
Radiation Exposure and Frequency of Dental, Bitewing and Occlusal Radiographs in Children and Adolescents
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Dose Values
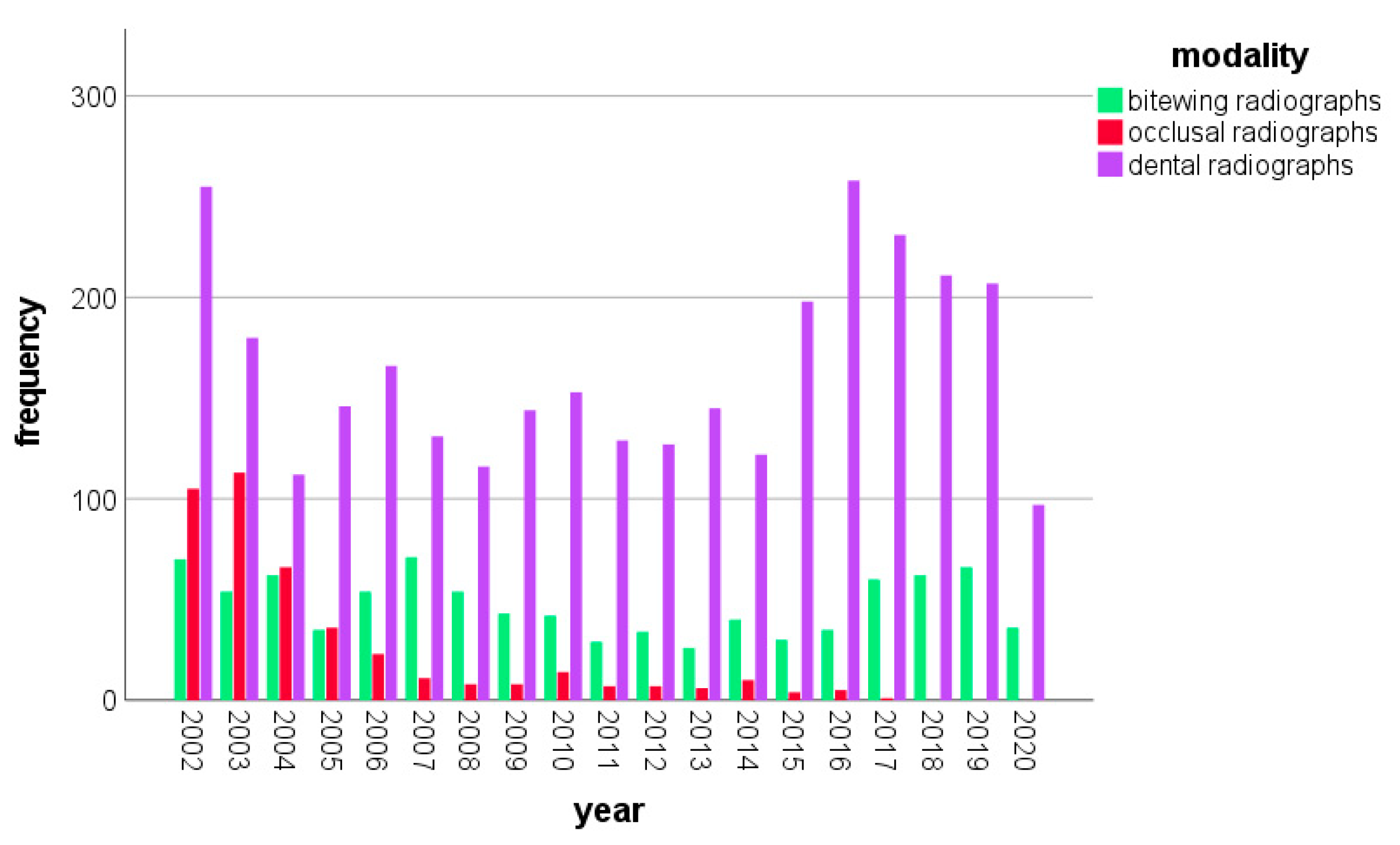
3.2. Annual Frequencies of Intraoral Dental Radiographs in Children and Adolescents
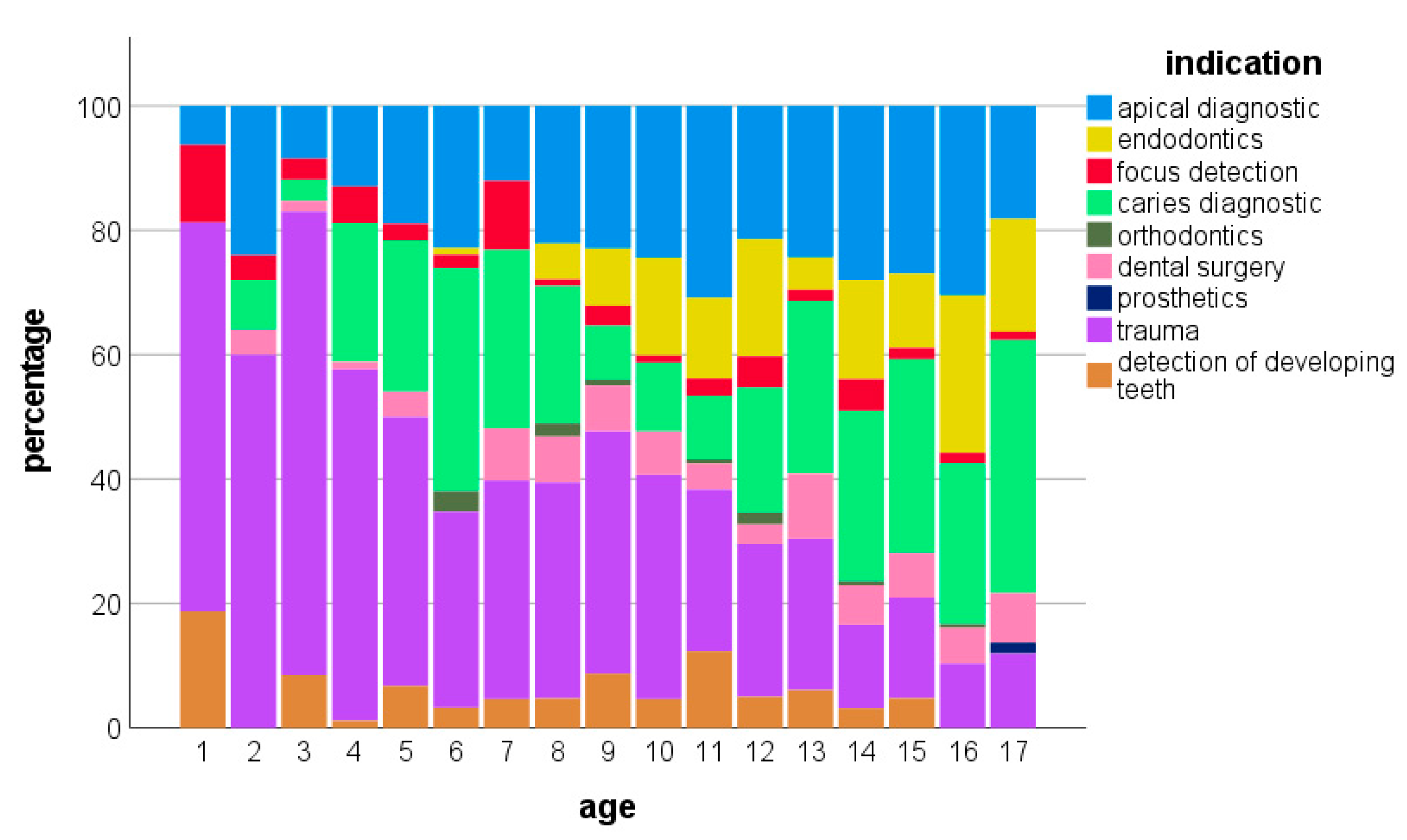
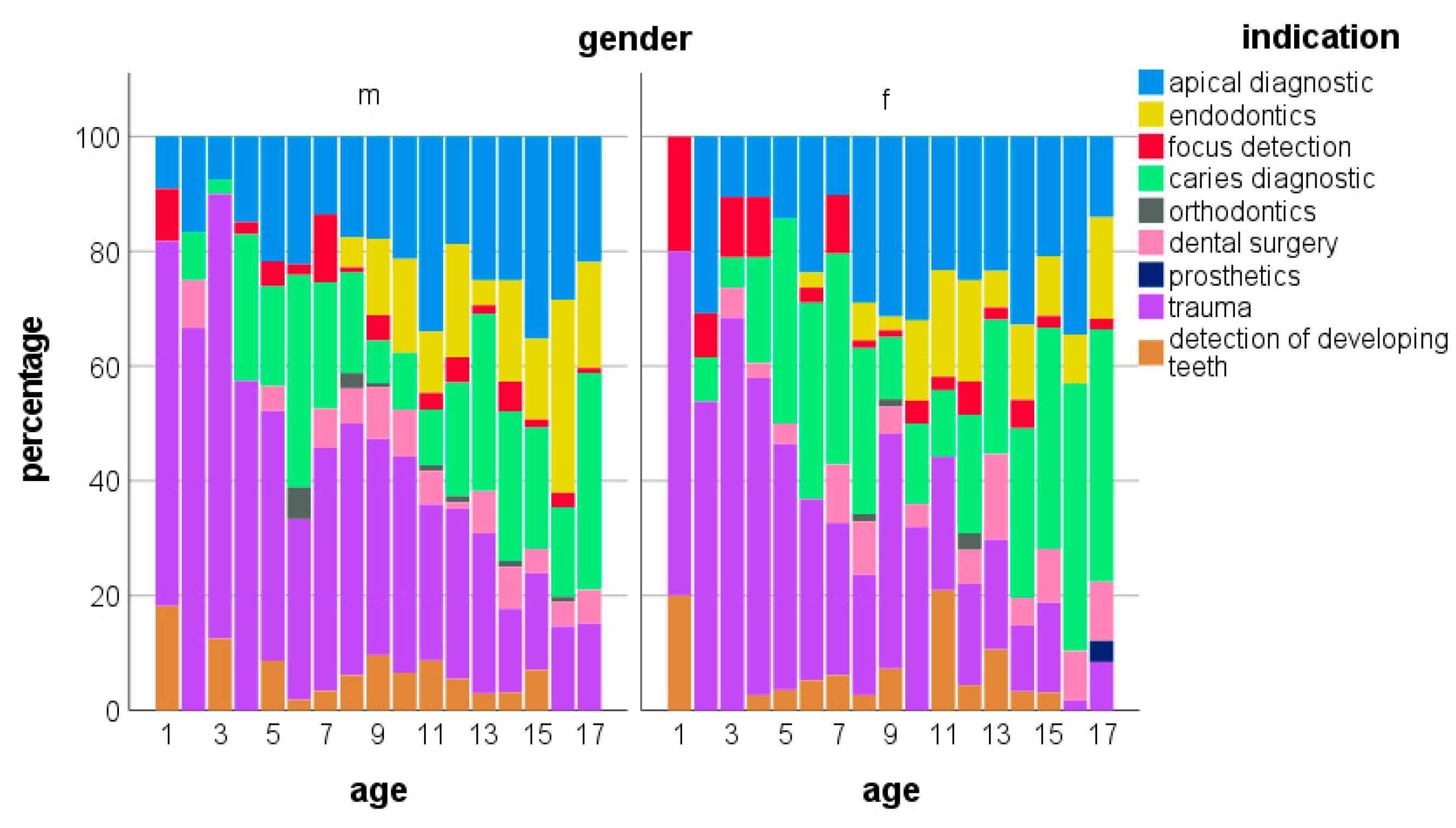
3.3. Indications for Intraoral Dental Radiographs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bundesamt für Strahlenschutz. Röntgendiagnostik: Häufigkeit und Strahlenexposition für die deutsche Bevölkerung. 2018. Available online: http://www.bfs.de/de/ion/medizin/diagnostik/roentgen/haeufigkeit_strahlenexposition.html (accessed on 2 March 2023).
- European Commission. Directorate-General for Energy, Medical Radiation Exposure of the European Population, Publications Office. 2015. Available online: https://data.europa.eu/doi/10.2833/708119 (accessed on 2 March 2023).
- Kühnisch, J.; Anttonen, V.; Duggal, M.S.; Spyridonos, M.L.; Rajasekharan, S.; Sobczak, M.; Stratigaki, E.; Van Acker, J.W.G.; Aps, J.K.M.; Horner, K.; et al. Best clinical practice guidance for prescribing dental radiographs in children and adolescents: An EAPD policy document. Eur. Arch. Paediatr. Dent. 2020, 21, 375–386. [Google Scholar] [CrossRef] [PubMed]
- White, S.C.; Mallya, S.M. Update on the biological effects of ionizing radiation, relative dose factors and radiation hygiene. Aust. Dent. J. 2012, 57 (Suppl. S1), 2–8. [Google Scholar] [CrossRef] [PubMed]
- Hall, J.D.; Godwin, M.; Clarke, T. Lifetime exposure to radiation from imaging investigations. Can. Fam. Physician 2006, 52, 976–977. [Google Scholar]
- Preethi, N.; Chikkanarasaiah, N.; Bethur, S.S. Genotoxic effects of X-rays in buccal mucosal cells in children subjected to dental radiographs. BDJ Open 2016, 2, 16001. [Google Scholar] [CrossRef] [PubMed]
- Hedesiu, M.; Marcu, M.; Salmon, B.; Pauwels, R.; Oenning, A.C.; Almasan, O.; Roman, R.; Baciut, M.; Jacobs, R. Irradiation provided by dental radiological procedures in a pediatric population. Eur. J. Radiol. 2018, 103, 112–117. [Google Scholar] [CrossRef]
- Benn, D.K.; Vig, P.S. Estimation of x-ray radiation related cancers in US dental offices: Is it worth the risk? Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2021, 132, 597–608. [Google Scholar] [CrossRef]
- Espelid, I.; Mejàre, I.; Weerheijm, K. EAPD guidelines for use of radiographs in children. Eur. J. Paediatr. Dent. Off. J. Eur. Acad. Paediatr. Dent. 2003, 4, 40–48. [Google Scholar]
- American Academy of Pediatric Dentistry. Prescribing dental radiographs for infants, children, adolescents, and individuals with special health care needs. Ref. Man. Pediatr. Dent. 2021, 273–276. [Google Scholar]
- White, S.C.; Scarfe, W.C.; Schulze, R.K.; Lurie, A.G.; Douglass, J.M.; Farman, A.G.; Law, C.S.; Levin, M.D.; Sauer, R.A.; Valachovic, R.W.; et al. The Image Gently in Dentistry campaign: Promotion of responsible use of maxillofacial radiology in dentistry for children. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 118, 257–261. [Google Scholar] [CrossRef]
- Oenning, A.C.; Jacobs, R.; Pauwels, R.; Stratis, A.; Hedesiu, M.; Salmon, B. Cone-beam CT in paediatric dentistry: DIMITRA project position statement. Pediatr. Radiol. 2018, 48, 308–316. [Google Scholar] [CrossRef]
- Lee, H.; Badal, A. A Review of Doses for Dental Imaging in 2010–2020 and Development of a Web Dose Calculator. Radiol. Res. Pract. 2021, 2021, 6924314. [Google Scholar] [CrossRef]
- Looe, H.K.; Eenboom, F.; Chofor, N.; Pfaffenberger, A.; Steinhoff, M.; Rühmann, A.; Poplawski, A.; Willborn, K.; Poppe, B. Conversion coefficients for the estimation of effective doses in intraoral and panoramic dental radiology from dose-area product values. Radiat. Prot. Dosim. 2008, 131, 365–373. [Google Scholar] [CrossRef]
- Gosch, D.; Gosch, K.; Kahn, T. Konversionsfaktoren zur Ermittlung der effektiven Dosis für Patienten aus dem Dosisflächenprodukt bei Röntgendurchleuchtungsuntersuchungen. Rofo 2007, 179, 1035–1042. [Google Scholar] [CrossRef]
- Aps, J.K.M.; Lim, L.Z.; Tong, H.J.; Kalia, B.; Chou, A.M. Diagnostic efficacy of and indications for intraoral radiographs in pediatric dentistry: A systematic review. Eur. Arch. Paediatr. Dent. 2020, 21, 429–462. [Google Scholar] [CrossRef]
- Granlund, C.; Thilander-Klang, A.; Ylhan, B.; Lofthag-Hansen, S.; Ekestubbe, A. Absorbed organ and effective doses from digital intra-oral and panoramic radiography applying the ICRP 103 recommendations for effective dose estimations. Br. J. Radiol. 2016, 89, 20151052. [Google Scholar] [CrossRef]
- ICRP. The 2007 Recommendations of the International Commission on Radiological Protection. ICRP Publication 103. Ann. ICRP 2007, 37, 1–32. [Google Scholar] [CrossRef]
- Kiefer, H.; Lambrecht, T.; Roth, J. Dose exposure from analog and digital full mouth radiography and panoramic radiography. Schweiz. Monatsschr. Zahnmed. 2004, 114, 687–693. [Google Scholar]
- Li, Y.; Huang, B.; Cao, J.; Fang, T.; Liu, G.; Li, X.; Wu, J. Estimating radiation dose to major organs in dental X-ray examinations: A phantom study. Radiat. Prot. Dosim. 2020, 192, 328–334. [Google Scholar] [CrossRef]
- Okano, T.; Sur, J. Radiation dose and protection in dentistry. Jpn. Dent. Sci. Rev. 2010, 46, 112–121. [Google Scholar] [CrossRef]
- Fontana, R.C.; Pasqual, E.; Miller, D.L.; Simon, S.L.; Cardis, E.; Thierry-Chef, I. Trends in Estimated Thyroid, Salivary Gland, Brain, and Eye Lens Doses From Intraoral Dental Radiography Over Seven Decades (1940 TO 2009). Health Phys. 2020, 118, 136–148. [Google Scholar] [CrossRef]
- Horner, K.; Rushton, V.E.; Walker, A.; Tsiklaskis, K.; Hirschmann, P.N.; van der Stelt, P.; Glenny, A.-M.; Velders, X.L.; Pavitt, S.; European Commission. Radiation Protection 136. European Guidelines on Radiation Protection in Dental Radiology. The Safe Use of Radiographs in Dental Practice; Office for Official Publications of the European Communities: Luxembourg, 2004. [Google Scholar]
- Fogarty, W.P.; Drummond, B.K.; Brosnan, M.G. The use of radiography in the diagnosis of oral conditions in children and adolescents. N. Z. Dent. J. 2015, 111, 144–150. [Google Scholar] [PubMed]
- Masthoff, M.; Gerwing, M.; Masthoff, M.; Timme, M.; Kleinheinz, J.; Berninger, M.; Heindel, W.; Wildgruber, M.; Schülke, C. Dental Imaging—A basic guide for the radiologist. Rofo 2019, 191, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Holan, G.; Yodko, E. Radiographic evidence of traumatic injuries to primary incisors without accompanying clinical signs. Dent. Traumatol. 2017, 33, 133–136. [Google Scholar] [CrossRef] [PubMed]
- Levin, L.; Day, P.F.; Hicks, L.; O’Connell, A.; Fouad, A.F.; Bourguignon, C.; Abbott, P.V. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: General introduction. Dent. Traumatol. Off. Publ. Int. Assoc. Dent. Traumatol. 2020, 36, 309–313. [Google Scholar] [CrossRef] [PubMed]
- Day, P.F.; Flores, M.T.; O’Connell, A.C.; Abbott, P.V.; Tsilingaridis, G.; Fouad, A.F.; Cohenca, N.; Lauridsen, E.; Bourguignon, C.; Hicks, L.; et al. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 3. Injuries in the primary dentition. Dent. Traumatol. Off. Publ. Int. Assoc. Dent. Traumatol. 2020, 36, 343–359. [Google Scholar] [CrossRef]
- Lembacher, S.; Schneider, S.; Lettner, S.; Bekes, K. Prevalence and patterns of traumatic dental injuries in primary teeth: A 3-year retrospective overview study in Vienna. Clin. Oral Investig. 2022, 26, 2085–2093. [Google Scholar] [CrossRef]
- Tewari, N.; Mathur, V.P.; Siddiqui, I.; Morankar, R.; Verma, A.R.; Pandey, R.M. Prevalence of traumatic dental injuries in India: A systematic review and meta-analysis. Indian J. Dent. Res. Off. Publ. Indian Soc. Dent. Res. 2020, 31, 601–614. [Google Scholar] [CrossRef]
- Foster Page, L.A.; Boyd, D.; Fuge, K.; Stevenson, A.; Goad, K.; Sim, D.; Thomson, W.M. The effect of bitewing radiography on estimates of dental caries experience among children differs according to their disease experience. BMC Oral Health 2018, 18, 137. [Google Scholar] [CrossRef]
- Poorterman, J.H.G.; Vermaire, E.H.; Hoogstraten, J. Value of bitewing radiographs for detecting approximal caries in 6-year-old children in the Netherlands. Int. J. Paediatr. Dent. 2010, 20, 336–340. [Google Scholar] [CrossRef]
- Pontes, L.R.A.; Novaes, T.F.; Lara, J.S.; Moro, B.L.P.; Gimenez, T.; Raggio, D.P.; Braga, M.M.; Mendes, F.M. Impact of the radiographic method on treatment decisions related to dental caries in primary molars: A before-after study. Clin. Oral Investig. 2019, 23, 4075–4081. [Google Scholar] [CrossRef]
- Pontes, L.R.A.; Novaes, T.F.; Lara, J.S.; Gimenez, T.; Moro, B.L.P.; Camargo, L.B.; Michel-Crosato, E.; Pannuti, C.M.; Raggio, D.P.; Braga, M.M.; et al. Impact of visual inspection and radiographs for caries detection in children through a 2-year randomized clinical trial: The Caries Detection in Children–1 study. J. Am. Dent. Assoc. 2020, 151, 407–415.e1. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Modality | DAP (CGy × cm2) | ED (µSv) |
|---|---|---|
| Dental radiograph | 2.57 | 0.77 |
| Bitewing radiograph | 2.57 | 0.77 |
| Occlusal radiograph | 7.43 | 2.22 |
| Indication | Number of Radiographs | Percentage (%) |
|---|---|---|
| Apical diagnostics | 495 | 22.7 |
| Endodontics | 244 | 11.2 |
| Focus detection | 68 | 3.1 |
| Caries diagnostics | 496 | 22.7 |
| Orthodontic | 15 | 0.7 |
| Dental surgery | 130 | 6.0 |
| Prosthetics | 4 | 0.2 |
| Trauma | 627 | 28.7 |
| Detection of developing teeth | 104 | 4.8 |
| TOTAL | 2138 | 100.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schüler, I.M.; Hennig, C.-L.; Buschek, R.; Scherbaum, R.; Jacobs, C.; Scheithauer, M.; Mentzel, H.-J. Radiation Exposure and Frequency of Dental, Bitewing and Occlusal Radiographs in Children and Adolescents. J. Pers. Med. 2023, 13, 692. https://doi.org/10.3390/jpm13040692
Schüler IM, Hennig C-L, Buschek R, Scherbaum R, Jacobs C, Scheithauer M, Mentzel H-J. Radiation Exposure and Frequency of Dental, Bitewing and Occlusal Radiographs in Children and Adolescents. Journal of Personalized Medicine. 2023; 13(4):692. https://doi.org/10.3390/jpm13040692
Chicago/Turabian StyleSchüler, Ina Manuela, Christoph-Ludwig Hennig, Rika Buschek, Rebecca Scherbaum, Collin Jacobs, Marcel Scheithauer, and Hans-Joachim Mentzel. 2023. "Radiation Exposure and Frequency of Dental, Bitewing and Occlusal Radiographs in Children and Adolescents" Journal of Personalized Medicine 13, no. 4: 692. https://doi.org/10.3390/jpm13040692