
A Comparative Study to Investigate the Effects of Bisoprolol in Patients with Chronic Heart Failure and Hypertension When Switched from Tablets to Transdermal Patches


Abstract
:1. Introduction
2. Methods
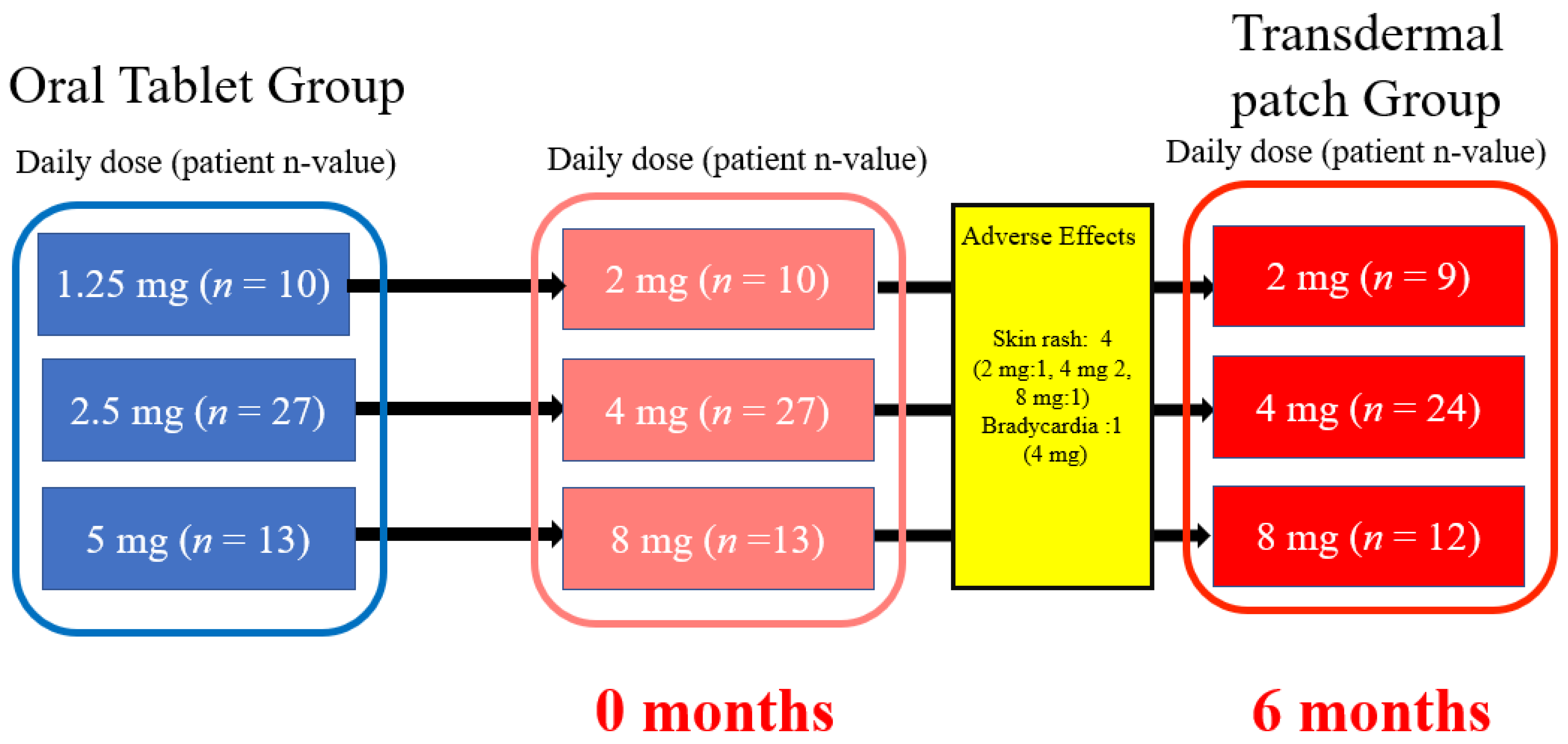
2.1. Study Protocol
2.2. Statistical Analysis
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Clinical Trial Registration
References
- Bauersachs, J. Heart failure drug treatment: The fantastic four. Eur. Heart J. 2021, 42, 681–683. [Google Scholar] [CrossRef] [PubMed]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: A report of the American College of Cardiology/American Heart Association joint committee on clinical practice guidelines. J. Am. Coll. Cariol. 2022, 79, e263–e421. [Google Scholar] [CrossRef] [PubMed]
- Schnabbel, P.; Maack, C.; Mies, F.; Tyroller, S.; Scheer, A.; Böhm, M. Binding properties of beta-blockers at recombinant beta1-, beta 2, beta 3-adrenoceptors. J. Cadiovasc. Pharmmacol. 2000, 36, 466–471. [Google Scholar] [CrossRef] [PubMed]
- Momomura, S.I.; Saito, Y.; Yasumura, Y.; Yamamoto, K.; Sakata, Y.; Daimon, M.; Kinugawa, K.; Okamoto, H.; Dohi, N.; Komuro, I. Efficacy and safety of switching from oral bisoprolol to transdermal patch in japanese patients with chronic heart failure. Circ. J. 2017, 2, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Matsuoka, H.; Kuwajima, I.; Shimada, K.; Mitamura, H.; Saruta, T. Comparison of efficacy and safety between bisoprolol transdermal patch (TY-0201) and bisoprolol fumarate oral formulation in Japanese patients with grade I or II essential hypertension: Randomized, double-blind, placebo-controlled study. J. Clin. Hypertens. 2013, 15, 806–814. [Google Scholar] [CrossRef] [PubMed]
- Sairaku, A.; Nakano, Y.; Shiode, N.; Suennari, K.; Oda, N.; Ono, K.; Kihara, Y. Head-to-head comparison of the heart rate variability between the bisoprolol transdermal patch and bisoprolol fumarate tablet. Cardiovasc. Ther. 2018, 36, e12325. [Google Scholar] [CrossRef] [PubMed]
- Yammashita, T.; Ikeda, T.; Akita, Y. Comparison of heart rate reduction effect and safety between bisoprolol transdermal patch and bisoprolol fumarate oral formulation in Japanese patients with persistent/permanent atrial fibrillation (BISONO-AF study). J. Cardiol. 2019, 3, 386–393. [Google Scholar] [CrossRef] [PubMed]
- Shinohara, M.; Fujino, T.; Yao, S.; Yano, K.; Akitsu, K.; Koike, H.; Yuzawa, H.Y.; Suzuki, T.S.; Fukunaga, S.F.; Kobayashi, K.K.; et al. Assessment of a novel transdermal selective b1-blocker, the bisoprolol patch, for treating frequent premature ventricular contractions in patients without structural heart disease. J. Cardiol. 2019, 73, 7–13. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total number of patients | 50 |
| Age (years) | 75.1 ± 9.5 |
| Sex: male, female | 28, 22 |
| Basic disease | n (%) |
| Ischemic heart disease | 13 (26%) |
| Valvular disease | 22 (44%) |
| Hypertensive heart disease | 13 (26%) |
| Other | 2 (4%) |
| Classification of heart failure | n (%) |
| HFrEF | 6 (12%) |
| HFmrEF | 5 (10%) |
| HFpEF | 33 (66%) |
| HFpEF improved | 6 (12%) |
| Risk factors | n (%) |
| Type 2 diabetes | 18 (36%) |
| Dyslipidemia | 41 (82%) |
| Hyperuricemia | 25 (50%) |
| Atrial fibrillation | 17 (34%) |
| Obesity | 9 (18%) |
| Medications | n (%) |
| Oral bisoprolol | |
| 1.25 mg | 10 (20%) |
| 2.5 mg | 27 (54%) |
| 5.0 mg | 13 (26%) |
| Calcium antagonist | 17 (34%) |
| Angiotensin II receptor blocker | 18 (36%) |
| ACE inhibitor | 4 (8%) |
| Aldosterone blocker | 22 (44%) |
| α-blocker | 5 (10%) |
| Diuretics | 17 (34%) |
| Oral hypoglycemic agent | 18 (36%) |
| Statin | 42 (84%) |
| Ezetimibe | 12 (24%) |
| Xanthanide oxidase antagonist | 25 (50%) |
| Antiarrhythmic drugs | n (%) |
| Bepridil | 4 (8%) |
| Disopyramide | 1 (2%) |
| Mexiletine | 10 (20%) |
| Pilsicanide | 4 (8%) |
| Verapamil | 2 (4%) |
| Tablet | Patch | p Value | |
|---|---|---|---|
| Systolic blood pressure (mm Hg) | 127 (117, 137.5) | 127.5 (116.5, 141.3) | 0.674 |
| Diastolic blood pressure (mm Hg) | 71.5 (65.8, 81.3) | 73.5 (66, 81) | 0.977 |
| Heart rate | |||
| Minimum (bpm) | 56 (51, 60.5) | 54 (51, 61) | 0.63 |
| Mean (bpm) | 73 (68.5, 80.5) | 72 (66.5, 77) | 0.227 |
| Maximum (bpm) | 115 (102.5, 126) | 112 (97.5, 126) | 0.359 |
| Total (n) | 100,865 (90,907, 109,855) | 96,953 (90,365, 106,020) | 0.467 |
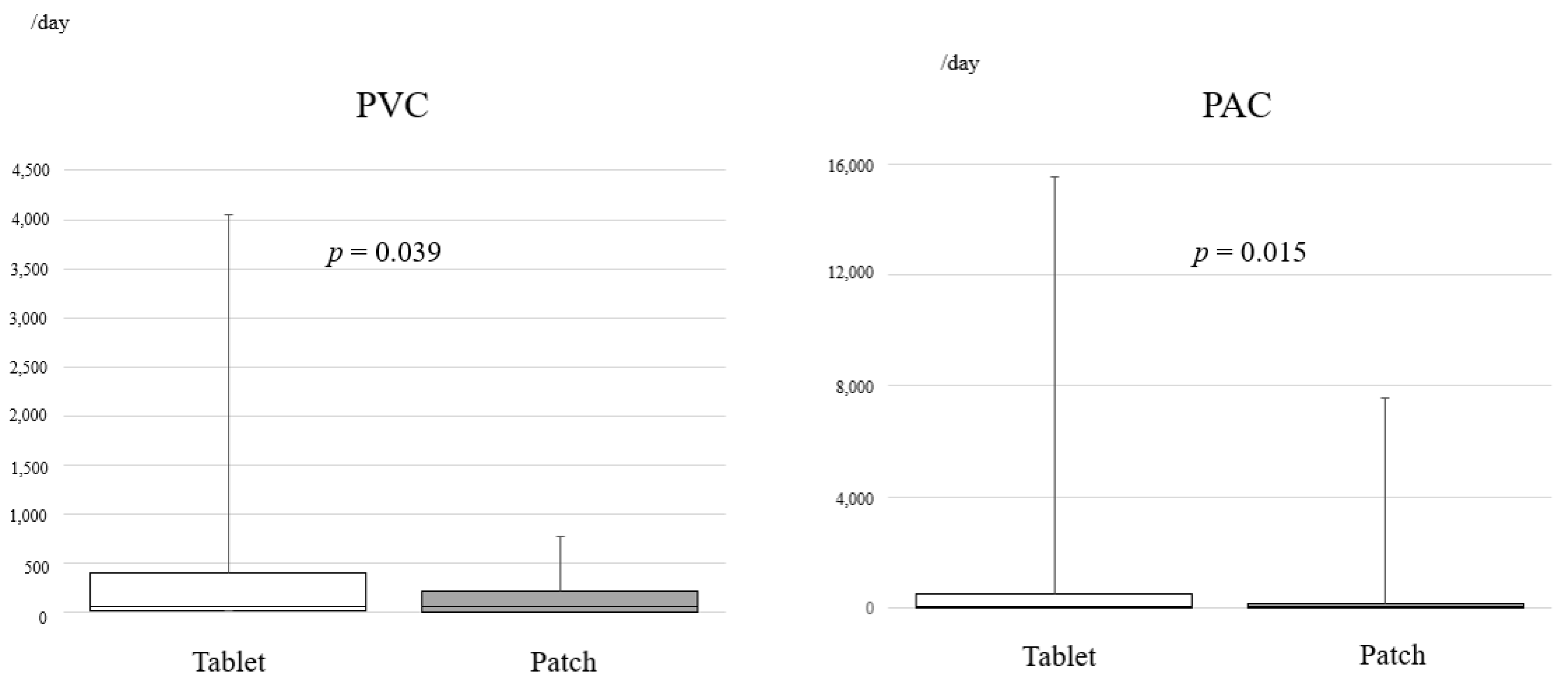
| PVC time segment (h) | |||
| 0–5 | 8 (1, 87) | 4 (0, 24.5) | 0.005 |
| 6–11 | 13 (3, 110) | 8 (5, 32.5) | 0.009 |
| 12–17 | 10 (3, 85) | 13 (1, 58.5) | 0.359 |
| 18–24 | 15 (2, 101) | 15 (1, 42.5) | 0.085 |
| PAC time segment (h) | |||
| 0–5 | 10 (0, 46.5) | 5 (0, 23.5) | 0.07 |
| 6–11 | 8 (0, 56) | 12 (0, 26) | 0.062 |
| 12–17 | 13 (0, 53) | 10 (0, 23.5) | 0.269 |
| 18–24 | 11 (0, 28) | 10 (0, 28.5) | 0.33 |
| Tablet | Patch | p-Value | |
|---|---|---|---|
| 6:00 | |||
| Minimum | 60 (55, 70.5) | 60 (54.5, 68) | 0.239 |
| Mean | 71 (61, 81.5) | 65 (61, 76) | 0.018 |
| Maximum | 85 (75, 101.5) | 79 (73.5, 93) | 0.003 |
| 12:00 | |||
| Minimum | 66 (60.5, 73) | 65 (58, 74,5) | 0.615 |
| Mean | 75 (70, 87.5) | 74 (68, 81.5) | 0.448 |
| Maximum | 92 (83, 108.5) | 89 (80.5, 105) | 0.368 |
| 18:00 | |||
| Minimum | 68 (61.5, 73) | 66 (60.5, 72.5) | 0.325 |
| Mean | 77 (67, 84.5) | 72 (68, 82.5) | 0.114 |
| Maximum | 91 (85.5, 101.5) | 87 (77.5, 100) | 0.082 |
| 0:00 | |||
| Minimum | 62 (55.5, 68) | 60 (55, 67.5) | 0.529 |
| Mean | 67 (61, 73) | 65 (58.5, 71) | 0.194 |
| Maximum | 78 (69, 86.5) | 76 (70, 82) | 0.403 |
|
0 Months (Tablet) |
3 Months (Patch) |
6 Months (Patch) | p -Value | |
|---|---|---|---|---|
| ANP levels (pg/mL) | 73.6 (46.9, 118.8) | 65.6 (50.3, 96.1) | 78.8 (45.2, 121.8) | 0.341 |
| BNP levels (pg/mL) | 89.8 (41.2, 174.5) | 83.4 (39.7, 174.7) | 87.1 (47.9, 186.4) | 0.428 |
| Echocardiography | 0 months (Tablet) | 6 months (Patch) | p-value | |
| LVDd (mm) | 45 (43, 51) | 45 (41, 52) | 0.861 | |
| LVDs (mm) | 29.5 (27, 34.3) | 29 (27, 34,3) | 0.638 | |
| Ejection fraction (%) | 64.5 (59.3, 68.3) | 63.7 (59.9, 67.4) | 0.400 | |
| E/e′ | 10,7 (7.9, 17.1) | 11 (8.1, 17.3) | 0.369 | |
| LVMI (g/m2) | 158.8 (121.5, 181.7) | 141.1 (120.8, 164.9) | 0.064 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sezai, A.; Sekino, H.; Taoka, M.; Osaka, S.; Tanaka, M. A Comparative Study to Investigate the Effects of Bisoprolol in Patients with Chronic Heart Failure and Hypertension When Switched from Tablets to Transdermal Patches. J. Pers. Med. 2023, 13, 785. https://doi.org/10.3390/jpm13050785
Sezai A, Sekino H, Taoka M, Osaka S, Tanaka M. A Comparative Study to Investigate the Effects of Bisoprolol in Patients with Chronic Heart Failure and Hypertension When Switched from Tablets to Transdermal Patches. Journal of Personalized Medicine. 2023; 13(5):785. https://doi.org/10.3390/jpm13050785
Chicago/Turabian StyleSezai, Akira, Hisakuni Sekino, Makoto Taoka, Shunji Osaka, and Masashi Tanaka. 2023. "A Comparative Study to Investigate the Effects of Bisoprolol in Patients with Chronic Heart Failure and Hypertension When Switched from Tablets to Transdermal Patches" Journal of Personalized Medicine 13, no. 5: 785. https://doi.org/10.3390/jpm13050785