
Investigating the Role of Maintenance TMS Protocols for Major Depression: Systematic Review and Future Perspectives for Personalized Interventions

 , , , , , and
, , , , , and 
Abstract
:1. Introduction
2. Materials and Methods
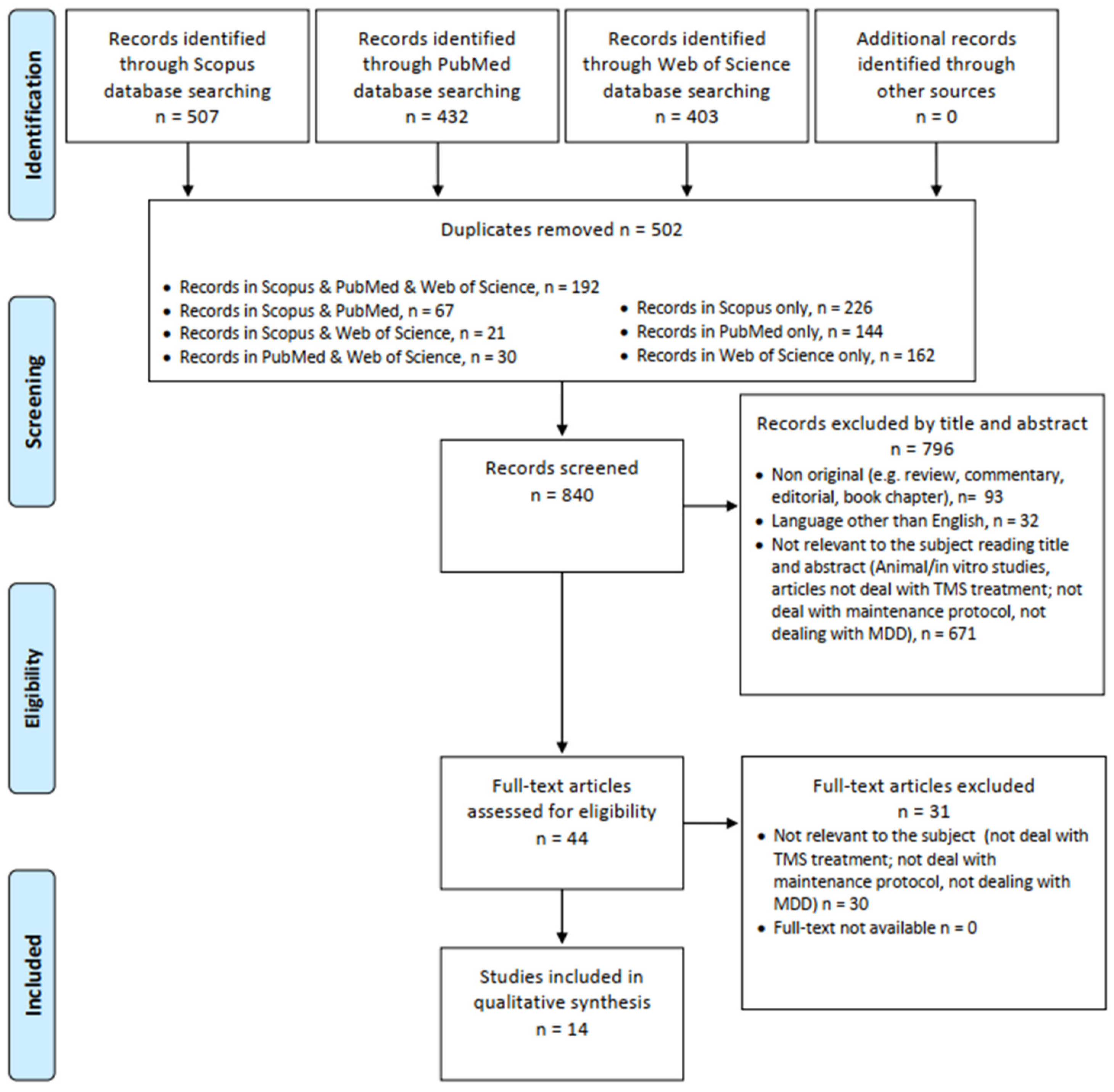
2.1. Systematic Review Procedures
2.2. Data Synthesis Strategy
2.3. Assessment of Risk of Bias
2.4. Data Extraction and Qualitative Synthesis
3. Results
3.1. Randomized Control Trials
3.2. Open-Label Studies
3.3. Case Reports and Case Series
4. Discussion
4.1. Target Populations, Stimulation Frequency, and Target Brain Areas
4.2. Frequency of Maintenance Sessions
4.3. Temporal Distance from Acute to Maintenance Protocol
4.4. Duration of Maintenance Protocol
4.5. A Possible Reliable Maintenance Protocol
4.6. Maintenance TMS: A New Resource against Recurrent Depression?
4.7. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. World Health Organization. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/depression (accessed on 19 November 2022).
- Monroe, S.M.; Harkness, K.L. Recurrence in major depression: A conceptual analysis. Psychol. Rev. 2011, 118, 655–674. [Google Scholar] [CrossRef] [PubMed]
- Gaynes, B. Assessing the risk factors for difficult-to-treat depression and treatment-resistant depression. J. Clin. Psychiatry 2016, 77 (Suppl. S1), 4–8. [Google Scholar] [CrossRef] [PubMed]
- Ruberto, V.L.; Jha, M.K.; Murrough, J.W. Pharmacological Treatments for Patients with Treatment-Resistant Depression. Pharmaceuticals 2020, 13, 116. [Google Scholar] [CrossRef] [PubMed]
- Conway, C.R.; George, M.S.; Sackeim, H.A. Toward an Evidence-Based, Operational Definition of Treatment-Resistant Depression: When Enough Is Enough. JAMA Psychiatry 2017, 74, 9–10. [Google Scholar] [CrossRef]
- Amos, T.B.; Tandon, N.; Lefebvre, P.; Pilon, D.; Kamstra, R.L.; Pivneva, I.; Greenberg, P.E. Direct and Indirect Cost Burden and Change of Employment Status in Treatment-Resistant Depression: A Matched-Cohort Study Using a US Commercial Claims Database. J. Clin. Psychiatry 2018, 79, 24–32. [Google Scholar] [CrossRef]
- Gałecki, P.; Bliźniewska-Kowalska, K. Treatment-resistant depression—Recommendations of the National Consultant in the field of psychiatry. Psychiatr. Pol. 2021, 55, 7–21. [Google Scholar] [CrossRef]
- Melfi, C.A.; Chawla, A.J.; Croghan, T.W.; Hanna, M.P.; Kennedy, S.; Sredl, K. The effects of adherence to antidepressant treatment guidelines on relapse and recurrence of depression. Arch. Gen. Psychiatry 1998, 55, 1128–1132. [Google Scholar] [CrossRef]
- Bosworth, H.B.; Voils, C.I.; Potter, G.G.; Steffens, D.C. The effects of antidepressant medication adherence as well as psychosocial and clinical factors on depression outcome among older adults. Int. J. Geriatr. Psychiatry 2008, 23, 129–134. [Google Scholar] [CrossRef]
- Miron, J.-P.; Jodoin, V.D.; Lespérance, P.; Blumberger, D.M. Repetitive transcranial magnetic stimulation for major depressive disorder: Basic principles and future directions. Ther. Adv. Psychopharmacol. 2021, 11, 1–14. [Google Scholar] [CrossRef]
- Miuli, A.; Sepede, G.; Stigliano, G.; Mosca, A.; Di Carlo, F.; D’andrea, G.; Lalli, A.; Spano, M.C.; Pettorruso, M.; Martinotti, G.; et al. Hypomanic/manic switch after transcranial magnetic stimulation in mood disorders: A systematic review and meta-analysis. World J. Psychiatry 2021, 11, 477–490. [Google Scholar] [CrossRef]
- D’Andrea, G.; Pettorruso, M.M.; D’Andrea, A.; Collevecchio, R.; Santovito, M.C.; Miuli, A.; Di Carlo, F.; Sensi, S.L.M.; Martinotti, G.M.; di Giannantonio, M. Combining Dopamine Agonists with Accelerated Repetitive Transcranial Magnetic Stimulation. J. ECT 2022, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.-M.; Li, C.-T.; Tsai, S.-J. Current Updates on Newer Forms of Transcranial Magnetic Stimulation in Major Depression. Adv. Exp. Med. Biol. 2021, 1305, 333–349. [Google Scholar] [CrossRef] [PubMed]
- Chou, P.-H.; Lin, Y.-F.; Lu, M.-K.; Chang, H.-A.; Chu, C.-S.; Chang, W.H.; Kishimoto, T.; Sack, A.T.; Su, K.-P. Personalization of Repetitive Transcranial Magnetic Stimulation for the Treatment of Major Depressive Disorder According to the Existing Psychiatric Comorbidity. Clin. Psychopharmacol. Neurosci. Off. Sci. J. Korean Coll. Neuropsychopharmacol. 2021, 19, 190–205. [Google Scholar] [CrossRef]
- Dalhuisen, I.; Ackermans, E.; Martens, L.; Mulders, P.; Bartholomeus, J.; de Bruijn, A.; Spijker, J.; van Eijndhoven, P.; Tendolkar, I. Longitudinal effects of rTMS on neuroplasticity in chronic treatment-resistant depression. Eur. Arch. Psychiatry Clin. Neurosci. 2021, 271, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.C.; Higgins, E.S.; George, M.S. Synaptic Plasticity 101: The Story of the AMPA Receptor for the Brain Stimulation Practitioner. Neuromodulation 2021, 25, 1289–1298. [Google Scholar] [CrossRef]
- Arnsten, A.F.T.; Joyce, M.K.P.; Roberts, A.C. The Aversive Lens: Stress effects on the prefrontal-cingulate cortical pathways that regulate emotion. Neurosci. Biobehav. Rev. 2023, 145, 105000. [Google Scholar] [CrossRef] [PubMed]
- Spano, M.C.; Lorusso, M.; Pettorruso, M.; Zoratto, F.; Di Giuda, D.; Martinotti, G.; Di Giannantonio, M. Anhedonia across borders: Transdiagnostic relevance of reward dysfunction for noninvasive brain stimulation endophenotypes. CNS Neurosci. Ther. 2019, 25, 1229–1236. [Google Scholar] [CrossRef]
- Arici, C.; Benatti, B.; Cafaro, R.; Cremaschi, L.; Degoni, L.; Pozzoli, S.; Oldani, L.; Molteni, L.; Giorgetti, F.; Priori, A.; et al. A 6-month follow-up study on response and relapse rates following an acute trial of repetitive transcranial magnetic stimulation in patients with major depression. CNS Spectr. 2022, 27, 93–98. [Google Scholar] [CrossRef]
- Demirtas-Tatlidede, A.; Mechanic-Hamilton, D.; Press, D.Z.; Perlman, C.; Stern, W.M.; Thall, M.; Pascual-Leone, A. An open-label, prospective study of repetitive transcranial magnetic stimulation (rTMS) in the long-term treatment of refractory depression: Reproducibility and duration of the antidepressant effect in medication-free patients. J. Clin. Psychiatry 2008, 69, 930–934. [Google Scholar] [CrossRef]
- Fitzgerald, P.B.; Benitez, J.; de Castella, A.R.; Brown, T.L.; Daskalakis, Z.J.; Kulkarni, J. Naturalistic study of the use of transcranial magnetic stimulation in the treatment of depressive relapse. Aust. New Zealand J. Psychiatry 2006, 40, 764–768. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Bernardo, W.M. PRISMA statement and PROSPERO. Int. Braz. J. Urol. 2017, 43, 383–384. [Google Scholar] [CrossRef] [PubMed]
- Benadhira, R.; Thomas, F.; Bouaziz, N.; Braha, S.; Andrianisaina, P.S.-K.; Isaac, C.; Moulier, V.; Januel, D. A randomized, sham-controlled study of maintenance rTMS for treatment-resistant depression (TRD). Psychiatry Res. 2017, 258, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Levkovitz, Y.; Isserles, M.; Padberg, F.; Lisanby, S.H.; Bystritsky, A.; Xia, G.; Tendler, A.; Daskalakis, Z.J.; Winston, J.L.; Dannon, P.; et al. Efficacy and safety of deep transcranial magnetic stimulation for major depression: A prospective multicenter randomized controlled trial. World Psychiatry 2015, 14, 64–73. [Google Scholar] [CrossRef]
- Wang, H.-N.; Wang, X.-X.; Zhang, R.-G.; Wang, Y.; Cai, M.; Zhang, Y.-H.; Sun, R.-Z.; Guo, L.; Qiao, Y.-T.; Liu, J.-C.; et al. Clustered repetitive transcranial magnetic stimulation for the prevention of depressive relapse/recurrence: A randomized controlled trial. Transl. Psychiatry 2017, 7, 1292. [Google Scholar] [CrossRef]
- Fitzgerald, P.B.; Grace, N.; Hoy, K.E.; Bailey, M.; Daskalakis, Z.J. An open label trial of clustered maintenance rTMS for patients with refractory depression. Brain Stimul. 2013, 6, 292–297. [Google Scholar] [CrossRef]
- Haesebaert, F.; Moirand, R.; Schott-Pethelaz, A.-M.; Brunelin, J.; Poulet, E. Usefulness of repetitive transcranial magnetic stimulation as a maintenance treatment in patients with major depression. World J. Biol. Psychizatry Off. J. World Fed. Soc. Biol. Psychiatry 2018, 19, 74–78. [Google Scholar] [CrossRef]
- Harel, E.V.; Rabany, L.; Deutsch, L.; Bloch, Y.; Zangen, A.; Levkovitz, Y. H-coil repetitive transcranial magnetic stimulation for treatment resistant major depressive disorder: An 18-week continuation safety and feasibility study. World J. Biol. Psychiatry Off. J. World Fed. Soc. Biol. Psychiatry 2014, 15, 298–306. [Google Scholar] [CrossRef]
- Philip, N.S.; Dunner, D.L.; Dowd, S.M.; Aaronson, S.T.; Brock, D.G.; Carpenter, L.L.; Demitrack, M.A.; Hovav, S.; Janicak, P.G.; George, M.S. Can Medication Free, Treatment-Resistant, Depressed Patients Who Initially Respond to TMS Be Maintained Off Medications? A Prospective, 12-Month Multisite Randomized Pilot Study. Brain Stimul. 2016, 9, 251–257. [Google Scholar] [CrossRef]
- Pridmore, S.; May, T. Relapse prevention (RP) TMS. Brain Stimul. 2018, 11, 1391–1392. [Google Scholar] [CrossRef]
- Pridmore, S.; Erger, S.; Rybak, M.; Kelly, E.; May, T. Early relapse (ER) transcranial magnetic stimulation (TMS) in treatment resistant major depression. Brain Stimul. 2018, 11, 1098–1102. [Google Scholar] [CrossRef] [PubMed]
- Richieri, R.; Guedj, E.; Michel, P.; Loundou, A.; Auquier, P.; Lançon, C.; Boyer, L. Maintenance transcranial magnetic stimulation reduces depression relapse: A propensity-adjusted analysis. J. Affect. Disord. 2013, 151, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Yip, A.G.; George, M.S.; Tendler, A.; Roth, Y.; Zangen, A.; Carpenter, L.L. 61% of unmedicated treatment resistant depression patients who did not respond to acute TMS treatment responded after four weeks of twice weekly deep TMS in the Brainsway pivotal trial. Brain Stimul. 2017, 10, 847–849. [Google Scholar] [CrossRef]
- O’Reardon, J.P.; Blumner, K.H.; Peshek, A.D.; Pradilla, R.R.; Pimiento, P.C. Long-term maintenance therapy for major depressive disorder with rTMS. J. Clin. Psychiatry 2005, 66, 1524–1528. [Google Scholar] [CrossRef]
- Chatterjee, B.; Kumar, N.; Jha, S. Role of repetitive transcranial magnetic stimulation in maintenance treatment of resistant depression. Indian J. Psychol. Med. 2012, 34, 286–289. [Google Scholar] [CrossRef] [PubMed]
- Langguth, B.; Landgrebe, M.; Zowe, M.; Gerst, M.; Hajak, G.; Eichhammer, P. Repetitive transcranial magnetic stimulation for maintenance treatment of depression: A case report. J. Clin. Psychiatry 2006, 67, 835–836. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Zhou, C.; Wu, B.; Wang, Y.; Li, Q.; Wei, Y.; Yang, D.; Mu, J.; Zhu, D.; Zou, D.; et al. Left versus right repetitive transcranial magnetic stimulation in treating major depression: A meta-analysis of randomised controlled trials. Psychiatry Res. 2013, 210, 1260–1264. [Google Scholar] [CrossRef]
- Brunoni, A.R.; Chaimani, A.; Moffa, A.H.; Razza, L.B.; Gattaz, W.F.; Daskalakis, Z.J.; Carvalho, A.F. Repetitive Transcranial Magnetic Stimulation for the Acute Treatment of Major Depressive Episodes: A Systematic Review With Network Meta-analysis. JAMA Psychiatry 2017, 74, 143–152. [Google Scholar] [CrossRef]
- Baeken, C. Accelerated rTMS: A Potential Treatment to Alleviate Refractory Depression. Front. Psychol. 2018, 9, 2017. [Google Scholar] [CrossRef]
- Rachid, F. Accelerated transcranial magnetic stimulation for the treatment of Patients with depression: A review. Asian J. Psychiatr. 2019, 40, 71–75. [Google Scholar] [CrossRef]
- Klomjai, W.; Katz, R.; Lackmy-Vallee, A. Basic principles of transcranial magnetic stimulation (TMS) and repetitive TMS (rTMS). Ann. Phys. Rehabil. Med. 2015, 58, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Sawada, N.; Uchida, H.; Suzuki, T.; Watanabe, K.; Kikuchi, T.; Handa, T.; Kashima, H. Persistence and compliance to antidepressant treatment in patients with depression: A chart review. BMC Psychiatry 2009, 9, 38. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, S.H.; Lam, R.W.; McIntyre, R.S.; Tourjman, S.V.; Bhat, V.; Blier, P.; Hasnain, M.; Jollant, F.; Levitt, A.J.; MacQueen, G.M.; et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: Section 3. Pharmacological Treatments. Can. J. Psychiatry 2016, 61, 540–560. [Google Scholar] [CrossRef] [PubMed]
- The Joanna Briggs Institute; Lockwood, C.; Porrit, K.; Munn, Z.; Rittenmeyer, L.; Salmond, S.; Bjerrum, M.; Loveday, H.; Carrier, J.; Stannard, D.; et al. Appendix 7.4 Critical Appraisal Checklist for Case Reports. Joanna Briggs Institute Reviewer’s Manual. 2017. Available online: https://jbi-global-wiki.refined.site/space/MANUAL/4689072 (accessed on 18 April 2023).
- The Joanna Briggs Institute; Lockwood, C.; Porrit, K.; Munn, Z.; Rittenmeyer, L.; Salmond, S.; Bjerrum, M.; Loveday, H.; Carrier, J.; Stannard, D.; et al. Appendix 7.3 Critical Appraisal Checklists for Case Series. Joanna Briggs Institute Reviewer’s Manual. 2017. Available online: https://jbi-global-wiki.refined.site/space/MANUAL/4689063/Appendix%2B7.3%2BCritical%2Bappraisal%2Bchecklists%2Bfor%2Bcase%2Bseries (accessed on 18 April 2023).
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomized studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]


{kind=link}
| Reference | Study Design | Sample | Acute Protocol | Distance between Acute and Maintenance Protocol | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Size (n) | Type | Duration (Weeks) | Type of TMS | Coil Position | Frequency; Intensity (% RMT) | Stimulation Time; N of Pulses | N of Total Sessions | |||
| Benadhira et al., 2017 [24] | RCT | 58 (35 to maintenance) | TRD | 4 | rTMS | LDLPFC | 10 Hz; 110% | 15 min; 2000 | 20 | 1 week |
| Levkovitz et al., 2015 [25] | RCT double-blinded | 181: 89 active, 91 sham | TRD | 4 | dTMS | LDLPFC | 15 Hz; 120% | 30 min; 980 | 20 | 1 week |
| Wang et al., 2017 [26] | RCT assessor-blinded | 281 tot (rTMS = 91, ADP = 108, rTMS + ADP = 82) | MDD | ND | rTMS | LDLPFC | ND | ND | ND | ND |
| Fitzgerald et al., 2013 [27] | OL | 35 | 26: MDD; 9: BD | ND | rTMS | LDLPFC; RDLPFC; bilateral | 10 Hz on LDLPFC at 110% (N = 14); 1–5 Hz on RDLPFC (N = 12); 1–1 Hz Bilateral (N = 6); 10–1 Hz Bilateral (N = 3) at 110% | 15 min; 1500 (LDLPFC); 900 (LDLPFC) | ND | 1–3 months |
| Haesebaert et al., 2018 [28] | OL | 66 (25 rTMS; 22 Venlafaxine; 19 Combined) | TRD | 2 to 6 | rTMS | RDLPFC | ND | ND | ND | 4 weeks |
| Harel et al., 2012 [29] | OL | 29 | MDD | 4 | rTMS | LDLPFC | 20 Hz; 120% | 15 min; 1680; | 20 | 1 week |
| Philip et al., 2016 [30] | OL | 49:23 maintenance TMS protocol (SCH group), 26 observation (OBS group) | MDD | 6 weeks + 3 weeks of TMS tapering | rTMS | 5,5 cm anterior from the MT location, along a left superior oblique plane | 10 Hz; 120% | 37 min 30 s; 3000 | 30 | 4 weeks |
| Pridmore et al., 2018a [31] | OL | 39 | TRD | 4 | rTMS | LDLPFC | 10 Hz; 110% | 12 min; 3000 | 40 | 4 weeks |
| Pridmore et al., 2018b [32] | OL | 14 | TRD | 4 | rTMS | LDLPFC | 10 Hz; 110% | 12 min; 3000 | 40 | 4 weeks |
| Richieri et al., 2013 [33] | OL | 59: 20 weeks of maintenance TMS (n = 37) or no additional TMS treatment (n = 22) | TRD | 4 | rTMS | LDLPFC-RDLPFC | LDLPFC: 10 Hz; 120% RDLPFC: 1 Hz; 80% | LDLPFC: 20 min; 2.000 RDLPFC: 14 min; 720 | 20 | ND |
| Yip et al., 2017 [34] | OL double-blinded | 33 | TRD | 4 | dTMS | LDLPFC | 18 Hz; 120% | 20 min; 1980 | 20 | 1 week |
| O’ Reardon et al. 2006 [35] | CS | 10 | TRD | ND | rTMS | LDLPFC | ND | 20 or 30 min; 2000 or 3000 | ND | 1 week |
| Chatterjee et al., 2012 [36] | CR | 1 (three separate maintenance treatments: a; b; c) | TRD | 3 | rTMS | LDLPFC | 15 Hz; 100% | 22 min; 4000 | 20 | a: 6 weeks; b: 7 weeks; c: 12 weeks. |
| Langguth et al., 2006 [37] | CR | 1 | MDD | 3 | rTMS | LDLPFC | 20 Hz; 90% | 18 min; 2000 | 15 | 5 weeks |
| Reference | Study Design | Sample | Maintenance Protocol | Results | ||||
|---|---|---|---|---|---|---|---|---|
| Size (n) | Type | Duration (weeks) and n of Stimulation/Week | Frequency; Intensity (% RMT) | Stimulation Time; N of Pulses | N of Total Sessions | |||
| Benadhira et al., 2017 [24] | RCT | 58 (35 to maintenance) | TRD | 44 weeks (11 months); 3/wk for 2 wks; 2/wk for 2 wks; 1/wk for 2 months; 2 per month for 8 months. | 10 Hz; 110% | 15 min; 2000 | 34 | HDRS: Significant improvement in active group from 1st to 4th month. No difference from 5th month to endpoint. No significant differences in HDRS-17, HAD, BDI and CGI scores at any endpoint. Effect of active treatment could be sustained for two months (no clinical differences at 2nd and 3rd month between groups). Antidepressant effect of maintenance sessions appeared three months after the treatment. One session per week could maintain antidepressant effect. Two sessions/month could be insufficient to maintain antidepressant effect. |
| Levkovitz et al., 2015) [25] | RCT double-blinded | 181:89 active, 91 sham | TRD | 2/wk dTMS; 12 weeks following the acute-phase, | 18 Hz; 120% | 20 min; 1980 | 24 | Response and remission rates were higher in the dTMS than in the sham group (response: 38.4 vs. 21.4%, p50.013; remission: 32.6 vs. 14.6%, p = 0.005). These differences between active and sham treatment were stable during the 12-week maintenance phase. From week 5 (end of acute phase) to week 16 (end of mantainance phase) response rates increase from 38.4% to 44.3% in active group, and from 21.3% to 25.6% in the sham group. |
| Wang et al., 2017 [26] | RCT assessor-blinded | 281 tot (rTMS = 91, ADP = 108, rTMS + ADP = 82) | MDD | 52 weeks, monthly clustered rTMS maintenance treatment, which involved 10 sessions over a 5-day period for the first 3 months and 5 sessions over a 3-day period thereafter. | 10 Hz; 120%; if not tolerated 80% | 15 min; 1150 | 75 | rTMS + ADP and rTMS significantly reduced the risk of relapse/recurrence compared with ADP (p = 0.000), with hazard ratios of 0.297 and 0.466, respectively. Both rTMS-containing regimens produced significantly lower relapse/recurrence rates than ADP (15.9% and 24.2% vs. 44.4%, p < 0.001). TMS + ADP reduce the risk of relapse/recurrence and the relapse/ recurrence rate by 8.3%. |
| Fitzgerald et al., 2013 [27] | OL | 35 | 26: MDD; 9: BD | Mean duration: 12 ± 9.7 months; 5 stimulations/month | 10 Hz on LDLPFC at 110% (N = 14); 1–5 Hz on RDLPFC (N = 12); 1–10 Hz Bilateral. 110% | 15 min. N of pulses: 1500 (LDLPFC); 900 (LDLPFC) | 5–120 | On 25 relapses (mean 10.2 months), 15 withdrew and 10 responded to a new active rTMS protocol followed by maintenance On 10 remissions, 4 withdrew and 6 remained well (mean 12.0 months). |
| Haesebaert et al., 2018 [28] | OL | 66 (25 rTMS; 22 Venlafaxina; 19 Combined) | TRD | 52 2/wk for one month; 1/wk for 2 months; once every two weeks for 9 months. | 1 Hz; 120% | 6 trains of a 1-min duration separated by 30-s inter-train “off” periods; 360 | 34 | Remission rate -rTMS group: 18.7% (n = 3) -venlafaxine group: 35.3% (n = 6) -combination group: 33.3% (n = 4) No difference between the groups regarding the number of patients who maintained remission at the end of the 12-month follow-up (Chi2 = 1.25; p = 0.3) Non-relapse rate (HDRS < 15) -rTMS group: 40.0% (10 of 25) -venlafaxine group: 45.1% (10 of 22) (Chi2 = 0.33; p = 0.8) -combination group: 36.88% (7 of 19) Relapse rate -rTMS group: 4.0% -venlafaxine group: 4.5% -combination group: 5.3% (Chi2 = 0.04; p = 0.9) Probability of non-relapse -rTMS group: 80.0% -venlafaxine group: 59.1% -combination group: 78.9% No significant difference was identified between the three groups regarding the survival distribution using the log rank method (Chi2 = 3.2848; p = 0.19). |
| Harel et al., 2012 [29] | OL | 29 | MDD | Continuation type I: 8 weeks, twice/week Continuation Type II: 10 weeks, once/week | 20 Hz; 120% | 14 min; 1680 | Continuation type I: 16 sessions Continuation Type II: 10 sessions | Kaplan–Meier estimated probability of response was 46.15% (SE = 9.78%) at the end of the acute phase, and 81.12% (SE = 9.32%) at the end of the study (22 weeks). Probability of remission at the end of the acute phase was 26.92% (SE = 8.70%) and 71.45% (SE = 10.99%) at the end of the study. Response in the acute phase was indicative of response in the continuation phases. |
| Philip et al., 2016 [30] | OL | 49:23 maintenance TMS protocol (SCH group), 26 observation (OBS group) | MDD | 40 weeks; once every month | 10 Hz; 120% | 37 min 30 s; 3000 | 11 | 32.7% completed all 53 weeks of the study -no statistically significant group differences in the primary outcome variable (i.e., the number of patients who did not require TMS reintroduction at any observation point during the maintenance phase): 39% in the SCH group and 35% in the OBS group à maintenance TMS schedule of only one treatment per month is not sufficient to prevent return of depressive symptoms within the year |
| Pridmore et al., 2018a [31] | OL | 39 | TRD | 20 weeks—once every month over 3 or 5 days/week | 10 Hz; 110% | 12 min; 3000 | 50 | Before TMS series 70% were no longer in remission (being in partial remission or relapse), and after TMS series, 79% were in remission. Pre-maintance HAM-6 = 6.24 ± 2.78; post-maintenance HAM-6 = 3.30 ± 2.28. |
| Pridmore et al., 2018b [32] | OL | 14 | TRD | 52 weeks—once month over 3 or 5 days/week | 10 Hz; 110% | 12 min; 3000 | at least 60 sessions | 12/14 Patients (85%) were on remission during and after the TMS mantainance period. Relapse rate: 15% |
| Richieri et al., 2013 [33] | OL | 59: 20 weeks of maintenance TMS (n = 37) or no additional TMS treatment (n = 22) | TRD | three sessions in week 1, two sessions in weeks 2 and 3, one session per week for 2 weeks one session per 2 weeks for 2 months, and then one session per month for 2 months. | 10 Hz; 120% 1 Hz; 80% | LDLPFC: 20 min; 2.000 RDLPFC: 14 min; 720 | 15 | Maintenance TMS was associated with a significantly lower relapse rate (37.8% vs 81.8%) in patients with pharmacoresistant depression in routine practice among responders. |
| Yip et al., 2017 [34] | OL double-blinded | 33 | TRD | 2/wk dTMS 12 weeks following the acute-phase, | 18 Hz; 120% | 20 min; 1980 | 24 | 24 participants (72.7%) achieved responder status during at least one rating with dTMS continuation—20 (60.6%) within four weeks, with 13 (39.4%) consistently meeting response criteria for the duration of the study. 20 (63.6%) achieved remission status at some point during treatment continuation. |
| O’ Reardon et al., 2006 [35] | CS | 10 | TRD | 1 or 2 session/weekly for periods ranging from 24 weeks to 288 weeks | 10 Hz;100% (n = 9) 20 Hz;100% (n = 1) | 20 or 30 min; 2000 or 3000 | patients with marked benefits: mean 257 sessions; patients with moderate benefits: mean 125 sessions; patients with minimal benefits: mean 98 sessions | 7/10 Subjects experienced marked or moderate benefit. 3 cases were without any oral antidepressant medications |
| Chatterjee et al., 2012 [36] | CR | 1 | TRD | a: 1 wk; 5/wk; b: 8 wk; 5/wk; c: 8 wk; 5/wk. | 20 Hz; 100% | 22 min; 4000 | a: 5; b: 20; c: 20. | In all the three mantenaince protocols (a, b, c), remission from the current MDE was achieved (MADRS score: a = 6, b = 4, c = 4) |
| Langguth et al., 2006 [37] | CR | 1 | MDD | 52 weeks 5 sessions of daily rTMS/monthly | 20 Hz; 90% | 18 min; 2000 | 60 | HAM-D score pre-TMS = 30 HAM-D score post-TMS: ranged between 0 and 3 every treatment week in 12 months |
| Maintenance Protocols | Description | Included Studies |
|---|---|---|
| Tapering rTMS | Referring to a progressive and gradual reduction of session and stimulation across several weeks. | Benhadira et al., 2017 [24]; Haesebaert et al., 2018 [28]; Philip et al., 2016 [30]; Richieri et al., 2013 [33] |
| Cluster rTMS | 5 intensive sessions delivered over 2.5–5 days, separated by monthly or greater non-treatment periods. | Fitzgerald et al., 2013 [27]; Langguth et al., 2006 [37]; Pridmore et al., 2018a [31]; Pridmore et al., 2018b [32]; Wang et al., 2017 [26] |
| Continuous rTMS | Maintenance sessions are delivered within the first week after acute protocol. | Harel et al., 2012 [29]; Levkovitz et al., 2015 [25]; O’ Reardon et al., 2006 [35]; Yip et al., 2017 [34] |
| Rescue rTMS | Multiple protocols delivered during a relapse of a depressive episode | Chatterjee et al., 2012 [36] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
d’Andrea, G.; Mancusi, G.; Santovito, M.C.; Marrangone, C.; Martino, F.; Santorelli, M.; Miuli, A.; Di Carlo, F.; Signorelli, M.S.; Clerici, M.; et al. Investigating the Role of Maintenance TMS Protocols for Major Depression: Systematic Review and Future Perspectives for Personalized Interventions. J. Pers. Med. 2023, 13, 697. https://doi.org/10.3390/jpm13040697
d’Andrea G, Mancusi G, Santovito MC, Marrangone C, Martino F, Santorelli M, Miuli A, Di Carlo F, Signorelli MS, Clerici M, et al. Investigating the Role of Maintenance TMS Protocols for Major Depression: Systematic Review and Future Perspectives for Personalized Interventions. Journal of Personalized Medicine. 2023; 13(4):697. https://doi.org/10.3390/jpm13040697
Chicago/Turabian Styled’Andrea, Giacomo, Gianluca Mancusi, Maria Chiara Santovito, Carlotta Marrangone, Fabrizio Martino, Mario Santorelli, Andrea Miuli, Francesco Di Carlo, Maria Salvina Signorelli, Massimo Clerici, and et al. 2023. "Investigating the Role of Maintenance TMS Protocols for Major Depression: Systematic Review and Future Perspectives for Personalized Interventions" Journal of Personalized Medicine 13, no. 4: 697. https://doi.org/10.3390/jpm13040697