, K.; Xu, Y.; Koeppe, R.A.; Stohler, C.S.; Goldman, D. COMT val 158 met Genotype Affects µ-Opioid Neurotransmitter Responses to a Pain Stressor. Science 2003, 299, 1240–1243. [Google Scholar] [CrossRef]
- Takashina, Y.; Naito, T.; Mino, Y.; Yagi, T.; Ohnishi, K.; Kawakami, J. Impact of CYP3A5 and ABCB1 Gene Polymorphisms on Fentanyl Pharmacokinetics and Clinical Responses in Cancer Patients Undergoing Conversion to a Transdermal System. Drug Metab. Pharmacokinet. 2012, 27, 414–421. [Google Scholar] [CrossRef]
- Wittwer, E.; Kern, S.E. Role of morphine’s metabolites in analgesia: Concepts and controversies. AAPS J. 2006, 8, E348–E352. [Google Scholar] [CrossRef]
- Ohno, S.; Kawana, K.; Nakajin, S. Contribution of UDP-Glucuronosyltransferase 1A1 and 1A8 to Morphine-6-Glucuronidation and Its Kinetic Properties. Drug Metab. Dispos. 2008, 36, 688–694. [Google Scholar] [CrossRef]
- Chen, Y.; Ning, M.; Tao, Y.; Hu, X.; Guo, L.; Ni, J.; Hu, J.; Shen, H. Roles of UGT2B7 C802T gene polymorphism on the efficacy of morphine treatment on cancer pain among the Chinese han population. Niger. J. Clin. Pract. 2019, 22, 1319–1323. [Google Scholar] [CrossRef]
- Holthe, M.; Klepstad, P.; Zahlsen, K.; Borchgrevink, P.; Hagen, L.; Dale, O.; Kaasa, S.; Krokan, H.; Skorpen, F. Morphine glucuronide-to-morphine plasma ratios are unaffected by the UGT2B7 H268Y and UGT1A1*28 polymorphisms in cancer patients on chronic morphine therapy: Clinical utility and future perspectives. Eur. J. Clin. Pharmacol. 2002, 58, 353–356. [Google Scholar] [CrossRef]
- Lötsch, J.; Skarke, C.; Liefhold, J.; Geisslinger, G. Genetic Predictors of the Clinical Response to Opioid Analgesics. Clin. Pharmacokinet. 2004, 43, 983–1013. [Google Scholar] [CrossRef]
- Hajj, A.; Halepian, L.; El Osta, N.; Chahine, G.; Kattan, J.; Khabbaz, L.R. OPRM1 c.118A>G Polymorphism and Duration of Morphine Treatment Associated with Morphine Doses and Quality-of-Life in Palliative Cancer Pain Settings. Int. J. Mol. Sci. 2017, 18, 669. [Google Scholar] [CrossRef]
- Chou, W.-Y.; Yang, L.-C.; Lu, H.-F.; Ko, J.-Y.; Wang, C.-H.; Lin, S.-H.; Lee, T.-H.; Concejero, A.; Hsu, C.-J. Association of μ-opioid receptor gene polymorphism (A118G) with variations in morphine consumption for analgesia after total knee arthroplasty. Acta Anaesthesiol. Scand. 2006, 50, 787–792. [Google Scholar] [CrossRef]
- Cheng, H.; Chu, X.; Yi, S. The Influence of OPRM1 A118G Polymorphism on the Dosage of Morphine in Patients with Advanced Liver Cancer. J. Coll. Physicians Surg. Pak. 2021, 31, 1375–1377. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zhang, L.; Zhao, X.; Shen, S.; Luo, X.; Zhang, Y. Association between MDR1/CYP3A4/OPRM1 gene polymorphisms and the post-caesarean fentanyl analgesic effect on Chinese women. Gene 2018, 661, 78–84. [Google Scholar] [CrossRef]
- Zhang, W.; Yuan, J.J.; Kan, Q.C.; Zhang, L.R.; Chang, Y.Z.; Wang, Z.Y. Study of the OPRM1 A118G genetic polymorphism associated with postoperative nausea and vomiting induced by fentanyl intravenous analgesia. Minerva Anestesiol. 2011, 77, 33–39. [Google Scholar] [PubMed]
- Zhang, W.; Chang, Y.Z.; Kan, Q.C.; Zhang, L.R.; Lu, H.; Chu, Q.J.; Wang, Z.Y.; Li, Z.S.; Zhang, J. Association of human μ-opioid receptor gene polymorphism A118G with fentanyl analgesia consumption in Chinese gynaecological patients. Anaesthesia 2010, 65, 130–135. [Google Scholar] [CrossRef]
- Theken, K.N.; Lee, C.R.; Gong, L.; Caudle, K.E.; Formea, C.M.; Gaedigk, A.; Klein, T.E.; Agúndez, J.A.; Grosser, T. Clinical Pharmacogenetics Implementation Consortium Guideline (CPIC) for CYP2C9 and Nonsteroidal Anti-Inflammatory Drugs. Clin. Pharmacol. Ther. 2020, 108, 191–200. [Google Scholar] [CrossRef] [PubMed]
- Dean, L. Venlafaxine Therapy and CYP2D6 Genotype. In Medical Genetics Summaries; Pratt, V.M., Scott, S.A., Pirmohamed, M., Esquivel, B., Kattman, B.L., Malheiro, A.J., Eds.; National Center for Biotechnology Information (US): Bethesda, MD, USA, 2012. [Google Scholar]
- Breitenstein, B.; Brückl, T.M.; Ising, M.; Müller-Myhsok, B.; Holsboer, F.; Czamara, D. ABCB1 gene variants and antidepressant treatment outcome: A meta-analysis. Am. J. Med. Genet. Part B Neuropsychiatr. Genet. 2015, 168, 274–283. [Google Scholar] [CrossRef]
- Breitenstein, B.; Scheuer, S.; Pfister, H.; Uhr, M.; Lucae, S.; Holsboer, F.; Ising, M.; Brückl, T.M. The clinical application of ABCB1 genotyping in antidepressant treatment: A pilot study. CNS Spectrums 2014, 19, 165–175. [Google Scholar] [CrossRef]
- Zheng, M.; McErlane, K.M.; Ong, M.C. Hydromorphone metabolites: Isolation and identification from pooled urine samples of a cancer patient. Xenobiotica 2002, 32, 427–439. [Google Scholar] [CrossRef]
- Zheng, M.; McErlane, K.M.; Ong, M.C. Identification and synthesis of norhydromorphone, and determination of antinociceptive activities in the rat formalin test. Life Sci. 2004, 75, 3129–3146. [Google Scholar] [CrossRef]
- Vandenbossche, J.; Richards, H.; Francke, S.; Bergh, A.V.D.; Lu, C.C.; Franc, M.A. The effect of UGT2B7*2 polymorphism on the pharmacokinetics of OROS® hydromorphone in Taiwanese subjects. J. Clin. Pharmacol. 2014, 54, 1170–1179. [Google Scholar] [CrossRef] [PubMed]
- Murray, A.; Hagen, N.A. Hydromorphone. J. Pain Symptom Manag. 2005, 29, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Smith, H.S. The Metabolism of Opioid Agents and the Clinical Impact of Their Active Metabolites. Clin. J. Pain 2011, 27, 824–838. [Google Scholar] [CrossRef] [PubMed]
- Freo, U.; Romualdi, P.; Kress, H.G. Tapentadol for neuropathic pain: A review of clinical studies. J. Pain Res. 2019, 12, 1537–1551. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Substance | Schedule |
|---|---|
| Oxycodone/Naloxone SR a 20/10 mg | 1-0-1-0 |
| Oxycodone oral Liq b 10 mg/mL | PRN c (max. 7 mg/day) |
| Ibuprofen 600 mg | 1-1-1-0 |
| Metamizol gtt d 0.5 mg/mL | 2-2-2-2 mL |
| Venlafaxine ER e 150 mg | 1-0-0-0 |
| Pantoprazole 40 mg | PRN c (max. 1 tablet/day) |
| various laxatives | different |
| Gene | Variant (Additionally Tested Variants in Gen Locus) | Genotype | Predicted Phenotype (Activity Score) |
|---|---|---|---|
| CYP2C9 | rs1057910 c.1075A > C (in *3) (rs1799853, rs9332131, rs7900194, rs28371685) | A/C | intermediate metabolizer (AS = 1, reduced function) |
| CYP2C8 | (rs10509681, rs11572080, rs1934951) | WT a, *1 | n.d. d (n.d. d) |
| CYP2C19 | (rs4244285, rs4986893, rs12248560, rs28399504) | WT a, *1 | normal metabolizer (n.d. d) |
| CYP2D6 | rs3892097 c.506-1G > A (in *4) rs1065852 c.100C > T (in *4 and *10) (CNV c, rs35742686, rs5030655, rs5030867, rs5030865, rs5030656, rs201377835, rs28371706, rs59421388, rs28371725) | G/A C/T | intermediate metabolizer (AS = 1, reduced function) |
| CYP3A5 | rs776746 c.219-237G > A (in *3) | A/G | intermediate metabolizer (n.d. d) |
| UGT2B7 | rs7439366 c.802C > T (in *2) | C/T | n.d.d (substance specific) |
| OPRM1 | rs1799971 c.118A > G | A/G | n.d. d (substance specific) |
| COMT | rs4680 c.472G > A (rs165599, rs4646316, rs9332377) | A/G | n.d. d (substance specific) |
| ABCB1 | rs2032583 c.2685 + 49T > C rs1045642 c.3435T > C rs2032582 c.2677G > A or c.2677G > T (rs1128503) | T/T C/T G/G | n.d. d (substance specific) |
| Substance | Clinical Effect | Pharmaceutical Assessment | Pharmaceutical Recommendation |
|---|---|---|---|
| Oxycodone | insufficient analgesic efficacy | Metabolic shift to inactive noroxycodone due to decreased activity of CYP2D6, increased activity of CYP3A5 and a drug interaction with metamizole. Impaired drug response at the µ-opioid receptor. | Avoid opiates that are bioactivated by CYP2D6 or inactivated by CYP3A5. Switch to hydromorphone or tapentadol. |
| Fentanyl | insufficient analgesic efficacy | Increased inactivation due to increased activity of CYP3A5 and a drug interaction with metamizole. Impaired drug response at the µ-opioid receptor. | |
| Morphine | insufficient analgesic efficacy | Impaired drug response at the µ-opioid receptor. | |
| Ibuprofen | gastrointestinal side effects | Decreased inactivation due to decreased activity of CYP2C9 and thus an increased risk of gastrointestinal side effects. | Avoid NSAIDs a that are inactivated by CYP2C9. Switch to paracetamol. Combine NSAIDs a with a PPI b. |
| Venlafaxine | good antidepressant but insufficient analgesic efficacy | Reduced metabolism to its active metabolite due to decreased activity of CYP2D6. Limited penetration of the blood–brain barrier due to the ABCB1 variant. | Continue venlafaxine therapy. Pregabalin as additional therapy option. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wiss, F.M.; Stäuble, C.K.; Meyer zu Schwabedissen, H.E.; Allemann, S.S.; Lampert, M.L. Pharmacogenetic Analysis Enables Optimization of Pain Therapy: A Case Report of Ineffective Oxycodone Therapy. J. Pers. Med. 2023, 13, 829. https://doi.org/10.3390/jpm13050829
Wiss FM, Stäuble CK, Meyer zu Schwabedissen HE, Allemann SS, Lampert ML. Pharmacogenetic Analysis Enables Optimization of Pain Therapy: A Case Report of Ineffective Oxycodone Therapy. Journal of Personalized Medicine. 2023; 13(5):829. https://doi.org/10.3390/jpm13050829
Chicago/Turabian StyleWiss, Florine M., Céline K. Stäuble, Henriette E. Meyer zu Schwabedissen, Samuel S. Allemann, and Markus L. Lampert. 2023. "Pharmacogenetic Analysis Enables Optimization of Pain Therapy: A Case Report of Ineffective Oxycodone Therapy" Journal of Personalized Medicine 13, no. 5: 829. https://doi.org/10.3390/jpm13050829