
SARS-CoV-2 Footprints in the Placenta: What We Know after Three Years of the Pandemic
 , and
, and
Abstract
:1. Introduction
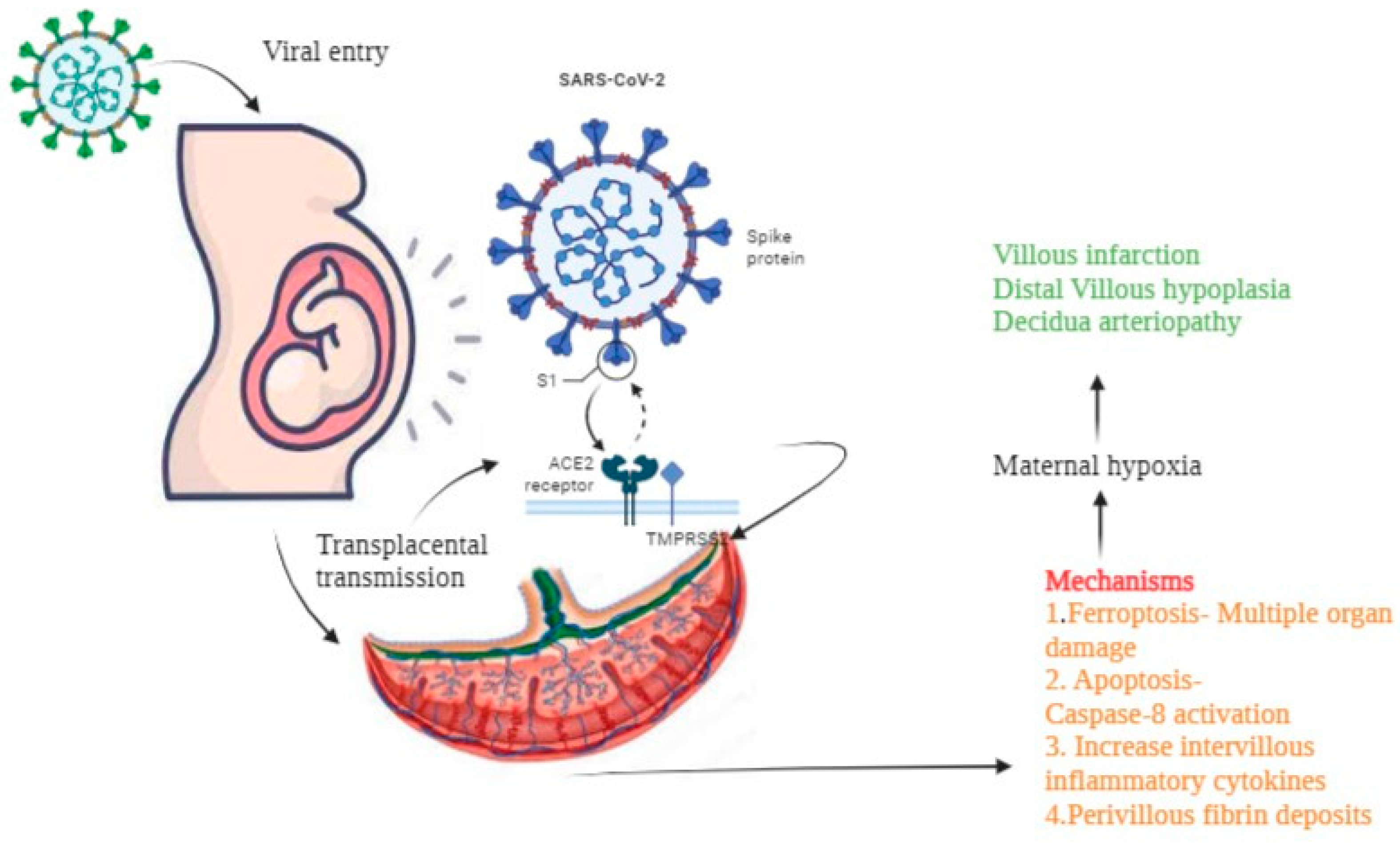
2. Mode of Entry
Vertical Transmission of SARS-CoV-2 from Mother to Fetus
3. SARS-CoV-2 Consequences for the Placenta
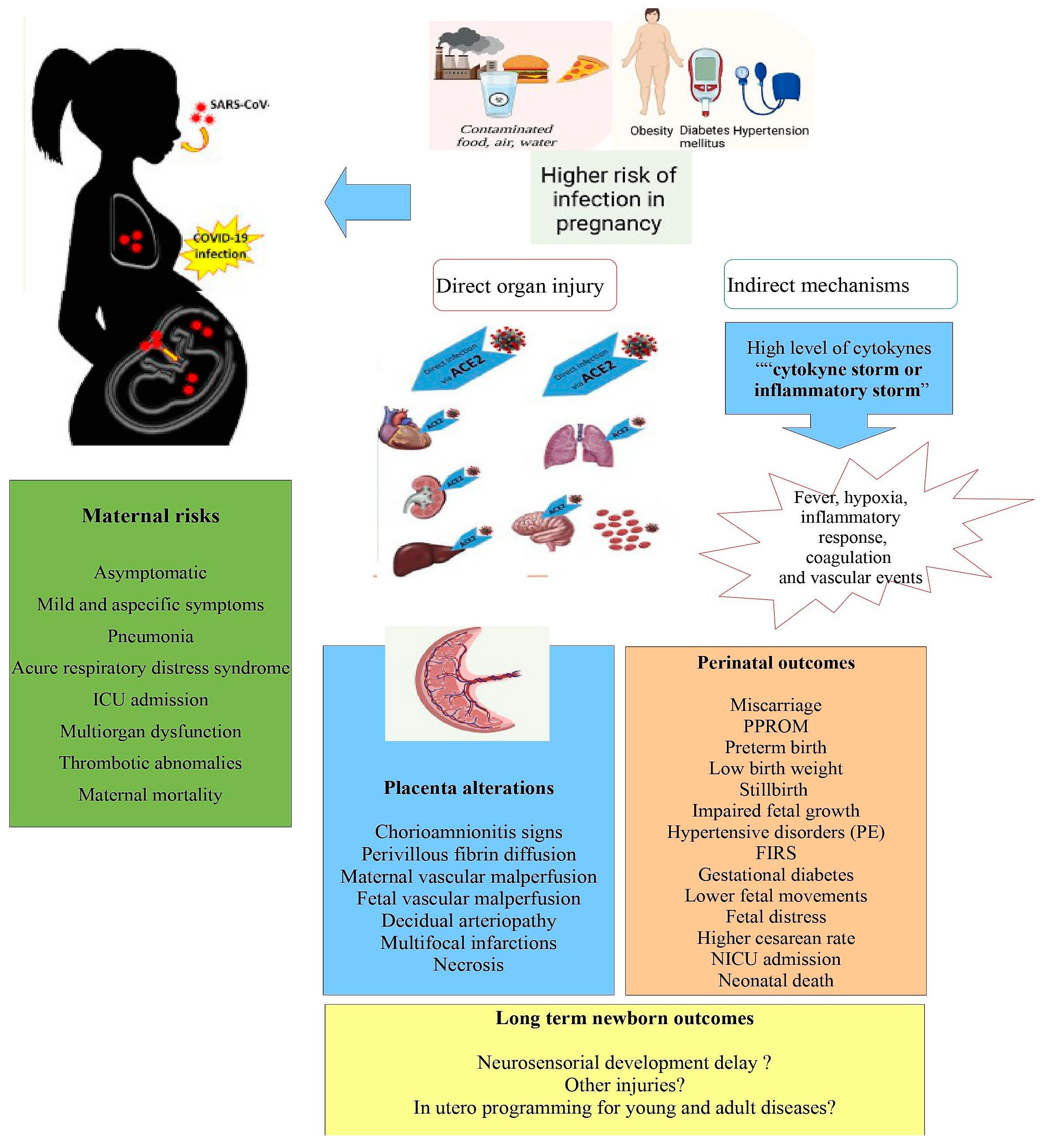
4. SARS-CoV-2 Infection and Pregnancy Outcomes
5. Placental Defense Mechanism
6. Route of SARS-CoV-2 during Pregnancy and Its Consequences
7. Future Perspectives
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 10 March 2023).
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Meyyazhagan, A.; Pushparaj, K.; Balasubramanian, B.; Kuchi Bhotla, H.; Pappusamy, M.; Arumugam, V.A.; Easwaran, M.; Pottail, L.; Mani, P.; Tsibizova, V.; et al. COVID-19 in pregnant women and children: Insights on clinical manifestations, complexities, and pathogenesis. Int. J. Gynaecol. Obstet. 2022, 156, 216–224. [Google Scholar] [CrossRef]
- Garcia-Flores, V.; Romero, R.; Xu, Y.; Theis, K.; Arenas-Hernandez, M.; Miller, D.; Peyvandipour, A.; Galaz, J.; Levenson, D.; Bhatti, G.; et al. Maternal-fetal immune responses in pregnant women infected with SARS-CoV-2. Nat. Commun. 2022, 13, 320. [Google Scholar] [CrossRef]
- Flannery, D.D.; Gouma, S.; Dhudasia, M.B.; Mukhopadhyay, S.; Pfeifer, M.R.; Woodford, E.C.; Triebwasser, J.E.; Gerber, J.S.; Morris, J.S.; Weirick, M.E.; et al. Assessment of maternal and neonatal cord blood SARS-CoV-2 antibodies and placental transfer ratios. JAMA Pediatr. 2021, 175, 594–600. [Google Scholar] [CrossRef]
- Metz, T.D.; Clifton, R.G.; Hughes, B.L.; Sandoval, G.J.; Grobman, W.A.; Saade, G.R.; Manuck, T.A.; Longo, M.; Sowles, A.; Clark, K.; et al. Association of SARS-CoV-2 infection with serious maternal morbidity and mortality from obstetric complications. JAMA 2022, 327, 748–759. [Google Scholar] [CrossRef]
- Yan, R.; Zhang, Y.; Li, Y.; Xia, L.; Guo, Y.; Zhou, Q. Structural basis for the recognition of SARS-CoV-2 by full-length human ACE2. Science 2020, 367, 1444–1448. [Google Scholar] [CrossRef]
- Li, B.; Yang, J.; Zhao, F.; Zhi, L.; Wang, X.; Liu, L.; Bi, Z.; Zhao, Y. Prevalence and impact of cardiovascular metabolic diseases on COVID-19 in China. Clin. Res. Cardiol. 2020, 109, 531–538. [Google Scholar] [CrossRef] [PubMed]
- Wei, S.Q.; Bilodeau-Bertrand, M.; Liu, S.; Auger, N. The impact of COVID-19 on pregnancy outcomes: A systematic review and meta-analysis. CMAJ 2021, 193, E540–E548. [Google Scholar] [CrossRef]
- Kotlyar, A.M.; Grechukhina, O.; Chen, A.; Popkhadze, S.; Grimshaw, A.; Tal, O.; Taylor, H.S.; Tal, R. Vertical transmission of coronavirus disease 2019: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2021, 224, 35–53.e33. [Google Scholar] [CrossRef]
- Kyle, M.H.; Dumitriu, D. Effects of in Utero SARS-CoV-2 Exposure on Newborn Health Outcomes. Encyclopedia 2023, 3, 15–27. [Google Scholar] [CrossRef]
- Ashary, N.; Bhide, A.; Chakraborty, P.; Colaco, S.; Mishra, A.; Chhabria, K.; Jolly, M.K.; Modi, D. Single-Cell RNA-seq Identifies Cell Subsets in Human Placenta That Highly Expresses Factors Driving Pathogenesis of SARS-CoV-2. Front. Cell. Dev. Biol. 2020, 8, 783. [Google Scholar] [CrossRef] [PubMed]
- Constantino, F.B.; Cury, S.S.; Nogueira, C.R.; Carvalho, R.F.; Justulin, L.A. Prediction of non-canonical routes for SARS-CoV-2 infection in human placenta cells. Front. Mol. Biosci. 2021, 8, 614728. [Google Scholar] [CrossRef] [PubMed]
- Wong, Y.P.; Tan, G.C.; Khong, T.Y. SARS-CoV-2 Transplacental Transmission: A Rare Occurrence? An Overview of the Protective Role of the Placenta. Int. J. Mol. Sci. 2023, 24, 4550. [Google Scholar] [CrossRef] [PubMed]
- Todros, T.; Masturzo, B.; Francia, S.D. COVID-19 infection: ACE2, pregnancy and preeclampsia. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 253, 330. [Google Scholar] [CrossRef] [PubMed]
- Beharier, O.; Kajiwara, K.; Sadovsky, Y. Ferroptosis, trophoblast lipotoxic damage, and adverse pregnancy outcome. Placenta 2021, 108, 32–38. [Google Scholar] [CrossRef]
- Shook, L.L.; Brigida, S.; Regan, J.; Flynn, J.P.; Mohammadi, A.; Etemad, B.; Siegel, M.R.; Clapp, M.A.; Li, J.Z.; Roberts, D.J.; et al. SARS-CoV-2 placentitis associated with B.1.617.2 (Delta) variant and fetal distress or demise. J. Infect. Dis. 2022, 225, 754–758. [Google Scholar] [CrossRef]
- Smith, E.R.; Oakley, E.; Grandner, G.W.; Ferguson, K.; Farooq, F.; Afshar, Y.; Ahlberg, M.; Ahmadzia, H.; Akelo, V.; Aldrovandi, G.; et al. Adverse maternal, fetal, and newborn outcomes among pregnant women with SARS-CoV-2 infection: An individual participant data meta-analysis. BMJ Glob. Health 2023, 8, e009495. [Google Scholar] [CrossRef]
- Valdespino-Vázquez, M.Y.; Helguera-Repetto, C.A.; León-Juárez, M.; Villavicencio-Carrisoza, O.; Flores-Pliego, A.; Moreno-Verduzco, E.R.; Díaz-Pérez, D.L.; Villegas-Mota, I.; Carrasco-Ramírez, E.; López-Martínez, I.E.; et al. Fetal and placental infection with SARS-CoV-2 in early pregnancy. J. Med. Virol. 2021, 93, 4480–4487. [Google Scholar] [CrossRef]
- Favre, G.; Mazzetti, S.; Gengler, C.; Bertelli, C.; Schneider, J.; Laubscher, B.; Capoccia, R.; Pakniyat, F.; Ben Jazia, I.; Eggel-Hort, B.; et al. Decreased fetal movements: A sign of placental SARS-CoV-2 infection with perinatal brain injury. Viruses 2021, 13, 2517. [Google Scholar] [CrossRef]
- Gengler, C.; Dubruc, E.; Favre, G.; Greub, G.; de Leval, L.; Baud, D. SARS-CoV-2 ACE-receptor detection in the placenta throughout pregnancy. Clin. Microbiol. Infect. 2021, 27, 489–490. [Google Scholar] [CrossRef]
- Heerema-McKenney, A. Defense and infection of the human placenta. APMIS 2018, 126, 570–588. [Google Scholar] [CrossRef]
- Rosenberg, A.Z.; Yu, W.; Hill, D.A.; Reyes, C.A.; Shwartz, D.A. Placental pathology of zika virus: Viral infection of the placenta induces villous stromal macrophage (hofbauer cell) proliferation and hyperplasia. Arch. Pathol. Lab. Med. 2017, 141, 43–48. [Google Scholar] [CrossRef]
- Arora, N.; Sadovsky, Y.; Dermody, T.S.; Coyne, C.B. Microbial vertical transmission during human pregnancy. Cell Host Microbe 2017, 21, 561–567. [Google Scholar] [CrossRef]
- Bayer, A.; Delorme-Axford, E.; Sleigher, C.; Frey, T.K.; Trobaugh, D.W.; Klimstra, W.B.; Emert-Sedlak, L.A.; Smithgall, T.E.; Kinchington, P.R.; Vadia, S.; et al. Human trophoblasts confer resistance to viruses implicated in perinatal infection. Am. J. Obstet. Gynecol. 2015, 212, 71.e1–71.e8. [Google Scholar] [CrossRef]
- Cardenas, I.; Means, R.E.; Aldo, P.; Koga, K.; Lang, S.M.; Booth, C.J.; Manzur, A.; Oyarzun, E.; Romero, R.; Mor, G. Viral infection of the placenta leads to fetal inflammation and sensitization to bacterial products predisposing to preterm labor. J. Immunol. 2010, 185, 1248–1257. [Google Scholar] [CrossRef]
- PrabhuDas, M.; Bonney, E.; Caron, K.; Dey, S.; Erlebacher, A.; Fazleabas, A.; Fisher, S.; Golos, T.; Matzuk, M.; McCune, J.M.; et al. Immune mechanisms at the maternal-fetal interface: Perspectives and challenges. Nat. Immunol. 2015, 16, 328–334. [Google Scholar] [CrossRef]
- Lee, J.K.; Oh, S.J.; Park, H.; Shin, O.S. Recent updates on research models and tools to study virus-host interactions at the placenta. Viruses 2019, 12, 5. [Google Scholar] [CrossRef]
- Smithgall, M.C.; Liu-Jarin, X.; Hamele-Bena, D.; Cimic, A.; Mourad, M.; Debelenko, L.; Chen, X. Third-trimester placentas of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)-positive women: Histomorphology, including viral immunohistochemistry and in-situ hybridization. Histopathology 2020, 77, 994–999. [Google Scholar] [CrossRef]
- Celik, E.; Vatansever, C.; Ozcan, G.; Kapucuoglu, N.; Alatas, C.; Besli, Y.; Palaoglu, E.; Gursoy, T.; Manici, M.; Turgal, M.; et al. Placental deficiency during maternal SARS-CoV-2 infection. Placenta 2022, 117, 47–56. [Google Scholar] [CrossRef]
- Aghaaamoo, S.; Ghods, K.; Rahmanian, M. Pregnant women with COVID-19: The placental involvement and consequences. J. Mol. Histol. 2021, 52, 427–435. [Google Scholar] [CrossRef]
- Meyer, J.A.; Roman, A.S.; Limaye, M.; Grossman, T.B.; Flaifel, A.; Vaz, M.J.; Thomas, K.M.; Penfield, C.A. Association of SARS-CoV-2 placental histopathology findings with maternal-fetal comorbidities and severity of COVID-19 hypoxia. J. Matern. Fetal. Neonatal. Med. 2022, 35, 8412–8418. [Google Scholar] [CrossRef]
- Gesaka, S.R.; Obimbo, M.M.; Wanyoro, A. Coronavirus disease 2019 and the placenta: A literature review. Placenta 2022, 126, 209–223. [Google Scholar] [CrossRef]
- Baud, D.; Nielsen-Saines, K.; Qi, X.; Musso, D.; Pomar, L.; Favre, G. Authors’ reply. Lancet Infect. Dis. 2020, 20, 775–776. [Google Scholar] [CrossRef]
- Vivanti, A.J.; Vauloup-Fellous, C.; Prevot, S.; Zupan, V.; Suffee, C.; Do Cao, J.; Benachi, A.; De Luca, D. Transplacental transmission of SARS-CoV-2 infection. Nat. Commun. 2020, 11, 3572. [Google Scholar] [CrossRef]
- Patane, L.; Morotti, D.; Giunta, M.R.; Sigismondi, C.; Piccoli, M.G.; Frigerio, L.; Mangili, G.; Arosio, M.; Cornolti, G. Vertical transmission of coronavirus disease 2019: Severe acute respiratory syndrome coronavirus 2 RNA on the fetal side of the placenta in pregnancies with coronavirus disease 2019-positive mothers and neonates at birth. Am. J. Obstet. Gynecol. MFM 2020, 2, 100145. [Google Scholar] [CrossRef]
- Li, M.; Chen, L.; Zhang, J.; Li, X. The SARS-CoV-2 receptor ACE2 expression of maternal–fetal interface and fetal organs by single-cell transcriptome study. PLoS ONE 2020, 15, e0230295. [Google Scholar] [CrossRef]
- Pique-Regi, R.; Romero, R.; Tarca, A.L.; Luca, F.; Xu, Y.; Alazizi, A.; Leng, Y.; Hsu, C.D.; Gomez-Lopez, N. Does the human placenta express the canonical cell entry mediators for SARS-CoV-2? Elife 2020, 9, e58716. [Google Scholar] [CrossRef]
- Ouyang, Y.; Bagalkot, T.; Fitzgerald, W.; Sadovsky, E.; Chu, T.; Martínez-Marchal, A.; Brieño-Enríquez, M.; Su, E.J.; Margolis, L.; Sorkin, A. Term human placental trophoblasts express SARS-CoV-2 entry factors ACE2, TMPRSS2, and Furin. MSphere 2021, 6, e00250-21. [Google Scholar] [CrossRef]
- Essalmani, R.; Jain, J.; Susan-Resiga, D.; Andréo, U.; Evagelidis, A.; Derbali, R.M.; Huynh, D.N.; Dallaire, F.; Laporte, M.; Delpal, A. Distinctive Roles of Furin and TMPRSS2 in SARS-CoV-2 Infectivity. J. Virol. 2022, 96, e00128-22. [Google Scholar] [CrossRef]
- Shook, L.L.; Bordt, E.A.; Meinsohn, M.; Pepin, D.; De Guzman, R.M.; Brigida, S.; Yockey, L.J.; James, K.E.; Sullivan, M.W.; Bebell, L.M.; et al. Placental Expression of ACE2 and TMPRSS2 in Maternal Severe Acute Respiratory Syndrome Coronavirus 2 Infection: Are Placental Defenses Mediated by Fetal Sex? J. Infect. Dis. 2021, 224 (Suppl. S6), S647–S659. [Google Scholar] [CrossRef]
- Dong, L.; Pei, S.; Ren, Q.; Fu, S.; Yu, L.; Chen, H.; Chen, X.; Yin, M. Evaluation of vertical transmission of SARS-CoV-2 in utero: Nine pregnant women and their newborns. Placenta 2021, 111, 91–96. [Google Scholar] [CrossRef]
- Schiuma, G.; Beltrami, S.; Santi, E.; Scutiero, G.; Sanz, J.M.; Semprini, C.M.; Rizzo, S.; Fernandez, M.; Zidi, I.; Gafà, R.; et al. Effect of SARS-CoV-2 infection in pregnancy on CD147, ACE2 and HLA-G expression. Placenta 2023, 132, 38–43. [Google Scholar] [CrossRef]
- Rizzo, R.; Stignani, M.; Amoudruz, P.; Nilsson, C.; Melchiorri, L.; Baricordi, O.; Sverremark-Ekström, E. Allergic women have reduced sHLA-G plasma levels at delivery. Am. J. Reprod. Immunol. 2009, 61, 368–376. [Google Scholar] [CrossRef]
- Ferrer-Oliveras, R.; Mendoza, M.; Capote, S.; Pratcorona, L.; Esteve-Valverde, E.; Cabero-Roura, L.; Alijotas-Reig, J. Immunological and physiopathological approach of COVID-19 in pregnancy. Arch. Gynecol. Obstet. 2021, 304, 39–57. [Google Scholar] [CrossRef]
- Singh, M.; Bansal, V.; Feschotte, C. A single-cell RNA expression map of human coronavirus entry factors. Cell Rep. 2020, 32, 108175. [Google Scholar] [CrossRef]
- Argueta, L.B.; Lacko, L.A.; Bram, Y.; Tada, T.; Carrau, L.; Zhang, T.; Uhl, S.; Lubor, B.C.; Chandar, V.; Gil, C.; et al. SARS-CoV-2 infects syncytiotrophoblast and activates inflammatory responses in the placenta. bioRxiv 2021, 2021, 06.01.446676. [Google Scholar] [CrossRef]
- Lyden, T.W.; Anderson, C.L.; Robinson, J.M. The endothelium but not the syncytiotrophoblast of human placenta expresses caveolae. Placenta 2002, 23, 640–652. [Google Scholar] [CrossRef]
- Celik, O.; Saglam, A.; Baysal, B.; Derwig, I.E.; Celik, N.; Ak, M.; Aslan, S.N.; Ulas, M.; Ersahin, A.; Tayyar, A.T.; et al. Factors preventing materno-fetal transmission of SARS-CoV-2. Placenta 2020, 97, 1–5. [Google Scholar] [CrossRef]
- Gychka, S.G.; Brelidze, T.I.; Kuchyn, I.L.; Savchuk, T.V.; Nikolaienko, S.I.; Zhezhera, V.M.; Chermak, I.I.; Suzuki, Y.J. Placental vascular remodeling in pregnant women with COVID-19. PLoS ONE 2022, 17, e0268591. [Google Scholar] [CrossRef]
- Al-Rawaf, S.A.; Mousa, E.T.; Kareem, N.M. Correlation between Pregnancy Outcome and Placental Pathology in COVID-19 Pregnant Women. Infect. Dis. Obstet. Gynecol. 2022, 2022, 8061112. [Google Scholar] [CrossRef]
- Perna, A.; Hay, E.; De Blasiis, P.; La Verde, M.; Caprio, F.; Torella, M.; Morlando, M.; Sellitto, C.; Guerra, G.; Lucariello, A.; et al. SARS-CoV-2 Infection: A Clinical and Histopathological Study in Pregnancy. Biology 2023, 12, 174. [Google Scholar] [CrossRef]
- Sherwani, N.; Singh, N.; Neral, A.; Jaiswal, J.; Nagaria, T.; Khandwal, O. Placental Histopathology in COVID-19-Positive Mothers. J. Microbiol. Biotechnol. 2022, 32, 1098–1102. [Google Scholar] [CrossRef]
- Takada, K.; Shimodai-Yamada, S.; Suzuki, M.; Trinh, Q.D.; Takano, C.; Kawakami, K.; Asai-Sato, M.; Komatsu, A.; Okahashi, A.; Nagano, N.; et al. Restriction of SARS-CoV-2 replication in the human placenta. Placenta 2022, 127, 73–76. [Google Scholar] [CrossRef]
- Ghosh, S.; Dellibovi-Ragheb, T.A.; Kerviel, A.; Pak, E.; Qiu, Q.; Fisher, M.; Takvorian, P.M.; Bleck, C.; Hsu, V.W.; Fehr, A.R.; et al. β-Coronaviruses use lysosomes for egress instead of the biosynthetic secretory pathway. Cell 2020, 183, 1520–1535.e14. [Google Scholar] [CrossRef]
- Tian, D.; Sun, Y.; Xu, H.; Ye, Q. The emergence and epidemic characteristics of the highly mutated SARS-CoV-2 Omicron variant. J. Med. Virol. 2022, 94, 2376–2383. [Google Scholar] [CrossRef]
- Fitzgerald, B.; O’Donoghue, K.; McEntagart, N.; Gillan, J.E.; Kelehan, P.; O’Leary, J.; Downey, P.; Dean, J.; De Gascun, C.F.; Bermingham, J.; et al. Fetal deaths in Ireland due to SARS-CoV-2 placentitis caused by SARS-CoV-2 Alpha. Arch. Pathol. Lab. Med. 2022, 146, 529–537. [Google Scholar] [CrossRef]
- Shen, W.-B.; Turan, S.; Wang, B.; Cojocaru, L.; Harman, C.; Logue, J.; Reece, E.A.; Frieman, M.B.; Yang, P. A SARS-CoV-2 Delta variant case manifesting as extensive placental infection and fetal transmission. Gynecol. Obstet. Investig. 2022, 87, 165–172. [Google Scholar] [CrossRef]
- Shanes, E.D.; Miller, E.S.; Otero, S.E. Placental pathology after SARS-CoV-2 infection in the pre-variant of concern, Alpha/Gamma, Delta, or omicron eras. Int. J. Surg. Pathol. 2022. [Google Scholar] [CrossRef]
- DeSisto, C.L.; Wallace, B.; Simeone, M.R.; Polen, K.; Ko, J.Y.; Delman, D.N.; Ellington, S.R. Risk for stillbirth among women with and without COVID-19 at delivery hospitalization—United States, March 2020–September 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 1640. [Google Scholar] [CrossRef] [PubMed]
- Stenton, S.; McPortland, J.; Shukla, R.; Turner, K.; Marton, T.; Hargitai, B.; Bamber, A.; Pryce, J.; Peres, C.L.; Burguess, N.; et al. SARS-CoV-2 placentitis and pregnancy outcome: A multicentre experience during the Alpha and early Delta waves of coronavirus pandemic in England. eClinicalMedicine 2022, 47, 101389. [Google Scholar] [CrossRef]
- Slack, J.C.; Parra-Herran, C. Life after Amsterdam: Placental Pathology Consensus Recommendations and Beyond. Surg. Pathol. Clin. 2022, 15, 175–196. [Google Scholar] [CrossRef] [PubMed]
- Wong, Y.P.; Khong, T.Y.; Tan, G.C. The Effects of COVID-19 on Placenta and Pregnancy: What Do We Know So Far? Diagnostics 2021, 11, 94. [Google Scholar] [CrossRef] [PubMed]
- Carvajal, G.; Casanello, P.; Toso, A.; Farías, M.; Carrasco-Negue, K.; Araujo, K.; Valero, P.; Fuenzalida, J.; Solari, C.; Sobrevia, L. Functional consequences of SARS-CoV-2 infection in pregnant women, fetoplacental unit, and neonate. Biochim. Biophys. Acta Mol. Basis Dis. 2023, 1869, 166582. [Google Scholar] [CrossRef] [PubMed]
- Smithgall, M.C.; Murphy, E.A.; Schatz-Siemers, N.; Matrai, C.; Tu, J.; Baergen, R.N.; Yang, Y.J. Placental pathology in women vaccinated and unvaccinated against SARS-CoV-2. Am. J. Obstet. Gynecol. 2022, 227, 782–784. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| “Entry Factors” | Function/Role |
|---|---|
| Angiotensin-converting enzyme-2 (ACE2) | The target receptor for SARS-CoV-2. |
| Trans-membrane serine protease 2 (TMPRSS2), Cathepsin B and L (Cat B/L) | Two host proteases. Enables membrane fusion. |
| Furin | Reduces the virus’s dependence on proteases for entry |
| Basigin (BSG/CD147), dipeptidyl peptidase-4 (DPP4/CD26), proteases (elastase, tyrosine, and membrane-associated serine proteinases (MASPs)) | May enhance viral infectivity |
| Basigin and DPP4 co-expression with interferon-induced transmembrane protein (IFITM1-3), lymphocyte antigen 6E (LY6E) | Reduces the permissibility of the placenta to viral entry |
| Neurolipin 1 (NRP1) | Alternative receptor for SARS-CoV-2 entry into the placenta |
| Human leukocyte antigen (HLA)-G (HLA-G) | Causes an increase in the immune-tolerogenic molecule HLA-G, which can act as immune escape mechanism for SARS-CoV-2 |
| Podoplanin (PDPN) | Marker of vasculogenesis. Possible down-regulation was observed in the villous stroma of women infected during the third trimester |
| Toll-like receptors (TLRs), Internalization receptors (E-Cadherin) | Pattern recognition receptors (PRRs); the receptors can be exploited by pathogens or modulated by inflammatory signals |
| Key Findings |
|---|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tosto, V.; Meyyazhagan, A.; Alqasem, M.; Tsibizova, V.; Di Renzo, G.C. SARS-CoV-2 Footprints in the Placenta: What We Know after Three Years of the Pandemic. J. Pers. Med. 2023, 13, 699. https://doi.org/10.3390/jpm13040699
Tosto V, Meyyazhagan A, Alqasem M, Tsibizova V, Di Renzo GC. SARS-CoV-2 Footprints in the Placenta: What We Know after Three Years of the Pandemic. Journal of Personalized Medicine. 2023; 13(4):699. https://doi.org/10.3390/jpm13040699
Chicago/Turabian StyleTosto, Valentina, Arun Meyyazhagan, Malek Alqasem, Valentina Tsibizova, and Gian Carlo Di Renzo. 2023. "SARS-CoV-2 Footprints in the Placenta: What We Know after Three Years of the Pandemic" Journal of Personalized Medicine 13, no. 4: 699. https://doi.org/10.3390/jpm13040699